
Screening for Human T-Cell Lymphotropic Virus (HTLV) in Pregnant Women in the Peruvian Amazon and Systematic Review with Meta-Analysis of HTLV Infection in Peru

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
2.1. HTLV Infection in Pregnant Women
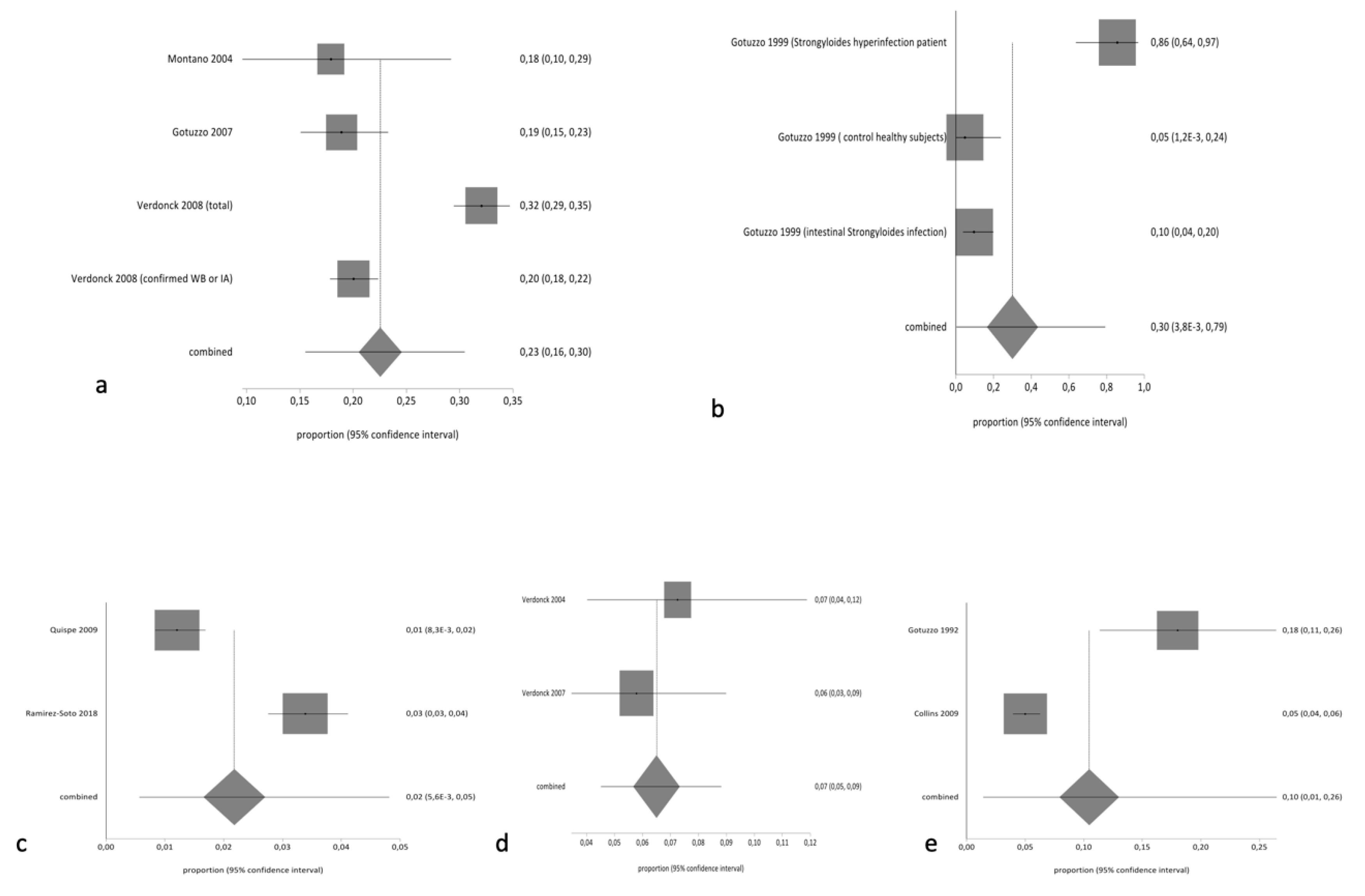
2.2. Systematic Review and Meta-Analysis of the Prevalence of HTLV Infection in Peru
3. Discussion
4. Materials and Methods
4.1. Type of Study and Study Period
4.2. Study Population and Data Collection
4.3. Data Analysis
4.4. Ethical Considerations
4.5. Literature Review of the Prevalence of HTLV Infection in Peru
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Paiva, A.; Smid, J.; Haziot, M.; Assone, T.; Pinheiro, S.; Fonseca, L.; Al, E. High risk of heterosexual transmission of human T-cell lymphotropic virus type 1 infection in Brazil. J. Med. Virol. 2017, 89, 1287–1294. [Google Scholar] [CrossRef]
- Rosadas, C.; Taylor, G.P. Mother-to-Child HTLV-1 Transmission: Unmet Research Needs. Front. Microbiol. 2019, 10, 999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, E.L. Infection with human T-lymphotropic virus types-1 and -2 (HTLV-1 and -2): Implications for blood transfusion safety. Transfus Clin. Biol. 2016, 23, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bangham, C.; Araujo, A.; Yamano, Y.; Taylor, G.P. HTLV-1-associated myelopathy/tropical spastic paraparesis. Nat. Rev. Dis. Prim. 2015, 1, 15012. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.A.; Harewood, J.C.K. Adult T Cell Leukemia-Lymphoma (ATL): State of the Art. Curr. Hematol. Malig. Rep. 2018, 13, 300–307. [Google Scholar] [CrossRef]
- Hino, S.; Katamine, S.; Miyata, H.; Tsuji, Y.; Yamabe, T.; Miyamoto, T. Primary Prevention of HTLV-I in Japan. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1996, 13, 199–203. [Google Scholar] [CrossRef]
- Dal Fabbro, M.M.F.J.; Da Cunha, R.V.; Bóia, M.N.; Portela, P.; Botelho, C.A.; De Freitas, G.M.B.; Soares, J.; Ferri, J.; Lupion, J. Infecção pelo HTLV 1/2: Atuação no pré-natal como estratégia de controle da doença no Estado de Mato Grosso do Sul. Rev. Soc. Bras. Med. Trop. 2008, 41, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Gessain, A.; Cassar, O. Epidemiological Aspects and World Distribution of HTLV-1 Infection. Front. Microbiol. 2012, 3, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagaya, Y.; Matsuoka, M.; Gallo, R. 40 years of the human T-cell leukemia virus: Past, present, and future. F1000Res 2019, 8, 228. [Google Scholar] [CrossRef] [Green Version]
- Quispe, N.C.; Feria, E.B.; De Santos-Fortuna, E.L.; Caterino-De-Araujo, A. Confirming the presence of HTLV-1 infection and the absence of HTLV-2 in blood donors from Arequipa, Peru. Rev. Inst. Med. Trop. Sao Paulo 2009, 51, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Wignall, F.S.; Hyams, K.C.; Phillips, I.A.; Escamilla, E.; Tejada, A.; Li, O.; Al, E. Sexual transmission of human T-lymphotropic virus type I in Peruvian prostitutes. J. Med. Virol. 1992, 38, 44–48. [Google Scholar] [CrossRef]
- Schwalb, A.; Pérez-Muto, V.; Cachay, R.; Tipismana, M.; Álvarez, C.; Mejía, F.; González-Lagos, E.; Gotuzzo, E. Early-Onset HTLV-1-Associated Myelopathy/Tropical Spastic Paraparesis. Pathogens 2020, 9, 450. [Google Scholar] [CrossRef]
- Gotuzzo, E.; Escamilla, J.; Phillips, I.A.; Sanchez, J.; Wignall, F.S.; Antigoni, J. The Impact of Human T-Lymphotrophic Virus Type I/II Infection on the Prognosis of Sexually Acquired Cases of Acquired Immunodeficiency Syndrome. Arch. Intern. Med. 1992, 152, 1429–1432. [Google Scholar] [CrossRef]
- Alva, I.E.; Orellana, E.R.; Blas, M.M.; Bernabe-Ortiz, A.; Cotrina, A.; Chiappe, M.; Kochel, T.J.; Carcamo, C.P.; García, P.J.; Zunt, J.R.; et al. HTLV-1 and -2 infections among 10 indigenous groups in the Peruvian Amazon. Am. J. Trop. Med. Hyg. 2012, 87, 954–956. [Google Scholar] [CrossRef] [Green Version]
- Cabezas, C.; Trujillo, O.; Balbuena, J.; Marin, L.; Suárez, M.; Themme, M.; Rodriguez, H.; Valencia, P.; Crispin-Huamani, L. Prevalencia de infección por los virus de la hepatitis B, D y por retrovirus en la etnia Matsés (Loreto, Peru). Rev. Peru Med. Exp. Salud Publica 2020, 37, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Medeot, S.; Nates, S.; Recalde, A.; Gallego, S.; Maturano, E.; Giordano, M.; Serra, H.; Reategui, J.; Cabezas, C. Prevalence of antibody to human T cell lymphotropic virus types 1/2 among aboriginal groups inhabiting northern Argentina and the Amazon region of Peru. Am. J. Trop. Med. Hyg. 1999, 60, 623–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, I.A.; Hyams, K.C.; Wignall, F.S.; Moran, A.; Gotuzzo, E.; Sanchez, J.; Roberts, C. HTLV-I Coinfection in a HIV-1-Infected Peruvian Population. J. Acquir. Immune Defic. Syndr. 1991, 4, 301–302. [Google Scholar] [PubMed]
- Hyams, K.C.; Phillips, I.A.; Tejada, A.; Wignall, F.S.; Roberts, C.R.; Escamilla, J. Three-year incidence study of retroviral and viral hepatitis transmission in a Peruvian prostitute population. J. Acquir. Immune Defic. Syndr. 1993, 6, 1353–1357. [Google Scholar] [PubMed]
- Gotuzzo, E.; Sánchez, J.; Escamilla, J.; Carrillo, C.; Phillips, I.A.; Moreyra, L.; Stamm, W.; Ashley, R.; Roggen, E.L.; Kreiss, J.; et al. Human T cell lymphotropic virus type I infection among female sex workers in Peru. J. Infect. Dis. 1994, 169, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, L.; Muñoz, D.; Gotuzzo, E.; Yi, A.; Watts, D. Prácticas sexuales y seroprevalencia de infección por VIH, HTLV-1 sífilis en meretrices clandestinas de Lima. Rev. Med. Hered 1996, 7, 162–171. [Google Scholar] [CrossRef] [Green Version]
- Gotuzzo, E.; Yamamoto, V.; Kanna, M.; Chauca, G.; Watts, D.M. Human T-cell lymphotropic virus type I infection among Japanese immigrants in Peru. Int. J. Infect. Dis. 1996, 1, 75–77. [Google Scholar] [CrossRef] [Green Version]
- Zurita, S.; Costa, C.; Waits, D.; Indacochea, S.; Campos, P.; Sanchez, J.; Gotuzzo, E. Prevalence of human retroviral infection in Quillabamba and Cuzco, Peru: A new endemic area for human T cell lymphotropic virus type 1. Am. J. Trop. Med. Hyg. 1997, 56, 561–565. [Google Scholar] [CrossRef]
- Garrido, P.; Anicama, R.; Gotuzzo, E.; Chauca, G.; Watts, D. HTLV-I en población de alto riesgo sexual de Pisco, Ica, Perú. Rev. Med. Hered 2013, 8, 104–107. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, D.; Trujillo, L.; Gotuzzo, E.; Nizama, M.; Watts, D. Prácticas sexuales de riesgo y seroprevalencia de infección por VIH-1. HTLV-1, sífilis y hepatitis B en varones drogadictos no endovenosos de Lima. Rev. Med. Hered 1997, 8, 92–103. [Google Scholar] [CrossRef]
- Fujiyoshi, T.; Li, H.C.; Lou, H.; Yashiki, S.; Karino, S.; Zaninovic, V.; Oneegllo, S.G.; Camacho, M.; Andrade, R.; Hurtado, L.V.; et al. Characteristic distribution of HTLV type I and HTLV type II carriers among native ethnic groups in South America. AIDS Res. Hum. Retroviruses 1999, 15, 1235–1239. [Google Scholar] [CrossRef]
- Zunt, J.R.; Alarcón, J.; Montano, S.; Longstreth, W.J.; Price, R.; Holmes, K. Quantitative assessment of subclinical spasticity in human T-cell lymphotropic virus type I infection. Neurology 1999, 53, 386. [Google Scholar] [CrossRef] [Green Version]
- Gotuzzo, E.; Terashima, A.; Alvarez, H.; Tello, R.; Infante, R.; Watts, D.M.; Freedman, D.O. Strongyloides stercoralis hyperinfection associated with human T cell lymphotropic virus type-1 infection in Peru. Am. J. Trop. Med. Hyg. 1999, 60, 146–149. [Google Scholar] [CrossRef] [Green Version]
- García Pinto, J.; Jiménez Luna, G. Estudio Comparativo Sobre la Seroprevalencia de HTLV-1 en Una Población de Adultos en Régimen Privado de Libertad y una Población Urbano Marginal de Lima. 2002. Available online: https://cybertesis.unmsm.edu.pe/bitstream/handle/20.500.12672/2076/Garcia_pj.pdf?sequence=1 (accessed on 4 January 2021).
- Zunt, J.R.; Dezzutti, C.S.; Montano, S.M.; Thomas, K.K.; Alarcón, J.O.V.; Quijano, E.; Courtois, B.N.; Sánchez, J.L.; Campos, P.; Gotuzzo, E.; et al. Cervical shedding of human T cell lymphotropic virus type I is associated with cervicitis. J. Infect. Dis. 2002, 186, 1669–1672. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Palacios, C.; Gotuzzo, E.; Vandamme, A.M.; Maldonado, Y. Seroprevalence and risk factors for human T-cell lymphotropic virus (HTLV-I) infection among ethnically and geographically diverse Peruvian women. Int. J. Infect. Dis. 2003, 7, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Verdonck, K.; Henriquez, C.; Echevarria, J.; Huayanay, L.; Agapito, J.; Cairampona, R.; Ramos, C.; Gotuzzo, E. Asociación entre infección por el virus linfotrópico humano de células T tipo I (HTLV-I) y mortalidad en pacientes hospitalizados con tuberculosis. Rev. Médica Hered. 2004, 15, 197–202. Available online: http://www.scielo.org.pe/pdf/rmh/v15n4/v15n4ao3.pdf (accessed on 4 January 2021). [CrossRef]
- Montano, S.M.; Zunt, J.R.; Rodriguez, L.; Quispe, I.; Rodriguez, C.; Altamirano, J.; Bautista, C.T.; Alarcón, J.O.V.; Longstreth, W.T.; Holmes, K.K. Human T cell lymphotropic virus type 1 infection and early neurologic development: A pilot study of 48 children. Clin. Infect. Dis. 2004, 39, 1079–1082. [Google Scholar] [CrossRef]
- Juscamaita, P.Z.; Torrealva, C.M.; Cairampoma, M.R.; Gotuzzo, H.E. Seroprevalencia del virus linfotropo T humano tipo 1 (HTLV-1) en gestantes y grupos de elevada prevalencia para enfermedades de transmisión sexual de Ayacucho, Perú. Rev. Peru. Med. Exp. Salud Publica 2004, 21, 269–272. [Google Scholar]
- Blas, M.; Bravo, F.; Castillo, W.; Castillo, W.J.; Ballona, R.; Navarro, P.; Catacora, J.; Cairampoma, R.; Gotuzzo, E. Norwegian scabies in Peru: The impact of human T cell lymphotropic virus type I infection. Am. J. Trop. Med. Hyg. 2005, 72, 855–857. [Google Scholar] [CrossRef]
- Laguna-Torres, V.A.; Pérez-Bao, J.; Chauca, G.; Sovero, M.; Blichtein, D.; Chunga, A.; Flores, W.; Retamal, A.; Mendoza, S.; Cruz, M.; et al. Epidemiology of transfusion-transmitted infections among multi-transfused patients in seven hospitals in Peru. J. Clin. Virol. 2005, 34, 2–9. [Google Scholar] [CrossRef]
- Alarcón, J.O.; Friedman, H.B.; Montano, S.M.; Zunt, J.R.; Holmes, K.K.; Quinnan, G.V.J. High endemicity of human T-cell lymphotropic virus type 1 among pregnant women in Peru. J. Acquir. Immune Defic. Syndr. 2006, 42, 604–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zunt, J.R.; La Rosa, A.M.; Peinado, J.; Lama, J.R.; Suarez, L.; Pun, M.; Cabezas, C.; Sanchez, J. Risk factors for HTLV-II infection in Peruvian men who have sex with men. Am. J. Trop. Med. Hyg. 2006, 74, 922–925. [Google Scholar] [CrossRef] [Green Version]
- Zunt, J.R.; Montano, S.M.; Beck, I.; Alarcón, J.O.V.; Frenkel, L.M.; Bautista, C.T.; Price, R.; Longstreth, W.T. Human T-lymphotropic virus type 1-associated myelopathy/tropical spastic paraparesis: Viral load and muscle tone are correlated. J. Neurovirol. 2006, 12, 466–471. [Google Scholar] [CrossRef] [Green Version]
- Gotuzzo, E.; Moody, J.; Verdonck, K.; Cabada, M.M.; González, E.; Van Dooren, S.; Vandamme, A.M.; Terashima, A.; Vermund, S.H. Frequent HTLV-1 infection in the offspring of Peruvian women with HTLV-1-associated myelopathy/tropical spastic paraparesis or strongyloidiasis. Rev. Panam. Salud Publica 2007, 22, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Verdonck, K.; González, E.; Henostroza, G.; Nabeta, P.; Llanos, F.; Cornejo, H.; Vanham, G.; Seas, C.; Gotuzzo, E. HTLV-1 infection is frequent among out-patients with pulmonary tuberculosis in northern Lima, Peru. Int. J. Tuberc. Lung Dis. 2007, 11, 1066–1072. [Google Scholar]
- Verdonck, K.; González, E.; Schrooten, W.; Vanham, G.; Gotuzzo, E. HTLV-1 infection is associated with a history of active tuberculosis among family members of HTLV-1-infected patients in Peru. Epidemiol. Infect. 2008, 136, 1076–1083. [Google Scholar] [CrossRef]
- La Rosa, A.M.; Zunt, J.R.; Peinado, J.; Lama, J.R.; Ton, T.G.N.; Suarez, L.; Pun, M.; Cabezas, C.; Sanchez, J. Retroviral Infection in Peruvian Men Who Have Sex with Men. Clin. Infect. Dis. 2009, 49, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Collins, J.A.; Hernández, A.V.; Hidalgo, J.A.; Salazar, R.; Rodríguez, L.; Castillo, R.; Vega, J.; Illescas, R.; Villena, J.; Sotelo, C.; et al. HTLV-I infection is not associated with a higher risk of death in Peruvian HIV-infected patients. Rev. Inst. Med. Trop. Sao Paulo 2009, 51, 197–201. [Google Scholar] [CrossRef] [Green Version]
- Delgado, S.; González, E.; Bravo, F.; Gotuzzo, E. Infección por HTLV-1 y HIV en pacientes con herpes zoster en Perú. Rev. Medica Hered. 2011, 22, 98–102. [Google Scholar] [CrossRef]
- Cárcamo, C.P.; Campos, P.E.; García, P.J.; Hughes, J.P.; Garnett, G.P.; Holmes, K.K. Prevalences of sexually transmitted infections in young adults and female sex workers in Peru: A national population-based survey. Lancet Infect. Dis. 2012, 12, 765–773. [Google Scholar] [CrossRef] [Green Version]
- Mayer, E.F.; Ita, F.; Gonzalez, E.; Verdonck, K.; Bravo, F.; Clark, D.; Gotuzzo, E. Association between onychodystrophy and human T-lymphotropic virus type 1 infection. Int. J. Infect. Dis. 2013, 17, e312–e316. [Google Scholar] [CrossRef] [Green Version]
- Blas, M.M.; Alva, I.E.; García, P.J.; Cárcamo, C.; Montano, S.; Mori, N.; Al, E. High prevalence of human T-lymphotropic virus infection in indigenous women from the peruvian Amazon. PLoS ONE 2013, 8, e73978. [Google Scholar] [CrossRef]
- Ita, F.; Mayer, E.F.; Verdonck, K.; Gonzalez, E.; Clark, D.; Gotuzzo, E. Human T-lymphotropic virus type 1 infection is frequent in rural communities of the southern Andes of Peru. Int. J. Infect. Dis. 2014, 19, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.; Heitzinger, K.; Pollett, S.; Calderón, M.; Alarcón, J.; Ton, T.G.N.; Zunt, J.R. The changing epidemiology of human t-cell lymphotropic virus type 1 infection in peruvian female sex workers, 1993-2010. Am. J. Trop. Med. Hyg. 2017, 96, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Soto, M.C.; Huichi-Atamari, M. Prevalence of hepatitis B and human T-lymphotropic virus infection among blood donors at a hospital in the south-central highlands of Peru. Transfus. Med. 2018, 28, 263–265. [Google Scholar] [CrossRef]
- Berini, C.A.; Delfino, C.; Torres, O.; García, G.; Espejo, R.; Pianciola, L.; Juarez, M.; Arribere, G.; Nadal, M.; Eirin, M.E.; et al. HTLV-1 cosmopolitan and HTLV-2 subtype b among pregnant women of non-endemic areas of Argentina. Sex. Transm. Infect. 2013, 89, 333–335. [Google Scholar] [CrossRef]
- Trenchi, A.; Gastaldelllo, R.; Balangero, M.; Irizar, M.; Cudolá, A.; Gallego, S. Retrospective Study of the Prevalence of Human T-Cell Lymphotropic Virus-Type 1/2, HIV, and HBV in Pregnant Women in Argentina. J. Med. Virol. 2007, 79, 1974–1978. [Google Scholar] [CrossRef] [PubMed]
- Figueiró-Filho, E.A.; Senefonte, F.R.D.A.; Lopes, A.H.A.; De Morais, O.O.; Souza, V.G.; Maia, T.L.; Duarte, G. Frequency of HIV-1, rubella, syphilis, toxoplasmosis, cytomegalovirus, simple herpes virus, hepatitis B, hepatitis C, Chagas’ disease and HTLV I/II infection in pregnant women of State of Mato Grosso do Sul. Rev. Soc. Bras. Med. Trop. 2007, 40, 181–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, L.H.M.; Viana, M.C. Prevalence and risk factors for HIV, syphilis, hepatitis B, hepatitis C, and HTLV-I/II infection in low-income postpartum and pregnant women in Greater Metropolitan Vitória, Espírito Santo State, Brazil. Cad. Saude Publica 2009, 25, 668–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carles, G.; Tortevoye, P.; Tuppin, P.; Ureta-Vidal, A.; Peneau, C.; El Guindi, W.; Gessain, A. HTLV1 infection and pregnancy. J. Gynecol. Obs. Biol Reprod. 2004, 33, 14–20. [Google Scholar] [CrossRef]
- Tortevoye, P.; Tuppin, P.; Peneau, C.; Carles, G.; Gessain, A. Decrease of human T-cell lymphotropic virus type I prevalence and low incidence among pregnant women from a high endemic ethnic group in French Guiana. Int. J. Cancer 2000, 87, 534–538. [Google Scholar] [CrossRef]
- Treviño, A.; Aguilera, A.; Caballero, E.; Toro, C.; Eiros, J.; Ortiz de Lejarazu, R.; Rodríguez-Calviño, J.; Tuset, C.; Gómez-Hernando, C.; Rodríguez-Iglesias, M.; et al. Seroprevalence of HTLV-1 y 2 Infection among Native and Immigrant Pregnant Women in Spain. AIDS Res. Hum. Retroviruses 2009, 25, 551–554. [Google Scholar] [CrossRef]
- Carvalho, E.M.; Da Fonseca Porto, A. Epidemiological and clinical interaction between HTLV-1 and Strongyloides stercoralis. Parasite Immunol. 2004, 26, 487–497. [Google Scholar] [CrossRef]
- Ponce-Eusebio, E.; Anguita, E.; Paulino-Ramirez, R.; Candel, F.J. HTLV-1 infection: An emerging risk. Pathogenesis, epidemiology, diagnosis and associated diseases. Rev Esp Quim. 2019, 32, 485–496. [Google Scholar]
- Ortiz-Martínez, S.; Ramos-Rincón, J.M.; Vásquez-Chasnamote, M.E.; Alarcón-Baldeón, J.J.; Parraguez-De-La-Cruz, J.; Gamboa-Paredes, O.N.; Schillyk-Guerra, P.; Espinoza-Venegas, L.A.; Pinedo-Cancino, V.V.; Perez-Tanoira, R.; et al. A cross-sectional study of seroprevalence of strongyloidiasis in pregnant women (Peruvian amazon basin). Pathogens 2020, 9, 348. [Google Scholar] [CrossRef]
- Buonfrate, D.; Formenti, F.; Perandin, F.; Bisoffi, Z. Novel approaches to the diagnosis of Strongyloides stercoralis infection. Clin. Microbiol. Infect. 2015, 21, 543–552. [Google Scholar] [CrossRef] [Green Version]
- Ramos-Rincón, J.-M.; Ortiz-Martínez, S.; Vásquez-Chasnamote, M.-E.; Gamboa-Paredes, O.-N.; Pinedo-Cancino, V.-V.; Ramal-Asayag, C.; Górgolas-Hernández-Mora, M.; Casapía-Morales, M. Chagas Disease in Pregnant Women in the Peruvian Amazon Basin. Cross-Sectional Study. Front. Vet. Sci. 2020, 7, 556. [Google Scholar] [CrossRef]
- Adaui, V.; Verdonck, K.; Best, I.; González, E.; Tipismana, M.; Arávalo, J.; Vanham, G.; Campos, M.; Zimic, M.; Gotuzzo, E. SYBR Green-based quantitation of human T-lymphotropic virus type 1 proviral load in Peruvian patients with neurological disease and asymptomatic carriers: Influence of clinical status, sex, and familial relatedness. J. Neurovirol. 2006, 12, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.-S.; Liu, X. Statistical methods in the meta-analysis of prevalence of human diseases. J. Biostat. Epidemiol. 2016, 2, 20–24. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Case | Age, Years | Gestational Age (Days) | Type of Pregnancy | Residence | HTLV-1/2 | Proviral Load (Copy /1000 Cell) | Strongyloides Serology |
|---|---|---|---|---|---|---|---|
| 1 | 19 | 88 | Primipara | Urban | HTLV-1 | Not available | Positive |
| 2 | 35 | 181 | Multipara | Urban | HTLV-1 | 950 | Negative |
| 3 | 20 | 233 | Multipara | Urban | HTLV-1 | Undetectable | Negative |
| 4 | 20 | 274 | Primipara | Periurban | HTLV-1 | <10 | Negative |
| 5 | 19 | 63 | Multipara | Periurban | HTLV-1 | 3324 | Positive |
| Study ID | Setting(s)/ (Department) | Population | Prevalence HTLV-1 | Diagnostic Procedure |
|---|---|---|---|---|
| Phillips 1991 [17] | Peru | 552 HIV: 495 men and 57 women | 18.6% men 5.3% women | -ELISA (Cambridge Bioscience) -Western blot (DuPont) -RIPA |
| Wignall 1992 [11] | Callao (Lima) Iquitos | 395 sex workers in Callao 72 sex workers in Iquitos 510 women attended in antenatal clinic in Lima | 21.8% 4.2% 3.1% | -EIA (Cambridge Bioscience; Worchester, MA) -Western blot (DuPont; Wilmington, DE) -RIPA |
| Gottuzo 1992 [13] | Lima | 111 men with HIV | 18% | -ELISA (Cambridge Bioscience Worcester, Mass) -Western blot (DuPont, Wilmington, Del) |
| Hyams 1993 [18] | Callao (Lima) | 966 sex workers | 17.6% | -ELISA (Cambridge Bioscence, Worcester, MA, USA) -Western blot (DuPont, Wilmington, DE, USA) -RIPA |
| Gotuzzo 1994 [19] | Lima | 400 sex workers | 7% | -ELISA (Genetic Systems, Seattle). -Western blot (Cambridge Biotech, Worcester, MA) |
| Trujillo 1996 [20] | Lima | 158 sex workers | 3.8% | -ELISA (Cambridge Biotech, Worcester, MA) -Western blot (Cambridge Biotech, Worcester, MA) |
| Gotuzzo 1996 [21] | Lima | 407 (280 women and 127 men) Japanese migrants and their children in Peru | 6.8% women 3.2% men | -ELISA (Gentic Systems, Seattle, WA) -Western blot (Cambridge Biotech, Worcester, MA) |
| Zurita 1997 [22] | Quillabamba and Cuzco | 370 volunteers 211 pregnant 51 sex workers 48 MSM 47 associated with ITS | 5.1% 2.3% 13.7% 6.2% 8.5% | -ELISA (Genetic Systems, Seattle, WA) -Western blot (Cambridge Biotech, Worcester, MA) |
| Garrido 1997 [23] | Pisco–Ica | 54 MSM 32 Sex workers | 1.9% 10.4% | -ELISA (Genetic Systems, Seattle) -Western blot (Cambridge Biotech, Worcester, MA) |
| Muñoz 1997 [24] | Lima | 298 non-intravenous drug users | 2.3% | -ELISA (Cambridge Biotech, Worcester, MA) -Western blot (Cambridge Biotech, Worcester, MA) |
| Medeot 1999 [16] | Peruvian Amazon | 456 participants | 0.44% | -Particle agglutination (PA) technique (Serodia; Fujirebio, Inc., Tokyo, Japan) -IFA -Western blot (Problot-HTLV-1; Fujirebio, Inc) |
| Fujiyoshi 1999 [25] | Peru | 66 participants from the Aymara ethnic group | 1.6% | -Particle agglutination (PA) (Serodia HTLV-1, Fujirebio, Tokyo, Japan) -Western blot (HTLV Blot 2.3/HTLV Blot 2.4; Diagnostic Biotechnology, Singapore) |
| Zunt 1999 [26] | Callao (Lima) | 255 sex workers | 13% | -ELISA (Cambridge Bioscience, Worcester, MA) -Western blot (Cambridge Bioscience) |
| Gotuzzo 1999 [27] | Lima | 21 Strongyloides hyperinfection patients 21 healthy controls 62 patients with intestinal Strongyloides infection | 85.7% 4.7% 9.7% | -ELISA (Cambridge Bioscience, Worcester, MA) -Western blot (DuPont, Wilmington, DE) |
| Garcia 2002 [28] | Lima | 400 prisoners (EPCROL) 400 participants from Puente de Piedra Hospital (Lima) | 1.5% 0.75% | -ELISA -Western blot |
| Zunt 2002 [29] | Lima | 1119 sex workers | 8.7% | -ELISA (Cambridge Bioscience) -Western blot (Cambridge Bioscience) |
| Sanchez-Palacios 2003 [30] | Huanta El Carmen Lima | 568 women | 2.5% | -ELISA (Platelia HTLV-I New, Sanofi Diagnostics Pasteur, Paris, France) -IFA (California Department of Health Services, Berkeley, CA, USA) -RIBA (Chiron Corporation, Emeryville, CA, USA) -Western blot (WB, Cambridge Biotech, Worcester, MA, USA) -PCR (Belgium, AM Vandamme) |
| Verdonck 2004 [31] | Lima | 193 tuberculosis patients | 7.3% | -ELISA -Western blot |
| Montano 2004 [32] | Lima | 67 children exposed to HTLV-1 | 18% | -ELISA (Platelia HTLV-1; Sanofi Pasteur) -Western blot (Genelabs Diagnostics) |
| Juscamaita 2004 [33] | Huamanga (Ayacucho) | 602 pregnant women 85 sex workers 74 MSM | 0.5% 0% 0% | -ELISA (Vironostika) -Inno-LIA HTLV I/II score (Innogenetics, Ghent, Belgium) |
| Blas 2005 [34] | Lima | 23 Norwegian scabies patients | 69.6% | -ELISA (Cambridge Bioscience, Worcester, MA) -Western immunoblot (DuPont, Wilmington, DE) |
| Laguna-Torres 2005 [35] | Lima y Cuzco | 351 multi-transfused patients | 3.1% | -ELISA (Vironostika) -lmmunoblot techniques (HTLV blot 2.4 Genelabs Diagnostic) |
| Alarcon 2006 [36] | Lima | 2492 pregnant women | 1.7% | -ELISA (Cambridge Bioscience Corp, Worcester, MA) -Western blot (Cambridge Bioscience Corp) |
| Zunt 2006 [37] | 6 Peruvian cities (Arequipa, Iquitos, Pucallpa, Lima, Piura and Sullana) | 2073 MSM | 2.1% | -ELISA (Vironostika) -Western blot (HTLV-I/II blot 2.4; Genelabs Diagnostics, Singapore) |
| Zunt 2006 [38] | Lima | 53 myelopathy patients | 81% | -ELISA (Cambridge Bioscience, Worcester, MA) -Western blot (Genelabs Diagnostics, Singapore) |
| Gotuzzo 2007 [39] | Lima | 370 descendants of mothers infected with HTLV-1 | 19% (there were 641 descendants, but only 370 agreed to be tested) | -ELISA (Sanofi Diagnostics Pasteur, France; Bio-Rad Laboratories, U.S.A.; or Cambridge Biotech, USA) -Western blot (Genelabs Diagnostics, Singapore) or (Innogenetics, Belgium) |
| Verdonck 2007 [40] | Lima | 311 tuberculosis patients | 5.8% | -ELISA (Ortho y Platelia) -Inno-LIA |
| Verdonck 2008 [41] | Lima | 1233 relatives of people infected with HTLV-1 | 32% 20% (confirmed WB or immunoassay) | -ELISA (Sanofi Diagnostics Pasteur, Marnes-la-Coquette, France; Bio-Rad Laboratories, Hercules, CA, USA; or Cambridge Biotech, Worcester, MA, USA) -Western blot (Genelabs Diagnostics, Singapore) |
| Quispe 2009 [10] | Arequipa | 2732 blood donors | 1.2% | -ELISA (Vironostika HTLV-I/II, BioMerieux, France) -BioELISA HTLV-I+II (BioKit S.A., Spain) -Western blot (WB 2.4, Genelabs Diagnostics, Singapore) |
| La Rosa 2009 [42] | Arequipa, Iquitos, Pucallpa, Lima, Piura, Sullana | 2655 MSM | 1.8% | -ELISA (Vironostika) -Western blot (HTLV-I/II blot 2.4; Genelabs Diagnostics, Singapore) |
| Collins 2009 [43] | Lima | 1456 HIV patients | 5% | -EIA (Sanofi Pasteur, France or Abbott, USA) -Western blot (Cambridge Biotech, USA or DAVIH-Blot, Cuba) |
| Delgado 2011 [44] | Lima | 44 herpes zoster patients | 5% | -ELISA (Ortho) |
| Alva 2012 [14] | 10 indigenous groups in the Amazon less than 12 h by boat from 4 ports: Iquitos, Pucallpa, Yurimaguas y Puerto Maldonado | 638 participants | 1.9% | -ELISA (Vironostika, NC) -Western blot (HTLV-1/2 Blot 2.4; Genelabs Diagnostics, Singapore) |
| Carcamo 2012 [45] | 24 cities with more than 50,000 inhabitants. Branch of the PREVENT trial | 1530 serum samples from participants aged 18 to 29 years old | 0.3% | -ELISA (Vironostika, Durham, NC, USA) -Western blot 2·4 (Genelabs Diagnostics, Science Park, Singapore) |
| Mayer 2013 [46] | Lima | 893 adults (428 close relatives of a person with HTLV-1 infection, 118 with neurological disorder, 160 with strongyloidiasis, and 181 others) | 26.4% | -ELISA (Murex, Ortho y Platelia) -Western blot -Inno-LIA |
| Blas 2013 [47] | Lima and Pucallpa | 1253 women of the Shipibo-Konibo ethnic group | 5.9% | -HTLV ELISA (Vironostika, North Carolina) -Western blot (HTLV-1/2 Blot 2.4, Genelabs Diagnostics, Singapore) |
| Ita 2014 [48] | Provinces of Cangallo, Vilcashuaman and Parinacochas (Ayacucho) | 397 participants | 2.8% | -ELISA HTLV I+II Murex Biotech Ltd., Dartford, UK. -HTLV-I/HTLV-II Ab.capture ELISA test system (Ortho Clinical Diagnostic, Amersham, UK) -Inno-LIA HTLV-I/II Score (Innogenetics, Ghent, Belgium) -Western blot HTLV Blot 2.4 (MP Diagnostics, Singapore) |
| Stewart 2017 [49] | Callao (Lima) | 1918 sex workers (n = 1477 in period 1, n = 62 in period 2, and n = 379 in period 3) | 9.6% | -HTLV EIA (Cambridge Bioscence, Worcester, MA) -Western blot (Cambridge Bioscence) -Vironostika HTLV I/II Microelisa System, Organon Teknika/Biomérieux, Durham, NC -HTLV I/II Western blots (Genelabs Diagnostics, Singapore) -Bioelisa HTLV I/II 5.0, Biokit, Barcelona, Spain -HTLV I/II score; Innogenetics, Ghent, Belgium |
| Ramirez-Soto 2018 [50] | Abancay | 2895 blood samples | 3.4% | -ELISA (Biokit, Barcelona, Spain) |
| Cabezas 2020 [15] | Requena (Loreto) | 806 participants (adults and children) | 0.6% | -ELISA (bioELISA) -LIA (Inmunogenetic) |
| Ramos et al. (present study) | Iquitos | 300 pregnant women | 1.7% | -ELISA (HTLV I+II ELISA recombinante v.4.0, Wiener lab, Rosario, Argentina) |
| Population Group | Pooled Prevalence | 95% CI | I2% |
|---|---|---|---|
| Pregnant women | 0.025 | 0.012–0.040 | 90.7 |
| Sex workers | 0.093 | 0.056–0.137 | 92.9 |
| HIV infection | 0.104 | 0.013–0.64 | 94.8 |
| Men who have sex with men | 0.033 | 0.009–0.069 | 97.1 |
| Relatives/descendants of HTLV patients | 0.225 | 0.155–0.304 | 94.7 |
| Strongyloides infections | 0.300 | 0.003–0.792 | 96 |
| Tuberculosis | 0.065 | 0.045–0.088 | 0 |
| Blood donors | 0.021 | 0.005–0.048 | 96.8 |
| General population | 0.029 | 0.012–0.053 | 95.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Rincón, J.-M.; Ortiz-Martínez, S.; Vásquez-Chasnamote, M.-E.; de-Miguel-Balsa, E.; Gamboa-Paredes, O.-N.; Talledo-Albujar, M.-J.; López-Campana, G.; Celis-Salinas, J.C.; Prieto-Pérez, L.; Górgolas-Hernández, M.; et al. Screening for Human T-Cell Lymphotropic Virus (HTLV) in Pregnant Women in the Peruvian Amazon and Systematic Review with Meta-Analysis of HTLV Infection in Peru. Pathogens 2021, 10, 260. https://doi.org/10.3390/pathogens10030260
Ramos-Rincón J-M, Ortiz-Martínez S, Vásquez-Chasnamote M-E, de-Miguel-Balsa E, Gamboa-Paredes O-N, Talledo-Albujar M-J, López-Campana G, Celis-Salinas JC, Prieto-Pérez L, Górgolas-Hernández M, et al. Screening for Human T-Cell Lymphotropic Virus (HTLV) in Pregnant Women in the Peruvian Amazon and Systematic Review with Meta-Analysis of HTLV Infection in Peru. Pathogens. 2021; 10(3):260. https://doi.org/10.3390/pathogens10030260
Chicago/Turabian StyleRamos-Rincón, José-Manuel, Sonia Ortiz-Martínez, María-Esteyner Vásquez-Chasnamote, Eva de-Miguel-Balsa, Olga-Nohelia Gamboa-Paredes, Michael-John Talledo-Albujar, Giovanni López-Campana, Juan Carlos Celis-Salinas, Laura Prieto-Pérez, Miguel Górgolas-Hernández, and et al. 2021. "Screening for Human T-Cell Lymphotropic Virus (HTLV) in Pregnant Women in the Peruvian Amazon and Systematic Review with Meta-Analysis of HTLV Infection in Peru" Pathogens 10, no. 3: 260. https://doi.org/10.3390/pathogens10030260