
Pulmonary Findings of [18F]FDG PET/CT Images on Asymptomatic COVID-19 Patients

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Data Sources and Review Approaches
3. Results
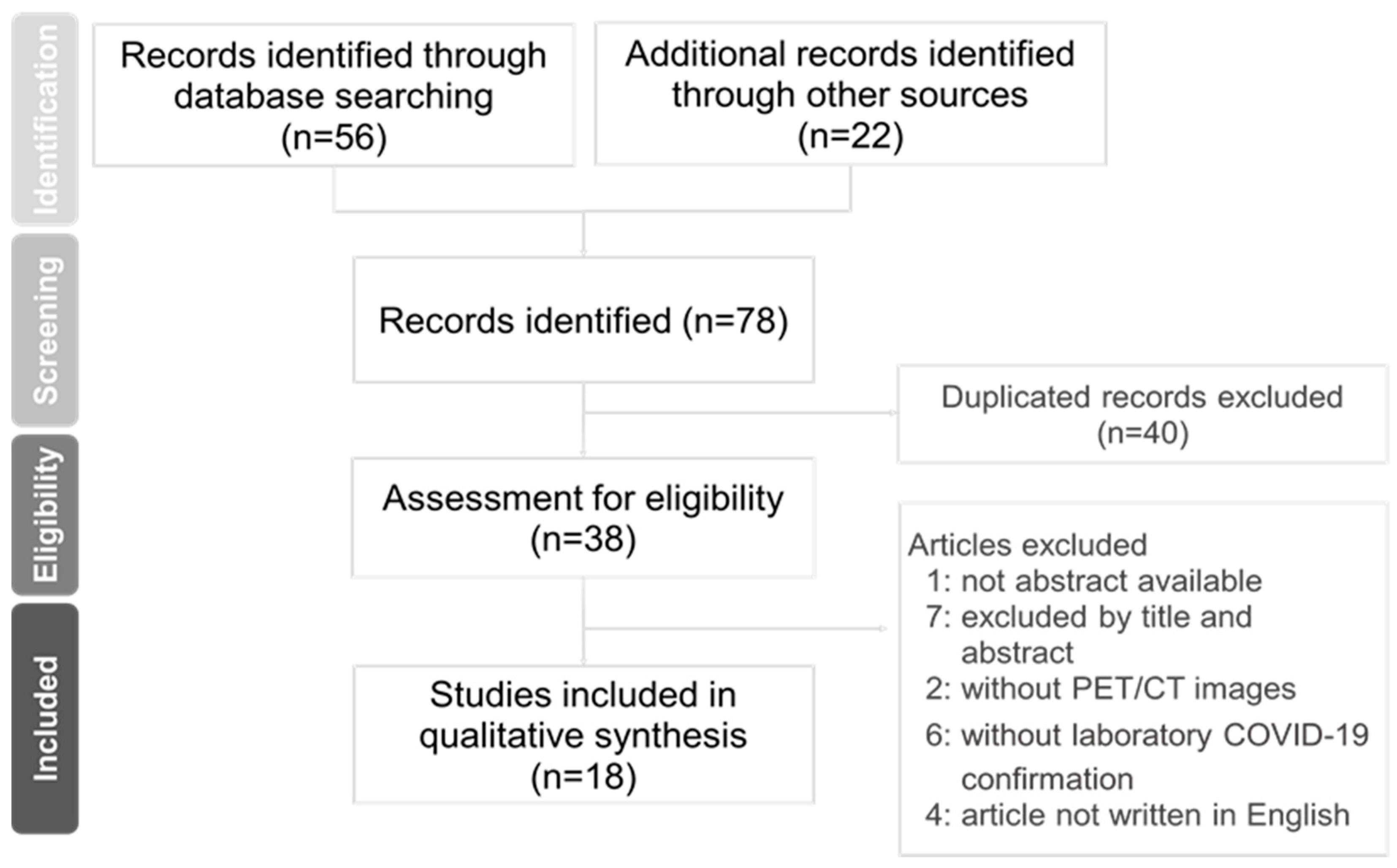
3.1. Selection of Studies
3.2. Patient Features
3.3. [18F]FDG PET/CT Findings
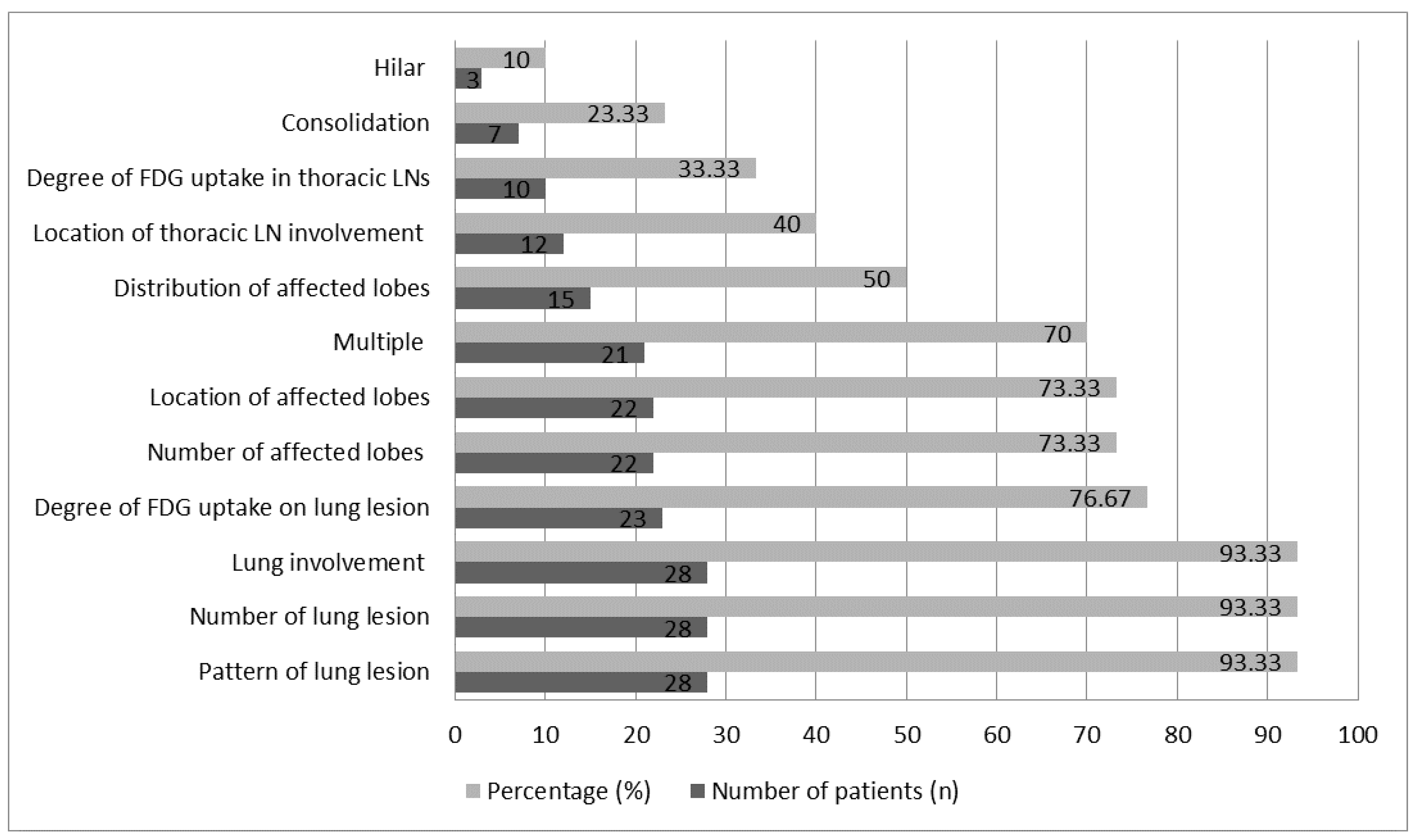
3.4. Characteristics of Pulmonary Findings
3.5. Patient Management and Hospital Infection Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19) Outbreak. Available online: https://www.who.int (accessed on 23 June 2021).
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef]
- Lee, Y.; Min, P.; Lee, S.; Kim, S.W. Prevalence and Duration of Acute Loss of Smell or Taste in COVID-19 Patients. J. Korean Med. Sci. 2020, 35, e174. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noh, J.Y.; Yoon, J.G.; Seong, H.; Choi, W.S.; Sohn, J.W.; Cheong, H.J.; Kim, W.J.; Song, J.Y. Asymptomatic infection and atypical manifestations of COVID-19: Comparison of viral shedding duration. J. Infect. 2020, 81, 816–846. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D. Role of functional imaging in the management of lymphoma. J. Clin. Oncol. 2011, 29, 1844–1854. [Google Scholar] [CrossRef] [PubMed]
- Fuster, D.; Duch, J.; Paredes, P.; Velasco, M.; Muñoz, M.; Santamaría, G.; Fontanillas, M.; Pons, F. Preoperative staging of large primary breast cancer with [18F]fluorodeoxyglucose positron emission tomography/computed tomography compared with conventional imaging procedures. J. Clin. Oncol. 2008, 26, 4746–4751. [Google Scholar] [CrossRef]
- Glaudemans, A.W.; de Vries, E.F.; Galli, F.; Dierckx, R.A.; Slart, R.H.; Signore, A. The use of 18F-FDG-PET/CT for diagnosis and treatment monitoring of inflammatory and infectious diseases. Clin. Dev. Immunol. 2013, 2013, 623036. [Google Scholar] [CrossRef] [Green Version]
- Albano, D.; Bertagna, F.; Bertoli, M.; Bosio, G.; Lucchini, S.; Motta, F.; Panarotto, M.B.; Peli, A.; Camoni, L.; Bengel, F.M.; et al. Incidental Findings Suggestive of COVID-19 in Asymptomatic Patients Undergoing Nuclear Medicine Procedures in a High-Prevalence Region. J. Nucl. Med. 2020, 61, 632–636. [Google Scholar] [CrossRef] [Green Version]
- Boulvard Chollet, X.L.E.; Romero Robles, L.G.; Garrastachu, P.; Cabrera Villegas, A.; Albornoz Almada, M.C.; Colletti, P.M.; Rubello, D.; Ramírez Lasanta, R.; Delgado Bolton, R.C. 18F-FDG PET/CT in Hodgkin Lymphoma With Unsuspected COVID-19. Clin. Nucl. Med. 2020, 45, 652–653. [Google Scholar] [CrossRef]
- Castanheira, J.; Mascarenhas Gaivão, A.; Mairos Teixeira, S.; Pereira, P.J.; Costa, D.C. Asymptomatic COVID-19 positive patient suspected on FDG-PET/CT. Nucl. Med. Commun. 2020, 41, 598–599. [Google Scholar] [CrossRef] [PubMed]
- Colandrea, M.; Gilardi, L.; Travaini, L.L.; Fracassi, S.L.V.; Funicelli, L.; Grana, C.M. 18F-FDG PET/CT in asymptomatic patients with COVID-19: The submerged iceberg surfaces. Jpn. J. Radiol. 2020, 38, 1007–1011. [Google Scholar] [CrossRef]
- Cosma, L.; Sollaku, S.; Frantellizzi, V.; De Vincentis, G. Early 18 F-FDG PET/CT in COVID-19. J. Med. Imaging Radiat. Oncol. 2020, 64, 671–673. [Google Scholar] [CrossRef]
- de Barry, O.; Cabral, D.; Kahn, J.E.; Vidal, F.; Carlier, R.Y.; El Hajjam, M. 18-FDG PSEUDOTUMORAL LESION WITH QUICK FLOWERING TO A TYPICAL LUNG CT COVID-19. Radiol. Case Rep. 2020, 15, 1813–1816. [Google Scholar] [CrossRef] [PubMed]
- Ferrando-Castagnetto, F.; Wakfie-Corieh, C.G.; García, A.M.B.; García-Esquinas, M.G.; Caro, R.M.C.; Delgado, J.L.C. Incidental and simultaneous finding of pulmonary thrombus and COVID-19 pneumonia in a cancer patient derived to 18F-FDG PET/CT. New pathophysiological insights from hybrid imaging. Radiol. Case Rep. 2020, 15, 1803–1805. [Google Scholar] [CrossRef] [PubMed]
- Habouzit, V.; Sanchez, A.; Dehbi, S.; Prevot, N.; Bonnefoy, P.B. Incidental Finding of COVID-19 Lung Infection in 18F-FDG PET/CT: What Should We Do? Clin. Nucl. Med. 2020, 45, 649–651. [Google Scholar] [CrossRef] [PubMed]
- López-Mora, D.A.; Fernández, A.; Duch, J.; Carrio, I. Follow-up 18F-FDG PET/CT in an oncological asymptomatic COVID-19 patient. Rev. Esp. Med. Nucl. Imagen Mol. 2020. [Google Scholar] [CrossRef]
- Mattoli, M.V.; Taralli, S.; Pennese, E.; D’Angelo, C.; Angrilli, F.; Villano, C. Atypical Presentation of COVID-19 Incidentally Detected at 18F-FDG PET/CT in an Asymptomatic Oncological Patient. Clin. Nucl. Med. 2020, 45, e383–e385. [Google Scholar] [CrossRef] [PubMed]
- Piciu, A.; Manole, S.; Piciu, D.; Dreve, T.; Roman, A. Asymptomatic COVID-19 cancer patients incidentally discovered during F18-FDG PET/CT monitoring. Med. Pharm. Rep. 2021, 94, 58–64. [Google Scholar] [PubMed]
- Scarlattei, M.; Baldari, G.; Silva, M.; Bola, S.; Sammartano, A.; Migliari, S.; Graziani, T.; Cidda, C.; Sverzellati, N.; Ruffini, L. Unknown SARS-CoV-2 pneumonia detected by PET/CT in patients with cancer. Tumori 2020, 106, 325–332. [Google Scholar] [CrossRef]
- Simand, C.; Bund, C.; Guffroy, B.; Chaban, V.; Herbrecht, R. Incidental Discovery of a COVID-19 Infection on a Reevaluation FDG PET/CT in a Patient Treated for Hodgkin Lymphoma. Clin. Nucl. Med. 2020, 45, 644–646. [Google Scholar] [CrossRef] [PubMed]
- Pillenahalli Maheshwarappa, R.; Graham, M.M. Asymptomatic COVID-19 Infection Detected on 18F-FDG PET/CT Scan Done for Multiple Myeloma. Clin. Nucl. Med. 2021, 46, e57–e58. [Google Scholar] [CrossRef]
- Martineau, P.; Kidane, B. FDG PET/CT Findings in an Asymptomatic Case of Confirmed COVID-19. Clin. Nucl. Med. 2020, 45, 647–648. [Google Scholar] [CrossRef] [PubMed]
- Krebs, S.; Petkovska, I.; Ho, A.L.; Ulaner, G.A. Laboratory-Proven Asymptomatic SARS-CoV-2 (COVID-19) Infection on 18F-FDG PET/CT. Clin. Nucl. Med. 2020, 45, 654–655. [Google Scholar] [CrossRef]
- Johnson, L.N.; Vesselle, H. COVID-19 in an asymptomatic patient undergoing FDG PET/CT. Radiol Case Rep. 2020, 15, 1809–1812. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Galougahi, M.; Yousefi-Koma, A.; Khalili, N.; Bakhshayeshkaram, M.; Haseli, S. Transient 18FDG-avid hilar lymph node on PET/CT imaging in asymptomatic COVID-19. ID Cases 2020, 22, e00981. [Google Scholar] [CrossRef] [PubMed]
- Tsikala Vafea, M.; Atalla, E.; Kalligeros, M.; Mylona, E.K.; Shehadeh, F.; Mylonakis, E. Chest CT findings in asymptomatic cases with COVID-19: A systematic review and meta-analysis. Clin. Radiol. 2020, 75, 876.e33–876.e39. [Google Scholar] [CrossRef] [PubMed]
- Beigelman-Aubry, C.; Godet, C.; Caumes, E. Lung infections: The radiologist’s perspective. Diagn. Interv. Imaging 2012, 93, 431–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayamajhi, S.J.; Mittal, B.R.; Maturu, V.N.; Agarwal, R.; Bal, A.; Dey, P.; Shukla, J.; Gupta, D. 18F-FDG and 18F-FLT PET/CT imaging in the characterization of mediastinal lymph nodes. Ann. Nucl. Med. 2016, 30, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Dutta, R.; Kannan, U.; Kumar, R.; Khilnani, G.C.; Gupta, S.D. Evaluation of mediastinal lymph nodes using F-FDG PET-CT scan and its histopathologic correlation. Ann. Thorac. Med. 2011, 6, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Semionov, A.; Rossi, A.; Perillo, M.; Sayegh, K.; Pressacco, J.; Kosiuk, J. Many Faces of Thoracic Histoplasmosis-Pictorial Essay. Can. Assoc. Radiol. J. 2019, 70, 273–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardanelli, F.; Cozzi, A.; Monfardini, L.; Bnà, C.; Foà, R.A.; Spinazzola, A.; Tresoldi, S.; Cariati, M.; Secchi, F.; Schiaffino, S. Association of mediastinal lymphadenopathy with COVID-19 prognosis. Lancet Infect. Dis. 2020, 20, 1230–1231. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients No./Sex/ Age (y) | Reference | Country | Clinical Disease | [18F]FDG PET/CT Indications | Extrapulmonary PET/CT Findings | The Pattern of PET/CT Finding in Pulmonary Regions |
|---|---|---|---|---|---|---|
| P1/M/70 | Boulvard Chollet XLE et al., 2021 [13] | Italy | Hodgkin Lymphoma | Staging | [18F]FDG-avid uptake in bilateral cervical lymphadenopathy, predominantly in the left side (SUVmax 9.0) | Tree-in-bud opacities and peripheral and subpleural GGOs in both lungs, corresponding to mild [18F]FDG uptake (SUVmax 2.4) |
| P2/F/80 | Habouzit V et al., 2020 [19] | France | Anal canal adenocarcinoma | Staging | Prominent [18F]FDG-avid tumor uptake in anal canal (SUVmax 12.8) | Subpleural patchy, rounded, and diffuse GGOs in right lung, with mildly diffuse [18F]FDG uptake (SUV max 2.4) |
| P3/F/69 | Pillenahalli Maheshwar- appa R et al., 2021 [25] | USA | Multiple myeloma | Follow-up | Uneven hot [18F]FDG uptake in right maxillary sinus, favored sinusitis | Prominent [18F]FDG-avid uptake of extensive GGOs in peripheral to subpleural region over bilateral lower lobes (SUVmax 12.0) |
| P4/M/87 | Krebs S et al., 2020 [27] | USA | Primary salivary duct carcinoma | Restaging | Prominent [18F]FDG-avid uptake in hepatic and colon metastases | Prominent [18F]FDG-avid uptake in multiple GGOs and patchy opacities, with intralobular septal thickening of lung in LUL and RLL |
| P5/M/59 | Mattoli MV et al., 2020 [21] | Italy | Diffuse B cell lymphoma | Therapeutic response | NR | Focally increasing [18F]FDG uptake with a consolidation surrounding a faint GGO in central RML (SUVmax 3.3) |
| P6/M/67 | Johnson LN et al., 2020 [28] | USA | Hereditary nonpolyposis colorectal cancer | Follow-up | Mild [18F]FDG uptake in the long segment of the small bowel at the mid-abdomen (SUVmax 4.7) and faint [18F]FDG uptake in lymph nodes at the lower abdomen (SUVmax 2.9) | Uneven [18F]FDG-avid uptake of GGOs in both lungs (SUVmax 9.5), mediastinal and hilar LNs (SUVmax 9.6) |
| P7/F/65 | Castanheira J et al., 2020 [14] | Portugal | Breast cancer | Follow-up | Recurrent breast cancer and bone marrow metastasis | Hot [18F]FDG uptake of a GGO in the RLL with interlobular thickening (SUVmax 8.0) and moderate increasing [18F]FDG uptake in ipsilateral hilar and subcarinal LN (SUVmax 4.0 to 5.0) |
| P8/M/54 | Colandrea M et al., 2020 [15] | Italy | Non-hodgkin lymphoma | Staging | Pathological increasing [18F]FDG uptake in right inguinal lymphadenopathy | Moderate-to-hot [18F]FDG uptake of GGOs in lower lobes of both lungs (SUV bw max 10.7); faint [18F]FDG uptake of focal consolidation in LUL (SUV bw max 3.9). Mediastinum and left subclavian LNs (SUV bw max 4.6) |
| P9/M/61 | Colandrea M et al., 2020 [15] | Italy | - | Characterization of unknow brain and lung LN lesion | NR | Mild-to-moderate [18F]FDG uptake including consolidation in RUL (SUV bw max 3.6), multiple GGOs in LLL (SUV bw max 4.9), mediastinal, carinal, and hilar LNs (SUV bw max 3.9) |
| P10/M/48 | Colandrea M et al., 2020 [15] | Italy | Lung cancer | Restating | Increased hot [18F]FDG uptake in retro-bronchial LNs (SUV bw max 9.8), favored recent radiotherapy related | Mild-to-moderate [18F]FDG uptake including consolidation in LUL (SUV bw max 3.3), multiple peripheral GGOs and septal thickening in LLL (SUV bw max 6.5) Mediastinal and left hilar LNs (SUV bw max 5.2) |
| P11/M/54 | Colandrea M et al., 2020 [15] | Italy | Melanoma | Follow-up | NR | Multiple small GGOs without corresponding [18F]FDG uptake in both lungs |
| P12/NR/NR | Colandrea M et al., 2020 [15] | Italy | Tongue cancer | Follow-up | NR | Increased [18F]FDG uptake in peripheral and parenchymal GGOs of both lower lobes (SUV bw max 6.3), focal consolidation in RUL (SUV bw max 6.8) and right hilar LNs (SUV bw max 5.9) |
| P13/F/56 | Albano D et al., 2020 [12] | Italy | Anal cancer | restaging | An inguinal metastatic nodule with corresponding [18F]FDG uptake | Mild [18F]FDG uptake of GGOs and consolidation in both lower lobes (SUVmax 3.6) |
| P14/M/77 | Albano D et al., 2020 [12] | Italy | Laryngeal cancer | Staging | Increased hot [18F]FDG uptake in right epiglottis and local cervical nodes | Faint [18F]FDG uptake of GGOs in both lungs (SUVmax 2.0) |
| P15/F/65 | Albano D et al., 2020 [12] | Italy | Ovarian cancer | Follow-up | No abnormal [18F]FDG uptake in primary site of ovarian malignancy | [18F]FDG-avid uptake of corresponding GGOs in both lungs (SUVmax 6.9) |
| P16/F/55 | Albano D et al., 2020 [12] | Italy | Hodgkin lymphoma | Therapeutic response | Increasing [18F]FDG uptake in the axillary nodes, suggestive of lymphoma nodule | [18F]FDG-avid uptake of corresponding GGOs in right lung (SUVmax 5.0) |
| P17/F/57 | Scarlattei M et al., 2020 [23] | Italy | Breast cancer | Restaging | [18F]FDG-avid tumor uptake in left breast (SUVmax 6.5) | Multiple mild-to-hot [18F]FDG uptake of GGOs in bilateral lower lobes (range of SUVmax 2.2 to 9.1), and moderate-to-hot [18F]FDG uptake in mediastinal, hilar, and carinal LNs (SUVmax 7.0) |
| P18/F/57 | Scarlattei M et al., 2020 [23] | Italy | - | Characterization of splenic lesion | No abnormal [18F]FDG uptake in splenic lesion | Several GGOs in both lungs with mild [18F]FDG uptake (SUVmax 4.6) and faint [18F]FDG uptake in bibasilar LNs (SUVmax 2.5) |
| P19/F/38 | Piciu A et al., 2021 [22] | Romania | Nasopharyngeal carcinoma | Therapeutic response | [18F]FDG-avid uptake in left supraclavicular lymphadenopathy | Faint [18F]FDG uptake of multiple GGOs in RML |
| P20/M/70 | Piciu A et al., 2021 [22] | Romania | Maxillary sinus carcinoma | Restaging | [18F]FDG-avid nodules in maxillary sinus | Hot [18F]FDG uptake of multiple GGOs in both lungs (SUV lbm max 6.8) |
| P21/F/64 | Piciu A et al., 2021 [22] | Romania | Follicular thyroid carcinoma | Follow-up | NR | A metastasis-associated nodule with minimally increased [18F]FDG uptake in peripheral RLL and without other lung alterations |
| P22/F/65 | Piciu A et al., 2021 [22] | Romania | Rectal cancer | Staging | [18F]FDG-avid uptake in rectal area, favored rectal malignant | Diffuse mild GGOs in both lungs (SUV lbm max 3.8) |
| P23/F/70 | Piciu A et al., 2021 [22] | Romania | Breast cancer | Follow-up | NR | Diffuse GGOs with crazy paving in both lungs with mild [18F]FDG uptake (SUV lbm max 3.7) |
| P24/F/27 | Karimi-Galougahi M et al., 2020 [29] | Iran | - | Characterization of unknow anosmia | NR | Right hilar LN (SUVmax 2.6) with mild [18F]FDG uptake, suspicious occult malignancy, then confirmation of a transient [18F]FDG-avid LN by scan 10 days later |
| P25/M/88 | Ferrando-Castagnetto F et al, 2020 [18] | Spain | Melanoma | Follow-up | Intense [18F]FDG-avid uptake in both left preauricular and bilateral cervical lymphadenopathy No changes in melanoma associated features | Mild [18F]FDG uptake of GGOs in both lungs and curvilinear lines in right lung (SUVmax 3.2); hot [18F]FDG uptake in mediastinal and bilateral hilar lymphadenopathy (largest size 9 mm, SUVmax 8.1) |
| P26/NR/NR | Cosma L et al., 2020 [16] | Italy | Colorectal cancer | Therapeutic response | NR | Multiple GGOs in right lung and a nodule in right interlobar region, which showed mild [18F]FDG uptake (SUVmax 2.4) |
| P27/M/68 | López-Mora DA et al., 2021 [20] | Spain | Urothelial carcinoma | Follow-up | No abnormal [18F]FDG uptake outside thoracic cavity | Multiple mild [18F]FDG uptake of GGOs in both lungs, then disappeared 3 months later |
| P28/M/67 | Martineau P, et al., 2020 [26] | Canada | - | Characterization of a suspicious lung nodule | No abnormal [18F]FDG uptake outside thoracic cavity | Focal increased [18F]FDG uptake of lung nodule (SUVmax 4.1), confirming adenocarcinoma by biopsy; moderate-to-hot [18F]FDG uptake of GGOs and consolidative opacities in both lungs (SUVmax from 5.0 to 7.2), also in mediastinal LNs, more likely reactive LNs by size evaluation |
| P29/F/27 | Simand C et al., 2020 [24] | France | Hodgkin lymphoma | Restaging | Increased [18F]FDG uptake in bone marrow | GGOs with consolidations in LLL (SUVmax 8.1) |
| P30/M/78 | de Barry O et al., 2020 [17] | France | - | Characterization of rheumatic polymyalgia | Increased [18F]FDG uptake of osteoarticular involvement in both shoulders | A GGO with consolidation in LUL with focal hot [18F]FDG uptake (SUVmax 5.4) |
| Pattern of Lung Lesion | Number of Lung Lesions | Number of Affected Lobes | Distribution of Affected Lobes | Location of Affected Lobes | Lung Involvement | Location of Thoracic LN Involvement | Degree of [18F]FDG Uptake | References and Images |
|---|---|---|---|---|---|---|---|---|
| Without lung lesion (n = 2) (P21, P24) | - | - | - | - | - | Hilar alone (n = 1) (P24) NR (n = 1) | LN: SUVmax 2.6 (n = 1) (P24) NR (n = 1) | [22]: Figure 4 (P21) [29]: Figure 1 (P24) |
| GGO alone (n = 13) (P2, P3, P6, P11, P14-20, P22, P27) | Multiple (n = 13) | 1 lobe (n = 2) (P2, P19) 2 lobes (n = 2) (P3, P17) 3 lobes (n = 1) (P4) 5 lobes (n = 4) (P11, P15, P20, P22) NR (n = 4) | PS (n = 1) (P6) SS (n = 4) (P2, P16-18) PS and SS (n = 1) (P3) NR (n = 7) | RML (n = 1) (P19) RLL (n = 2) (P2, P6) RLL and LLL (n = 2) (P3, P17) Right lung lobes (n = 1) (P16) All lung lobes (n = 4) (P11, P15, P20, P22) NR (n = 3) | Unilateral (n = 3) (P2, P16, P19) Bilateral (n = 10) (P3, P6, P11, P14, P15, P17 P18, P20, P22, P27) | No involvement (n = 2) (P2, P11) Hilar alone (n = 1) (P18) Mediastinal alone (n = 1) (P15) Mediastinal and hilar (n = 1) (P6) Mediastinal, hilar, and carinal (n = 1) (P17) NR (n = 7) | Lung lesion: No [18F]FDG uptake (n = 1) (P11) SUV max 2 to 12 (n = 8) (P2, P3, P6, P14-18) SUV lbm max 6.8 (n = 1) (P20) NR (n = 3) (P19, P20, P27) LN: SUVmax 2.5 to 9.6 (n = 3) (P6, P17, P18) NR (n = 10) | [12]: Figures 2, 4 and 6 (P14, P15, P16) [15]: Figure 3 (P11) [19,20,25,28]: Figure 1 (P2, P3, P6, P27) [22]: Figures 2, 3 and 5 (P19, P20, P22) [23]: Figure 2 and Supplementary Figure 3 (P17, P18) |
| GGO plus consolidation (n = 7) (P5, P8, P9, P12, P13, P28, P29) | Unique (n = 1) (P5) Multiple (n = 5) (P8, P12, P13, P28, P29) Mixed (n = 1) (P9) | 1 lobe (n = 1) (P5) 2 lobes (n = 3) (P9, P13) 3 lobes (n = 2) (P8, P12) 5 lobes (n = 1) (P28) | PS (n = 3) (P8, P12, P28) SS (n = 1) (P29) NR (n = 3) (P5, P9, P13) | RML (n = 1) (P5) RUL and LLL (n = 2) (P9, P29) RLL and LLL (n = 1) (P13) RUL, RLL, and LLL (n = 1) (P12) RLL and left lung lobes (n = 1) (P8) All lung lobes (n = 1) (P28) | Unilateral (n = 1) (P5) Bilateral (n = 6) (P8, P9, P12, P13, P28, P29) | Hilar alone (n = 1) (P12) Mediastinal and left subclavian (n = 1) (P8) Mediastinal, hilar, and carinal (n = 1) (P9) Mediastinal lymphadenopathy (n = 1) (P28) NR (n = 3) | Lung lesion: SUVmax 3.3 to 8.1 (n = 4) (P5, P13, P28, P29) SUV bw max 3.6 to 10.7 (n = 3) (P8, P9, 12) LN: SUV bw max 3.9 to 5.9 (n = 3) (P8, P9, P12) NR (n = 4) | [12,21,26]: Figure 1 (P5, P13, P28) [15]: Figures 1 and 4 (P8, P9, P12) [24]: Figures 1 and 2 (P29) |
| GGO plus consolidation and septal thickening (n = 1) (P10) | Mixed | 2 lobes | PS | LUL and LLL | Unilateral | Mediastinal and hilar | Lung lesion: SUV bw max 3.3 (consolidation); 6.5 (GGOs) LN: SUV bw max 5.2 | [15]: Figure 2 |
| GGO plus consolidation and curvilinear line (n = 1) (P30) | Unique | 4 lobes | NR | Right lung lobes and LUL | Bilateral | NR | Lung lesion: SUVmax 5.4 | [17]: Figure 1 |
| GGO plus interlobular thickening (n = 1) (P7) | Unique | 1 lobe | PS | RLL | Unilateral | Ipsilateral hilar and subcarinal | Lung lesion: SUVmax 8 LN: SUVmax 5 | [14]: Figure 1 |
| GGO plus intralobular thickening (n = 1) (P4) | Multiple | 2 lobes | NR | RLL and LUL | Bilateral | NR | NR | [27]: Figure 1 |
| GGO plus tree-in-bud opacities (n = 1) (P1) | Multiple | NR | PS and SS | NR | Bilateral | NR | Lung lesion: SUVmax 2.4 | [13]: Figure 1 |
| GGO plus crazy paving (n = 1) (P23) | Unique | 5 lobes | NR | All lung lobes | Bilateral | NR | Lung lesion: SUV lbm max 3.7 | [22]: Figure 6 |
| GGO plus a nodule (n = 1) (P26) | Mixed | 3 lobes | PS | Right lung lobes | Unilateral | NR | Lung lesion: SUVmax 2.4 (GGOs) | [16]: Figures 1 and 2 |
| GGO plus curvilinear line, thrombus, and lung infiltrates (n = 1) (P25) | Multiple | NR | SS and CS | NR | Bilateral | Mediastinal and hilar | Lung lesion: SUVmax 3.2 LN: SUVmax 8.1 (mediastinal) | [18]: Figure 1 |
| Reference | Facility | Country | Patients No. (Reference Table 1) | Patient Management | Hospital Infection Control |
|---|---|---|---|---|---|
| Boulvard Chollet XLE et al., 2021 [13] | University Hospital San Pedro and Centre | Italy | P1 | Immediately isolated, RT-PCR testing, and started COVID-19 treatment with paracetamol and hydroxychloroquine sulphate (dolquine), plus omeprazole, enoxaparin, furosemide, azithromycin, and tranxilium | NR |
| Mattoli MV et al., 2020 [21] | NR | Italy | P5 | Chest X-ray for reevaluation, then RT-PCR testing immediately and home quarantine | NR |
| Colandrea M et al., 2020 [15] | European Institute of Oncology IRCCS | Italy | P8, 9, 10, 11, and 12 | Laboratory COVID-19 testing immediately in dedicated COVID-19 medical units (P8 and P9), another center (P10), or hospitals (P11 and P12), and home quarantine for all patients | NR |
| Albano D et al., 2020 [12] | Spedali Civili Brescia | Italy | P13, 14, 15, and 16 | All patients: RT-PCR testing immediately P13 and P14: postponed oncological therapy, referred to dedicated COVID-19 medical unit, and started COVID-19 treatment with hydroxychloroquine plus ritonavir-lopinavir | NR |
| Scarlattei M et al., 2020 [23] | University Hospital of Parma | Italy | P17 and P18 | Immediate home quarantine, and retrospectively confirmed by serology test | NR |
| Cosma L et al., 2020 [16] | NR | Italy | P26 | RT-PCR was performed at the time of symptom development | NR |
| Habouzit V et al., 2020 [19] | CHU Saint-Etienne | France | P2 | RT-PCR testing immediately | Screened the COVID-19 infection risk for every patient before and upon entering the unit, cleaned the imaging equipment after every using, cancel nonurgent investigations when pervious patients with confirmed or suspected COVID-19, notified the suspected COVID-19 and their contacted person should be self-monitoring |
| Simand C et al., 2020 [24] | University Hospital of Strasbourg | France | P29 | FDG PET/CT scanning again at ten days after the time of first imaging | NR |
| de Barry O et al., 2020 [17] | Ambroise ParéTeaching Hospital | France | P30 | PCR test was performed at time of symptoms developed | NR |
| Piciu A et al., 2021 [22] | NR | Romania | P19, 20, 21, 22, and 23 | PCR testing immediately, postponed oncological therapy, referred to dedicated COVID-19 medical units and started the COVID-19 treatment with azithromycin plus chloroquine | NR |
| Ferrando-Castagnetto F et al, 2020 [18] | Hospital de Clínicas Dr. Manuel Quintela | Spain | P25 | RT-PCR testing immediately and started COVID-19 treatment with ceftriaxone, azithromycin, and methylprednisolone for five days in hospital, then prolonged subcutaneous treatment with enoxaparin at home | NR |
| López-Mora DA et al., 2021 [20] | Hospital de la Santa Creu i Sant Pau | Spain | P27 | Home quarantine, RT-PCR was performed at the time of symptom development, and received incomplete COVID-19 treatment with hydroxychloroquine and oxygen-therapy due to voluntary abandonment | NR |
| Castanheira J et al., 2020 [14] | Champalimaud Centre for the Unknown | Portugal | P7 | RT-PCR testing immediately and home quarantine | Separated the employees into the rotational teams, screened the COVID-19 infection risk for every patient before and upon entering the facility, canceled the radiopharmaceutical imaging investigation when previous patients were confirmed or suspected to have COVID-19 |
| Karimi-Galougahi M et al., 2020 [29] | NR | Iran | P24 | RT-PCR testing immediately | NR |
| Martineau P, et al., 2020 [26] | Health Sciences Centre Winnipeg | Canada | P28 | PCR testing immediately | NR |
| Pillenahalli Maheshwar- appa R et al., 2021 [25] | University of Iowa Hospitals and Clinics | USA | P3 | RT-PCR testing immediately and home quarantine | NR |
| Krebs S et al., 2020 [27] | Memorial Sloan Kettering Cancer Center | USA | P4 | RT-PCR testing immediately and home quarantine | NR |
| Johnson LN et al., 2020 [28] | NR | USA | P6 | RT-PCR testing immediately and home quarantine | If it had received patients with confirmed or suspected COVID-19, the imaging room would be closed for one hour and cleaned by a high-efficiency particulate air (HEPA filter). Employees exposed to COVID-19 were required to self-screen daily and return to work when they were asymptomatic or had a lack of relevant symptoms |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, T.-C.; Chang, C.-C.; Chan, H.-P.; Huang, Y.-F.; Chen, Y.-M.A.; Chuang, K.-P.; Lee, C.-H.; Yuan, C.-H.; Deng, Y.-Z.; Yang, M.-H.; et al. Pulmonary Findings of [18F]FDG PET/CT Images on Asymptomatic COVID-19 Patients. Pathogens 2021, 10, 839. https://doi.org/10.3390/pathogens10070839
Ho T-C, Chang C-C, Chan H-P, Huang Y-F, Chen Y-MA, Chuang K-P, Lee C-H, Yuan C-H, Deng Y-Z, Yang M-H, et al. Pulmonary Findings of [18F]FDG PET/CT Images on Asymptomatic COVID-19 Patients. Pathogens. 2021; 10(7):839. https://doi.org/10.3390/pathogens10070839
Chicago/Turabian StyleHo, Tzu-Chuan, Chin-Chuan Chang, Hung-Pin Chan, Ying-Fong Huang, Yi-Ming Arthur Chen, Kuo-Pin Chuang, Che-Hsin Lee, Cheng-Hui Yuan, Yu-Zhen Deng, Ming-Hui Yang, and et al. 2021. "Pulmonary Findings of [18F]FDG PET/CT Images on Asymptomatic COVID-19 Patients" Pathogens 10, no. 7: 839. https://doi.org/10.3390/pathogens10070839
APA StyleHo, T.-C., Chang, C.-C., Chan, H.-P., Huang, Y.-F., Chen, Y.-M. A., Chuang, K.-P., Lee, C.-H., Yuan, C.-H., Deng, Y.-Z., Yang, M.-H., & Tyan, Y.-C. (2021). Pulmonary Findings of [18F]FDG PET/CT Images on Asymptomatic COVID-19 Patients. Pathogens, 10(7), 839. https://doi.org/10.3390/pathogens10070839