
Tracking the Epidemiologic Shifts in Hepatitis A Sero-Prevalence Using Age Stratification: A Cross-Sectional Study at Jordan University Hospital

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Ethical Considerations
2.4. Paper-Based Questionnaire
2.5. Source of Drinking Water
2.6. Patterns of Fast Food Consumption among the Study Participants
2.7. Detection of HAV IgG Using ELISA
2.8. Statistical Analysis
3. Results
3.1. General Features of the Study Population
3.2. Assessment of the Overall HAV Sero-Prevalence
3.3. Variables Correlated with a Higher Sero-Prevalence of HAV in Participants Aged 10 or Less
3.4. Variables Correlated with a Higher Sero-Prevalence of HAV in Participants Aged 15 or Less
3.5. Variables Correlated with a Higher Sero-Prevalence of HAV in Participants Aged 30 or Less
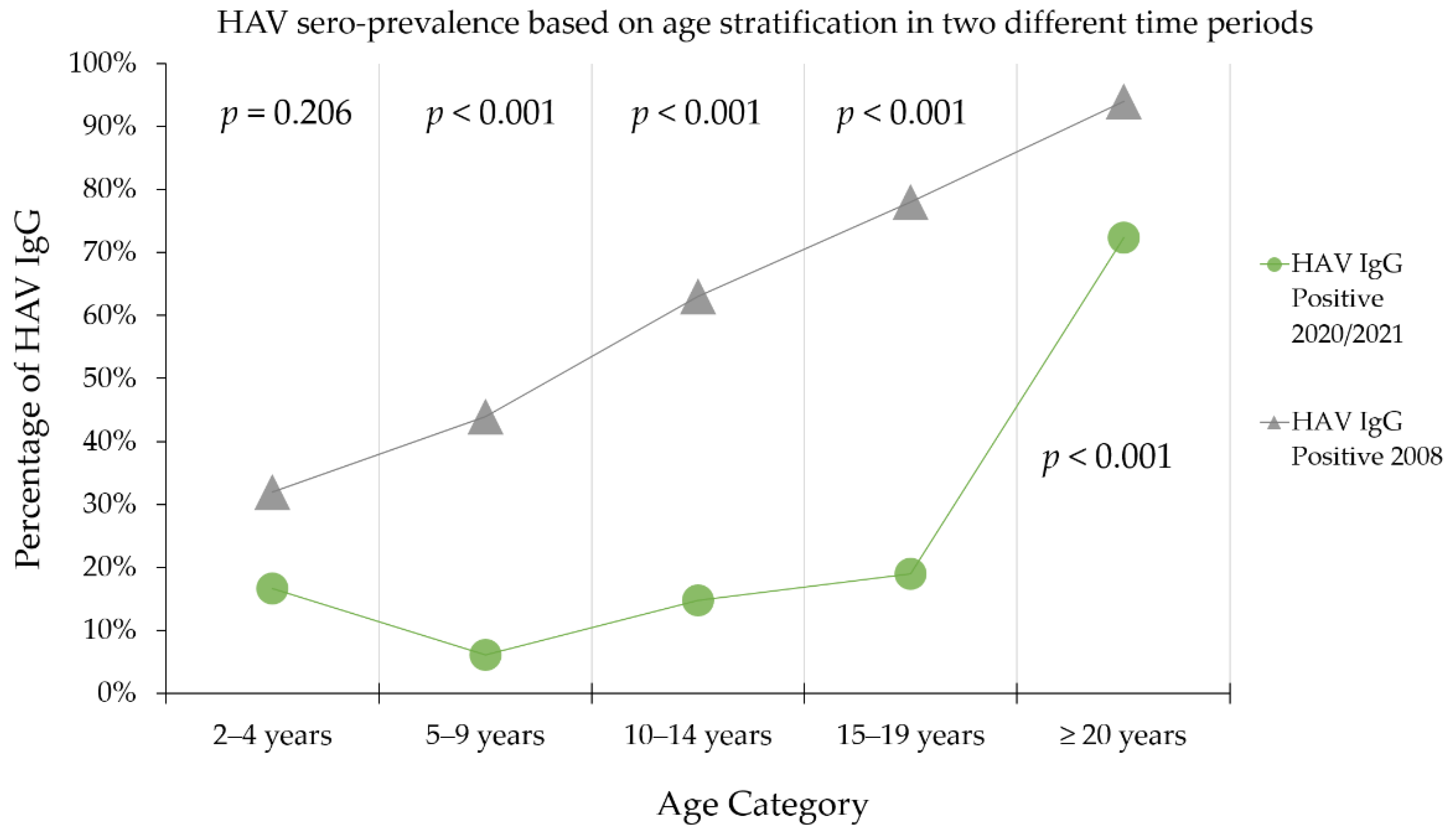
3.6. Demonstration of an Epidemiologic Shift in HAV Sero-Prevalence in Jordan between 2008 and 2021
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Hepatitis A. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-a (accessed on 7 June 2021).
- Franco, E. Hepatitis A: Epidemiology and prevention in developing countries. World J. Hepatol. 2012, 4, 68–73. [Google Scholar] [CrossRef]
- Jeong, S.-H.; Lee, H.-S. Hepatitis A: Clinical manifestations and management. Intervirology 2010, 53, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, J.A. Hepatitis A: Old and new. Clin. Microbiol. Rev. 2001, 14, 38–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, C.N.; Margolis, H.S. Worldwide epidemiology of hepatitis A virus infection. J. Hepatol. 1993, 18, S11–S14. [Google Scholar] [CrossRef]
- Hu, X.; Collier, M.G.; Xu, F. Hepatitis A outbreaks in developed countries: Detection, control, and prevention. Foodborne Pathog. Dis. 2020, 17, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Frank, C.; Walter, J.; Muehlen, M.; Jansen, A.; Van Treeck, U.; Hauri, A.M.; Zoellner, I.; Schreier, E.; Hamouda, O.; Stark, K. Large outbreak of hepatitis A in tourists staying at a hotel in Hurghada, Egypt, 2004—Orange juice implicated. Wkly. Releases (1997–2007) 2005, 10, 2720. [Google Scholar] [CrossRef] [PubMed]
- Lanini, S.; Minosse, C.; Vairo, F.; Garbuglia, A.; Di Bari, V.; Agresta, A.; Rezza, G.; Puro, V.; Pendenza, A.; Loffredo, M.R.; et al. A large ongoing outbreak of hepatitis A predominantly affecting young males in Lazio, Italy; August 2016–March 2017. PLoS ONE 2017, 12, e0185428. [Google Scholar] [CrossRef] [Green Version]
- Gall, A.M.; Mariñas, B.J.; Lu, Y.; Shisler, J.L. Waterborne viruses: A barrier to safe drinking water. PLoS Pathog. 2015, 11, e1004867. [Google Scholar] [CrossRef]
- Pintó, R.M.; Costafreda, M.I.; Bosch, A. Risk assessment in shellfish-borne outbreaks of hepatitis A. Appl. Environ. Microbiol. 2009, 75, 7350–7355. [Google Scholar] [CrossRef] [Green Version]
- Di Cola, G.; Fantilli, A.C.; Pisano, M.B.; Ré, V.E. Foodborne transmission of hepatitis A and hepatitis E viruses: A literature review. Int. J. Food Microbiol. 2020, 338, 108986. [Google Scholar] [CrossRef]
- Manka, P.; Verheyen, J.; Gerken, G.; Canbay, A. Liver failure due to acute viral hepatitis (A-E). Visc. Med. 2016, 32, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L. Hepatitis A vaccination. Hum. Vaccines Immunother. 2020, 16, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, K.; Koopman, J.S. Declining hepatitis A seroprevalence: A global review and analysis. Epidemiol. Infect. 2004, 132, 1005–1022. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.P.; Murphy, T.V. Hepatitis A: The changing epidemiology of hepatitis A. Clin. Liver Dis. 2013, 2, 227–230. [Google Scholar] [CrossRef]
- Jacobsen, K. Globalization and the changing epidemiology of hepatitis a virus. Cold Spring Harb. Perspect. Med. 2018, 8, a031716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gossner, C.M.; Severi, E.; Danielsson, N.; Hutin, Y.; Coulombier, D. Changing hepatitis A epidemiology in the European Union: New challenges and opportunities. Eurosurveillance 2015, 20, 21101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanafiah, K.M.; Jacobsen, K.H.; Wiersma, S.T. Challenges to mapping the health risk of hepatitis A virus infection. Int. J. Health Geogr. 2011, 10, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). The Immunological Basis for Immunization Series: Module 18—Hepatitis A Update 2019. Available online: https://www.who.int/publications/i/item/97892516327 (accessed on 12 July 2021).
- Chakravarti, A.; Bharara, T. Epidemiology of Hepatitis A: Past and Current Trends; IntechOpen: London, UK, 2020. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO position paper on hepatitis A vaccines—June 2012. Weekly Epidemiological Record. Rel. Epidémiol. Hebdomad. 2012, 87, 261–276. [Google Scholar]
- Lemon, S.M.; Ott, J.J.; Van Damme, P.; Shouval, D. Type A viral hepatitis: A summary and update on the molecular virology, epidemiology, pathogenesis and prevention. J. Hepatol. 2018, 68, 167–184. [Google Scholar] [CrossRef] [Green Version]
- Ntouva, A.; Sibal, B.; Balogun, K.; Mandal, S.; Harding, N. Hepatitis A in primary care: Working in partnership for diagnosis, management, and prevention of outbreaks. Br. J. Gen. Pr. 2019, 69, 521–522. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.P.; Weng, M.K.; Hofmeister, M.G.; Moore, K.L.; Doshani, M.; Kamili, S.; Koneru, A.; Haber, P.; Hagan, L.; Romero, J.R.; et al. Prevention of hepatitis a virus infection in the United States: Recommendations of the Advisory Committee on Immunization Practices, 2020. MMWR. Recomm. Rep. 2020, 69, 1–38. [Google Scholar] [CrossRef]
- Battikhi, M.N.G.; Battikhi, E.G. The seroepidemiology of Hepatitis A virus in Amman, Jordan. New Microbiol. 2004, 27, 215–220. [Google Scholar] [PubMed]
- Hayajneh, W.A.; Balbeesi, A.; Faouri, S. Hepatitis A virus age-specific sero-prevalence and risk factors among Jordanian children. J. Med. Virol. 2015, 87, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Hayajneh, W.A.; Daniels, V.J.; James, C.K.; Kanıbir, M.N.; Pilsbury, M.; Marks, M.; Goveia, M.G.; Elbasha, E.H.; Dasbach, E.; Acosta, C.J. Public health impact and cost effectiveness of routine childhood vaccination for hepatitis a in Jordan: A dynamic model approach. BMC Infect. Dis. 2018, 18, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toukan, A.U.; Sharaiha, Z.K.; Abu-El-Rob, O.A.; Hmoud, M.K.; Dahbour, S.; Abu-Hassan, H.; Yacoub, S.M.; Margolis, H.S. The seroepidemiology of hepatitis A virus infection in Jordan. Trop. Gastroenterol. 1988, 9, 76–79. [Google Scholar] [PubMed]
- Sharara, S.L.; Kanj, S.S. War and infectious diseases: Challenges of the Syrian Civil War. PLoS Pathog. 2014, 10, e1004438. [Google Scholar] [CrossRef] [Green Version]
- Koroglu, M.; Jacobsen, K.H.; Demiray, T.; Ozbek, A.; Erkorkmaz, U.; Altindis, M. Socioeconomic indicators are strong predictors of hepatitis A seroprevalence rates in the Middle East and North Africa. J. Infect. Public Health 2017, 10, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Sacy, R.G.; Abu-Elyazeed, R.; Khoriati, A.; Gerbaka, B.J.; Baasiri, G.; Haddad, M. Hepatitis a in lebanon: A changing epidemiological pattern. Am. J. Trop. Med. Hyg. 2005, 73, 453–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turky, A.M.; Akram, W.; Al-Naaimi, A.S.; Omer, A.R.; Rawi, J.R.A. Analysis of acute viral hepatitis (A and E) in Iraq. Glob. J. Health Sci. 2011, 3, 70. [Google Scholar] [CrossRef]
- Yassin, K.; Awad, R.; Tebi, A.; Queder, A.; Laaser, U.; Yassin, K.; Awad, R.; Tebi, A.; Queder, A.; Laaser, U. The epidemiology of hepatitis A infection in Palestine: A universal vaccination programme is not yet needed. Epidemiol. Infect. 2001, 127, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Antaki, N.; Kebbewar, M.K. Hepatitis A seroprevalence rate in Syria. Trop. Dr. 2000, 30, 99–101. [Google Scholar] [CrossRef]
- Salama, I.; Samy, S.; Shaaban, F.; Hassanin, A.; Ismail, L.A. Seroprevalence of hepatitis A among children of different socioeconomic status in Cairo. East. Mediterr. Health J. 2007, 13, 1256–1264. [Google Scholar] [CrossRef]
- Melhem, N.M.; Talhouk, R.; Rachidi, H.; Ramia, S. Hepatitis A virus in the Middle East and North Africa region: A new challenge. J. Viral Hepat. 2014, 21, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Khoury, S.; Graczyk, T.; Burnham, G.; Goldman, L. Drinking water system trearment and contamination in Shatila Refugee Camp in Beirut, Lebanon. East. Mediterr. Health J. 2016, 22, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Habib, R.R.; Ziadee, M.; Younes, E.A.; El Asmar, K.; Jawad, M. The association between living conditions and health among Syrian refugee children in informal tented settlements in Lebanon. J. Public Health 2019, 42, e323–e333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Rousan, T.; Schwabkey, Z.; Jirmanus, L.; Nelson, B.D. Health needs and priorities of Syrian refugees in camps and urban settings in Jordan: Perspectives of refugees and health care providers. East. Mediterr. Health J. 2018, 24, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Itani, T.; Jacobsen, K.H.; Nguyen, T.; Wiktor, S.Z. A new method for imputing country-level estimates of hepatitis A virus endemicity levels in the Eastern Mediterranean region. Vaccine 2014, 32, 6067–6074. [Google Scholar] [CrossRef]
- Gassowski, M.; Michaelis, K.; Wenzel, J.J.; Faber, M.; Figoni, J.; Mouna, L.; Friesema, I.H.; Vennema, H.; Avellon, A.; Varela, C.; et al. Two concurrent outbreaks of hepatitis A highlight the risk of infection for non-immune travellers to Morocco, January to June 2018. Eurosurveillance 2018, 23, 1800329. [Google Scholar] [CrossRef] [PubMed]
- Couturier, E.; Roque-Afonso, A.M.; Letort, M.J.; Dussaix, E.; Vaillant, V.; de Valk, H. Cluster of cases of hepatitis A with a travel history to Egypt, September-November 2008, France. Eurosurveillance 2009, 14, 19094. [Google Scholar] [CrossRef] [PubMed]
- Beauté, J.; Westrell, T.; Schmid, D.; Müller, L.; Epstein, J.; Kontio, M.; Couturier, E.; Faber, M.; Mellou, K.; Borg, M.-L.; et al. Travel-associated hepatitis A in Europe, 2009 to 2015. Eurosurveillance 2018, 23, 1700583. [Google Scholar] [CrossRef]
- Sane, J.; De Sousa, R.; Van Pelt, W.; Petrignani, M.; Verhoef, L.; Koopmans, M. Risk of hepatitis a decreased among Dutch travelers to endemic regions in 2003 to 2011. J. Travel Med. 2015, 22, 208–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobsen, K.H.; Koopman, J.S. The effects of socioeconomic development on worldwide hepatitis A virus seroprevalence patterns. Int. J. Epidemiol. 2005, 34, 600–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unicef. Water, Sanitation and Hygiene. Access to Safe Water and Sanitation for Every Child. Available online: https://www.unicef.org/jordan/water-sanitation-and-hygiene (accessed on 17 July 2021).
- USAID. Water Resources and Environment. Available online: https://www.usaid.gov/jordan/water-and-wastewater-infrastructure (accessed on 17 July 2021).



{kind=link}
{kind=link}
{kind=link}
| Variable | Number | Percentage | |
|---|---|---|---|
| Age in years (mean, SD 1) | 23.7 (19.6) | ||
| Number of household inhabitants (mean, SD) | 5.4 (1.8) | ||
| Sex | Male | 148 | 41.1% |
| Female | 212 | 58.9% | |
| Nationality | Jordanian | 353 | 98.1% |
| Non-Jordanian | 7 | 1.9% | |
| Region 2 | North | 19 | 5.3% |
| Central | 332 | 92.2% | |
| South | 9 | 2.5% | |
| Monthly income of household | Less than 500 JOD 3 | 118 | 32.8% |
| 500–1000 JOD | 156 | 43.3% | |
| More than 1000 JOD | 86 | 23.9% | |
| Educational level | High school or less | 294 | 81.7% |
| Undergraduate study | 54 | 15.0% | |
| Postgraduate study | 12 | 3.3% | |
| Drinking water source | Mineral water | 5 | 1.4% |
| Municipal water filtered at home | 124 | 34.4% | |
| Filtered by a local provider | 199 | 55.3% | |
| Unfiltered municipal water | 27 | 7.5% | |
| Stream or well water | 5 | 1.4% | |
| Variable | Category | HAV IgG Positive | HAV IgG Negative | p-Value 5 | ||
|---|---|---|---|---|---|---|
| N 4 | % | N | % | |||
| Sex | Male | 7 | 9.1% | 70 | 90.9% | 0.232 |
| Female | 12 | 15.4% | 66 | 84.6% | ||
| Region 1 | North | 2 | 25.0% | 6 | 75.0% | 0.019 |
| Central | 14 | 10.0% | 126 | 90.0% | ||
| South | 3 | 42.9% | 4 | 57.1% | ||
| Monthly income | Less than 500 JOD 3 | 5 | 10.6% | 42 | 89.4% | 0.457 |
| 500–1000 JOD | 11 | 15.7% | 59 | 84.3% | ||
| More than 1000 JOD | 3 | 7.9% | 35 | 92.1% | ||
| Drinking water source 2 | Filtered municipal water | 5 | 9.8% | 46 | 90.2% | 0.036 |
| Unfiltered municipal water | 4 | 33.3% | 8 | 66.7% | ||
| Age | 1–5 years | 4 | 13.3% | 26 | 86.7% | 0.115 |
| 6–10 years | 4 | 6.0% | 63 | 94.0% | ||
| 11–15 years | 11 | 19.0% | 47 | 81.0% | ||
| Variable | Category | HAV IgG Positive | HAV IgG Negative | p-Value 5 | ||
|---|---|---|---|---|---|---|
| N 4 | % | N | % | |||
| Sex | Male | 17 | 15.7% | 91 | 84.3% | 0.096 |
| Female | 40 | 24.1% | 126 | 75.9% | ||
| Region 1 | North | 6 | 37.5% | 10 | 62.5% | 0.042 |
| Central | 47 | 18.9% | 202 | 81.1% | ||
| South | 4 | 44.4% | 5 | 55.6% | ||
| Monthly income | Less than 500 JOD 3 | 14 | 17.9% | 64 | 82.1% | 0.594 |
| 500–1000 JOD | 30 | 23.4% | 98 | 76.6% | ||
| More than 1000 JOD | 13 | 19.1% | 55 | 80.9% | ||
| Drinking water source 2 | Filtered municipal water | 15 | 16.3% | 77 | 83.7% | 0.093 |
| Unfiltered municipal water | 6 | 33.3% | 12 | 66.7% | ||
| Age | 3–5 years | 4 | 13.3% | 26 | 86.7% | <0.001 |
| 6–10 years | 4 | 6.0% | 63 | 94.0% | ||
| 11–15 years | 11 | 19.0% | 47 | 81.0% | ||
| 16–20 years | 17 | 20.5% | 66 | 79.5% | ||
| 21–25 years | 9 | 40.9% | 13 | 59.1% | ||
| 26–30 years | 12 | 85.7% | 2 | 14.3% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kareem, N.; Al-Salahat, K.; Bakri, F.G.; Rayyan, Y.; Mahafzah, A.; Sallam, M. Tracking the Epidemiologic Shifts in Hepatitis A Sero-Prevalence Using Age Stratification: A Cross-Sectional Study at Jordan University Hospital. Pathogens 2021, 10, 1081. https://doi.org/10.3390/pathogens10091081
Kareem N, Al-Salahat K, Bakri FG, Rayyan Y, Mahafzah A, Sallam M. Tracking the Epidemiologic Shifts in Hepatitis A Sero-Prevalence Using Age Stratification: A Cross-Sectional Study at Jordan University Hospital. Pathogens. 2021; 10(9):1081. https://doi.org/10.3390/pathogens10091081
Chicago/Turabian StyleKareem, Nariman, Khaled Al-Salahat, Faris G. Bakri, Yaser Rayyan, Azmi Mahafzah, and Malik Sallam. 2021. "Tracking the Epidemiologic Shifts in Hepatitis A Sero-Prevalence Using Age Stratification: A Cross-Sectional Study at Jordan University Hospital" Pathogens 10, no. 9: 1081. https://doi.org/10.3390/pathogens10091081