
Acute-phase Serum Cytokine Levels and Correlation with Clinical Outcomes in Children and Adults with Primary and Secondary Dengue Virus Infection in Myanmar between 2017 and 2019

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Samples
2.2. Ethical Approval
2.3. Serology and NS1 Ag Detection
2.4. Quantification of DENV Genomic RNA and Serotyping
2.5. Identification and Quantification of Cytokines
2.6. Statistical Analysis
3. Results
3.1. Clinical Presentation of the Study Population
3.2. Serological Analyses
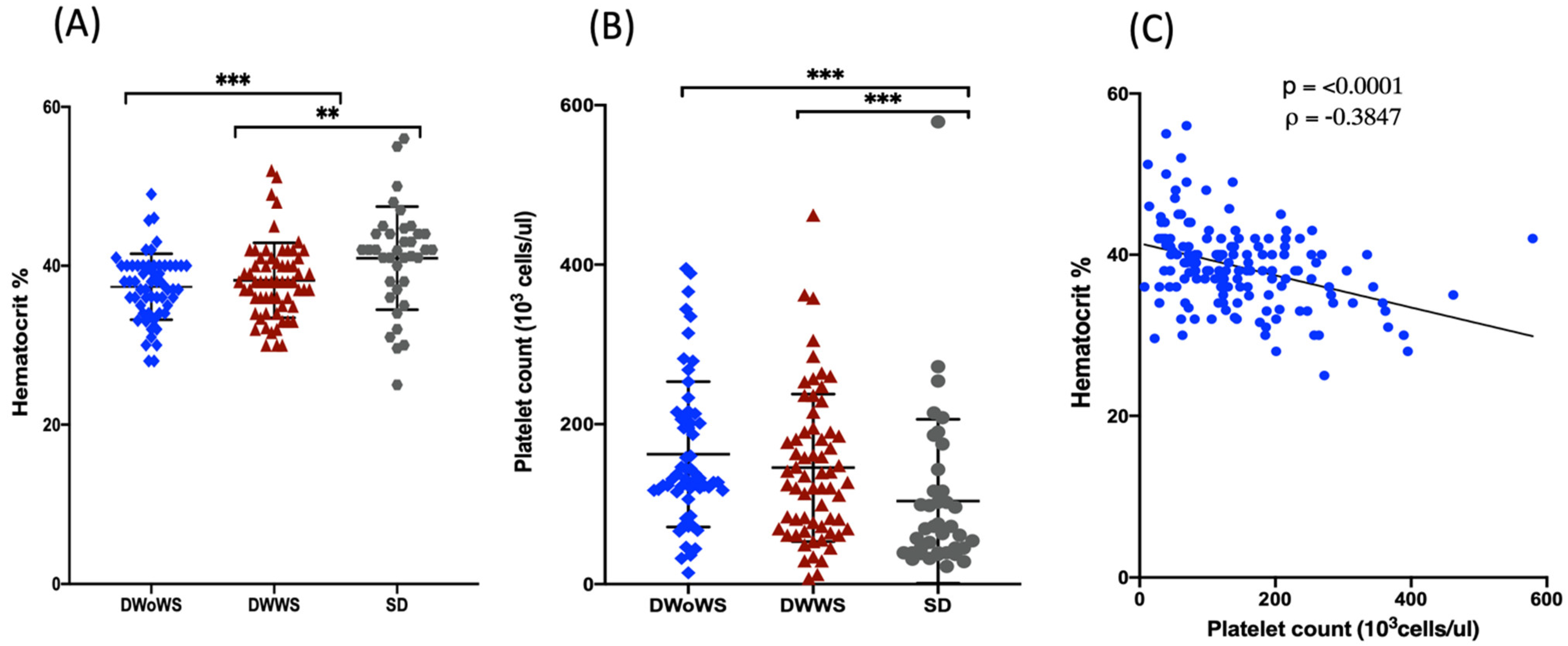
3.3. Virus Serotypes and Viremia
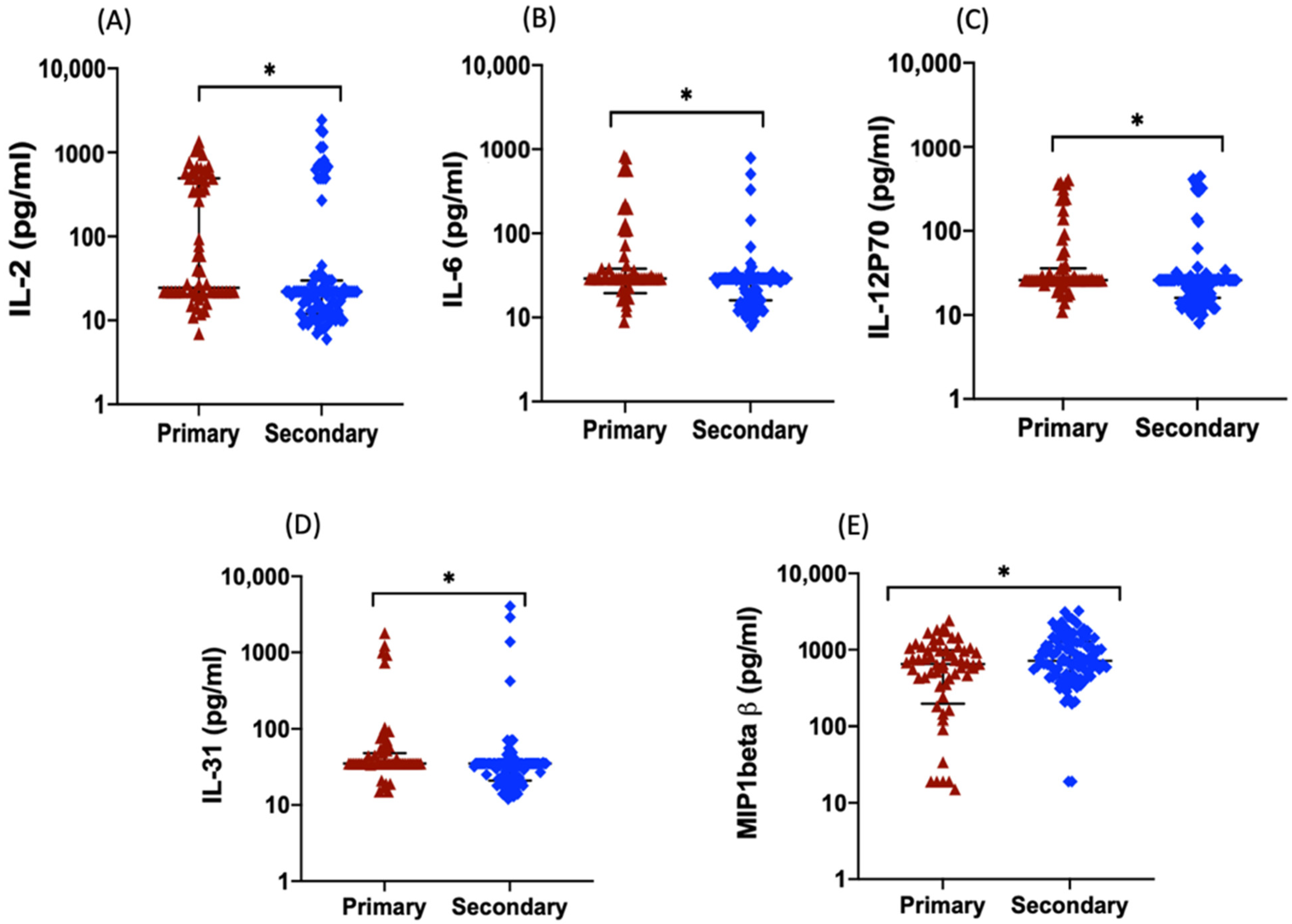
3.4. Serum Levels of Inflammatory Cytokines, Chemokines, and Growth Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brady, O.J.; Gething, P.W.; Bhatt, S.; Messina, J.P.; Brownstein, J.S.; Hoen, A.G.; Moyes, C.L.; Farlow, A.W.; Scott, T.W.; Hay, S.I. Refining the Global Spatial Limits of Dengue Virus Transmission by Evidence-Based Consensus. PLoS Negl. Trop. Dis. 2012, 6, e1760. [Google Scholar] [CrossRef] [PubMed]
- National Strategic Plan, Released by Ministry of Health and Sports, Myanmar. National Strategic Plan for Dengue Prevention and Control Vector Borne Disease Control Programme Ministry of Health and Sports the Union of Republic of Myanmar. 2020. Available online: https://www.mindbank.info/item/7249 (accessed on 1 May 2022).
- Oo, P.M.; Wai, K.T.; Harries, A.D.; Shewade, H.D.; Oo, T.; Thi, A.; Lin, Z. The Burden of Dengue, Source Reduction Measures, and Serotype Patterns in Myanmar, 2011 to 2015-R2. Trop. Med. Health 2017, 45, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Dengue Guidelines for Diagnosis, Treatment Prevention, and Control: New Edition; World Health Organization: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/handle/10665/44188 (accessed on 19 May 2020).
- Raj Kumar Patro, A.; Mohanty, S.; Prusty, B.K.; Singh, D.K.; Gaikwad, S.; Saswat, T.; Chattopadhyay, S.; Das, B.K.; Tripathy, R.; Ravindran, B. Cytokine Signature Associated with Disease Severity in Dengue. Viruses 2019, 11, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Cruz Hernández, S.I.; Puerta-Guardo, H.N.; Aguilar, H.F.; Mateos, S.G.; Martinez, I.L.; Ortiz-Navarrete, V.; Ludert, J.E.; del Angel, R.M. Primary Dengue Virus Infections Induce Differential Cytokine Production in Mexican Patients. Mem. Inst. Oswaldo Cruz 2016, 111, 161–167. [Google Scholar] [CrossRef]
- Bozza, F.A.; Cruz, O.G.; Zagne, S.M.O.; Azeredo, E.L.; Nogueira, R.M.R.; Assis, E.F.; Bozza, P.T.; Kubelka, C.F. Multiplex Cytokine Profile from Dengue Patients: MIP-1beta and IFN-Gamma as Predictive Factors for Severity. BMC Infect. Dis. 2008, 8, 86. [Google Scholar] [CrossRef] [Green Version]
- Bundo, K.; Igarashi, A. Antibody-capture ELISA for detection of immunoglobulin M in sera from Japanese encephalitis and dengue hemorrhagic fever patients. J. Virol. Methods 1985, 11, 15–22. [Google Scholar] [CrossRef]
- Inoue, S.; Alonzo, M.T.G.; Kurosawa, Y.; Mapua, C.A.; Reyes, J.D.; Dimaano, E.M.; Alera, M.T.P.; Saito, M.; Oishi, K.; Hasebe, F.; et al. Evaluation of a dengue IgG indirect enzyme-linked immunosorbent assay and a Japanese encephalitis IgG indirect enzyme-linked immunosorbent assay for diagnosis of secondary dengue virus infection. Vector Borne Zoonotic Dis. 2020, 10, 143–150. [Google Scholar] [CrossRef]
- Tun, M.M.N.; Kyaw, A.K.; Nabeshima, T.; Soe, A.M.; Nwe, K.M.; Htet, K.K.K.; Aung, T.H.; Htwe, T.T.; Aung, T.; Myaing, S.S.; et al. Detection of Genotype-1 of Dengue Virus Serotype 3 for the First Time and Complete Genome Analysis of Dengue Viruses during the 2018 Epidemic in Mandalay, Upper Myanmar. PLoS ONE 2021, 16, e0251314. [Google Scholar] [CrossRef]
- Ngwe Tun, M.M.; Muthugala, R.; Nabeshima, T.; Rajamanthri, L.; Jayawardana, D.; Attanayake, S.; Soe, A.M.; Prakash Dumre, S.; Ando, T.; Hayasaka, D.; et al. Unusual, Neurological and Severe Dengue Manifestations during the Outbreak in Sri Lanka, 2017. J. Clin. Virol. 2020, 125, 104304. [Google Scholar] [CrossRef]
- Ito, M.; Takasaki, T.; Yamada, K.I.; Nerome, R.; Tajima, S.; Kurane, I. Development and Evaluation of Fluorogenic TaqMan Reverse Transcriptase PCR Assays for Detection of Dengue Virus Types 1 to 4. J. Clin. Microbiol. 2004, 42, 5935–5937. [Google Scholar] [CrossRef] [Green Version]
- Ngwe Tun, M.M.; Thuy Nguyen, T.T.; Ando, T.; Dumre, S.P.; Soe, A.M.; Buerano, C.C.; Nguyen, M.T.; Nhan Le, N.T.; Pham, V.Q.; Nguyen, T.H.; et al. Clinical, Virological, and Cytokine Profiles of Children Infected with Dengue Virus during the Outbreak in Southern Vietnam in 2017. Am. J. Trop. Med. Hyg. 2020, 102, 1217. [Google Scholar] [CrossRef]
- Tramontini, F.; de Sousa, G.; Baimukanova, G.; Lanteri, C.; Keating, S.M.; Ferreira, F.M.; Heitman, J. Serum from Dengue Virus-Infected Patients with and without Plasma Leakage Differentially Affects Endothelial Cells Barrier Function in Vitro. PLoS ONE 2017, 12, e0178820. [Google Scholar]
- Soe, A.M.; Myat, M.; Tun, N.; Nabeshima, T.; Myat, T.W.; Htun, M.M.; Lin, H.; Hom, N.S.; Inoue, S.; Nwe, K.M.; et al. Emergence of a Novel Dengue Virus 3 (DENV-3) Genotype-I Coincident with Increased DENV-3 Cases in Yangon, Myanmar Between 2017 and 2019. Viruses 2021, 13, 1152. [Google Scholar] [CrossRef]
- Sehrawat, P.; Biswas, A.; Kumar, P.; Singla, P.; Wig, N.; Dar, L.; Sood, R. Role of Cytokines as Molecular Marker of Dengue Severity. Mediterr. J. Hematol. Infect. Dis. 2018, 10, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Gowri Sankar, S.; Alwin Prem Anand, A. Cytokine IP-10 and GM-CSF Are Prognostic Biomarkers for Severity in Secondary Dengue Infection. Hum. Immunol. 2021, 82, 438–445. [Google Scholar] [CrossRef]
- Kyaw, A.K.; Ngwe Tun, M.M.; Moi, M.L.; Nabeshima, T.; Soe, K.T.; Thwe, S.M.; Myint, A.A.; Maung, K.T.T.; Aung, W.; Hayasaka, D.; et al. Clinical, Virological and Epidemiological Characterization of Dengue Outbreak in Myanmar, 2015. Epidemiol. Infect. 2017, 145, 1886–1897. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Bisht, P.; Bhattacharya, S.; Guchhait, P. Role of Platelet Cytokines in Dengue Virus Infection. Front. Cell. Infect. Microbiol. 2020, 10, 549. [Google Scholar] [CrossRef]
- Sirisena, N.; Noordeen, F.; Fernando, L.K. NS 1 Lasts Longer than the Dengue Virus Nucleic Acid in the Clinically Suspected Patients with Dengue Fever and Dengue Haemorrhagic Fever. VirusDisease 2017, 28, 341–344. [Google Scholar] [CrossRef]
- Libraty, D.H.; Young, P.R.; Pickering, D.; Endy, T.P.; Kalayanarooj, S.; Green, S.; Vaughn, D.W.; Nisalak, A.; Ennis, F.A.; Rothman, A.L. High Circulating Levels of the Dengue Virus Nonstructural Protein NS1 Early in Dengue Illness Correlate with the Development of Dengue Hemorrhagic Fever. J. Infect. Dis. 2002, 186, 1165–1168. [Google Scholar] [CrossRef]
- Moi, M.L.; Omatsu, T.; Tajima, S.; Lim, C.K.; Kotaki, A.; Ikeda, M.; Harada, F.; Ito, M.; Saijo, M.; Kurane, I.; et al. Detection of Dengue Virus Nonstructural Protein 1 (NS1) by Using ELISA as a Useful Laboratory Diagnostic Method for Dengue Virus Infection of International Travelers. J. Travel Med. 2013, 20, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Jayathilaka, D.; Gomes, L.; Jeewandara, C.; Jayarathna, G.S.B.; Herath, D.; Perera, P.A.; Fernando, S.; Wijewickrama, A.; Hardman, C.S.; Ogg, G.S.; et al. Secondary Dengue Infection. Nat. Commun. 2018, 9, 5242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duyen, H.T.L.; Ngoc, T.V.; Ha, D.T.; Hang, V.T.T.; Kieu, N.T.T.; Young, P.R.; Farrar, J.J.; Simmons, C.P.; Wolbers, M.; Wills, B.A. Kinetics of Plasma Viremia and Soluble Nonstructural Protein 1 Concentrations in Dengue: Differential Effects According to Serotype and Immune Status. J. Infect. Dis. 2011, 203, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Cuellar, C.; Lovera, D.; Galeano, F.; Gatti, L.; Arbo, A. Non-Structural Protein 1 (NS1) of Dengue Virus Detection Correlates with Severity in Primary but Not in Secondary Dengue Infection. J. Clin. Virol. 2020, 124, 104259. [Google Scholar] [CrossRef] [PubMed]
- De Melo Iani, F.C.; Caldas, S.; Duarte, M.M.; Cury, A.L.F.; Cecílio, A.B.; Costa, P.A.C.; Antonelli, L.R.; Gollob, K.J. Dengue Patients with Early Hemorrhagic Manifestations Lose Coordinate Expression of the Anti-Inflammatory Cytokine Il-10 with the Inflammatory Cytokines IL-6 and IL-8. Am. J. Trop. Med. Hyg. 2016, 95, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Puc, I.; Ho, T.; Yen, K.; Vats, A.; Tsai, J.; Chen, P.; Chien, Y.; Lo, Y.; Perng, G.C. Cytokine Signature of Dengue Patients at Different Severity of the Disease. Int. J. Mol. Sci. 2021, 22, 2879. [Google Scholar] [CrossRef]
- Inyoo, S.; Suttitheptumrong, A.; Pattanakitsakul, S.N. Synergistic Effect of TNF-α and Dengue Virus Infection on Adhesion Molecule Reorganization in Human Endothelial Cells. Jpn. J. Infect. Dis. 2017, 70, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Branche, E.; Tang, W.W.; Viramontes, K.M.; Young, M.P.; Sheets, N.; Joo, Y.; Nguyen, A.V.T.; Shresta, S. Synergism between the Tyrosine Kinase Inhibitor Sunitinib and Anti-TNF Antibody Protects against Lethal Dengue Infection. Antiviral Res. 2018, 158, 1–7. [Google Scholar] [CrossRef]
- Enhancement, A.; Storm, C.; Assolini, P.; Tomiotto-pellissier, F. Highlights for dengue immunopathogenesis: Antibody-dependent enhancement, cytokine storm, and beyond. J. Interferon Cytokine Res. 2018, 38, 69–80. [Google Scholar] [CrossRef]
- Senaratne, T.; Carr, J.; Noordeen, F. Elevation in Liver Enzymes Is Associated with Increased IL-2 and Predicts Severe Outcomes in Clinically Apparent Dengue Virus Infection. Cytokine 2016, 83, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Meena, A.A.; Murugesan, A.; Sopnajothi, S.; Yong, Y.K.; Ganesh, P.S.; Vimali, I.J.; Vignesh, R.; Elanchezhiyan, M.; Kannan, M.; Dash, A.P.; et al. Increase of Plasma TNF-α Is Associated with Decreased Levels of Blood Platelets in Clinical Dengue Infection. Viral Immunol. 2020, 33, 54–60. [Google Scholar] [CrossRef]
- Srikiatkhachorn, A.; Mathew, A.; Rothman, A.L. Immune-mediated cytokine storm and its role in severe dengue. In Seminars in Immunopathology; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- Masood, K.I.; Jamil, B.; Rahim, M.; Islam, M.; Farhan, M.; Hasan, Z. Role of TNF α, IL-6 and CXCL10 in Dengue Disease Severity. Iran. J. Microbiol. 2018, 10, 202–207. [Google Scholar]
- Hottz, E.D.; Medeiros-de-Moraes, I.M.; Vieira-de-Abreu, A.; de Assis, E.F.; Vals-de-Souza, R.; Castro-Faria-Neto, H.C.; Weyrich, A.S.; Zimmerman, G.A.; Bozza, F.A.; Bozza, P.T. Platelet Activation and Apoptosis Modulate Monocyte Inflammatory Responses in Dengue. J. Immunol. 2014, 193, 1864–1872. [Google Scholar] [CrossRef] [Green Version]
- Tsai, T.T.; Chuang, Y.J.; Lin, Y.S.; Wan, S.W.; Chen, C.L.; Lin, C.F. An Emerging Role for the Anti-Inflammatory Cytokine Interleukin-10 in Dengue Virus Infection. J. Biomed. Sci. 2013, 20, 40. [Google Scholar] [CrossRef] [Green Version]
- Shen, P.; Fillatreau, S. Antibody-Independent Functions of B Cells: A Focus on Cytokines. Nat. Rev. Immunol. 2015, 15, 441–451. [Google Scholar] [CrossRef]
- Kumar, Y.; Liang, C.; Bo, Z.; Rajapakse, J.C.; Ooi, E.E.; Tannenbaum, S.R. Serum Proteome and Cytokine Analysis in a Longitudinal Cohort of Adults with Primary Dengue Infection Reveals Predictive Markers of DHF. PLoS Negl. Trop. Dis. 2012, 6, e1887. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; MacDougald, O.A. Stem Cell Factor: The Bridge between Bone Marrow Adipocytes and Hematopoietic Cells. Haematologica 2019, 104, 1689–1691. [Google Scholar] [CrossRef]
- Her, Z.; Kam, Y.; Gan, V.C.; Lee, B.; Thein, T.; Tan, J.J.L.; Platform, S.I.; Lee, L.K. Severity of Plasma Leakage Is Associated with High Levels of Interferon γ—Inducible Protein 10, Hepatocyte Growth Factor, Matrix Metalloproteinase 2 (MMP-2), and MMP-9 During Dengue Virus Infection. J. Infect. Dis. 2017, 215, 42–51. [Google Scholar] [CrossRef]
- Wang, W.H.; Lin, C.Y.; Chang, K.; Urbina, A.N.; Assavalapsakul, W.; Thitithanyanont, A.; Lu, P.L.; Chen, Y.H.; Wang, S.F. A Clinical and Epidemiological Survey of the Largest Dengue Outbreak in Southern Taiwan in 2015. Int. J. Infect. Dis. 2019, 88, 88–99. [Google Scholar] [CrossRef] [Green Version]
- Butthep, P.; Chunhakan, S.; Yoksan, S.; Tangnararatchakit, K. Alteration of Cytokines and Chemokines During Febrile Episodes Associated with Endothelial Cell Damage and Plasma Leakage in Dengue Hemorrhagic Fever. Pediatric Infect. Dis. J. 2012, 31, 232–238. [Google Scholar] [CrossRef]
- Varghese, A.; Thomas, T.; Oommen, S.; Mathew, A.; Philip, T. Assay of Proinflannatory Cytokines (IL-6, IFN γ, TNFα) and Its Correlation with Disease Severity in Dengue Fever. Int. J. Contemp. Med. Res. 2019, 6, 6–9. [Google Scholar] [CrossRef]
- Thakur, P.; Chakravarti, A.; Aggarwal, S.; Uppal, B. Elevated Levels of Vascular Endothelial Growth Factor in Adults with Severe Dengue Infection. VirusDisease 2016, 27, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Kou, Z.; Zhang, F.; Yao, X.; Liu, S.; Ma, J.; Zhou, Y.; Zhao, W.; Tang, X.; Jin, X. Both Viremia and Cytokine Levels Associate with the Lack of Severe Disease in Secondary Dengue 1 Infection among Adult Chinese Patients. PLoS ONE 2010, 5, e15631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Azeredo, E.L.; Monteiro, R.Q.; Pinto, L.M. Thrombocytopenia in Dengue: Interrelationship between Virus and the Imbalance between Coagulation and Fibrinolysis and Inflammatory Mediators. Mediat. Inflamm. 2015, 2015, 313842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adikari, T.N.; Gomes, L.; Wickramasinghe, N.; Salimi, M.; Wijesiriwardana, N.; Kamaladasa, A.; Shyamali, N.L.A. Dengue NS1 Antigen Contributes to Disease Severity by Inducing Interleukin (IL)-10 by Monocytes. Clin. Exp. Immunol. 2016, 184, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Huang, X.; Hong, W.; Qiu, S.; Wang, J.; Yu, L.; Zeng, Y.; Tan, X.; Zhang, F. Slow Resolution of Inflammation in Severe Adult Dengue Patients. BMC Infect. Dis. 2016, 16, 291. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DWoWS (n = 64) | DWWS (n = 64) | SD (n = 39) | Total (n = 167) | |
|---|---|---|---|---|
| Male | 37 | 45 | 24 | 106 |
| Female | 27 | 19 | 15 | 61 |
| Primary infection | 23 | 34 | 7 | 64 |
| Secondary infection | 41 | 30 | 32 | 103 |
| Age: <1 year | 0 | 1 | 0 | 1 |
| 1–5 years | 13 | 16 | 2 | 31 |
| 6–12 years | 30 | 37 | 34 | 101 |
| 13–18 years | 11 | 7 | 3 | 21 |
| >19 years | 10 | 3 | 0 | 13 |
| DENV RNA-positive | 32 | 33 | 18 | 83 |
| DENV-1 | 10 | 13 | 7 | 30 |
| DENV-3 | 14 | 12 | 7 | 33 |
| DENV-4 | 8 | 8 | 4 | 20 |
| DENV NS1 Ag-positive (RDT) | 64 | 64 | 39 | 167 |
| IgM positive | 50 | 48 | 33 | 131 |
| IgG positive | 41 | 31 | 33 | 105 |
| Cytokines | Control vs. DWoWS | Control vs. DWWS | Control vs. SD | DWoWS vs. DWWS | DWoWS vs. SD | DWWS vs. SD |
|---|---|---|---|---|---|---|
| CCL5 | <0.001 | <0.001 | <0.001 | 0.044 | 0.205 | 0.393 |
| IL-15 | 0.775 | 0.211 | 0.669 | 0.036 | 0.788 | 0.065 |
| SCF | 0.003 | <0.001 | <0.001 | 0.027 | 0.311 | 0.265 |
| PDGF-BB | 0.171 | 0.308 | 0.017 | 0.447 | 0.165 | 0.028 |
| IL-10 | <0.001 | 0.005 | 0.002 | 0.703 | 0.014 | 0.261 |
| TNF-⍺ | 0.079 | 0.143 | 0.042 | 0.642 | 0.07 | 0.231 |
| IL1β | 0.001 | 0.002 | 0.003 | 0.76 | 0.277 | 0.312 |
| IL-5 | 0.009 | 0.004 | 0.007 | 0.108 | 0.884 | 0.051 |
| IP10 (CXCL10) | <0.001 | <0.001 | <0.001 | 0.125 | 0.86 | 0.188 |
| IL-7 | 0.006 | 0.001 | 0.001 | 0.055 | 0.434 | 0.239 |
| IL-8 (CXCL8) | <0.001 | <0.001 | <0.001 | 0.836 | 0.439 | 0.223 |
| PIGF1 | 0.001 | <0.001 | <0.001 | 0.133 | 0.577 | 0.418 |
| IL-13 | 0.049 | 0.049 | 0.412 | 0.297 | 0.608 | 0.259 |
| IL-17A | 0.027 | 0.018 | 0.11 | 0.527 | 0.535 | 0.292 |
| MIP-1β | 0.002 | 0.001 | 0.002 | 0.461 | 0.938 | 0.512 |
| CCL2 | 0.001 | 0.001 | 0.004 | 0.858 | 0.401 | 0.444 |
| VEGFD | 0.004 | 0.004 | 0.004 | 0.658 | 0.556 | 0.244 |
| NGFβ | 0.012 | <0.001 | <0.001 | 0.066 | 0.05 | 0.883 |
| EGF | 0.033 | 0.014 | 0.019 | 0.204 | 0.841 | 0.329 |
| IL1⍺ | 0.001 | <0.001 | <0.001 | 0.70 | 0.718 | 0.292 |
| IL-23 | 0.01 | 0.002 | 0.002 | 0.082 | 0.392 | 0.310 |
| FGF2 | 0.007 | 0.001 | 0.002 | 0.071 | 0.826 | 0.113 |
| Cytokine | Spearman’s Rank Correlation | p-Value |
|---|---|---|
| Correlation with platelet count | ||
| IL-2 | −0.019 | 0.017 |
| IL-6 | −0.063 | 0.039 |
| TNF-⍺ | −0.208 | 0.008 |
| VEGF-D | −0.177 | 0.025 |
| Correlation with NS1 Ag levels | ||
| IL-1⍺ | 0.162 | 0.038 |
| SCF | 0.190 | 0.015 |
| CCL5 | 0.176 | 0.024 |
| IFN-⍺ | 0.336 | <0.0001 |
| IL-22 | −0.212 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nwe, K.M.; Ngwe Tun, M.M.; Myat, T.W.; Sheng Ng, C.F.; Htun, M.M.; Lin, H.; Hom, N.S.; Soe, A.M.; Elong Ngono, A.; Hamano, S.; et al. Acute-phase Serum Cytokine Levels and Correlation with Clinical Outcomes in Children and Adults with Primary and Secondary Dengue Virus Infection in Myanmar between 2017 and 2019. Pathogens 2022, 11, 558. https://doi.org/10.3390/pathogens11050558
Nwe KM, Ngwe Tun MM, Myat TW, Sheng Ng CF, Htun MM, Lin H, Hom NS, Soe AM, Elong Ngono A, Hamano S, et al. Acute-phase Serum Cytokine Levels and Correlation with Clinical Outcomes in Children and Adults with Primary and Secondary Dengue Virus Infection in Myanmar between 2017 and 2019. Pathogens. 2022; 11(5):558. https://doi.org/10.3390/pathogens11050558
Chicago/Turabian StyleNwe, Khine Mya, Mya Myat Ngwe Tun, Theingi Win Myat, Chris Fook Sheng Ng, Moh Moh Htun, Htin Lin, Nang Sarm Hom, Aung Min Soe, Annie Elong Ngono, Shinjiro Hamano, and et al. 2022. "Acute-phase Serum Cytokine Levels and Correlation with Clinical Outcomes in Children and Adults with Primary and Secondary Dengue Virus Infection in Myanmar between 2017 and 2019" Pathogens 11, no. 5: 558. https://doi.org/10.3390/pathogens11050558
APA StyleNwe, K. M., Ngwe Tun, M. M., Myat, T. W., Sheng Ng, C. F., Htun, M. M., Lin, H., Hom, N. S., Soe, A. M., Elong Ngono, A., Hamano, S., Morita, K., Thant, K. Z., Shresta, S., Thu, H. M., & Moi, M. L. (2022). Acute-phase Serum Cytokine Levels and Correlation with Clinical Outcomes in Children and Adults with Primary and Secondary Dengue Virus Infection in Myanmar between 2017 and 2019. Pathogens, 11(5), 558. https://doi.org/10.3390/pathogens11050558