
Interleukin-6 and Its Soluble Receptor Complex in Intensive Care Unit COVID-19 Patients: An Analysis of Second Wave Patients

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef]
- Utrero-Rico, A.; Ruiz-Hornillos, J.; González-Cuadrado, C.; Rita, C.G.; Almoguera, B.; Minguez, P.; Herrero-González, A.; Fernández-Ruiz, M.; Carretero, O.; Taracido-Fernández, J.C.; et al. IL-6–based mortality prediction model for COVID-19: Validation and update in multicenter and second wave cohorts. J. Allergy Clin. Immunol. 2021, 147, 1652–1661. [Google Scholar] [CrossRef] [PubMed]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in Covid-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Paces, J.; Strizova, Z.; Smrz, D.; Cerny, J. COVID-19 and the Immune System. Physiol. Res. 2020, 69, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.-W.; Kok, K.-H.; Zhu, Z.; Chu, H.; To, K.K.-W.; Yuan, S.; Yuen, K.-Y. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg. Microbes Infect. 2020, 9, 221–236. [Google Scholar] [CrossRef]
- Dong, X.; Cao, Y.-Y.; Lu, X.-X.; Zhang, J.-J.; Du, H.; Yan, Y.-Q.; Akdis, C.A.; Gao, Y.-D. Eleven faces of coronavirus disease 2019. Allergy 2020, 75, 1699–1709. [Google Scholar] [CrossRef]
- Rizzo, P.; Vieceli Dalla Sega, F.; Fortini, F.; Marracino, L.; Rapezzi, C.; Ferrari, R. COVID-19 in the heart and the lungs: Could we “Notch” the inflammatory storm? Basic Res. Cardiol. 2020, 115, 30–37. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus infections and immune responses. J. Med. Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg. Microbes Infect. 2020, 9, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Liu, J.; Zhang, D.; Xu, Z.; Ji, J.; Wen, C. Cytokine Storm in COVID-19: The Current Evidence and Treatment Strategies. Front. Immunol. 2020, 11, 1708. [Google Scholar] [CrossRef]
- Gadient, R.A.; Patterson, P.H. Leukemia Inhibitory Factor, Interleukin 6, and Other Cytokines Using the GP130 Transducing Receptor: Roles in Inflammation and Injury. Stem Cells 1999, 17, 127–137. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef]
- Chen, L.; Liu, H.G.; Liu, W.; Liu, J.; Liu, K.; Shang, J.; Deng, Y.; Wei, S. Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, 203–208. [Google Scholar]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Tan, M.; Liu, Y.; Zhou, R.; Deng, X.; Li, F.; Liang, K.; Shi, Y. Immunopathological characteristics of coronavirus disease 2019 cases in Guangzhou, China. Immunology 2020, 160, 261–268. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Chang, Z.; Yang, W.; Wang, Q.; Liao, G. Clinical significance of serum hs-CRP, IL-6, and PCT in diagnosis and prognosis of patients with COVID-19. Drugs Clin. 2020, 35, 417–420. [Google Scholar]
- Li, G.; Li, L.; He, M.; Lin, H.; Ke, P.; Zhong, Z.; Yin, S.; Yang, K.; Ma, J. Value of various inflammatory markers combined with lymphocyte subsets on clinical diagnosis of different clinical types of COVID-19. J ChongMed. Univ. 2020, 45, 971–975. [Google Scholar]
- Zhang, C.; Wu, Z.; Li, J.-W.; Zhao, H.; Wang, G.Q. Cytokine Release Syndrome in Severe COVID-19: Interleukin-6 Receptor Antagonist Tocilizumab may be the Key to Reduce Mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef] [PubMed]
- Scheller, J.; Rose-John, S. Interleukin-6 and its receptor: From bench to bedside. Med. Microbiol. Immunol. 2006, 195, 173–183. [Google Scholar] [CrossRef]
- Weissenbach, J.; Chernajovsky, Y.; Zeevi, M.; Shulman, L.; Soreq, H.; Nir, U.; Wallach, D.; Perricaudet, M.; Tiollais, P.; Revel, M. Two interferon mRNAs in human fibroblasts: In vitro translation and Escherichia coli cloning studies. Proc. Natl. Acad. Sci. USA 1980, 77, 7152–7156. [Google Scholar] [CrossRef]
- Papanicolaou, D.A.; Wilder, R.L.; Manolagas, S.C.; Chrousos, G.P. The Pathophysiologic Roles of Interleukin-6 in Human Disease. Ann. Intern. Med. 1998, 128, 127–137. [Google Scholar] [CrossRef]
- Sutherland, A.M.; Walley, K.R.; Manocha, S.; Russell, J.A. The Association of Interleukin 6 Haplotype Clades With Mortality in Critically Ill Adults. Arch. Intern. Med. 2005, 165, 75–82. [Google Scholar] [CrossRef]
- Jones, S.A.; Jenkins, B.J. Recent insights into targeting the IL-6 cytokine family in inflammatory diseases and cancer. Nat. Rev. Immunol. 2018, 18, 773–789. [Google Scholar] [CrossRef]
- Hunter, C.A.; Jones, S.A. IL-6 as a keystone cytokine in health and disease. Nat. Immunol. 2017, 16, 448–457. [Google Scholar] [CrossRef]
- Yamasaki, K.; Taga, T.; Hirata, Y.; Yawata, H.; Kawanishi, Y.; Seed, B.; Taniguchi, T.; Hirano, T.; Kishimoto, T. Cloning and expression of the human interleukin-6 (BSF-2/IFN beta 2) receptor. Science 1988, 241, 825–828. [Google Scholar] [CrossRef]
- Baran, P.; Hansen, S.; Waetzig, G.H.; Akbarzadeh, M.; Lamertz, L.; Huber, H.J.; Ahmadian, M.R.; Moll, J.M.; Scheller, J. The balance of interleukin (IL)-6, IL-6·soluble IL-6 receptor (sIL-6R), and IL-6·sIL-6R·sgp130 complexes allows simultaneous classic and trans-signaling. J. Biol. Chem. 2018, 293, 6762–6775. [Google Scholar] [CrossRef] [PubMed]
- Briso, E.M.; Dienz, O.; Rincon, M. Cutting Edge: Soluble IL-6R Is Produced by IL-6R Ectodomain Shedding in Activated CD4 T Cells. J. Immunol. 2008, 180, 7102–7106. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I.L.; Erta, M.; Lim, S.L.; Frausto, R.; May, U.; Rose-John, S.; Scheller, J.; Hidalgo, J. Trans-Signaling Is a Dominant Mechanism for the Pathogenic Actions of Interleukin-6 in the Brain. J. Neurosci. 2014, 34, 2503–2513. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.A. Directing Transition from Innate to Acquired Immunity: Defining a Role for IL-6. J. Immunol. 2005, 175, 3463–3468. [Google Scholar] [CrossRef]
- Cacciapaglia, G.; Cot, C.; Sannino, F. Second wave COVID-19 pandemics in Europe: A temporal playbook. Sci. Rep. 2020, 10, 15514. [Google Scholar] [CrossRef]
- Bontempi, E. The europe second wave of COVID-19 infection and the Italy “strange” situation. Environ. Res. 2021, 193, 110476. [Google Scholar] [CrossRef]
- Le Gall, J.-R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Ely, E.W.; Truman, B.; Shintani, A.; Thomason, J.W.; Wheeler, A.P.; Gordon, S.; Francis, J.; Speroff, T.; Gautam, S.; Margolin, R. Monitoring sedation status over time in ICU patients: Reliability and validity of the Richmond Agita-tion-Sedation Scale (RASS). JAMA 2003, 289, 2983–2991. [Google Scholar] [CrossRef]
- Servillo, G.; Vargas, M.; Pastore, A.; Procino, A.; Iannuzzi, M.; Capuano, A.; Memoli, A.; Riccio, E.; Memoli, B. Immunomodulatory effect of continuous veno-venous hemofiltration during sepsis: Preliminary data. Biomed. Res. Int. 2013, 2013, 108951. [Google Scholar] [CrossRef]
- Di Spigna, G.; Cernia, D.S.; Vargas, M.; Buonavolontà, L.; Servillo, G.; Postiglione, L. Drastically elevated levels of Interleukin-6 and its soluble receptor complex in COVID-19 patients with acute respiratory distress. Clin. Med. Investig. 2020, 5, 1–4. [Google Scholar] [CrossRef]
- Kuswardhani, R.T.; Henrina, J.; Pranata, R.; Lim, M.A.; Lawrensia, S.; Suastika, K. Charlson comorbidity index and a composite of poor outcomes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Sabaka, P.; Koščálová, A.; Straka, I.; Hodosy, J.; Lipták, R.; Kmotorková, B.; Kachlíková, M.; Kušnírová, A. Role of interleukin 6 as a predictive factor for a severe course of Covid-19: Retrospective data analysis of patients from a long-term care facility during Covid-19 outbreak. BMC Infect. Dis. 2021, 21, 308. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | N = 104 |
|---|---|
| Age (years) | 68.72 ± 18.32 |
| ICU-LOS (days) | 11.51 ± 7.51 |
| Charlson comorbidity index (points) | 4.42 ± 3.34 |
| SAPS II (points) | 33.66 ± 14.51 |
| RASS (points) | −1.3 ± 2.1 |
| Male (%) | 68 (65.38%) |
| Diabetes (%) | 24 (23.12%) |
| Hypertension (%) | 66 (63.46%) |
| Chronic kidney disease (%) | 22 (21.15%) |
| Death (%) | 48 (46.15%) |
| Patients | Survivors | Non-Survivors | p-Value | |
|---|---|---|---|---|
| Age (years) | 60.32 ± 15.12 | 72.51 ± 11.34 | n.s. | |
| Sex (%) | F | 17 (18.7%) | 19 (9.8%) | p = 0.543 |
| M | 43 (42.2%) | 25 (30.4%) | n.s. | |
| Length of stay (days) | 10.36 ± 6.21 | 11.42 ± 8.19 | p = 0.299 | |
| Charlson comorbidity index (points) | 2.36 ± 3.81 | 8.49 ± 2.93 | n.s. | |
| SAPS II (points) | 24.52 ± 9.44 | 43.15 ± 17.51 | n.s. | |
| RASS (points) | 0 ± 1 | −3 ± 3 | n.s. | |
| Diabetes (%) | 11 (10.9%) | 13 (11.9%) | p = 0.202 | |
| Hypertension (%) | 33 (34.7%) | 22 (25.7%) | p = 0.612 | |
| Chronic kidney disease (%) | 7 (6.9%) | 15 (17.8%) | n.s. | |
| C-reactive protein at admission (mg/L) | 79.8 ± 81 | 125.9 ± 86.3 | 0.004 | |
| C-reactive protein after 72 h (mg/L) | 59 ± 60.3 | 103.5 ± 72.6 | 0.001 | |
| Procalcitonin at admission (ng/mL) | 3.26 ± 6.68 | 2.67 ± 6.97 | 0.796 | |
| Procalcitonin after 72 h (ng/mL) | 0.22 ± 0.2 | 2.82 ± 1,24 | 0.042 | |
| White blood cell counts at admission (109/L) | 11.62 ± 6.74 | 15.74 ± 9.01 | 0.027 | |
| White blood cell counts after 72 h (109/L) | 11.82 ± 6.01 | 13.05 ± 6.26 | 0.299 | |
| Controls | Patients | p-Value | |
|---|---|---|---|
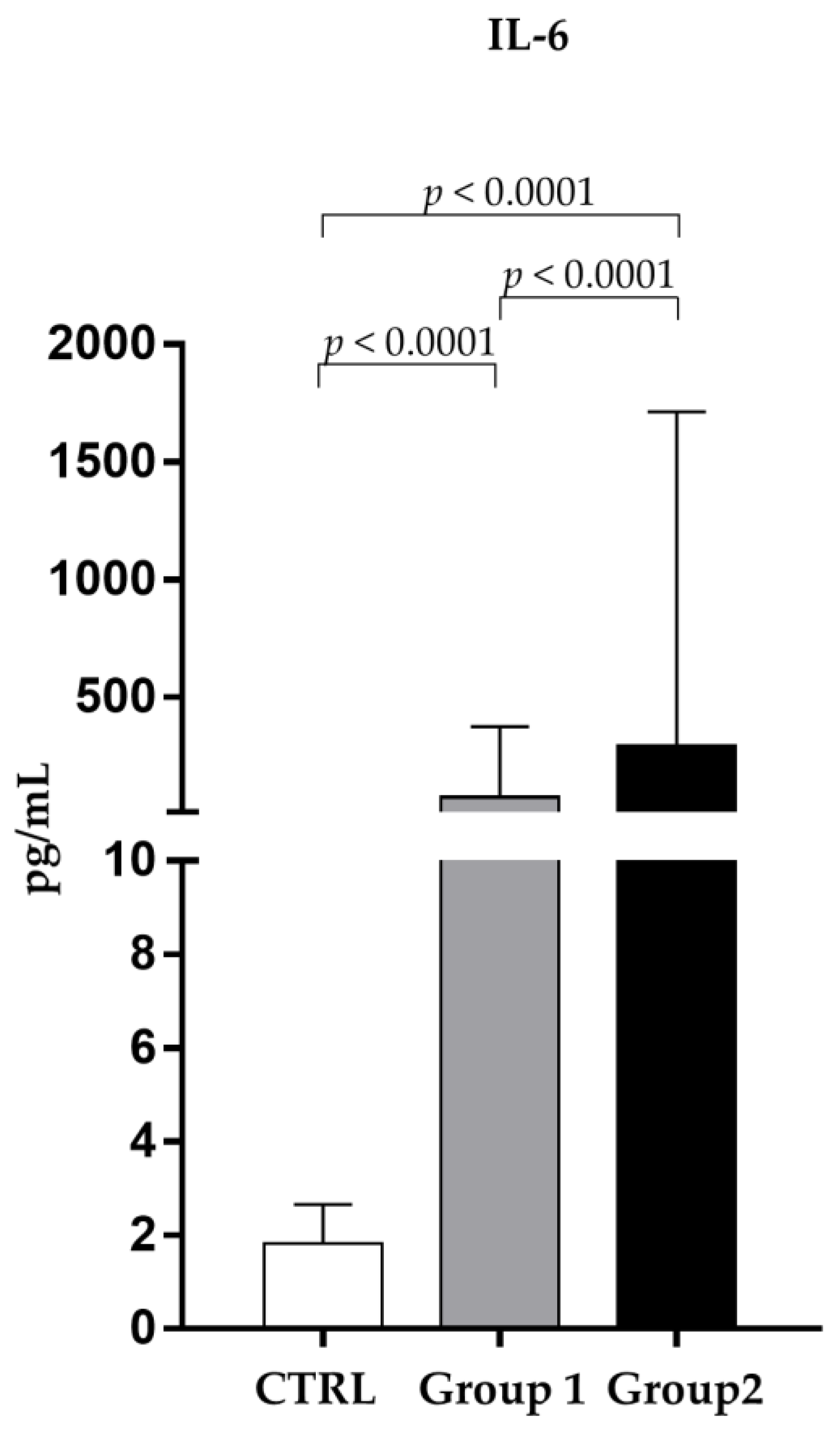
| IL-6 (pg/mL) | 1.92 ± 0.58 | 265.51 ± 976.82 | p < 0.0001 |
| sIL-6R (ng/mL) | 30.01 ± 7.68 | 39.71 ± 17.87 | p < 0.005 |
| sgp130 (ng/mL) | 324.31 ± 43.58 | 181.52 ± 67.29 | p < 0.0001 |
| Correlations | SAPS II | Charlson Index | RASS | |
|---|---|---|---|---|
| IL-6 | Person, p | −0.057, 0.568 | −0.015, 0.882 | 0.068, 0.497 |
| Spearman, p | 0.017, 0.87 | 0.026, 0.795 | −0.051, 0.609 | |
| sIL-6R | Person, p | 0.052, 0.61 | 0.139, 0.168 | −0.155, 0.124 |
| Spearman, p | 0.058, 0.567 | 0.106, 0.294 | −0.141, 0.162 | |
| sgp-130 | Person, p | −0.029, 0.773 | −0.036, 0.722 | −0.086, 0.392 |
| Spearman, p | −0.055, 0.588 | −0.07, 0.491 | −0.071, 0.485 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Spigna, G.; Spalletti Cernia, D.; Covelli, B.; Vargas, M.; Rubino, V.; Iacovazzo, C.; Napolitano, F.; Postiglione, L. Interleukin-6 and Its Soluble Receptor Complex in Intensive Care Unit COVID-19 Patients: An Analysis of Second Wave Patients. Pathogens 2023, 12, 1264. https://doi.org/10.3390/pathogens12101264
Di Spigna G, Spalletti Cernia D, Covelli B, Vargas M, Rubino V, Iacovazzo C, Napolitano F, Postiglione L. Interleukin-6 and Its Soluble Receptor Complex in Intensive Care Unit COVID-19 Patients: An Analysis of Second Wave Patients. Pathogens. 2023; 12(10):1264. https://doi.org/10.3390/pathogens12101264
Chicago/Turabian StyleDi Spigna, Gaetano, Daniela Spalletti Cernia, Bianca Covelli, Maria Vargas, Valentina Rubino, Carmine Iacovazzo, Filomena Napolitano, and Loredana Postiglione. 2023. "Interleukin-6 and Its Soluble Receptor Complex in Intensive Care Unit COVID-19 Patients: An Analysis of Second Wave Patients" Pathogens 12, no. 10: 1264. https://doi.org/10.3390/pathogens12101264
APA StyleDi Spigna, G., Spalletti Cernia, D., Covelli, B., Vargas, M., Rubino, V., Iacovazzo, C., Napolitano, F., & Postiglione, L. (2023). Interleukin-6 and Its Soluble Receptor Complex in Intensive Care Unit COVID-19 Patients: An Analysis of Second Wave Patients. Pathogens, 12(10), 1264. https://doi.org/10.3390/pathogens12101264