Abstract
Infections due to the Aspergillus species constitute an important challenge for human health. Invasive aspergillosis represents a life-threatening disease, mostly in patients with immune defects. Drugs used for fungal infections comprise amphotericin B, triazoles, and echinocandins. However, in the last decade, an increased emergence of azole-resistant Aspergillus strains has been reported, principally belonging to Aspergillus fumigatus species. Therefore, both the early diagnosis of aspergillosis and its epidemiological surveillance are very important to establish the correct antifungal therapy and to ensure a successful patient outcome. In this paper, a literature review is performed to analyze the prevalence of Aspergillus antifungal resistance in European countries. Amphotericin B resistance is observed in 2.6% and 10.8% of Aspergillus fumigatus isolates in Denmark and Greece, respectively. A prevalence of 84% of amphotericin B-resistant Aspergillus flavus isolates is reported in France, followed by 49.4%, 35.1%, 21.7%, and 20% in Spain, Portugal, Greece, and amphotericin B resistance of Aspergillus niger isolates is observed in Greece and Belgium with a prevalence of 75% and 12.8%, respectively. The prevalence of triazole resistance of Aspergillus fumigatus isolates, the most studied mold obtained from the included studies, is 0.3% in Austria, 1% in Greece, 1.2% in Switzerland, 2.1% in France, 3.9% in Portugal, 4.9% in Italy, 5.3% in Germany, 6.1% in Denmark, 7.4% in Spain, 8.3% in Belgium, 11% in the Netherlands, and 13.2% in the United Kingdom. The mechanism of resistance is mainly driven by the TR34/L98H mutation. In Europe, no in vivo resistance is reported for echinocandins. Future studies are needed to implement the knowledge on the spread of drug-resistant Aspergillus spp. with the aim of defining optimal treatment strategies.
1. Introduction
Aspergillus spp. are filamentous fungi found ubiquitously in the environment, in places such as soil, decaying vegetative material, and dust [1]. Furthermore, the fungi might colonize oligotrophic water systems: more than 400 different species have been found to inhabit different water sources [2], underlining that as well as air, water might also be a potential source of the transmission of filamentous fungi [3].
In different geographical areas, climatic factors such as humidity, rainy season, and temperature influence the prevalence of Aspergillus spp. [4].
The inhalation of Aspergillus conidia gives rise to different respiratory infections, affecting immunocompromised patients more severely.
Despite great advances in the diagnosis and treatment of aspergillosis, mortality remains high, particularly in subjects with important immune defects and invasive diseases.
Infections are generally due to Aspergillus fumigatus, even if other species are increasingly detected as etiological agents [5].
Recently, Aspergillus fumigatus was added to the list of the 19 fungal pathogens to be prioritized by the World Health Organization (WHO) and inserted into the critical group together with Cryptococcus neoformans, Candida auris, and Candida albicans [6].
Antifungal resistance is an emerging and important challenge in different parts of the world, with up to 20% of Aspergillus isolates displaying de novo resistance to commonly used antifungal drugs [7].
The aims of this review are to update the different antifungal-resistance mechanisms found in Aspergillus spp. and describe the prevalence of drug-resistant Aspergillus spp. in European countries to provide information for the adequate treatment of aspergillosis in this geographic area.
2. Summary of the Clinically Relevant Species
The genus Aspergillus is included in the family Aspergillaceae, order Eurotiales [8], and comprises six subgenera: Aspergillus, Circumdati, Cremei, Fumigati, Nidulantes, and Polypaecilum [9,10,11]. Every subgenus is divided into sections. In particular, two sections are included in the subgenus Aspergillus; 10 sections are included in the subgenus Circumdati; only one section is included in the subgenus Cremei; in the subgenus Fumigati, there are 4 sections; in the subgenus Nidulantes, there are 9 sections and, in the subgenus Polypaecilum, only one section is included (Figure 1) [9,10,11].

Figure 1.
Classification of Aspergillus spp.
Clinically relevant Aspergillus spp. are mostly included in the sections Fumigati, Flavi, Nidulantes, Nigri, Terrei, and Usti.
In the Fumigati section, there are 63 species [12]. Aspergillus fumigatus [12,13] is the species of this section mostly found in different countries and associated with human infection. Other clinically relevant species found are A. felis, A. fischeri, A. fumigatiaffinis, A. fumisynnematus, A. hiratsukae, A. laciniosus, A. lentulus, A. novofumigatus, A. pseudoviridinutans, A. spinosus, A. thermomutatus, A. udagawae, and A. viridinutans [12,14,15].
In the Flavi section, there are 35 species, according to the new taxonomy revision, where the most prevalent species in human infections was represented by Aspergillus flavus, followed by nine other species [11,12,16,17,18,19,20].
In the Terrei section, which comprises 17 species [11], A. terreus is the most frequent species of the section associated with invasive aspergillosis in immunocompromised patients and is responsible for 5.2% of all fungal infections [21,22,23,24].
The section Nigri includes 30 species, of which only 8 were found to be responsible for invasive aspergillosis: A. brasiliensis, A. carbonarius, A. japonicus, A. luchuensis, A. niger, A. tubingensis, A. uvarum, and A. welwitschiae [10,12,25].
In the Nidulantes section, there are 74 species [12,26]. Of them, only 11 species have been associated with human infections and the most prevalent species was A. nidulans, identified as an etiological agent of invasive aspergillosis and chronic granulomatous disease [27,28,29,30,31,32,33].
In the Usti section, there are 25 species, of which A. calidoustus was the species most often associated with invasive infections [12].
3. Clinical Picture
Aspergillus spp. are etiological agents responsible for different clinical manifestations in humans [34,35]. The severity of infections is dependent on the immune status of the patient and can be classified into noninvasive infections and invasive infections according to host immunocompetency.
3.1. Noninvasive Infections in the Immunocompetent Host
3.1.1. Chronic Pulmonary Aspergillosis
Chronic pulmonary aspergillosis (CPA) includes the chronic forms of aspergillosis, as well as aspergilloma, which generally affects patients with a preexisting pulmonary pathology such as tuberculosis or other cavitary chronic lung diseases [36]. The most common picture of CPA is chronic cavitary pulmonary aspergillosis (CCPA). Without effective therapy, CCPA may lead to chronic fibrosing pulmonary aspergillosis (CFPA). Aspergilloma, characterized by mycelial mass, inflammatory cells, fibrin and mucus, and Aspergillus nodules, is a less severe clinical picture of CPA [37].
Clinical symptoms of patients with CPA are chronic productive cough, weight loss, and hemoptysis with the presence of nodules and fungal balls at radiological observation [37].
CPA is estimated to affect 3 million people annually, but because it is often not recognized, the real incidence may be greater [37,38,39].
3.1.2. Allergic Bronchopulmonary Aspergillosis
Allergic bronchopulmonary (ABPA) is caused by hypersensitivity to Aspergillus fumigatus and affects almost exclusively atopic individuals and patients with cystic fibrosis, affecting nearly 5 million people annually [36,38]. In particular, the rate of ABPA in patients with cystic fibrosis is estimated to be 7.8% and is different among patients with various gene mutations [40].
Clinical symptoms are chronic cough, wheezing, low-grade fever, chest pain, blood eosinophilia, and central bronchiectasis on chest imaging.
3.2. Invasive Infections in the Immunocompromised Host
Invasive aspergillosis (IA) is the most severe clinical picture of aspergillosis, occurring in severely immunocompromised hosts [36]. The respiratory tract is the most common primary site of invasive aspergillosis, but because Aspergillus hyphae may invade pulmonary arterioles, a hematogenous spread with thrombosis, hemorrhagic infarction, and invasion of distant organs such as kidneys, liver, spleen, sinuses, and the central nervous system might occur in about 25% of patients.
Other clinical manifestations of IA, although less common, are osteomyelitis, arthritis, or subacute thyroiditis [9]. Endophthalmitis, secondary to intraocular surgery or hematogenous dissemination, is related to poor ocular prognosis [41]. The incidence of IA, which is estimated to affect 250,000 people globally, is still growing [38]. This rise is potentially due to the increased use of immunosuppressive treatments for cancer, hematological tumors, stem cell transplants, and solid organ transplants responsible for neutropenia in affected patients. Neutrophil recruitment and the production of reactive oxygen species play an important role in the inhibition of the germination of Aspergillus conidia. Therefore, severe and prolonged neutropenia is considered a major risk for IA. However, a shift in incidences of IA from neutropenic to non-neutropenic patients was recently observed, in particular in patients with viral infections such as influenza and SARS-CoV-2 [36,42] and in patients with CD4+ T-cell dysfunction [43].
It has also been found that invasive pulmonary aspergillosis shows different pathophysiological mechanisms based on the type of immunosuppression. Angio-invasive manifestation is principally detected in patients with neutropenia, while non-angio-invasive form was found in patients with corticosteroid-induced immunosuppression [44,45].
When IA is refractory to the therapy, the mortality rates are higher, ranging from 50% to 100% [46].
4. Diagnosis and Therapy
The improvement of disease outcomes in patients at higher risk of developing invasive aspergillosis is strictly associated with rapid diagnosis. To date, because there is not a specific assay, a combination of clinical, radiological, and microbiological features is recommended for an accurate diagnosis of invasive aspergillosis [47,48,49].
Routine microbiological tests include direct microscopic examination and culture with limited sensitivity that cannot alone discriminate between colonization and infection; furthermore, prior therapy is associated with false-negative culture results [50,51].
Other microbiological approaches are serological tests targeting the cell-wall component galactomannan (GM) in serum and bronchoalveolar fluid (BALF), the detection of the fungal cell-wall component 1, 3-β-D glucan in serum (although nonspecific for Aspergillus diseases only), the detection of Aspergillus-specific siderophores in BALF and urine, the detection of GM by a lateral flow device assay (LFD), and molecular tests such as PCR [52,53,54,55,56,57,58,59].
To overcome the limited sensitivity of any individual tests, combining different diagnostic assays is the currently recommended procedure because it has been shown that there is a significant increase in sensitivity with a slight reduction of specificity [60].
The antifungal drugs currently used for the therapy of aspergillosis comprise three classes of compounds, two of which target ergosterol (triazoles and amphotericin B), and a third class (echinocandins) that arrests the synthesis of beta-1,3 glucan, an important constituent of the cell wall [61,62,63,64,65]. However, allergic forms of infection may need glucocorticoids or anti-IgE therapy, as well as antifungal drugs, while aspergilloma can be treated by surgery.
Voriconazole, isavuconazole, and posaconazole, belonging to the triazoles class, are the first-line agents for invasive infections, while voriconazole or itraconazole are the first-line agents for chronic diseases [66,67,68].
For the management of refractory aspergillosis, a combination therapy with drugs that have different mechanisms of action, such as voriconazole or amphotericin B and an echinocandin, is the suggested approach [69]. Resistance to first-line agents among Aspergillus spp. has given rise to the elevated utilization of second-line agents represented by echinocandins in monotherapy [70]; these drugs were initially approved by the FDA for the management of invasive aspergillosis refractory to the standard therapy [71].
Antifungal susceptibility testing to assess antifungal drug activity is performed by broth microdilution tests or gradient strip tests according to the guidelines of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) or the Clinical and Laboratory Standards Institute (CLSI) [72]. For Aspergillus spp., in contrast to A. fumigatus, because of the absence of clinical breakpoints, epidemiological cut-off values (ECOFFs) are available from the EUCAST for the most used drugs (triazoles) [73].
5. Antifungal-Resistance Mechanisms
The emergence of resistance to antifungals affects their clinical effectiveness, leading to a great public health problem worldwide. Here, we summarize all mechanisms underlying antifungal resistance in Aspergillus spp.
5.1. Amphotericin B Resistance
Amphotericin B acts by interacting with sterols, in particular with ergosterol, the principal component of the fungal cell membrane. The integration of amphotericin B into the fungal membrane leads to the formation of channels (Figure 2). This formation impairs barrier membrane function, increasing the permeability responsible for the leakage of potassium, protons, cations, and cytoplasmic materials that induce cell death [74]. Furthermore, amphotericin B can produce reactive oxygen species (ROS) that give rise to cellular damage [75]. Among Aspergillus spp., Aspergillus terreus is the strain harboring intrinsic resistance to amphotericin B [76].
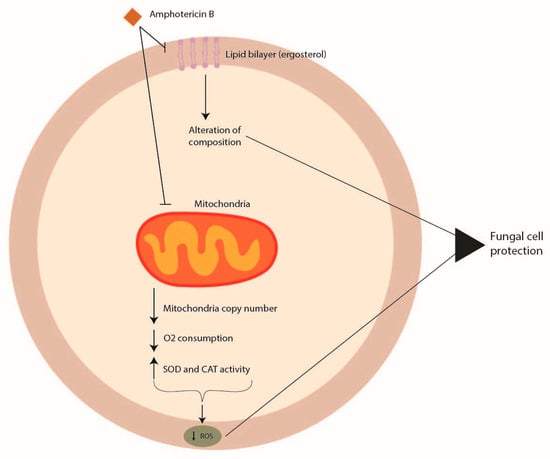
Figure 2.
Mechanisms of Aspergillus spp. antifungal drug resistance: amphotericin B resistance.
The mode of action of amphotericin B in Aspergillus terreus has not been well elucidated, and no genomic features have been identified to date that might be linked to amphotericin B resistance. However, amphotericin B resistance in section Terrei seems to be associated with the modulation of molecular chaperones, targeting ROS by mitochondria and influencing cellular redox homeostasis, with an increase in the level of catalase and superoxide dismutase with respect to other Aspergillus species [76,77,78] (Figure 2).
Following the increasing rate of azole resistance [79], the use of amphotericin B has enhanced, and this might be the reason why, recently, an increase in MIC values for amphotericin B in different Aspergillus species has been reported [80,81,82,83], even if resistance to this drug remains extremely rare [84].
In a recent study [85], among 26,909 Aspergillus isolates analyzed, resistance to amphotericin B was detected in 36.8% of Aspergillus terreus, 14.9% of Aspergillus flavus, 5.2% of Aspergillus niger, and 2.01% of Aspergillus fumigatus isolates. Furthermore, some Aspergillus lentulus and Aspergillus ustus isolates have been reported to show amphotericin B resistance [86,87]. Additionally, an increasing trend in amphotericin B resistance was observed in Aspergillus fumigatus between 2016 and 2020, together with a decreasing trend in amphotericin B resistance in Aspergillus terreus and Aspergillus flavus [85].
5.2. Azole Resistance
Azole antifungal drugs act by interfering with the synthesis of ergosterol, mediated by the fungal sterol 14 alpha-demethylases (Cyp51A and Cyp51B) (Figure 3).

Figure 3.
Mechanisms of Aspergillus spp. antifungal drug resistance: azole resistance.
The principal mechanisms of azole resistance involve (a) mutations in the sterol-demethylase gene cyp51A reducing the affinity between the azole drug and its target; (b) the overexpression of the sterol-demethylase gene cyp51A leading to an increase of the azole concentration able to inhibit fungal growth; (c) the overexpression of efflux pump systems decreasing the intracellular drug concentration [88,89]. Alternate mechanisms associated with azole resistance are the modification of HapE [90], the involvement of the mitochondrial complex 1 and the cytochrome b5-CybE redox systems [91,92], the transcription factors SrbA and AtrR [93,94] and biofilm formation (Figure 3) [95].
The acquisition of azole resistance occurs in two ways: in vivo, by selection of resistant isolates during long therapy with azoles, and in vitro, by the selection of resistant isolates as a consequence of an extensive use of azole fungicide in agriculture [96,97,98].
5.2.1. Mutations in the Sterol-Demethylase Gene Cyp51
Cyp51 genes are the major targets studied for azole resistance in fungal pathogens—resistance that might also be acquired by horizontal gene transfer (HGT) [99]. Different species of Aspergillus exhibit several numbers of cyp51 paralogs in their genome. This genetic redundancy gives the fungus an advantage to survive when exposed to fungicides, increasing its azole resistance [100]. In Aspergillus fumigatus, Aspergillus terreus, and Aspergillus niger, there are only two paralogs (cyp51A and cyp51B), while in Aspergillus flavus, three paralogs exist (cyp51A, cyp51B and cyp51C) [101]. However, only specific mutations in Cyp51A and Cyp51C proteins have been shown to have an impact on azole resistance, while the Cyp51B protein might play other roles that need to be studied in detail [102].
In Aspergillus fumigatus, amino-acid mutations in the Cyp51A protein related to azole resistance were G54, Y121, G138, P216, F219, M220, A284, Y431, G432, G434, and G448 [103,104,105,106,107,108,109]. No mutations were associated with azole resistance in the CypB protein [88,110].
Also, in Aspergillus lentulus, it was demonstrated by targeted cyp51A gene knockout that intrinsic azole resistance was related to this gene [111].
In Aspergillus flavus with reduced voriconazole susceptibility, different mutations were reported in Cyp51A, Cyp51B, and Cyp51C proteins, even if their role in azole resistance needs to be clarified by further studies. Amino-acid changes in Cyp51A protein were identified at positions R450S, K197N/D282E/M288L, and Y132N/T469S [112]; in Cyp51B protein, detected mutations were H399P, D411N, T454P, T486P 105, and Q354K [113]; in Cyp51C protein, the Y319H mutation was identified from an azole-resistant clinical isolate [114] and the mutations S196F, A324P, N423D, and V465M [115,116].
In section Nigri, in Cyp51A protein, many mutations were identified, but their role in inducing azole resistance is still uncertain [117].
In particular, in Aspergillus tubingensis, a recent study found the amino-acid change H467Q in combination with the mutations K64E or V377I exclusively in non-wildtype isolates [118], while in Aspergillus niger, no mutation is associated with azole resistance [118].
However, it has been found that single-gene deletions of cyp51A and cyp51B genes in Aspergillus tubingensis and Aspergillus niger decrease the voriconazole MIC values below the ECV established by CLSI [119].
In Aspergillus braziliensis with reduced azole susceptibility, there were no mutations present in Cyp51A protein [118].
Regarding the Terrei section, few studies are available in the literature about their azole resistance; only a mutation of methionine in position 217 in Aspergillus terreus has been reported [120,121].
In the Usti section, the intrinsically azole-resistant species Aspergillus calidoustus exhibited a mutation M220V in Cyp51A protein, a position already associated with azole resistance in Aspergillus fumigatus [88].
5.2.2. Overexpression of the Sterol-Demethylase Cyp51
The overexpression of Cyp51 is considered another mechanism of azole resistance in Aspergillus spp., in particular in Aspergillus fumigatus.
Regarding Aspergillus flavus, the overexpression of Cyp51A and Cyp51B was not related to azole resistance because the levels of gene expression were the same both in wild and non-wildtype strains [122,123]. Also, in the Nigri section, this mechanism seems not to be related to azole resistance, even if Cyp51A is upregulated after azole exposure [118,124].
Changes in the promoter region of cyp51 have been described as a mechanism to contrast azole toxicity, mostly in Aspergillus fumigatus, such as the insertion of tandem repeats (TR) of 34bp, 46bp, and 53 bp leading to upregulation of cyp51 [125]. These insertions were often associated with amino-acid substitutions in Cyp51A and have been observed in strains that exhibit reduced susceptibility to azoles [126].
In particular, the TR34/L98H mutation was found principally in resistant environmental isolates, linked to total resistance to itraconazole and reduced susceptibility to voriconazole and posaconazole [89,127,128].
Furthermore, the TR46/Y121F/T289A mutation was found in isolates with high levels of resistance to voriconazole and other azoles [129]. For the tandem repeat of 53 bp, no amino-acid substitution has been found to date [128,130].
Other transcription factors were found able to regulate cyp51 expression in Aspergillus fumigatus, such as SrbA, HapE, and AtrR.
SrbA is a transcriptional regulator that is involved in different processes, as well as sterol biosynthesis [131,132,133], and its deletion leads to greater azole susceptibility [93].
The mutation P88L in heme activator protein E (HapE), a subunit of the CCAAT-binding transcription factor complex (CBC), determines an upregulation of the cyp51A gene and confers azole resistance [134]. A decrease in CBC activity, a negative regulator of the ergosterol pathway, increases the expression of the enzymes involved in its biosyntheses, such as HMG-CoA-synthase, HMG-CoA-reductase, and sterol C14-demethylase contributing to azole resistance [90].
Furthermore, a Zn2Cys6 cluster-containing transcription factor, called ABC transporter regulator or AtrR, was found to be important for azole tolerance both in Aspergillus fumigatus and Aspergillus flavus [135,136]. Additionally, cytochrome b5CybE has been found to be able to regulate the expression level of cyp51A [92].
Furthermore, biofilm production was also hypothesized to play a role in the azole resistance of Aspergillus fumigatus. The cell density reached in a mature biofilm, together with the production of polysaccharide extracellular matrix, protects the mold by the action of the immune system and the antifungal drugs [96].
5.2.3. Overexpression of Efflux Pump Systems
Efflux pumps are transmembrane proteins that expel drugs from the cell, reducing their intracellular concentration. Therefore, the overexpression of these proteins might be related to azole resistance. The principal types of efflux pumps are the ATP-binding cassette (ABC) transporter and the major facilitator superfamily (MFS) transporter, which differ in structure and activity [137]. ABC transporters use ATP as an energy source, while MFS transporters use a proton gradient to pump out the drugs [138].
The more studied ABC transporters involved in azole resistance are cdr1B, mdr1, mdr2, mdr3, mdr4, abcD, abcE, atrI, atrB, atrC, and atrF. In Aspergillus fumigatus and Aspergillus flavus, only the ABC transporter Cdr1B has been found to be related to azole resistance [139,140].
MFS transporters were less studied, and among them, only mdrA has been associated with an increase of itraconazole and voriconazole susceptibility in Aspergillus fumigatus [141].
5.3. Echinocandin Resistance
Echinocandins (caspofungin, anidulafungin, and micafungin) act by inhibiting the glucan synthase, an enzyme codified by the FKS1 and FSK2 genes, important for the synthesis of the beta1, 3 glucan (Figure 4). However, because echinocandins have only a fungistatic activity against Aspergillus spp., they are used only in combination with a polyene or an azole to obtain an important synergistic effect. To date, the echinocandin resistance is rarely found in Aspergillus spp. [142].

Figure 4.
Mechanisms of Aspergillus spp. antifungal drug resistance: echinocandin resistance.
Some studies have reported mutations in FSK genes [143] and changes in the lipid profile around the enzyme [144] as possible mechanisms of echinocandin resistance (Figure 4). In Aspergillus fumigatus, two mutations (S678P and E671Q) in the FSK1 gene were associated with echinocandin resistance [145,146], while in Aspergillus flavus it was shown that P-type ATPase and ubiquinone biosynthesis methyltransferase COQ5 might be involved in caspofungin resistance [147].
6. Prevalence of Aspergillus spp. Drug Resistance in Europe
6.1. Amphotericin B Resistance
Amphotericin B resistance is rarely represented in Aspergillus fumigatus, while poor susceptibility to this drug was reported for Aspergillus terreus, Aspergillus flavus, and Aspergillus niger [85].
In distinct geographical areas, prevalence of these molds was different: amphotericin B-resistant Aspergillus niger isolates were found at higher frequencies in Asia and America (20.9% and 2.7%, respectively) than in Europe (0.62%) [85], while for amphotericin B-resistant Aspergillus terreus isolates, a lower prevalence was found in America (25.1%) than Asia and Europe (40.4% and 40.1%, respectively) [85].
In European countries, the prevalence of amphotericin B-resistant Aspergillus species was quite different (Figure 5). In France, a prevalence of 84% (31/37) isolates of Aspergillus flavus was reported [81], while in Spain, 38/77 (49.4%) isolates of Aspergillus flavus were amphotericin B-resistant 80. In Italy, a different prevalence of amphotericin B was reported between distinct Aspergillus species, with 5/13 (38.5%) isolates of Aspergillus terreus, 2/10 (20%) isolates of Aspergillus flavus and 6/38 (15.7%) isolates of Aspergillus oryzae [148].
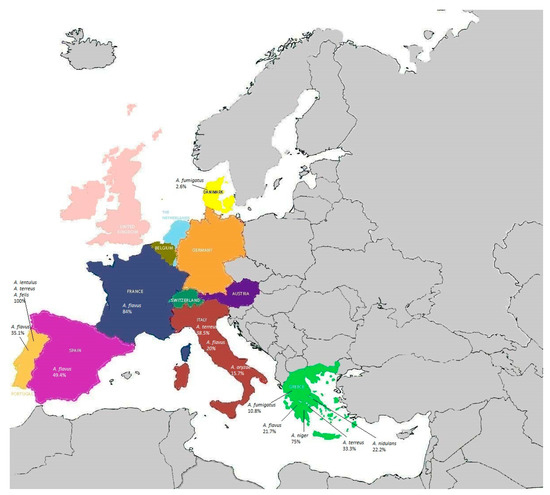
Figure 5.
Prevalence of amphotericin B-resistant Aspergillus spp. in European countries.
In Greece, a total prevalence of amphotericin B resistance of 17.6% (18/102) was found, which was distributed as follows: 21.7% in Aspergillus flavus isolates (5/23), 10.8% in Aspergillus fumigatus isolates (4/37), 75% in Aspergillus niger isolates (3/4), 33.3% in Aspergillus terreus isolates (4/12), and 22.2% in Aspergillus nidulans isolates (2/9) [149]. In Portugal, a prevalence of amphotericin B resistance of 35.7% in Aspergillus flavus (5/14) was reported, while all the Aspergillus lentulus, Aspergillus terreus, and Aspergillus felis isolates were resistant to this drug [150].
In Belgium, amphotericin B resistance had a prevalence of 12.8% in Aspergillus section Nigri isolates [151], and in Denmark, 3/112 isolates of Aspergillus fumigatus (2.6%) exhibited amphotericin B resistance [152].
The accurate establishment of amphotericin B resistance is difficult because different MIC assays might be used in different laboratories. Moreover, there is a lack of breakpoints for Aspergillus species different from Aspergillus fumigatus, and changes in amphotericin B susceptibility breakpoints have been reported.
6.2. Azole Resistance
Many studies have principally focused on azole-resistant Aspergillus fumigatus isolates because they represent the predominant pathogen of aspergillosis. The overall azole resistance rate of Aspergillus fumigatus was reported as ranging from 0.6 to 27.8%, depending on the isolation country, the type of disease, and the emergence of the environmental resistance mechanism [153].
Most of the environmental azole-resistant isolates were found in Europe (56.7%) than in other countries due to the higher azole fungicide application per hectare of agricultural land [39].
The Netherlands was the European country using the greatest amount of azole fungicide, followed by Germany and France. In fact, the first environmental pan-azole-resistant Aspergillus fumigatus isolate was detected in the Netherlands [154].
The most recent studies found in the literature have reported the prevalence of azole resistance in Aspergillus spp. from Austria, the United Kingdom, Belgium, France, Denmark, Portugal, the Netherlands, Greece, Spain, Switzerland, Italy, and Germany (Figure 6).

Figure 6.
Prevalence of azole-resistant Aspergillus fumigatus strains in European countries.
A survey conducted in Tyrol, Austria, showed a low prevalence (1/388 isolates, 0.29%) of azole resistance of Aspergillus fumigatus, while Aspergillus terreus had a percentage of resistance to posaconazole ranging from 0.3% during the period 2007–2009 to 0.6% during the period 2010–2012 fading away from 2013 to 2017 [155].
In the United Kingdom, analysis of urban and rural environments showed a prevalence of azole-resistant Aspergillus fumigatus of 6.7%, reaching a prevalence of 13.8% in urban environments. The TR34/L98H mutation was the most detected one. The TR46/Y121F/T289A resistance allele was also identified for the first time in this country [156].
For clinical isolates, a study performed in a cardiothoracic center in London detected a higher prevalence of azole-resistant Aspergillus fumigatus (13.2%) principally associated with the environmentally driven TR34/L98H mutation [157].
In Belgium, the prevalence of azole resistance of Aspergillus fumigatus isolates analyzed in a hospital in Leuven was found to be stable during the study period (2016–2020) ranging from 8.3% in 2016 to 7.4% in 2020, with an overall five-year azole resistance prevalence of 7.1%. The TR34/L98H mutation was the most predominant (83%), followed by the TR46/Y121F/ T289A (13.8%) [158].
A recent study performed in Lyon, France [159] detected a prevalence of azole resistance of 2.1% (4/195) of Aspergillus fumigatus isolates, which increased to 4.3% in patients with cystic fibrosis, a percentage similar to that found in Paris [160] and similar to that found in Rennes (5% of isolates resistant to voriconazole) [161], but lower than that observed in Nantes (6.8%) [162] for the same category of patients. One azole-resistant isolate exhibited the F46Y, M172V, and 427K mutations in the cyp51A gene. No mutations were identified in the cyp51A promoter, but significant induction of cyp51A, cyp51B, atrF, and cdr1B gene expression was observed in the resistant isolates.
In Denmark, an azole resistance prevalence of 6.1% was observed during the nationwide surveillance study period (2018–2020), with a TR34/L98H mutation identified in 3.6% of patients, while the TR46/Y121F/T289A mutation was not detected [163]. Furthermore, in the Danish population affected by cystic fibrosis, an azole prevalence of 7.3%, including 3.7% TR34/L98H, was observed.
Furthermore, in Denmark, a fatal clinical case of infection with an isolate of Aspergillus fumigatus that acquired an unusual 120-bp tandem repeat resistance mechanism during long-term azole treatment was recently described [164].
In Portugal, a survey performed in three hospitals showed a prevalence of isolates belonging to Aspergillus fumigatus complex (86.7%) and 7.5% of isolates belonging to cryptic species. The latter presented percentages of 47.1%, 82.4%, and 100% of voriconazole, posaconazole, and isavuconazole resistance, respectively [137]. Eight Aspergillus fumigatus sensu stricto isolates showed azole resistance (8/227, 3.5%). Three isolates of them with pan-azole-resistant profiles exhibited the TR34/L98H and TR46/Y121F/T289A mutations; the other three azole-resistant ones showed F46Y/M172V/N248T/D255E/E427K mutations, while the other two isolates carried no mutations.
During the 6-year study period (2013–2018), the prevalence of azole resistance of Aspergillus fumigatus isolates in the Netherlands was 11% (508/4496), rising from 7.6% in 2013 to 14.7% in 2018 [165]. The predominant detected mutations were TR34/L98H (69%) and TR46/Y121/T289A (17%).
A soil-sampling survey was conducted in Greece [166] to analyze the prevalence of environmental azole-resistant Aspergillus spp. showing that Aspergillus niger was the most frequent species complex (57%), followed by Aspergillus terreus (17%), Aspergillus fumigatus (14%), and Aspergillus flavus (5%). All non-fumigatus Aspergillus species exhibited full susceptibility to azoles, while only one isolate (1/101, 1%) of Aspergillus fumigatus was pan-azole-resistant, carrying the TR46/Y121/T289A mutation in the cyp51A gene.
In Spain, the prevalence of azole resistance observed in Aspergillus fumigatus sensu lato was 7.4% (63/847). Azole resistance was higher in cryptic species (18/19, 95%) than in Aspergillus fumigatus sensu stricto (45/828, 5.5%) and principally associated with the TR34/L98H mutation (24/63, 38%) [167].
A screening of 160 clinical samples performed to detect azole-resistant Aspergillus fumigatus isolates in the Hospital of Geneva, Switzerland, reported only two pan-azole-resistant isolates (1.2%) with the TR34/L98H mutation [168].
A multicenter study performed in Italy reported an overall azole resistance prevalence of 4.9% and 6.9%, considering only the Aspergillus fumigatus sensu stricto isolate associated with the TR34/L98H mutation [169]. Furthermore, the F46Y/M172V/N248T/D255E/E427K amino-acid changes were observed in one azole-resistant isolate.
In Germany, a multicenter study detected a prevalence of azole-resistant Aspergillus fumigatus isolates of 5.3% (51/961) from patients with cystic fibrosis, and the most frequent mutation was TR34/L98H [170].
6.3. Echinocandin Resistance
In the literature, there were no reports about the echinocandin resistance of Aspergillus spp. isolates in Europe. Only a clinical isolate of Aspergillus fumigatus, recovered from a patient on micafungin therapy for chronic pulmonary aspergillosis, with an echinocandin resistance-associated point mutation in the well-conserved hot-spot 1 region of fks1 conferring an F675S amino-acid substitution, was reported [143].
7. Conclusions
Our review underlines that, to date, in European countries, amphotericin B resistance is rarely detected in Aspergillus fumigatus isolates. By contrast, the emergence of azole-resistant Aspergillus fumigatus isolates represents an important concern in Europe, with countries from Austria, which reported the lowest prevalence (0.3%), to the United Kingdom and the Netherlands, which presented the highest prevalence (13.2% and 11%, respectively), increasing in patients with cystic fibrosis. Furthermore, the principal mechanism of azole resistance relies on the TR34/L98H mutation, which comprises many of the resistant isolates. This allele was the first to be linked to pan-azole resistance, and it has been related to the overuse of environmental azoles, underlining the need to limit the use of azoles in agriculture.
On the other side, the frequency of invasive fungal disease caused by other non-fumigatus Aspergillus species is increasing. Furthermore, the treatment of these invasive fungal diseases is complicated by their often intrinsic resistance to amphotericin B and the exhibition of various high MICs against triazoles.
Therefore, susceptibility testing of clinically important isolates has been strongly recommended in the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) aspergillosis guidelines, suggesting a combination therapy until a susceptibility pattern is known that can guide towards a targeted systemic antifungal treatment.
These data highlight the requirement of continuous surveillance to monitor the frequency of Aspergillus species involved in fungal diseases in different geographical areas and the occurrence of antifungal drug resistance to start with the appropriate therapy as soon as possible for a successful patient outcome.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The author is deeply grateful to Crea Kajal for the figure’s artwork.
Conflicts of Interest
The author declares no conflict of interest.
References
- Denning, D.W. Invasive aspergillosis. Clin. Infect. Dis. 1998, 26, 781–803. [Google Scholar] [CrossRef]
- Babic, N.; Gunde-Cimerman, N.; Vargha, M.; Tischnner, Z.; Magyar, D.; Verissimo, C.; Sabino, R.; Viegas, C.; Meyer, W.; Brandão, J. Fungal contaminants in drinlink water regulaton? A tle of ecology, exposure, purification and clinical relevance. Int. J. Environ. Res. Public Health 2017, 14, 636. [Google Scholar] [CrossRef]
- Warris, A.; Klaassen, C.H.W.; Meis, J.F.G.M.; de Ruiter, M.T.; de Valk, H.A.; Abrahamsen, T.G.; Gaustad, P.; Verweij, P.E. Molecular epidemiology of Aspergillus fumigatus isolates recovered from water, air, and patients shows two clusters of genetically distinct strains. J. Clin. Microbiol. 2003, 41, 4101–4106. [Google Scholar] [CrossRef] [PubMed]
- Panackai, A.A.; Li, H.; Kontoyiannis, D.P.; Mori, M.; Perego, C.A.; Boeckh, M.; Marr, K.A. Geoclimatic influences on invasive aspergillosis after hematopoietic stem cell transplantation. Clin. Infect. Dis. 2010, 50, 1588–1597. [Google Scholar] [CrossRef] [PubMed]
- Zanganeh, E.; Zarrinfar, H.; Rezaeetalab, F.; Fata, A.; Tohidi, M.; Najafzadeh, M.J.; Alizadeh, M.; Seyedmousavi, S. Predominance of non-fumigatus Aspergillus species among patients suspectedto pulmonary aspergillosis in a tropical and subtropical region of the MiddleEast. Microb. Pathog. 2018, 116, 296–300. [Google Scholar] [CrossRef]
- Cadena, J.; Thompson, G.R.; Patterson, T.F. Aspergillosis. Epidemiology, diagnosis and treatment. Infect. Dis. Clin. N. Am. 2021, 3, 415–434. [Google Scholar] [CrossRef]
- WHO Fungal Priority Pathogens List to Guide Research, Development and Public Health Action; World Health Organization: Geneva, Switzerland, 2022.
- Houbraken, J.; Samson, R.A. Pylogeny of Penicillium and the segregation of Trichocomaceae into three families. Stud. Mycol. 2011, 70, 1–51. [Google Scholar] [CrossRef]
- Chandanadukkam, R.K.; Prakash, P.Y. Taxonomic updates with key focus on medically important fungi. In Diagnostics and Marker Developments; Sing, B.P., Gupta, V.K., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 251–255. [Google Scholar]
- Samson, R.A.; Visagie, C.M.; Houbraken, J.; Hong, S.B.; Hubka, V.; Klaasen, C.H.; Perrone, G.; Seifert, K.A.; Susca, A.; Tanney, J.B.; et al. Phylogeny, identification and nomenclature of the genus Aspergillus. Stud. Mycol. 2014, 78, 141–173. [Google Scholar] [CrossRef]
- Houbraken, J.; Kocsube, S.; Visagie, C.M.; Yilmaz, N.; Wang, X.C.; Meijer, M.; Kraak, B.; Hubka, V.; Bensch, K.; Samson, R.A.; et al. Classification of Aspergillus, Penicillium, Talaromyces and related genera (Eurotiales): An overview of families, genera, subgenera, sections, series and species. Stud. Mycol. 2020, 95, 5–169. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A.; Houbraken, J.; Lombardi, L.; Garcia-Rubio, R.; Jenks, J.D.; Rivero-Menendez, O.; Aljohani, R.; Jacobsen, I.D.; Berman, J.; et al. Aspergillus fumigatus and aspergillosis: From basics to clinics. Stud. Mycol. 2021, 100, 100115. [Google Scholar] [CrossRef]
- Binder, U.; Lass-Flörl, C. New insights into invasive aspergillosis-from the pathogen to the disease. Curr. Pharm. Des. 2013, 19, 3679–3688. [Google Scholar] [CrossRef] [PubMed]
- Sugui, J.A.; Peterson, S.W.; Figat, A.; Hansen, B.; Samson, R.A.; Mellado, E.; Cuenca-Estrella, M.; Kwon-Chung, K.J. Genetic relatedness versus biological compatibility between Aspergillus fumigatus and related species. J. Clin. Microbiol. 2014, 52, 3707–3721. [Google Scholar] [CrossRef] [PubMed]
- Frisvad, J.C.; Larsen, T.O. Extrolites of Aspergillus fumigatus and other pathogenic species in Aspergillus section Fumigati. Front. Microbiol. 2016, 6, 1485. [Google Scholar] [CrossRef] [PubMed]
- Visagie, C.M.; Varga, J.; Houbraken, J.; Meijer, M.; Kocsubé, S.; Yilmaz, N.; Fotedar, R.; Seiferrt, K.A.; Frisvad, J.C.; Samson, R.A. Ochratoxin production and taxonomy of the yellow aspergilli (Aspergillus section Circumdati). Stud. Mycol. 2014, 78, 1–61. [Google Scholar] [CrossRef] [PubMed]
- Frisvad, J.C.; Hubka, V.; Ezekiel, C.N.; Hong, S.B.; Nováková, A.; Chen, A.J.; Aezanlou, M.; Larsen, T.O.; Sklenář, F.; Mahakarnchanakul, W.; et al. Taxonomy of Aspergillus section Flavi and their production of aflatoxins, ochratoxins and other mycotoxins. Stud. Mycol. 2019, 93, 1–63. [Google Scholar] [CrossRef]
- Hedayati, M.T.; Pasqualotto, A.C.; Warn, P.A.; Bowyer, P.; Denning, D.W. Aspergillus flavus: Human pathogen, allergen and mycotoxin producer. Microbiology 2007, 153, 1677–1692. [Google Scholar] [CrossRef]
- Alshehri, B.; Palanisamy, M. Evaluation of molecular identification of Aspergillus species causing fungal keratitis. Saudi J. Biol. Sci. 2020, 27, 751–756. [Google Scholar] [CrossRef]
- Rudramurthy, S.M.; Paul, R.A.; Chakrabarti, A.; Mouton, J.W.; Meis, J.F. Invasive aspergillosis by Aspergillus flavus: Epidemiology, diagnosis, antifungal resistance and management. J. Fungi 2019, 5, 55. [Google Scholar] [CrossRef]
- Lass-Flörl, C.; Griff, K.; Mayr, A.; Petzer, A.; Gastl, G.; Bonatti, H.; Freund, M.; Kropshofer, G.; Dierich, M.P.; Nachbaur, D. Epidemiology and outcome of infections due to Aspergillus terreus: 10-year single centre experience. Br. J. Haematol. 2005, 131, 201–207. [Google Scholar] [CrossRef]
- Lass-Flörl, C.; Griff, K.; Kontoyiannis, D.P. Molecular typing of Aspergillus terreus isolates collected in Houston, Texas and Innsbruck, Austria: Evidence of great genetic diversity. J. Clin. Microbiol. 2007, 45, 2686–2690. [Google Scholar] [CrossRef]
- Perfect, J.R.; Cox, G.M.; Lee, J.Y.; Kauffman, C.A.; de Repentigny, L.; Chapman, S.W.; Morrison, V.A.; Pappas, P.; Hiemenz, J.W.; Stevens, D.A.; et al. The impact of culture isolation of Aspergillus species: A hospital-based survey of aspergillosis. Clin. Infect. Dis. 2001, 33, 1824–1833. [Google Scholar] [CrossRef]
- Rissleger, B.; Zoran, T.; Lackner, M.; Aigner, M.; Sánchez-Reus, F.; Rezusta, A.; Chowdhary, A.; Taj-Aldeen, S.J.; Arendrup, M.C.; Oliveri, S.; et al. A prospective international Aspergillus terreus survey: An EFISG, ISHAM and ECMM joint study. Clin. Microbiol. Infect. 2017, 23, 776.e1–776.e5. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wang, J.; Zhang, M.; Zhu, M.; Wang, M.; Sun, Y.; Gu, H.; Cao, J.; Li, X.; Zhang, S.; et al. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry for rapid identification of fungal rhinosinusitis pathogens. J. Med. Microbiol. 2017, 66, 328–333. [Google Scholar] [CrossRef]
- Sklenar, F.; Jurevic, Z.; Peterson, S.W.; Kolañk, M.; Nováková, A.; Flieger, M.; Stodůlkova, E.; Kubátová, A.; Hubka, V. Increasing the species diversity in the Aspergillus section Nidulantes; six novel species mainly from the indoor environment. Mycologia 2020, 112, 342–370. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, E.; Fothergill, A.W.; Brescini, L.; Sutton, D.A.; Marchionni, E.; Orsetti, E.; Staffolani, S.; Catelli, P.; Gesuita, R.; Barchiesi, F. Osteomyelitis caused by Aspergillus species: A review of 310 reported cases. Clin. Microbiol. Infect. 2014, 20, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Chrenkova, V.; Hubka, V.; Cetkovsky, P.; Kouba, M.; Weinbergerova, B.; Lyskova, P.; Hornofova, L.; Hubacek, P. Proven invasive pulmonary aspergillosis in stem cell transplant recipient due to Aspergillus sublatus, a cryptic species of A. nidulans. Mycopathologia 2018, 183, 423–429. [Google Scholar] [CrossRef]
- Seyedmousavi, S.; Lionakis, M.S.; Parta, M.; Peterson, S.W.; Kwon-Chung, K.J. Emerging Aspergillus species almost exclusively associated with primary immunodeficiens. Open Forum Infect. Dis. 2018, 5, ofy213. [Google Scholar] [CrossRef]
- Tavakoli, M.; Rivero-Menendez, O.; Abastabar, M.; Hedayatu, M.T.; Sabino, R.; Siopi, M.; Zarrinfar, H.; Nouripour-Sisakht, S.; van der Lee, H.; Valadan, R.; et al. Genetic diversity and antifungal susceptibility patterns of Aspergillus nidulans complex obtained from clinical and environmental sources. Mycoses 2020, 63, 78–88. [Google Scholar] [CrossRef]
- Blumental, S.; Mouy, R.; Mahlaoui, N.; Bougnoux, M.E.; Debré, M.; Beauté, J.; Lortholary, O.; Blanche, S.; Fischer, A. Invasive mold infections in chronic granulomatous disease. A 25-year retrospective survey. Clin. Infect. Dis. 2011, 53, e159–e169. [Google Scholar] [CrossRef]
- King, J.; Henriet, S.S.V.; Warris, A. Aspergillosis in chronic granulomatous disease. J. Fungi 2016, 2, 15. [Google Scholar] [CrossRef]
- Khalid, M.; Ali, S.A. Fungal osteomyelitis in a patient with chronic granulomatous disease: Case report and review of the literature. JPMA 2018, 68, 1387–1390. [Google Scholar]
- van de Veerdonk, F.L.; Gresnigt, M.S.; Romani, L.; Netea, M.G.; Latge, J.P. Aspergillus fumigatus morphology and dynamic host interactions. Nat. Rev. Microbiol. 2017, 15, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Kosmidis, C.; Denning, D.W. The clinical spectrum of pulmonary aspergillosis. Thorax 2015, 70, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Latgé, J.P.; Chamilos, G. Aspergillus fumigatus and aspergillosis in 2019. Clin. Microbiol. Rev. 2020, 33, e00140-18. [Google Scholar] [CrossRef]
- Kanj, A.; Abdallah, N.; Soubani, A.O. The spectrum of pulmonary aspergillosis. Respir. Med. 2018, 141, 121–131. [Google Scholar] [CrossRef]
- Bongomin, F.; Gago, S.; Oladele, R.; Denning, D. Global and multi-national prevalence of fungal diseases-estimate precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef]
- Burks, C.; Darby, A.; Gomez Londoño Momany, M.; Brewer, M.T. Azole-resistant Aspergillus fumigatus in the environment: Identifying key reservoirs and hotspots of antifungal resistance. PLoS Pathog. 2021, 17, e1009711. [Google Scholar] [CrossRef]
- Mastella, G.; Rainisio, M.; Harms, H.K.; Hodson, M.E.; Koch, C.; Navarro, J.; Strandvik, B.; McKenzie, S.G. Allergic bronchopulmonary aspergillosis in cystic fibrosis. A European epidemiological study, epidemiologic registry of cystic fibrosis. Eur. Respir. J. 2000, 16, 464–471. [Google Scholar] [CrossRef]
- Dave, V.P.; Pappuru, R.; Pathengay, A.; Gupta, R.; Joseph, J.; Sharma, S.; Das, T. Aspergillus endophthalmitis and factors determining outcomes. Asia-Pac. J. Ophtalmol. 2020, 9, 9–13. [Google Scholar] [CrossRef]
- Salmanton-Garcia, J.; Sprute, R.; Stemler, J.; Bartoletti, M.; Dupont, D.; Valerio, M.; Garcia-Vidal, C.; Falces-Romero, I.; Machado, M.; de la Villa, S.; et al. COVID-19 associated pulmonary aspergillosis, March-August 2020. Emerg. Infect. Dis. 2021, 27, 1077–1086. [Google Scholar] [CrossRef]
- Cramer, R.A.; Rivera, A.; Hohl, T.M. Immune responses against Aspergillus fumigatus: What we have learned? Curr. Opin. Infect. Dis. 2011, 24, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, A.; Porcher, R.; Sulahian, A.; de Bazelaire, C.; Chagnon, K.; Raffoux, E.; Vekhoff, A.; Cornet, M.; Isnard, F.; Brethon, B.; et al. The strategy for the diagnoss of invasive pulmonary aspergillosis should depend on both the underlying condition and the leukocyte count of patients with hematologic malignancies. Blood 2012, 119, 1831–1837. [Google Scholar] [CrossRef] [PubMed]
- Jenks, J.D.; Mehta, S.R.; Taplitz, R.; Aslam, S.; Reed, S.L.; Hoenigl, M. Point of care diagnosis of invasive aspergillosis in non-neutropenic patients: Aspergillus galactomannan lateral flow assay versus Aspergillus specific lateral flow device test in bronchoalveolar lavage. Mycoses 2019, 62, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Meis, J.F.; Chowdhary, A.; Rhodes, J.L.; Fisher, M.C.; Verweij, P.E. Clinical implications of globally emerging azole resistance in Aspergillus fumigatus. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20150460. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and update of the consensus definitions of invasive fungal disease from the European organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Nucci, M.; Nouer, S.A.; Grazziutti, M.; Kumar, N.S.; Barlogie, B.; Anaissie, E. Probable invasive aspergillosis without prespecified radiologic findings: Proposal for inclusion of a new category of aspergillosis and implications for studying novel therapies. Clin. Infect. Dis. 2010, 51, 1273–1280. [Google Scholar] [CrossRef]
- Denis, B.; Guiguet, M.; de Castro, N.; Mechai, F.; Revest, M.; Melica, G.; Costagliola, D.; Lortholary, O. Relevance of EORTC criteria for the diagnosis of invasive aspergillosis in HIV-infected patients, and survival trends over a 20-year period in France. Clin. Infect. Dis. 2015, 61, 1273–1280. [Google Scholar] [CrossRef]
- Munoz, P.; Alcala, L.; Sanchez Conde, M.; Palomo, J.; Yáñez, J.; Pelaez, T.; Bouza, E. The isolation of Aspergillus fumigatus from respiratory tract specimens in heart transplant recipients is highly predictive of invasive aspergillosis. Transplantion 2003, 75, 326–329. [Google Scholar]
- Horvart, J.A.; Dummer, S. The use of respiratory tract cultures in the diagnosis of invasive pulmonary aspergillosis. Am. J. Med. 1996, 100, 171–178. [Google Scholar]
- Heldt, S.; Eigl, S.; Prattes, J.; Flick, H.; Rabensteiner, J.; Prüller, F.; Niedrist, T.; Neumeister, P.; Wölfler, A.; Strohmaier, H.; et al. Levels of interleukin (IL)-6 and IL-8 areelevated in serum and bronchoalveolar lavage fluid of haematological patients with invasive pulmonary aspergillosis. Mycoses 2017, 60, 818–882. [Google Scholar] [CrossRef]
- de Heer, K.; Gerritsen, M.G.; Visser, C.E.; Leeflang, M.M. Galactomannan detection in broncho-alveolar lavage fluid for invasive aspergillosis in immunocompromised patients. Cochrane Database Syst. Rev. 2019, 5, CD012399. [Google Scholar] [CrossRef] [PubMed]
- Eigl, S.; Prattes, J.; Reinwald, M.; Thornton, C.R.; Reischies, F.; Spiess, B.; Neumeister, P.; Zollner-Schwetz, I.; Raggam, R.B.; Flick, H.; et al. Influence of mould-active antifungal treatment on the performance of the Aspergillus-specific bronchoalveolar lavage fluid lateral-flow device test. Int. J. Antimicrob. Agents 2015, 46, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Eigl, S.; Hoenigl, M.; Spiess, B.; Heldt, S.; Prattes, J.; Neumeister, P.; Wolfler, A.; Rabensteiner, J.; Prueller, F.; Krause, R.; et al. Galactomannan testing and Aspergillus PCR in same-day bronchoalveolar lavage and blood samples for diagnosis of invasive aspergillosis. Med. Mycol. 2017, 55, 528–534. [Google Scholar] [PubMed]
- Heldt, S.; Hoenigl, M. Lateral flow assays for the diagnosis of invasive aspergillosis: Current status. Curr. Fungal Infect. Rep. 2017, 11, 45–51. [Google Scholar] [CrossRef]
- Prattes, J.; Hoenigl, M.; Zinke, S.E.; Heldt, S.; Eigl, S.; Johnson, G.L.; Bustin, S.; Stelzl, E.; Kessler, H.H. Evaluation of the new AspID polymerase chain reaction assay for detection of Aspergillus species: A pilot study. Mycoses 2018, 61, 355–359. [Google Scholar] [CrossRef]
- Reischies, F.M.; Prattes, J.; Pruller, F.; Eigl, S.; List, A.; Wolfler, A.; Buzina, W.; Zollner-Scwetz, I.; Valentin, T.; Rabensteiner, J.; et al. Prognostic potential of 1,3-beta-D-glucan levels in bronchoalveolar lavage fluid samples. J. Infect. 2016, 72, 29–35. [Google Scholar] [CrossRef]
- McCarthy, M.W.; Petraitiene, R.; Walsh, T.J. Nucleic acid amplification methodologies for the detection of pulmonary mold infections. Expert Rev. Mol. Diagn. 2017, 17, 271–279. [Google Scholar] [CrossRef]
- Arvanitis, M.; Anagnostou, T.; Mylonakis, E. Galactomannan and polymerase chain reaction-based screening for invasive aspergillosis among high-risk hematology patients: A diagnostic meta-analysis. Clin. Infect. Dis. 2015, 61, 1263–1272. [Google Scholar] [CrossRef]
- Holt, S.L.; Drew, R.H. Echinocandins: Addressing outstanding questions surrounding treatment of invasive fungal infections. Am. J. Health Syst. Pharm. 2011, 68, 1207–1220. [Google Scholar] [CrossRef]
- Allen, D.; Wilson, D.; Drew, R.; Perfect, J. Azole antifungals: 35 years of invasisive fungal infection management. Expert Rev. Anti Infect. Ther. 2015, 13, 787–798. [Google Scholar] [CrossRef]
- Nett, J.E.; Andes, D.R. Antifungal agents: Spectrum of activity, pharmacology, and clinical indications. Infect. Dis. Clin. N. Am. 2016, 30, 51–83. [Google Scholar] [CrossRef] [PubMed]
- Robbins, N.; Wright, G.D.; Cowen, L.E. Antifungal drugs: The current armamentarium and development of new agents. Microbiol. Spectr. 2016, 4, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Perfect, J.R. The antifungal pipeline: A reality check. Nat. Rev. Drug Discov. 2017, 16, 603–616. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Jenks, J.D.; Mehta, S.R.; Hoenigl, M. Broad spectrum triazoles for invasive mold infections in adults: Which drug and when? Med. Mycol. 2019, 57, S168–S178. [Google Scholar] [CrossRef]
- Elefanti, A.; Mouton, J.W.; Verweij, P.E.; Tsakris, A.; Zerva, L.; Meletiadis, J. Amphotericin B and voriconazole-echinocandin combinations against Aspergillus spp.: Effect of serum on inhibitory and fungicidal interactions. Antimicrob. Agents Chemother. 2013, 57, 4656–4663. [Google Scholar] [CrossRef]
- Aruanno, M.; Giampedakis, E.; Lamoth, F. Echinocandins for the treatment of invasive aspergillosis: From laboratory to bedside. Antimicrob. Agents Chemother. 2019, 63, e00399–e00419. [Google Scholar] [CrossRef]
- Johnson, M.D.; Perfect, J.R. Caspofungin: First approved agent in a new class of antifungals. Expert Opin. Pharmacother. 2003, 4, 807–823. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Cuenca-Estrella, M.; Cantón, E. EUCAST and CLSI: Working together towards a harmonized method for antifungal susceptibility testing. Curr. Fungal Infect. Rep. 2013, 7, 59–67. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs for Antifungal Agents. 2020. Available online: http://www.policlinico.pa.it/portal/pdf/news/CIO/Breakpoint%20EUCAST%20per%20l_interpretazione%20delle%20MIC%20per%20farmaci%20antimicotici%202022.pdf (accessed on 4 February 2020).
- Seo, K.; Akiyoshi, H.; Ohnishi, Y. Alteration of cell wall components leads to amphotericin B resistance in Aspergillus flavus. Microbiol. Immunol. 1999, 4, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.R.; Bicanic, T.; Salim, R.; Hope, W. Liposomal amphotericin B (AmBisome®): A review of the pharmacokinetics, pharmacodynamics, clinical experience and future directions. Drugs 2016, 76, 485–500. [Google Scholar] [CrossRef] [PubMed]
- Blum, G.; Perkhofer, S.; Haas, H.; Schrettl, M.; Würzner, R.; Dierich, M.P.; Lass-Flörl, C. Potential basis for amphotericin B resistance in Aspergillus terreus. Antimicrob. Agents Chemother. 2008, 52, 1553–1555. [Google Scholar] [CrossRef]
- Jukic, E.; Blatzer, M.; Posch, W.; Steger, M.; Binder, U.; Lass-Flörl, C.; Wilflingseder, D. Oxidative stress response tips the balance in Aspergillus terreus amphotericin B resistance. Antimicrob. Agents Chemother. 2017, 61, e00670-17. [Google Scholar] [CrossRef] [PubMed]
- Posch, W.; Blatzer, M.; Wilflingseder, D.; Lass-Flörl, C. Aspergillus terreus: Novel lessons learned on amphotericin B resistance. Med. Mycol. 2018, 56, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Ostrosky-Zeichner, L.; Marr, K.A.; Rex, J.H.; Cohen, S.H. Amphotericin B: Time for a new “gold standard”. Clin. Infect. Dis. 2003, 37, 415–425. [Google Scholar]
- Reichert-Lima, F.; Lyra, L.; Pontes, L.; Moretti, M.L.; Pham, C.D.; Lockhart, S.R.; Zaninelli Scrhreiber, A. Surveillance for azoles resistance in Aspergillus spp. highlights a high number of amphotericin B-resistant isolates. Mycoses 2018, 61, 360–365. [Google Scholar] [CrossRef]
- Hadrich, I.; Makni, F.; Neji, S.; Cheikhrouhou, F.; Bellaaj, H.; Elloumi, M.; Ayadi, A.; Ranque, S. Amphotericin B in vitro resistance is associated with fatal Aspergillus flavus infection. Med. Mycol. 2012, 50, 829–834. [Google Scholar] [CrossRef]
- Rudramurthy, S.M.; Chakrabarti, A.; Geertsen, E.; Mouton, J.W.; Meis, J.F. In vitro activity of isavuconazole against 208 Aspergillus flavus isolates in comparison with 7 other antifungal agents: Assessment according to the methodology of the European Committee on Antimicrobial Susceptibility Testing. Diagn. Microbiol. Infect. Dis. 2011, 71, 370–377. [Google Scholar] [CrossRef]
- Gonçalves, S.S.; Stchigel, A.M.; Cano, J.; Guarro, J.; Colombo, A.L. In vitro antifungal susceptibility of clinically relevant species belonging to Aspergillus section Flavi. Antimicrob. Agents Chemother. 2013, 57, 1944–1947. [Google Scholar] [CrossRef]
- Gray, K.C.; Palacios, D.S.; Dailey, I.; Endo, M.M.; Uno, B.E.; Wilcock, B.C.; Burke, M.D. Amphotericin primarily kills yeast by simply binding ergosterol. Proc. Natl. Acad. Sci. USA 2012, 109, 2234–2239. [Google Scholar] [CrossRef] [PubMed]
- Fakhim, H.; Badali, H.; Dannaoui, E.; Nasirian, M.; Jahangiri, F.; Raei, M.; Vaseghi, N.; Ahmaadikia, K.; Vaezi, A. Trends in the prevalence of amphotericin B resistance (AmBR) among clinical isolates of Aspergillus species. J. Mycol. Med. 2022, 32, 101310. [Google Scholar] [CrossRef]
- Balajee, S.A.; Gribskov, J.L.; Hanley, E.; Nickle, D.; Marr, K.A. Aspergillus lentulus sp. nov., a new sibling species of A. fumigatus. Eukaryot. Cell 2005, 4, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Azzola, A.; Passweg, J.; Habicht, J.; Bubendorf, L.; Tamm, M.; Gratwohl, A.; Eich, G. Use of lung resection and voriconazole for successful treatment of invasive pulmonary Aspergillus ustus infection. J. Clin. Microbiol. 2004, 42, 4805–4808. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, D.; Watanabe, A.; Kamei, K.; Goldman, G.H. Epidemiological and genomic landscape of azole resistance mechanisms in Aspergillus fungi. Front. Microbiol. 2016, 7, 1382. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; Meis, J.F. Azole-resistant aspergillosis: Epidemiology, molecular mechanisms, and treatment. J. Infect. Dis. 2017, 216, S436–S444. [Google Scholar] [CrossRef] [PubMed]
- Gsaller, F.; Hortschansky, P.; Furukawa, T.; Carr, P.D.; Rash, B.; Capilla, J.; Müller, C.; Bracher, F.; Bowyer, P.; Haas, H.; et al. Sterol biosynthesis and azole tolerance is governed by the opposing actions of SrbA and the CCAAT binding complex. PLoS Pathog. 2016, 12, e1005775. [Google Scholar]
- Bromley, M.; Johns, A.; Davies, E.; Fraczek, M.; Mabey Gilsenan, J.; Kurbatova, N.; Keays, M.; Kapushesky, M.; Gut, M.; Gut, I.; et al. Mitochondrial complex I is a global regulator of secondary metabolism virulence and azole sensitivity in fungi. PLoS ONE 2016, 11, e0158724. [Google Scholar] [CrossRef]
- Misslinger, M.; Gsaller, F.; Hortschansky, P.; Muller, C.; Bracher, F.; Bromley, M.J.; Haas, H. The cytochrome b5 CybE is regulated by iron availability and is crucial for azole resistance in A. fumigatus. Metallomics 2017, 9, 1655–1665. [Google Scholar] [CrossRef]
- Hagiwara, D.; Watanabe, A.; Kamei, K. Sensitisation of an azole resistant Aspergillus fumigatus strain containing the Cyp51A-related mutation by deleting the SrbA gene. Sci. Rep. 2016, 6, 38833. [Google Scholar] [CrossRef]
- Hagiwara, D.; Miura, D.; Shimizu, K.; Paul, S.; Ohba, A.; Gonoi, T.; Watanabe, A.; Kamei, K.; Shintani, T.; Moye-Rowley, W.S.; et al. A novel Zn2-Cys6 transcription factor AtrR plays a key role in an azole resistance mechanism of Aspergillus fumigatus by co-regulating cyp51A and cdr1B expressions. PLoS Pathog. 2017, 13, e1006096. [Google Scholar] [CrossRef] [PubMed]
- Morelli, K.A.; Kerkaert, J.D.; Cramer, R.A. Aspergillus fumigatus biofilms: Toward understanding how growth as a multicellular network increases antifungal resistance and disease progression. PLoS Pathog. 2021, 17, e1009794. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Chowdhary, A.; Melchers, W.J.; Meis, J.F. Azole Resistance in Aspergillus fumigatus: Can We Retain the Clinical Use of Mold-Active Antifungal Azoles? Clin. Infect. Dis. 2016, 62, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Snelders, E.; Kema, G.H.; Mellado, E.; Melchers, W.J. Azole resistance in Aspergillus fumigatus: A side-effect of environmental fungicide use? Lancet Infect. Dis. 2009, 9, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Buil, J.B.; Hare, R.K.; Zwaan, B.J.; Arendrup, M.C.; Melchers, W.J.G.; Verweij, P.E. The fading boundaries between patient and environmental routes of triazole resistance selection in Aspergillus fumigatus. PLoS Pathog. 2019, 15, e1007858. [Google Scholar] [CrossRef] [PubMed]
- Morogovsky, A.; Handelman, M.; Kandil, A.A.; Shadkchan, Y.; Osherov, N. Horizontal gene transfer of triazole resistance in Aspergillus fumigatus. Microbiol. Spectr. 2022, 10, e0111222. [Google Scholar] [CrossRef]
- Hawkins, N.J.; Cools, H.J.; Sierotzki, H.; Shaw, M.W.; Knogge, W.; Kelly, S.L.; Kelly, D.E.; Fraaije, B.A. Paralog re-emergence: A novel, historically contigent mechanism in the evolution of antimicrobial resistance. Mol. Biol. Evol. 2014, 31, 1793–1802. [Google Scholar] [CrossRef]
- Mellado, E.; Diaz-Guerra, T.M.; Cuenca-Estrella, M.; Rodriguez-Tudela, J.L. Identification of two different 14-alpha-sterol-demethylase-related genes (cyp51A and cyp51B) in Aspergillus fumigatus and other Aspergillus species. J. Clin. Microbiol. 2001, 39, 2431–2438. [Google Scholar] [CrossRef]
- Warrilow, A.G.S.; Parker, J.E.; Price, C.L.; Nes, W.D.; Kelly, S.L.; Kelly, D.E. In vitro bio-chemical study of CYP51-mediated azole resistance in Aspergillus fumigatus. Antimicrob. Agents Chemother. 2015, 59, 7771–7778. [Google Scholar] [CrossRef]
- Mann, P.A.; Parmegiani, R.M.; Wei, S.Q.; Mendrick, C.A.; Li, X.; Loebenberg, D.; DiDomenico, B.; Hare, R.S.; Walker, S.S.; McNicholas, P.M. Mutations in Aspergillus fumigatus resulting in reduced susceptibility to posaconazole appear to be restricted to a single amino acid in the cytochrome P450 14 α-demethylase. Antimicrob. Agents Chemother. 2003, 47, 577–581. [Google Scholar] [CrossRef]
- Nascimento, A.M.; Goldman, G.H.; Park, S.; Marras, S.A.E.; Delmas, G.; Oza, U.; Dudley, M.N.; Mann, P.A.; Perlin, D.S. Multiple resistance mechanisms among Aspergillus fumigatus mutants with high-level resistance to itraconazole. Antimicrob. Agents Chemother. 2003, 47, 1719–1726. [Google Scholar] [CrossRef]
- Bader, O.; Weig, M.; Reichard, U.; Lugert, R.; Kuhns, M.; Christner, M.; Hels, J.; Peter, S.; Schumacher, Y.; Bucheidt, D.; et al. cyp51A—Based mechanisms of Aspergillus fumigatus azole drug resistance present in clinical samples from Germany. Antimicrob. Agents Chemother. 2013, 57, 3513–3517. [Google Scholar] [CrossRef] [PubMed]
- Lescar, J.; Meyer, I.; Akshita, K.; Srinivasaraghavan, K.; Verma, C.; Palous, M.; Mazier, D.; Datry, A.; Fekkar, A. Aspergillus fumigatus harbouring the sole Y121F mutation shows decreased susceptibility to voriconazole but maintained susceptibility to itraconazole and posaconazole. J. Antimicrob. Chemother. 2014, 69, 3244–3247. [Google Scholar] [CrossRef] [PubMed]
- Mellado, E.; Garcia-Effron, G.; Alcazar-Fuoli, L.; Cuenca-Estrella, M.; Rodriguez-Tudela, J.L. Substitutions at methionine 220 in the 14 α-sterol demethylase (Cyp51A) of Aspergillus fumigatus are responsible for resistance in vitro to azole antifungal drugs. Antimicrob. Agents Chemother. 2004, 48, 2747–2750. [Google Scholar] [CrossRef]
- Howard, S.J.; Cerar, D.; Anderson, M.J.; Albarrag, A.; Fisher, M.C.; Pasqualotto, A.C.; Arendrup, M.C.; Perlin, D.S.; Denning, D.W. Frequency and evolution of azole resistance in Aspergillus fumigatus associ-ated with treatment failure. Emerg. Infect. Dis. 2009, 15, 1068–1076. [Google Scholar] [CrossRef]
- Albarrag, A.M.; Anderson, M.J.; Howard, S.J.; Robson, G.D.; Warn, P.A.; Sanglard, D.; Denning, D.W. Interrogation of related clinical pan-azole-resistant Aspergillus fumigatus strains: G138C, Y431C, and G434C single nucleotide polymorphisms in cyp51A, upregulation of cyp51A, and integration and activation of transposon Atf1 in the cyp51A promoter. Antimicrob. Agents Chemother. 2011, 55, 5113–5121. [Google Scholar] [CrossRef] [PubMed]
- Dudakova, A.; Spiess, B.; Tangwattanachuleeporn, M.; Sasse, C.; Buchheidt, D.; Weig, M.; Grob, U.; Bader, O. Molecular tools for the detection and deduction of azole antifungal drug resistance phenotypes in Aspergillus species. Clin. Microbiol. Rev. 2017, 30, 1065–1091. [Google Scholar] [CrossRef]
- Mellado, E.; Alcazar-Fuoli, L.; Cuenca-Estrella, M.; Rodriguez-Tudela, J.L. Role of Aspergillus lentulus 14-a sterol demethylase (Cyp51A) in azole drug susceptibility. Antimicrob. Agents Chemother. 2011, 55, 5459–5468. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Cantero, A.; Lopez-Fernandez, L.; Guarro, J.; Capilla, J. Azole resistance mechanisms in Aspergillus: Update and recent advances. Int. J. Antimicrob. Agents 2020, 55, 105807. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.; Manavathu, E.K.; Chandrasekar, P.H. Aspergillus flavus: An emerging non-fumigatus Aspergillus species of significance. Mycoses 2009, 52, 206–222. [Google Scholar] [CrossRef]
- Paul, R.A.; Rudramurthy, S.M.; Meis, J.F.; Mouton, J.W.; Chakrabarti, A. A Novel Y319H substitution in CYP51C associated with azole resistance in Aspergillus flavus. Antimicrob. Agents Chemother 2015, 59, 6615–6619. [Google Scholar] [CrossRef] [PubMed]
- Krishnan-Natesan, S.; Chandrasekar, P.H.; Alangaden, G.J.; Manavathu, E.K. Molecular characterisation of cyp51A and cyp51B genes coding for P450 14 α-lanosterol demethylases A (CYP51Ap) and B (CYP51Bp) from voriconazole-resistant laboratory isolates of Aspergillus flavus. Int. J. Antimicrob. Agents 2008, 32, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Sharma, C.; Kumar, R.; Kumar, N.; Masih, A.; Gupta, D.; Chowdhary, A. Investigation of multiple resistance mechanisms in voriconazole-resistant Aspergillus flavus clinical isolates from a chest hospital surveillance in Delhi. India. Antimicrob. Agents Chemother. 2018, 62, e01928-17. [Google Scholar] [CrossRef] [PubMed]
- Howard, S.J.; Harrison, E.; Bowyer, P.; Varga, J.; Denning, D.W. Cryptic species and azole resistance in the Aspergillus niger complex. Antimicrob. Agents Chemother. 2011, 55, 4802–4809. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Cantero, A.; López-Fernández, L.; Guarro, J.; Capilla, J. New insights into the Cyp51 contribution to azole resistance in Aspergillus section Nigri. Antimicrob. Agents Chemother. 2019, 63, e00543-19. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Cantero, A.; Martin-Vicente, A.; Guarro, J.; Fortwendel, J.R.; Capilla, J. Analysis of the contribution of cyp51 genes to azole resistance in Aspergillus section Nigri with the CRISPR-Cas9 technique. Antimicrob. Agents Chemother. 2021, 65, e01996-20. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Jensen, R.H.; Grif, K.; Skov, M.; Pressler, T.; Johansen, H.K.; Lass-Flörl, C. In vivo emergence of Aspergillus terreus with reduced azole susceptibility and a Cyp51a M217I alteration. J. Infect. Dis 2012, 206, 981–985. [Google Scholar] [CrossRef]
- Zoran, T.; Sartori, B.; Sappl, L.; Aigner, M.; Sánchez-Reus, F.; Rezusta, A.; Chowdhary, A.; Taj-Aldeen, S.J.; Arendrup, M.C.; Oliveri, S.; et al. Azole-resistance in Aspergillus terreus and related species: An emerging problem or a rare phenomenon? Front. Microbiol. 2018, 9, 516. [Google Scholar] [CrossRef]
- Paul, R.A.; Rudramurthy, S.M.; Dhaliwal, M.; Singh, P.; Ghosh, A.K.; Kaur, H.; Varma, S.; Agarwal, R.; Chakrabarti, A. Magnitude of voriconazole resistance in clinical and environmental isolates of Aspergillus flavus and investigation into the role of multidrug efflux pumps. Antimicrob. Agents Chemother. 2018, 62, e01022-18. [Google Scholar] [CrossRef]
- Liu, W.; Sun, Y.; Chen, W.; Liu, W.; Wan, Z.; Bu, D.; Varma, S.; Agarwal, R.; Chakrabarti, A. The T788G mutation in the cyp51C gene confers voriconazole resistance in Aspergillus flavus causing aspergillosis. Antimicrob. Agents Chemother. 2012, 56, 2598–2603. [Google Scholar] [CrossRef]
- Hashimoto, A.; Hagiwara, D.; Watanabe, A.; Yahiro, M. Drug sensitivity and resis-tance mechanism in Aspergillus section Nigri strains from Japan. Antimicrob. Agents Chemother. 2017, 61, e02583-16. [Google Scholar] [CrossRef] [PubMed]
- Price, C.L.; Parker, J.E.; Warrilow, A.G.; Kelly, D.E.; Kelly, S.L. Azole fungicides—Under-standing resistance mechanisms in agricultural fungal pathogens. Pest Manag. Sci. 2015, 71, 1054–1058. [Google Scholar] [CrossRef]
- Hodiamont, C.J.; Dolman, K.M.; Ten Berge, I.J.M.; Melchers, W.J.G.; Verweij, P.E.; Pajkrt, D. Multiple-azole-resistant Aspergillus fumigatus osteomyelitis in a patient with chronic granulomatous disease successfully treated with long-term oral posaconazole and surgery. Med. Mycol. 2009, 47, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; Hagen, F.; Meis, J.F. Exploring azole antifungal drug resis-tance in Aspergillus fumigatus with special reference to resistance mechanisms. Future Microbiol. 2014, 9, 697–711. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.; Abdolrasouli, A.; Dunne, K.; Sewell, T.R.; Zhang, Y.; Ballard, E.; Brackin, A.P.; van Rhijn, N.; Chown, H.; Tsitsopoulou, A.; et al. Population genomics confirms acquisition of drug-resistant Aspergillus fumigatus infection by humans from the environment. Nat. Microbiol. 2022, 7, 663–674. [Google Scholar] [CrossRef]
- Snelders, E.; Camps, S.M.; Karawajczyk, A.; Rijs, A.J.; Zoll, J.; Verweij, P.E.; Melchers, W.J.G. Genotype-phenotype complexity of the TR46/Y121F/T289A cyp51A azole resistance mechanism in Aspergillus fumigatus. Fungal Genet. Biol. 2015, 82, 129–135. [Google Scholar] [CrossRef]
- Garcia-Rubio, R.; Escribano, P.; Gomez, A.; Guinea, J.; Mellado, E. Comparison of two highly discriminatory typing methods to analyze Aspergillus fumigatus azole resistance. Front. Microbiol. 2018, 9, 1626. [Google Scholar] [CrossRef]
- Willger, S.D.; Puttikamonkul, S.; Kim, K.H.; Burritt, J.B.; Grahl, N.; Metzel, L.J.; Barbuch, R.; Bard, M.; Lawrence, C.B.; Cramer, R.A., Jr. A sterol-regulatory element binding protein is required for cell polarity, hypoxia adaptation, azole drug resistance, and virulence in Aspergillus fumigatus. PLoS Pathog. 2008, 4, e1000200. [Google Scholar] [CrossRef]
- Chung, D.; Barker, B.M.; Carey, C.C.; Merriman, B.; Werner, E.R.; Lechner, B.E.; Dhingra, S.; Cheng, C.; Xu, W.; Blosser, S.J.; et al. ChIP-seq and in vivo transcriptome analyses of the Aspergillus fumigatus SREBP SrbA reveals a new regulator of the fungal hypoxia response and virulence. PLoS Pathog. 2014, 10, e1004487. [Google Scholar] [CrossRef]
- Dhingra, S.; Cramer, R.A. Regulation of sterol biosynthesis in the human fungal pathogen Aspergillus fumigatus: Opportunities for therapeutic development. Front. Microbiol. 2017, 8, 92. [Google Scholar] [CrossRef]
- Camps, S.M.T.; Dutilh, B.E.; Arendrup, M.C.; Rijs, A.J.M.M.; Snelders, E.; Huynen, M.A.; Melchers, W.J.G. Discovery of a hapE mutation that causes azole resistance in Aspergillus fumigatus through whole genome sequencing and sexual crossing. PLoS ONE 2012, 7, e50034. [Google Scholar] [CrossRef]
- Paul, S.; Stamnes, M.; Thomas, G.H.; Liu, H.; Hagiwara, D.; Gomi, K.; Filler, S.G.; Moye-Rowley, W.S. AtrR is an essential determinant of azole resistance in Aspergillus fumigatus. MBio 2019, 10, e02563-18. [Google Scholar] [CrossRef] [PubMed]
- Ukai, Y.; Kuroiwa, M.; Kurihara, N.; Naruse, H.; Homma, T.; Maki, H.; Naito, A. Contributions of yap1 mutation and subsequent atrF upregulation to voriconazole resistance in Aspergillus flavus. Antimicrob. Agents Chemother. 2018, 62, e01216-18. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Zhang, Y.; Lu, L. The molecular mechanism of azole resistance in Aspergillus fumigatus: From bedside to bench and back. J. Microbiol. 2015, 53, 91–99. [Google Scholar] [CrossRef]
- Law, C.J.; Maloney, P.C.; Wang, D.N. Ins and outs of major facilitator superfamily antiporters. Ann. Rev. Microbiol. 2008, 62, 289–305. [Google Scholar] [CrossRef] [PubMed]
- Fraczek, M.G.; Bromley, M.; Buied, A.; Moore, C.B.; Rajendran, R.; Rautemaa, R.; Rautemaa, R.; Ramage, G.; Denning, D.W.; Bowyer, P. The cdr1B efflux transporter is associated with non-cyp51a -mediated itraconazole resistance in Aspergillus fumigatus. J. Antimicrob. Chemother. 2013, 68, 1486–1496. [Google Scholar] [CrossRef]
- Paul, S.; Diekema, D.; Moye-Rowley, W.S. Contributions of both ATP-binding cassette transporter and Cyp51A proteins are essential for azole resistance in Aspergillus fumigatus. Antimicrob. Agents Chemother. 2017, 61, e02748-16. [Google Scholar] [CrossRef]
- Meneau, I.; Coste, A.T.; Sanglard, D. Identification of Aspergillus fumigatus multidrug transporter genes and their potential involvement in antifungal resistance. Med. Mycol. 2016, 54, 616–627. [Google Scholar] [CrossRef]
- Arastehfar, A.; Lass-Flörl, C.; Garcia-Rubio, R.; Daneshnia, F.; Ilkit, M.; Boekhout, T.; Gabaldon, T.; Perlin, D.S. The quiet and underappreciated rise of drug-resistant invasive fungal pathogens. J. Fungi 2020, 6, 138. [Google Scholar] [CrossRef]
- Jimenez-Ortigosa, C.; Moore, C.; Denning, D.W.; Perlin, D.S. Emergence of echinocandin resistance due to a point mutation in the fks1 gene of Aspergillus fumigatus in a patient with chronic pulmonary aspergillosis. Antimicrob. Agents Chemother. 2017, 61, e01277. [Google Scholar] [CrossRef]
- Satish, S.; Jimenez-Ortigosa, C.; Zhao, Y.; Lee, M.H.; Dolgov, E.; Krüger, T.; Park, S.; Denning, D.W.; Kniemeyer, O.; Brakhage, A.A.; et al. Stress-induced changes in the lipid microenvironment of β-(1,3)-d-glucan synthase cause clinically important echinocandin resistance in Aspergillus fumigatus. MBio 2019, 10, e00779–e00819. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, R.E.; Souteropoulos, P.; Park, S.; Perlin, D.S. Characterization of Aspergillus fumigatus mutants with reduced susceptibility to caspofungin. Med. Mycol. 2005, 43, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.P.; Miranda, I.M.; Branco, J.; Oliveira, P.; Faria-Ramos, I.; Silva, R.M.; Rodrigues, A.G.; Costa-de-Oliveira, S. FKS1 mutation associated with decreased echinocandin susceptibility of Aspergillus fumigatus following anidulafungin exposure. Sci. Rep. 2020, 10, 11976. [Google Scholar] [CrossRef] [PubMed]
- Yassin, Z.; Loftali, E.; Khourgami, M.R.; Omidi, N.; Fattahi, A.; Nasrollahi, S.A.; Ghasemi, R. Caspofungin resistance in clinical Aspergillus flavus isolates. J. Mycol. Med. 2021, 31, 1011166. [Google Scholar] [CrossRef] [PubMed]
- Colozza, C.; Posteraro, B.; Santilli, S.; De Carolis, E.; Sanguinetti, M.; Girmenia, C. In vitro activities of amphotericin B and AmBisome against Aspergillus isolates recovered from Italian patients treated for haematological malignancies. Int. J. Antimicrob. Agents 2012, 39, 440–443. [Google Scholar] [CrossRef]
- Arabatzis, M.; Kambouris, M.; Kyprianou, M.; Chrysaki, A.; Foustoukou, M.; Kanellopoulou, M.; Kondylo, L.; Kouppari, G.; Koutsia-Karouzou, C.; Lebessi, E.; et al. Polyphasic identification and susceptibility to seven antifungals of 102 Aspergillus isolates recovered from immunocompromised hosts in Greece. Antimicrob. Agents Chemother. 2011, 55, 3025–3030. [Google Scholar] [CrossRef]
- Hendrickx, M.; Beguin, H.; Detandt, M. Genetic re-identification and antifungal susceptibility testing of Aspergillus section Nigri strains of the BCCM/IHEM collection. Mycoses 2012, 55, 148–155. [Google Scholar] [CrossRef]
- Mortensen, K.; Johansen, H.; Fuursted, K.; Knudsen, J.; Gahrn-Hansen, B.; Jensen, R.; Howard, S.J.; Arendrup, M.C. A prospective survey of Aspergillus spp. in respiratory tract samples: Prevalence, clinical impact and antifungal susceptibility. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 1355–1363. [Google Scholar] [CrossRef]
- Vermeulen, E.; Lagrou, K.; Verweij, P.E. Azole resistance in Aspergillus fumigatus: Agrowingpublichealthconcern. Curr. Opin. Infect. Dis. 2013, 26, 493–500. [Google Scholar] [CrossRef]
- Verweij, P.E.; Mellado, E.; Melchers, W.J.G. Multiple-triazole–resistant aspergillosis. N. Engl. J. Med. 2007, 356, 1481–1483. [Google Scholar] [CrossRef]
- Lass-Florl, C.; Mayr, A.; Aigner, M.; Lackner, M.; Orth-Holler, D. A nationwide passive surveillance on fungal infections shows a low burden of azole resistance in molds and yeasts in Tyrol, Austria. Infection 2018, 46, 701–704. [Google Scholar] [CrossRef]
- Sewell, T.R.; Zhang, Y.; Brackin, A.P.; Shelton, J.M.G.; Rhodes, J.; Fisher, M.C. Elevated prevalence of azole-resistant Aspergillus fumigatus in urban versus rural environments in the United Kingdom. Antimicrob. Agents Chemother. 2019, 63, e00548-19. [Google Scholar] [CrossRef] [PubMed]
- Abdolrasouli, A.; Scourfiels, A.; Rhodes, J.; Shah, A.; Elborn, J.S.; Fisher, M.C.; Schelenz, S.; Armstrong-James, D. High prevalence of triazole resistance in clinical Aspergillus fumigatus isolates in a specialist cardiothoracic centre. Int. J. Antimicrob. Agents 2018, 52, 637–642. [Google Scholar] [CrossRef]
- Resendiz-Sharpe, A.; Merckx, R.; Verweij, P.E.; Maertens, J.; Lagrou, K. Stable prevalence of triazole-resistance in Aspergillus fumigatus complex clinical isolates in a Belgian tertiary care center from 2016 to 2020. J. Infect. Chemother. 2021, 27, 1774–1778. [Google Scholar] [CrossRef] [PubMed]
- Simon, L.; Déméautis, T.; Dupont, D.; Krafmer, R.; Garnier, H.; Durieu, I.; Sénéchal, A.; Reix, P.; Couraus, S.; Devouassoux, G.; et al. Azole resistance in Aspergillus fumigatus isolates from respiratory specimens in Lyon University Hospitals, France: Prevalence and mechanisms involved. Int. J. Antimicrob. Agents 2021, 58, 106447. [Google Scholar] [CrossRef] [PubMed]
- Burgel, P.R.; Baixench, M.T.; Amsellem, M.; Audureau, E.; Chapron, J.; Kanaan, R.; Honoré, I.; Doupouy-Camet, J.; Dusser, D.; Klaassen, C.H.; et al. High prevalence of azole-resistant Aspergillus fumigatus in adults with cystic fibrosis exposed to itraconazole. Antimicrob. Agents Chemother. 2012, 56, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Lavergne, R.A.; Morio, F.; Danner-Boucher, I.; Horeau-Langlard, D.; David, V.; Hagen, F.; Meis, J.F.; Le Pape, P. One year prospective survey of azole resistance in Aspergillus fumigatus at a French cystic fibrosis reference centre: Prevalence and mechanisms of resistance. J. Antimicrob. Chemother. 2019, 74, 1884–1889. [Google Scholar] [CrossRef]
- Guegan, H.; Prat, E.; Robert-Gangneux, F.; Gangneux, J.P. Azole Resistance in Aspergillus fumigatus: A Five-Year Follow Up Experience in a Tertiary Hospital With a Special Focus on Cystic Fibrosis. Front. Cell. Infect. Microbiol. 2021, 10, 613774. [Google Scholar] [CrossRef]
- Risum, M.; Hare, R.K.; Gertsen, J.B.; Kristensen, L.; Rosevinge, F.S.; Sulim, S.; Abou-Chakra, N.; Bangsborg, J.; Løwe Røder, B.; Marmolin, E.S.; et al. Azole resistance in Aspergilllus fumigatus. The first 2-year’s data from the Danish national surveillance study, 2018–2020. Mycoses 2022, 65, 419–428. [Google Scholar] [CrossRef]
- Hare, R.K.; Gertsen, J.B.; Astvad, K.M.T.; Degn, K.B.; Løkke, A.; Stegger, M.; Andersenm, P.S.; Kristensen, L.; Arendrup, M.C. In vivo selection of a unique tandem repeat mediated azole resistance mechanism (TR120) in Aspergillus fumigatus cyp51A, Denmark. Emerg. Infect. Dis. 2019, 25, 577–580. [Google Scholar] [CrossRef]
- Pinto, E.; Monteiro, C.; Maia, M.; Faria, M.A.; Lopes, V.; Lameiras, C.; Pinheiro, D. Aspergillus Species and Antifungals Susceptibility in Clinical Setting in the North of Portugal: Cryptic Species and Emerging Azoles Resistance in A. fumigatus. Front. Microbiol. 2018, 9, 1656. [Google Scholar] [CrossRef]
- Lestrade, P.P.A.; Buil, J.B.; van der Beek, T.; Kuijper, E.J.; van Dijk, K.; Kampinga, G.A.; Rijnders, B.J.; Vonk, A.G.; de Greeff, S.C.; Schoffelen, A.F.; et al. Paradoxal trends in azole-resistant Aspergillus fumigatus in a national multicenter surveillance program, the Netherlands, 2013–2018. Emerg. Infect. Dis. 2020, 26, 1447–1455. [Google Scholar] [CrossRef] [PubMed]
- Siopi, M.; Rivero-Menendez, O.; Gkotsis, G.; Panara, A.; Thomaisis, N.; Alastruey-Izquierdo, A.; Pournaras, S.; Meletiadis, J. Nationwide surveillance of azole-resistant Aspergillus fumigatus environmental isolates in Greece. Detection of pan-azole resistance associated with the TR46/Y121F/T289A cyp51A mutation. J. Antimicrob. Chemother. 2020, 75, 3181–3188. [Google Scholar] [CrossRef]
- Escribano, P.; Rodriguez-Sanchez, B.; Diaz-Garcia, J.; Martin-Gomez, M.T.; Ibáñez-Martinez, E.; Rodriguez-Mayo, M.; Peláez, T.; García-Gómez de la Pedrosa, E.; Tejero-García, R.; Marimón, J.M.; et al. Azole resistance survey on clinical Aspergillus fumigatus isolates in Spain. Clin. Microbiol. Infect. 2021, 27, 1170. [Google Scholar] [CrossRef] [PubMed]
- Riat, A.; Plojoux, J.; Gindro, K.; Schrenzel, J.; Sanglard, D. Azole resistance of environmental and clinical Aspergillus fumigatus isolates from Switzerland. Antimicrob. Agents Chemother. 2018, 62, e02088-17. [Google Scholar] [CrossRef] [PubMed]
- Prigitano, A.; Esposto, M.C.; Grancini, A.; Biffi, A.; Innocenti, P.; Cavanna, C.; Lallitto, F.; Mollaschi, E.M.G.; Bandettini, R.; Oltolini, C.; et al. Azole resistance in Aspergillus isolates by different types of patients and correlation with environment—An Italian prospective multicentre study (ARiA study). Mycoses 2021, 64, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Seufert, R.; Sedlacek, L.; Kahl, B.; Hogardt, M.; Hamprecht, A.; Haase, G.; Gunzer, F.; Haas, A.; Grauling-Halama, S.; MacKenzie, C.R.; et al. Prevalence and characterization of azole-resistant Aspergillus fumigatus in patients with cystic fibrosis: A prospective multicentre study in Germany. J. Antimicrob. Chemother. 2018, 73, 2047–2053. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).