

Risk Factors for Hepatitis E Virus Infection and Eating Habits in Kidney Transplant Recipients

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population, Clinical and Laboratory Data
2.2. Data Collection of Food Habits
2.3. Serologic and Molecular Diagnostics and Genotyping of Hepatitis E Infection
2.4. Assessment of Liver Stiffness
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics of KTRs with HEV Infection and Controls
3.2. Risk Factors for Persisting Hepatitis E Viremia with Subsequent RBV Treatment versus Viral Clearance without RBV Treatment
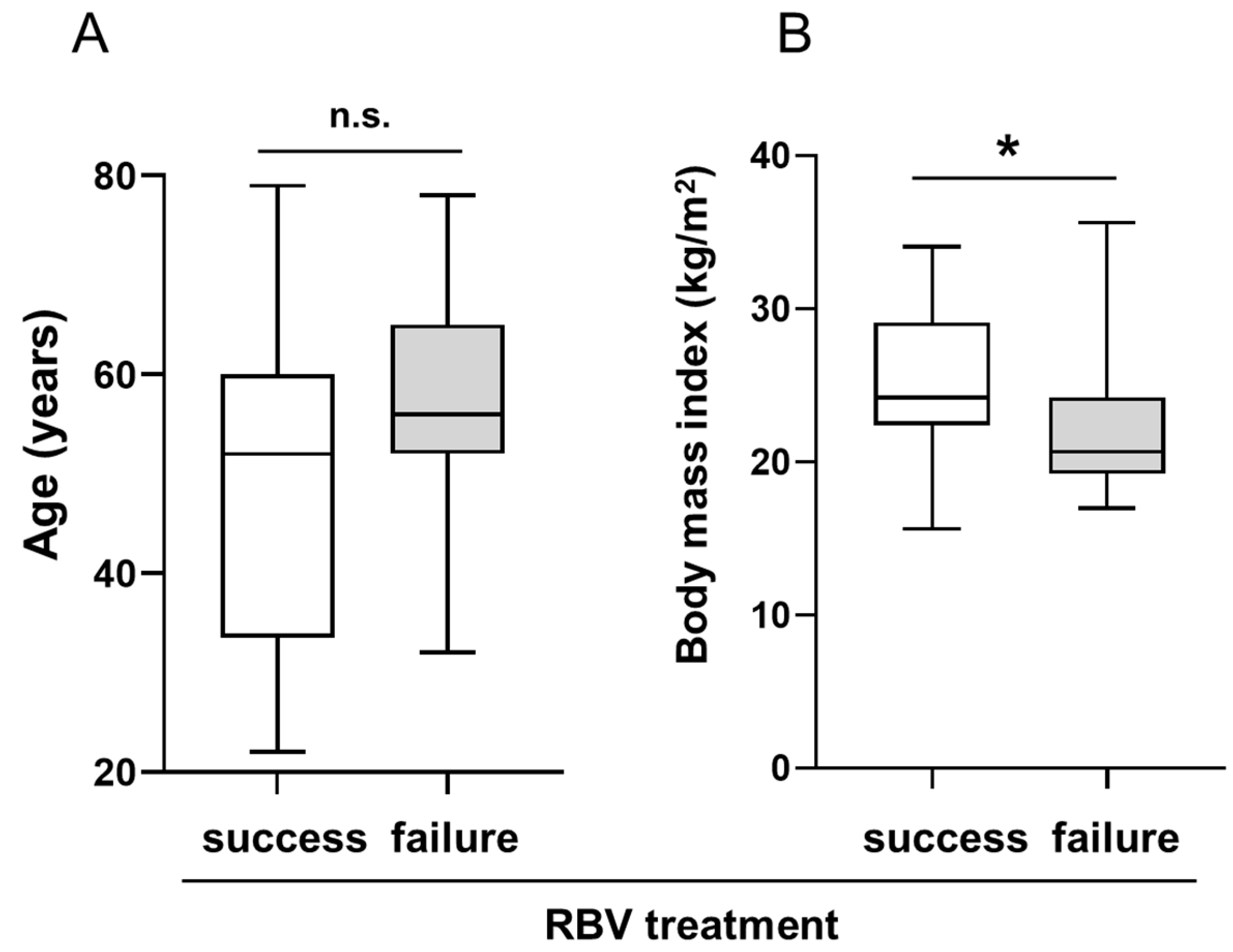
3.3. Risk Factors for RBV Treatment Failure
3.4. Eating Habits of KTRs with or without HEV Infection
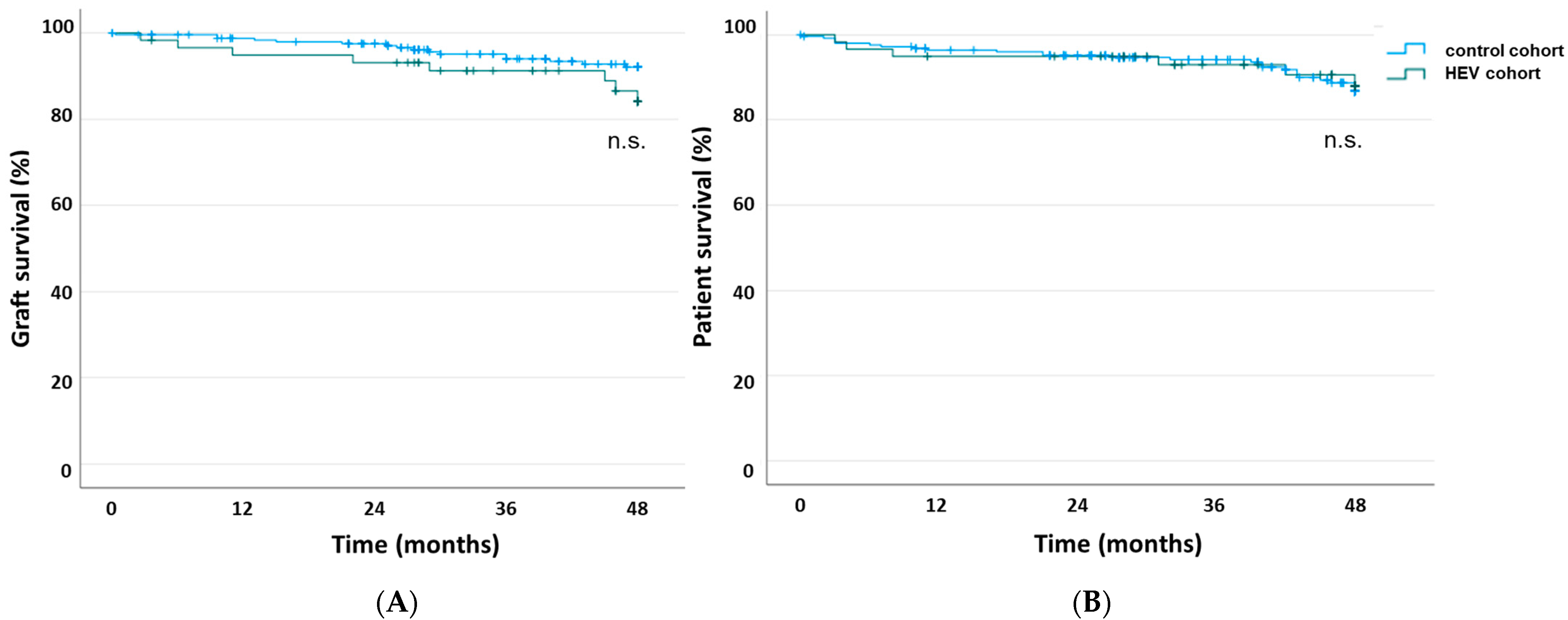
3.5. LongTerm Follow-Up and Allograft Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoofnagle, J.H.; Nelson, K.E.; Purcell, R.H. Hepatitis E. N. Engl. J. Med. 2012, 367, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; LegrandAbravanel, F.; Izopet, J.; Rostaing, L. Hepatitis E virus: What transplant physicians should know. Am. J. Transplant. 2012, 12, 2281–2287. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Mansuy, J.M.; Cointault, O.; Selves, J.; Abravanel, F.; Danjoux, M.; Otal, P.; Esposito, L.; Durand, D.; Izopet, J.; et al. Hepatitis E virusrelated cirrhosis in kidney and kidneypancreastransplant recipients. Am. J. Transplant. 2008, 8, 1744–1748. [Google Scholar] [CrossRef]
- Choi, M.; Hofmann, J.; Kohler, A.; Wang, B.; Bock, C.T.; Schott, E.; Reinke, P.; Nickel, P. Prevalence and Clinical Correlates of Chronic Hepatitis E Infection in German Renal Transplant Recipients With Elevated Liver Enzymes. Transplant. Direct 2018, 4, e341. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Garrouste, C.; Haagsma, E.B.; Garrigue, V.; Pischke, S.; Chauvet, C.; Dumortier, J.; Cannesson, A.; CassutoViguier, E.; Thervet, E.; et al. Factors associated with chronic hepatitis in patients with hepatitis E virus infection who have received solid organ transplants. Gastroenterology 2011, 140, 1481–1489. [Google Scholar] [CrossRef] [PubMed]
- Aslan, A.T.; Balaban, H.Y. Hepatitis E virus: Epidemiology, diagnosis, clinical manifestations, and treatment. World J. Gastroenterol. 2020, 26, 5543–5560. [Google Scholar] [CrossRef] [PubMed]
- Dalton, H.R.; Kamar, N. Treatment of hepatitis E virus. Curr. Opin. Infect. Dis. 2016, 29, 639–644. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Behrendt, P.; Hofmann, J.; Pageaux, G.P.; Barbet, C.; Moal, V.; Couzi, L.; Horvatits, T.; De Man, R.A.; et al. Ribavirin for Hepatitis E Virus Infection After Organ Transplantation: A Large European Retrospective Multicenter Study. Clin. Infect. Dis. 2020, 71, 1204–1211. [Google Scholar] [CrossRef]
- Kamar, N.; Izopet, J.; Tripon, S.; Bismuth, M.; Hillaire, S.; Dumortier, J.; Radenne, S.; Coilly, A.; Garrigue, V.; D’Alteroche, L.; et al. Ribavirin for chronic hepatitis E virus infection in transplant recipients. N. Engl. J. Med. 2014, 370, 1111–1120. [Google Scholar] [CrossRef] [Green Version]
- Kramer, P.; ten Kate, F.W.; Bijnen, A.B.; Jeekel, J.; Weimar, W. Recombinant leucocyte interferon A induces steroidresistant acute vascular rejection episodes in renal transplant recipients. Lancet 1984, 323, 989–990. [Google Scholar] [CrossRef]
- Magnone, M.; Holley, J.L.; Shapiro, R.; Scantlebury, V.; McCauley, J.; Jordan, M.; Vivas, C.; Starzl, T.; Johnson, J.P. Interferonalphainduced acute renal allograft rejection. Transplantation 1995, 59, 1068–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weclawiack, H.; Kamar, N.; Mehrenberger, M.; GuilbeauFrugier, C.; Modesto, A.; Izopet, J.; Ribes, D.; Sallusto, F.; Rostaing, L. Alphainterferon therapy for chronic hepatitis C may induce acute allograft rejection in kidney transplant patients with failed allografts. Nephrol. Dial. Transplant. 2008, 23, 1043–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornberg, M.; Pischke, S.; Muller, T.; Behrendt, P.; Piecha, F.; Benckert, J.; Todt, D.; Steinmann, E.; Papkalla, A.; von Karpowitz, M.; et al. Sofosbuvir monotherapy fails to achieve HEV RNA elimination in patients with chronic hepatitis E—The HepNet SofE pilot study. J. Hepatol. 2020, 73, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Colson, P.; Borentain, P.; Queyriaux, B.; Kaba, M.; Moal, V.; Gallian, P.; Heyries, L.; Raoult, D.; Gerolami, R. Pig liver sausage as a source of hepatitis E virus transmission to humans. J. Infect. Dis. 2010, 202, 825–834. [Google Scholar] [CrossRef] [Green Version]
- RiveiroBarciela, M.; Minguez, B.; Girones, R.; RodriguezFrias, F.; Quer, J.; Buti, M. Phylogenetic demonstration of hepatitis E infection transmitted by pork meat ingestion. J. Clin. Gastroenterol. 2015, 49, 165–168. [Google Scholar] [CrossRef]
- Wichmann, O.; Schimanski, S.; Koch, J.; Kohler, M.; Rothe, C.; Plentz, A.; Jilg, W.; Stark, K. Phylogenetic and casecontrol study on hepatitis E virus infection in Germany. J. Infect. Dis. 2008, 198, 1732–1741. [Google Scholar] [CrossRef] [Green Version]
- Faber, M.; Askar, M.; Stark, K. Casecontrol study on risk factors for acute hepatitis E in Germany, 2012 to 2014. Euro Surveill. 2018, 23, 1700469. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, D.; Osmanodja, B.; Pfefferkorn, M.; Graf, V.; Raschke, D.; Duettmann, W.; Naik, M.G.; Gethmann, C.J.; Mayrdorfer, M.; Halleck, F.; et al. TBase—An Integrated Electronic Health Record and Research Database for Kidney Transplant Recipients. J. Vis. Exp. 2021. [Google Scholar] [CrossRef]
- Kamar, N.; Rostaing, L.; LegrandAbravanel, F.; Izopet, J. How should hepatitis E virus infection be defined in organtransplant recipients? Am. J. Transplant. 2013, 13, 1935–1936. [Google Scholar] [CrossRef]
- Papp, C.P.; Biedermann, P.; Harms, D.; Wang, B.; Kebelmann, M.; Choi, M.; Helmuth, J.; Corman, V.M.; Thurmer, A.; Altmann, B.; et al. Advanced sequencing approaches detected insertions of viral and human origin in the viral genome of chronic hepatitis E virus patients. Sci. Rep. 2022, 12, 1720. [Google Scholar] [CrossRef]
- Schulz, M.; Choi, M.; Bachmann, F.; Koch, N.; Holtmann, T.M.; Mohr, R.; Tacke, F.; Wree, A. Shear wave elastographybased liver fibrosis assessment in patients with chronic hepatitis E displays elevated liver stiffness regardless of previous antiviral therapy. Quant. Imaging Med. Surg. 2022, 12, 3528–3538. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; FriedrichRust, M.; Gilja, O.H.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Long Version). Ultraschall Med. 2017, 38, e16–e47. [Google Scholar] [CrossRef] [Green Version]
- Ferraioli, G.; Filice, C.; Castera, L.; Choi, B.I.; Sporea, I.; Wilson, S.R.; Cosgrove, D.; Dietrich, C.F.; Amy, D.; Bamber, J.C.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 3: Liver. Ultrasound Med. Biol. 2015, 41, 1161–1179. [Google Scholar] [CrossRef] [Green Version]
- Ferraioli, G.; Maiocchi, L.; Dellafiore, C.; Tinelli, C.; Above, E.; Filice, C. Performance and cutoffs for liver fibrosis staging of a twodimensional shear wave elastography technique. Eur. J. Gastroenterol. Hepatol. 2021, 33, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Sandrin, L.; Fourquet, B.; Hasquenoph, J.M.; Yon, S.; Fournier, C.; Mal, F.; Christidis, C.; Ziol, M.; Poulet, B.; Kazemi, F.; et al. Transient elastography: A new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med. Biol. 2003, 29, 1705–1713. [Google Scholar] [CrossRef]
- Schemmerer, M.; Wenzel, J.J.; Stark, K.; Faber, M. Molecular epidemiology and genotypespecific disease severity of hepatitis E virus infections in Germany, 2010–2019. Emerg. Microbes Infect. 2022, 11, 1754–1763. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Abravanel, F.; Selves, J.; Garrouste, C.; Esposito, L.; Lavayssiere, L.; Cointault, O.; Ribes, D.; Cardeau, I.; Nogier, M.B.; et al. Influence of immunosuppressive therapy on the natural history of genotype 3 hepatitisE virus infection after organ transplantation. Transplantation 2010, 89, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; Biedermann, P.; Bock, C.T.; Hofmann, J.; Choi, M.; Tacke, F.; Hanitsch, L.G.; Mueller, T. RituximabContaining Treatment Regimens May Imply a LongTerm Risk for DifficultToTreat Chronic Hepatitis E. Int. J. Environ. Res. Public. Health 2020, 17, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alnuaimi, K.; Lavole, J.; LascouxCombes, C.; Roque Afonso, A.M.; Sogni, P.; Pol, S.; Mallet, V. Chronic hepatitis E in patients with indolent lymphoma after treatment with rituximab and bendamustine. Hepatology 2018, 67, 2468–2470. [Google Scholar] [CrossRef] [Green Version]
- FriebusKardash, J.; Eisenberger, U.; Ackermann, J.; Kribben, A.; Witzke, O.; Wenzel, J.; Rohn, H.; Fiedler, M. Prevalence of active hepatitis E virus infection and efficacy of ribavirin treatment in renal allograft recipients. Transpl. Infect. Dis. 2019, 21, e13088. [Google Scholar] [CrossRef]
- Hansrivijit, P.; Trongtorsak, A.; Puthenpura, M.M.; Boonpheng, B.; Thongprayoon, C.; Wijarnpreecha, K.; Choudhury, A.; Kaewput, W.; Mao, S.A.; Mao, M.A.; et al. Hepatitis E in solid organ transplant recipients: A systematic review and metaanalysis. World J. Gastroenterol. 2021, 27, 1240–1254. [Google Scholar] [CrossRef] [PubMed]
- Puttini, C.; Riccio, M.L.; Redi, D.; Tordini, G.; Cenerini, M.; Romanello, F.; De Luca, A.; Carmellini, M.; Fossombroni, V.; Cusi, M.G.; et al. Seroprevalence of hepatitis E virus (HEV) infection in blood donors and renal transplant recipients: A retrospective study from central Italy. Infez. Med. 2015, 23, 253–256. [Google Scholar] [PubMed]
- Capai, L.; Masse, S.; Gallian, P.; Souty, C.; Isnard, C.; Blanchon, T.; Peres, B.; de Lamballerie, X.; Charrel, R.; Falchi, A. Seroprevalence Study of AntiHEV IgG among Different Adult Populations in Corsica, France, 2019. Microorganisms 2019, 7, 460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izopet, J.; Labrique, A.B.; Basnyat, B.; Dalton, H.R.; Kmush, B.; Heaney, C.D.; Nelson, K.E.; Ahmed, Z.B.; Zaman, K.; Mansuy, J.M.; et al. Hepatitis E virus seroprevalence in three hyperendemic areas: Nepal, Bangladesh and southwest France. J. Clin. Virol. 2015, 70, 39–42. [Google Scholar] [CrossRef]
- Moal, V.; Legris, T.; Motte, A.; VacherCoponat, H.; Fages, L.; JourdeChiche, N.; Borentain, P.; Jaubert, D.; Gerolami, R.; Colson, P. Systematic serological testing for hepatitis E virus in kidney transplant recipients. J. Clin. Microbiol. 2015, 53, 1523–1530. [Google Scholar] [CrossRef] [Green Version]
- Pankovics, P.; Nemethy, O.; Boros, A.; Par, G.; Szakaly, P.; Reuter, G. Fouryear long (2014–2017) clinical and laboratory surveillance of hepatitis E virus infections using combined antibody, molecular, antigen and avidity detection methods: Increasing incidence and chronic HEV case in Hungary. J. Clin. Virol. 2020, 124, 104284. [Google Scholar] [CrossRef]
- Pas, S.D.; de Man, R.A.; Mulders, C.; Balk, A.H.; van Hal, P.T.; Weimar, W.; Koopmans, M.P.; Osterhaus, A.D.; van der Eijk, A.A. Hepatitis E virus infection among solid organ transplant recipients, the Netherlands. Emerg. Infect. Dis. 2012, 18, 869–872. [Google Scholar] [CrossRef]
- Kamar, N.; Weclawiak, H.; GuilbeauFrugier, C.; LegrandAbravanel, F.; Cointault, O.; Ribes, D.; Esposito, L.; CardeauDesangles, I.; Guitard, J.; Sallusto, F.; et al. Hepatitis E virus and the kidney in solidorgan transplant patients. Transplantation 2012, 93, 617–623. [Google Scholar] [CrossRef]
- Kovvuru, K.; Carbajal, N.; Pakanati, A.R.; Thongprayoon, C.; Hansrivijit, P.; Boonpheng, B.; Pattharanitima, P.; Nissaisorakarn, V.; Cheungpasitporn, W.; Kanduri, S.R. Renal manifestations of hepatitis E among immunocompetent and solid organ transplant recipients. World J. Hepatol. 2022, 14, 516–524. [Google Scholar] [CrossRef]
- ElMokhtar, M.A.; Seddik, M.I.; Osman, A.; Adel, S.; Abdel Aziz, E.M.; Mandour, S.A.; Mohammed, N.; Zarzour, M.A.; AbdelWahid, L.; Radwan, E.; et al. Hepatitis E Virus Mediates Renal Injury via the Interaction between the Immune Cells and Renal Epithelium. Vaccines 2020, 8, 454. [Google Scholar] [CrossRef]
- Ozkok, A.; Yildiz, A. Hepatitis C virus associated glomerulopathies. World J. Gastroenterol. 2014, 20, 7544–7554. [Google Scholar] [CrossRef]
- Marion, O.; Abravanel, F.; Del Bello, A.; Esposito, L.; Lhomme, S.; PuissantLubrano, B.; Alric, L.; Faguer, S.; Izopet, J.; Kamar, N. Hepatitis E virusassociated cryoglobulinemia in solidorgantransplant recipients. Liver Int. 2018, 38, 2178–2189. [Google Scholar] [CrossRef]
- Pischke, S.; Polywka, S.; Haag, F.; IkingKonert, C.; Sterneck, M.; Lutgehetmann, M.; Dammermann, W.; Luth, S.; Schirmer, J.H. Association of hepatitis E virus and essential cryoglobulinemia? J. Clin. Virol. 2015, 67, 23–24. [Google Scholar] [CrossRef]
- Shiina, T.; Nightingale, K.R.; Palmeri, M.L.; Hall, T.J.; Bamber, J.C.; Barr, R.G.; Castera, L.; Choi, B.I.; Chou, Y.H.; Cosgrove, D.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: Basic principles and terminology. Ultrasound Med. Biol. 2015, 41, 1126–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debing, Y.; Gisa, A.; Dallmeier, K.; Pischke, S.; Bremer, B.; Manns, M.; Wedemeyer, H.; Suneetha, P.V.; Neyts, J. A mutation in the hepatitis E virus RNA polymerase promotes its replication and associates with ribavirin treatment failure in organ transplant recipients. Gastroenterology 2014, 147, 1008–1011.e7; quiz e15-6. [Google Scholar] [CrossRef] [PubMed]
- Lhomme, S.; Kamar, N.; Nicot, F.; Ducos, J.; Bismuth, M.; Garrigue, V.; PetitjeanLecherbonnier, J.; Ollivier, I.; AlessandriGradt, E.; Goria, O.; et al. Mutation in the Hepatitis E Virus Polymerase and Outcome of Ribavirin Therapy. Antimicrob. Agents Chemother. 2015, 60, 1608–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unzueta, A.; Valdez, R.; Chang, Y.H.; Desmarteau, Y.M.; Heilman, R.L.; Scott, R.L.; Douglas, D.D.; Rakela, J. Hepatitis E virus serum antibodies and RNA prevalence in patients evaluated for heart and kidney transplantation. Ann. Hepatol. 2016, 15, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Sakulsaenprapha, V.; Wasuwanich, P.; Thawillarp, S.; Ingviya, T.; Phimphilai, P.; Sue, P.K.; Jackson, A.M.; Kraus, E.S.; Tehsale, E.H.; Kamili, S.; et al. Risk factors associated with Hepatitis E virus infection in kidney transplant recipients in a single tertiary Center in the United States. Transpl. Immunol. 2023, 78, 101809. [Google Scholar] [CrossRef]
- Kamar, N.; Lhomme, S.; Abravanel, F.; Cointault, O.; Esposito, L.; CardeauDesangles, I.; Del Bello, A.; Dorr, G.; Lavayssiere, L.; Nogier, M.B.; et al. An Early Viral Response Predicts the Virological Response to Ribavirin in Hepatitis E Virus Organ Transplant Patients. Transplantation 2015, 99, 2124–2131. [Google Scholar] [CrossRef]
- Wallace, S.J.; Swann, R.; Donnelly, M.; Kemp, L.; Guaci, J.; Murray, A.; Spoor, J.; Lin, N.; Miller, M.; Dalton, H.R.; et al. Mortality and morbidity of locally acquired hepatitis E in the national Scottish cohort: A multicentre retrospective study. Aliment. Pharmacol. Ther. 2020, 51, 974–986. [Google Scholar] [CrossRef] [Green Version]
- Pallerla, S.R.; Schembecker, S.; Meyer, C.G.; Linh, L.T.K.; Johne, R.; Wedemeyer, H.; Bock, C.T.; Kremsner, P.G.; Velavan, T.P. Hepatitis E virus genome detection in commercial pork livers and pork meat products in Germany. J. Viral Hepat. 2021, 28, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Szabo, K.; Trojnar, E.; AnheyerBehmenburg, H.; Binder, A.; Schotte, U.; Ellerbroek, L.; Klein, G.; Johne, R. Detection of hepatitis E virus RNA in raw sausages and liver sausages from retail in Germany using an optimized method. Int. J. Food Microbiol. 2015, 215, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, J.J.; Preiss, J.; Schemmerer, M.; Huber, B.; Plentz, A.; Jilg, W. Detection of hepatitis E virus (HEV) from porcine livers in Southeastern Germany and high sequence homology to human HEV isolates. J. Clin. Virol. 2011, 52, 50–54. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristics | KTRs with HEV Infection | KTRs w/o HEV Infection | Statistical Group | Univariable OR (95% CI) |
|---|---|---|---|---|
| N = 59 | N = 251 | Difference, | ||
| N (%) | N (%) | p-Value | ||
| Gender | ||||
| Male | 46 (78.0) | 141 (56.2) | 0.002 | 2.76 (1.42–5.36) |
| Female | 13 (22.0) | 110 (43.8) | ||
| Age | ||||
| Mean (y) | 50.9 ± 15 | 54.5 ± 13.3 | 0.103 | |
| <40 | 16 (27.1) | 41 (16.3) | Reference | |
| 40–60 | 27 (45.8) | 127 (50.6) | 0.063 | 1.91 (0.98–3.70) |
| >60 | 16 (27.1) | 83 (33.1) | 0.439 | 0.75 (0.40–1.42) |
| Renal disease | ||||
| Glomerulonephritis | 20 (33.9) | 66 (26.3) | 0.260 | 1.44 (0.78–2.6) |
| Cystic kidney disease | 7 (11.9) | 44 (17.5) | 0.335 | 0.63 (0.27–1.49) |
| Diabetic nephropathy | 7 (11.9) | 33 (13.1) | 1.000 | 0.89 (0.37–2.12) |
| Hypoplastic kidneys | 4 (6.8) | 13 (5.2) | 0.541 | 1.33 (0.42–4.24) |
| Other | 6 (10.2) | 44 (17.5) | 0.237 | 0.53 (0.22–1.32) |
| Unknown | 16 (27.1) | 44 (17.5) | 0.101 | 1.75 (0.91–3.39) |
| Co-morbidities | ||||
| Hypertension | 47 (79.7) | 201 (80.0) | 1.000 | 0.97 (0.48–1.97) |
| Diabetes mellitus | 14 (23.7) | 69 (27.5) | 0.626 | 0.82 (0.42–1.60) |
| Arteriosclerosis | 19 (32.2) | 64 (25.5) | 0.328 | 1.39 (0.75–2.57) |
| History of cancer | 12 (20.3) | 34 (13.5) | 0.221 | 1.63 (0.79–3.38) |
| Chronic liver disease | 8 (13.6) | 52 (20.7) | 0.272 | 0.60 (0.27–1.34) |
| BMI (kg/m2) | 24.2 ± 4.7 | 25.5 ± 4.9 | 0.114 | |
| Time after transplantation (m) | 93 ± 80 | 92 ± 85 | 0.631 | |
| Type of transplant | 0.688 | |||
| Kidney | 51 (86.4) | 226 (90.0) | ||
| Pancreas–kidney | 5 (8.5) | 17 (6.8) | ||
| Other multi-visceral | 3 (5.1) | 8 (3.2) | ||
| Type of donation | 0.109 | |||
| Postmortem | 41 (69.5) | 186 (74.1) | ||
| Living donation | 12 (20.3) | 54 (21.5) | ||
| ABOi living donation | 6 (10.2) | 9 (3.6) | ||
| Re-transplant | 10 (16.9) | 27 (10.8) | 0.187 | 1.69 (0.77–3.73) |
| Immunosuppressive regimen | ||||
| Tacrolimus | 49 (83.0) | 179 (71.0) | 0.072 | 1.97 (0.95–4.10) |
| Cyclosporine A | 3 (5.1) | 52 (20.7) | 0.004 | 0.21 (0.06–0.68) |
| Mycophenolic acid | 57 (96.6) | 222 (88.4) | 0.088 | 3.72 (0.86–16.07) |
| mTOR inhibitor | 6 (10.2) | 10 (4.0) | 0.093 | 2.73 (0.95–7.84) |
| Steroid | 47 (79.7) | 196 (78.1) | 0.862 | 1.10 (0.55–2.22) |
| Belatacept | 3 (5.1) | 11 (4.4) | 0.735 | 1.17 (0.32–4.33) |
| Triple IS | 45 (76.3) | 176 (70.1) | 0.425 | 1.37 (0.71–2.65) |
| Dual IS | 14 (23.7) | 75 (30.0) | 0.424 | 0.72 (0.38–1.40) |
| Previous treatment of any rejection | 29 (49.2) | 87 (34.7) | 0.051 | 1.82 (1.03–3.23) |
| Use of thymoglobulin | 20 (33.9) | 59 (23.5) | 0.134 | 1.67 (0.90–3.08) |
| Use of high dose steroids | 33 (55.9) | 83 (33.1) | 0.002 | 2.57 (1.44–4.58) |
| Use of rituximab | 10 (16.9) | 14 (5.6) | 0.007 | 3.46 (1.45–8.23) |
| Treatment of aABMR | 7 (11.9) | 6 (2.4) | 0.004 | 5.47 (1.77–18.96) |
| Baseline eGFR | 52 ± 21 | 51 ± 22 | ||
| eGFR at diagnosis (mL/min) | 52 ± 20 | 52 ± 22 | ||
| Creatinine at diagnosis (mg/dL) | 1.58 ± 0.6 | 1.64 ± 0.9 | 0.856 | |
| Baseline proteinuria (mg/g creatinine) * | 344 ± 551 | 302 ± 649 | 0.667 | |
| Peak proteinuria at liver enzyme elevation (mg/g creatinine) | 713 ± 919 | 580 ± 1045 | 0.671 | |
| Rise in proteinuria during observation period | 15/50 (30.0) | 31/215 (14.4) | 0.009 | |
| Liver enzymes | ||||
| ALT max (U/L, ref < 35) | 224 ± 230 | 118 ± 126 | <0.001 | |
| AST max (U/L, ref < 31) | 135 ± 135 | 83 ± 82 | <0.001 | |
| gGT max (U/L, ref 5–36) | 222 ± 175 | 275 ± 381 | 0.948 | |
| Serology | <0.001 | |||
| IgG pos | 56/56 (100) | 80 (31.9) | ||
| IgM pos | 49/56 (87.5) | 11 (4.4) | ||
| IgM and IgG positive | 49/56 (87.5) | 11 (4.4) | ||
| IgM and IgG negative | 0 (0) | 171 (68.1) | ||
| Not done | 3 (5.1) | 0 (0) |
| Variable | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Male sex | 3.19 (1.58–6.43) | 0.001 |
| Previous use of high-dose steroids | 2.13 (1.15–3.94) | 0.016 |
| Previous use of rituximab | 2.96 (1.13−7.75) | 0.027 |
| Use of CyA as maintenance IS | 0.24 (0.07–0.80) | 0.021 |
| Patient Characteristics | Persistent HEV Viremia (RBV-Treated) | Remission Without RBV Treatment | Statistical Group Difference, p-Value | Univariable OR (95% CI) |
|---|---|---|---|---|
| N = 48 | N = 11 | |||
| N (%) | N (%) | |||
| Gender | 0.426 | 0.30 (0.04–2.59) | ||
| Male | 36 (75) | 10 (90.9) | ||
| Female | 12 (25) | 1 (9.1) | ||
| Age | ||||
| Mean (y) | 52 ± 15 | 46 ± 14 | 0.134 | |
| <40 | 12 (25) | 4 (36.4) | Reference | |
| 40–60 | 21 (43.75) | 6 (54.5) | 1.000 | 0.86 (0.20–3.66) |
| >60 | 15 (31.25) | 1 (9.1) | 0.333 | 5.00 (0.49–50.8) |
| Renal disease | ||||
| Glomerulonephritis | 17 (29.2) | 3 (27.3) | 0.734 | 1.46 (0.34–6.25) |
| Cystic kidney disease | 7 (14.6) | 0 (0) | 0.328 | 1.17 (1.04–1.32) |
| Diabetic nephropathy | 5 (10.4) | 2 (18.2) | 0.604 | 0.52 (0.09–3.14) |
| Hypoplastic kidneys | 4 (8.3) | 0 (0) | 1.000 | 1.09 (1.00–1.19) |
| Other | 4 (8.3) | 2 (18.2) | 0.310 | 0.41 (0.07–2.58) |
| Unknown | 12 (25) | 4 (36.4) | 0.468 | 0.58 (0.15–2.35) |
| Co-morbidities | ||||
| Hypertension | 37 (77.1) | 10 (90.9) | 0.431 | 0.34 (0.39–2.93) |
| Diabetes mellitus | 10 (20.8) | 4 (36.4) | 0.432 | 0.46 (0.12–1.89) |
| Arteriosclerosis | 16 (33.3) | 3 (27.3) | 1.000 | 1.33 (0.31–5.72) |
| History of cancer | 11 (22.9) | 1 (9.1) | 0.431 | 2.97 (0.34–25.9) |
| Chronic liver disease | 7 (14.6) | 1 (9.1) | 1.000 | 1.71 (0.19–15.5) |
| BMI (kg/m2) | 24 ± 4.7 | 25 ± 5.0 | 0.350 | |
| Time after transplantation (m) | 96 ± 83 | 80 ± 67 | 0.647 | |
| Type of transplant | 0.329 | |||
| Kidney | 42 (87.5) | 9 (81.2) | ||
| Pancreas–kidney | 3 (6.25) | 2 (18.2) | ||
| Other multi-visceral | 3 (6.25) | 0 (0) | ||
| Type of donation | 0.424 | |||
| Postmortem | 33 (68.75) | 8 (72.3) | ||
| ABOc living donation | 11 (22.9) | 1 (9.1) | ||
| ABOi living donation | 4 (8.3) | 2 (18.2) | ||
| Re-transplantation | 7 (14.6) | 3 (27.3) | 0.376 | 0.46 (0.10–2.15) |
| Immunosuppressive regimen | ||||
| Tacrolimus | 41 (85.4) | 8 (72.7) | 0.376 | 2.20 (0.47–2.15) |
| Cyclosporine | 1 (2.1) | 2 (18.2) | 0.086 | 0.10 (0.08–1.17) |
| Mycophenolic acid | 47 (97.9) | 10 (90.9) | 0.341 | 4.70 (0.27–81.6) |
| mTOR inhibitor | 6 (12.5) | 0 (0) | 0.582 | 1.14 (1.03–1.27) |
| Steroid | 40 (83.3) | 7 (63.6) | 0.209 | 2.86 (0.67–12.1) |
| Belatacept | 2 (4.2) | 1 (9.1) | 0.468 | 0.44 (0.04–5.28) |
| Triple IS | 39 (81.3) | 6 (54.5) | 0.110 | 3.61 (0.90–14.5) |
| Dual IS | 9 (18.8) | 5 (45.5) | 0.110 | 0.28 (0.07–1.11) |
| Reduction/switch of IS after diagnosis | 16 (33.3) | 3 (27.3) | 1.000 | 1.33 (0.31–5.72) |
| Previous treatment of any rejection | 26 (54.2) | 3 (27.3) | 0.181 | 3.15 (0.74–13.4) |
| Use of thymoglobulin | 16 (33.3) | 4 (36.4) | 1.000 | 0.88 (0.22–4.49) |
| Use of high-dose steroids | 29 (60.4) | 4 (36.4) | 0.187 | 2.67 (0.69–10.4) |
| Use of rituximab | 9 (18.8) | 1 (9.1) | 0.670 | 2.31 (0.26–20.4) |
| Treatment of aABMR | 7 (14.6) | 0 (0) | 0.328 | 1.17 (1.04–1.32) |
| eGFR at diagnosis (mL/min) | 47 ± 30 | 48 ± 56 | 0.325 | |
| Creatinine at diagnosis (mg/dL) | 1.6 ± 0.6 | 1.5 ± 0.6 | 0.546 | |
| eGFR during HEV infection | ||||
| Stable | 18 (37.5) | 8 (72.7) | ||
| Deterioration (≥5 mL/min) | 30 (62.5) | 3 (27.3) | 0.046 | |
| Baseline proteinuria (mg/g creatinine) | 361 ± 578 | 72 ± 66 | 0.014 | |
| Peak proteinuria during HEV infection (mg/g creatinine) | 735 ± 959 | 164 ± 376 | 0.008 | |
| Rise in proteinuria during HEV viremia (≥300 mg/g crea) | 15/42 (35.7) | 0/8 (0) | 0.086 | |
| Liver enzymes | ||||
| ALT max (U/L, ref < 35) | 226 ± 249 | 217 ± 120 | 0.414 | |
| AST max (U/L, ref < 31) | 133 ± 138 | 140 ± 130 | 0.869 | |
| gGT max (U/L, ref 5–36) | 233 ± 183 | 169 ± 126 | 0.217 | |
| Max HEV RNA (mio cop/mL) | 1.8 ± 2.1 | 0.7 ± 1.5 | 0.010 | |
| Grade of liver fibrosis | ||||
| 0 | 2 (4.2) | 0 | ||
| 1 | 11 (22.9) | 4 (36.4) | ||
| 2 | 3 (6.25) | 0 | ||
| 3 | 9 (18.75) | 0 | ||
| 4 | 3 (6.25) | 0 | ||
| Not done | 20 (41.7) | 7 (63.4) | ||
| Outcome | ||||
| Time of viremia (d) | 278 ± 203 | 126 ± 104 | 0.002 | |
| (range: min–max) | (84–989) | (21–334) | ||
| Relapse | 17 (29.2) | 0 (0) | 0.040 | 1.59 (1.27–1.98) |
| SVR (>6 m) | 33 (68.75) | 11 (100) | 0.050 |
| Patient Characteristics | RBV Treatment Failure * | RBV Treatment Success | Statistical Group Difference, p-Value | Univariable OR (95% CI) |
|---|---|---|---|---|
| N = 19 | N = 29 | |||
| N (%) | N (%) | |||
| Gender | ||||
| Male | 15 (78.9) | 21 (72.4) | 0.739 | 0.70 (0.18–2.76) |
| Female | 4 (21.1) | 8 (27.6) | ||
| Age | ||||
| Mean (y) | 56.1 ± 13.7 | 49.5 ± 15.7 | 0.054 | |
| <40 | 2 (10.5) | 10 (34.5) | Ref | |
| 40–60 | 8 (42.1) | 13 (44.8) | 0.259 | 3.08 (0.53–17.80) |
| >60 | 9 (47.4) | 6 (20.7) | 0.047 | 7.50 (1.20–47.05) |
| Co-morbidities | ||||
| Hypertension | 16 (84.2) | 21 (72.4) | 0.488 | 2.03 (0.46–8.90) |
| Diabetes mellitus | 5 (26.3) | 5 (17.2) | 0.487 | 1.71 (0.42–6.98) |
| Arteriosclerosis | 9 (47.9) | 7 (24.1) | 0.124 | 2.83 (0.82–9.76) |
| History of cancer | 5 (26.3) | 6 (20.7) | 0.732 | 1.40 (0.35–5.34) |
| Chronic liver disease | 5 (26.3) | 2 (6.9) | 0.097 | 4.82 (0.83–28.1) |
| BMI (kg/m2) | 22.2 ± 4.2 | 25.3 ± 4.7 | 0.019 | |
| BMI ≤ 20 kg/m2 | 8 (42.1) | 3 (10.3) | 0.032 | 5.8 (1.29–26.25) |
| Time after transplantation (m) | 90 ± 83 | 99 ± 85 | 0.524 | |
| Type of transplant | ||||
| Kidney | 16 (84.2) | 26 (89.7) | Ref | |
| Pancreas–kidney | 1 (5.3) | 2 (6.9) | 1.000 | 0.81 (0.07–9.70) |
| Other multi-visceral | 2 (10.5) | 1 (3.4) | 0.555 | 3.25 (0.27–38.81) |
| Immunosuppressive regimen | ||||
| Tacrolimus | 16 (84.2) | 25 (86.2) | 1.000 | 0.85 (0.17–4.33) |
| Cyclosporine A | 0 (0) | 1 (3.4) | 1.000 | 0.60 (0.47–0.75) |
| Mycophenolic acid | 19 (100) | 28 (96.6) | 1.000 | 1.68 (1.33–2.12) |
| mTOR inhibitor | 2 (10.5) | 4 (14.0) | 1.000 | 0.74 (0.12–4.47) |
| Steroids | 17 (89.5) | 23 (79.3) | 0.451 | 2.22 (0.40–12.4) |
| Belatacept | 2 (10.5) | 0 (0) | 0.152 | 2.71 (0.19–3.95) |
| Triple IS | 16 (84.2) | 23 (79.3) | 1.000 | 1.39 (0.30–6.40) |
| Dual IS | 3 (15.8) | 6 (20.7) | 1.000 | 0.72 (0.16–3.31) |
| Previous treatment of any rejection | 8 (42.1) | 18 (62.1) | 0.239 | 2.25 (0.69–7.32) |
| Use of thymoglobulin | 6 (31.6) | 10 (34.5) | 1.000 | 1.14 (0.33–3.92) |
| Use of high-dose steroids | 11 (57.9) | 18 (62.1) | 1.000 | 1.19 (0.37–3.87) |
| Use of rituximab | 4 (21.1) | 5 (17.2) | 1.000 | 0.78 (0.18–3.38) |
| Treatment of aABMR | 2 (10.5) | 5 (17.2) | 0.687 | 1.77 (0.31–10.2) |
| Renal function | ||||
| Creatinine at diagnosis (mg/dL) | 1.6 ± 0.6 | 1.6 ± 0.6 | 0.847 | |
| eGFR at diagnosis (mL/min) | 49 ± 18 | 45 ± 36 | 0.819 | |
| Minimal eGFR at disease (mL/min) | 35 ± 20 | 45 ± 20 | 0.362 | |
| Renal function during HEV viremia | ||||
| Stable | 4 (21.1) | 14 (48.3) | Ref | |
| Deterioration (≥5 mL/min) | 15 (78.9) | 15 (51.7) | 0.073 | 3.5 (0.93–13.13) |
| Baseline proteinuria (mg/g crea) | 253 ± 555 | 432 ± 591 | 0.292 | |
| Peak proteinuria during HEV (mg/g crea) | 1004 ± 1243 | 560 ± 684 | 0.167 | |
| Rise in proteinuria during HEV (≥300 mg/g crea) | 8/16 (50) | 7/26 (26.9) | 0.188 | 2.71 (0.73–10.04) |
| Liver enzymes | ||||
| ALT max (U/L, ref < 35) | 215 ± 256 | 232 ± 249 | 0.829 | |
| AST max (U/L, ref < 31) | 157 ± 105 | 138 ± 127 | 0.927 | |
| gGT max (U/L, ref 5–36) | 248 ± 184 | 224 ± 185 | 0.699 | |
| HEV RNA max (mio cop/mL) | 1.8 ± 2.3 | 1.8 ± 1.9 | 0.558 | |
| Duration of RBV treatment (d) | 471 ± 511.5 | 118 ± 58.5 | <0.001 | |
| (range: min–max) | (45–2155) | (39–310) | ||
| RBV dosage (mg/d) | 363 ± 201 | 381 ± 152 | 0.332 | |
| Hemolytic anemia | 15 (78.9) | 17 (58.6) | 0.111 | 3.53 (0.83–14.9) |
| Side effects of treatment | 18 (95) | 23 (79) | 0.219 | 4.70 (0.52–42.6) |
| Negative HEV PCR 4 weeks after start of treatment | 9 (47) | 20 (69) | 0.120 | 0.32 (0.09–1.10) |
| Remission after last treatment | 13 (68) | 29 (100) | 0.002 | |
| SVR | 4 (21) | 29 (100) | <0.001 |
| Characteristics | RBV Treatment Failure | RBV Treatment Success | Statistical Group Difference, p-Value |
|---|---|---|---|
| N = 19 | N = 29 | ||
| N (%) | N (%) | ||
| Duration of RBV treatment (d) | 471 ± 511.5 | 118 ± 58.5 | <0.001 |
| (range: min–max) | (45–2155) | (39–310) | |
| Mean RBV dosage (mg/d) | 363 ± 201 | 381 ± 152 | 0.332 |
| Median start dose | 300 | 400 | 0.347 |
| (range: min–max) | (200–800) | (200–1000) | |
| Start dose lower than GFR-adapted dosing | 9 (47.4) | 13 (44.8) | 1.000 |
| Increase of dosage | 6 (31.6) | 1 (3.4) | 0.770 |
| - After a mean time of (d) | 204 ± 194 | 14 | 0.500 |
| Reduction of dosage | 6 (31.6) | 7 (24.1) | 0.741 |
| - After a mean time of (d) | 71.5 ± 30.8 | 63.4 ± 43.9 | 0.366 |
| RBV-induced anemia | 15 (78.9) | 17 (58.6) | 0.111 |
| Interruption due to hemolytic anemia | 3 (15.8) | 3 (10.3) | 0.662 |
| - After a mean time of (d) | 113.3 ± 61.1 | 67.7 ± 23.7 | 0.400 |
| EPO treatment before RBV | 7 (36.8) | 11 (37.9) | 1.000 |
| EPO start after RBV | 7 (36.8) | 5 (17.2) | 0.168 |
| - After a mean time of (d) | 67.6 ± 49.5 | 16.0 ± 15.2 | 0.048 |
| Increase in EPO dosage | 12 (63.2) | 14 (48.3) | 0.245 |
| Variable | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Age > 60 years | 4.34 (1.05–17.96) | 0.043 |
| BMI ≤ 20 kg/m2 | 7.73 (1.53–39.05) | 0.013 |
| Patient Characteristics | KTRs with HEV Infection N = 40 N (%) | KTRs w/o HEV Infection N = 80 N (%) | Statistical Group Difference, p-Value | Univariable OR (95% CI) |
|---|---|---|---|---|
| Gender | ||||
| Male | 30 (75) | 51 (63.75) | ||
| Female | 10 (25) | 29 (36.25) | ||
| Age | ||||
| Mean (y) | 52 ± 13.6 | 55.6 ± 13.6 | 0.241 | |
| Fish | (39) | (79) | ||
| At least weekly | 6 (15.4) | 39 (49.4) | 0.003 | 0.11 (0.03–0.46) |
| Less than weekly | 27 (69.2) | 36 (45.6) | 0.359 | 0.54 (0.15–1.87) |
| Never | 6 (15.4) | 4 (5.1) | Ref | |
| Seafood | (40) | (76) | ||
| At least weekly | 0 (0) | 1 (1.3) | 1.000 | 0.60 (0.54–0.73) |
| Less than weekly | 3 (7.5) | 18 (25) | 0.043 | 0.26 (0.07–0.95) |
| Never | 36 (90) | 56 (73.7) | Ref | |
| Salad | ||||
| At least weekly | 28 (70) | 67 (83.75) | 0.511 | 0.42 (0.03–6.92) |
| Less than weekly | 11 (27.5) | 12 (15) | 1.000 | 0.92 (0.05–16.4) |
| Never | 1 (2.5) | 1 (1.25) | Ref | |
| Raw vegetables | ||||
| At least weekly | 18 (45) | 62 (77.5) | 0.297 | 0.47 (0.14–1.60) |
| Less than weekly | 17 (42.5) | 10 (69.6) | 0.185 | 0.37 (0.09–1.44) |
| Never | 5 (12.5) | 10 (11.4) | Ref | |
| Raw milk products | (31) | (69) | ||
| At least weekly | 1 (3.2) | 19 (27.6) | 0.002 | 0.07 (0.01–0.56) |
| Less than weekly | 4 (12.9) | 15 (21.7) | 0.109 | 0.36 (0.11–1.21) |
| Never | 26 (83.9) | 35 (50.7) | Ref | |
| Raw minced pork meat | (37) | (78) | ||
| At least weekly | 2 (5.4) | 2 (2.6) | 0.598 | 2.07 (0.28–15.4) |
| Less than weekly | 6 (16.2) | 16 (20.5) | 0.799 | 0.78 (0.28–2.19) |
| Never | 29 (78.4) | 60 (76.9) | Ref | |
| Cooked minced pork meat | (37) | (79) | ||
| At least weekly | 5 (13.5) | 5 (6.3) | 0.205 | 3.75 (0.71–19.7) |
| Less than weekly | 28 (75.7) | 59 (75.6) | 0.417 | 1.78 (0.54–5.86) |
| Never | 4 (10.8) | 15 (19.2) | Ref | |
| Pork steak | (39) | (79) | ||
| At least weekly | 12 (30.8) | 8 (10.1) | 0.011 | 6.38 (1.56–26.1) |
| Less than weekly | 23 (59.0) | 54 (68.4) | 0.415 | 0.55 (0.17–1.82) |
| Never | 4 (10.2) | 17 (20.5) | Ref | |
| Raw minced beef meat | (38) | (77) | ||
| At least weekly | 1 (2.6) | 2 (2.6) | 1.000 | 1.00 (0.09–11.45) |
| Less than weekly | 5 (13.2) | 11 (14.3) | 1.000 | 0.91 (0.29–2.84) |
| Never | 32 (84.2) | 64 (83.1) | Ref | |
| Beef steak undercooked | (36) | (77) | ||
| At least weekly | 1 (2.8) | 3 (3.9) | 1.000 | 0.73 (0.07–7.36) |
| Less than weekly | 9 (25) | 17 (22.1) | 0.812 | 1.16 (0.64–2.95) |
| Never | 26 (72.2) | 57 (74.0) | Ref | |
| Wild boar meat | (37) | (58) | ||
| Yes | 2 (5.4) | 7 (12.1) | ||
| No | 35 (94.6) | 51 (87.9) | 0.279 | 0.42 (0.08–2.12) |
| Meat processing at home | (38) | (70) | ||
| At least weekly | 12 (31.6) | 3 (4.3) | 0.027 | 5.43 (1.29–22.9) |
| Less than weekly | 12 (31.6) | 48 (68.6) | 0.030 | 0.34 (0.13–0.87) |
| Never | 14 (36.8) | 19 (27.1) | Ref | |
| Touching raw meat with bare hands | (22) | (64) | ||
| Yes | 18 (81.8) | 37 (57.8) | 0.043 | 3.28 (1.00–10.81) |
| No | 4 (18.2) | 27 (42.2) | Ref | |
| Salami, raw sausage | (38) | (78) | ||
| At least weekly | 18 (47.4) | 24 (30.8) | 0.039 | 3.45 (1.10–10.83) |
| Less than weekly | 15 (39.5) | 31 (39.7) | 0.189 | 2.23 (0.71–7.01) |
| Never | 5 (13.1) | 23 (29.5) | Ref | |
| Spreadable sausage (Teeschinken) | (35) | (78) | ||
| At least weekly | 14 (40.0) | 11 (14.1) | <0.001 | 7.16 (2.41–21.3) |
| Less than weekly | 13 (37.1) | 22 (28.2) | 3.32 (1.20–9.20) | |
| Never | 8 (22.9) | 45 (57.7) | 0.023 | Ref |
| Raw ham | (38) | (78) | ||
| At least weekly | 12 (31.6) | 22 (28.2) | 0.190 | 2.18 (0.77–6.21) |
| Less than weekly | 18 (47.4) | 24 (30.8) | 0.034 | 3.0 (1.12–8.05) |
| Never | 8 (21.1) | 32 (41.0) | Ref | |
| Cured pork meat (Pökel) | (35) | (77) | ||
| At least weekly | 5 (14.3) | 14 (18.2) | 0.015 | 7.14 (1.52–33.5) |
| Less than weekly | 16 (45.7) | <0.001 | 4.90 (1.95–12.3) | |
| Never | 14 (40.0) | 60 (77.9) | Ref | |
| Boiled sausage (Brühwurst) | (36) | (77) | ||
| At least weekly | 12 (33.3) | 14 (18.2) | 0.002 | 5.88 (1.95–17.8) |
| Less than weekly | 17 (47.2) | 15 (19.5) | <0.001 | 7.77 (2.71–22.3) |
| Never | 7 (19.4) | 48 (62.3) | Ref | |
| Jellied sausage (Sülzwurst) | (34) | (77) | ||
| At least weekly | 0 (0) | 5 (6.5) | 0.318 | 0.71 (0.62–0.81) |
| Less than weekly | 9 (26.5) | 10 (13.0) | 0.173 | 2.23 (0.81–6.15) |
| Never | 25 (73.5) | 62 (80.5) | Ref | |
| Blood sausage (Blutwurst) | (35) | (72) | ||
| At least weekly | 0 (0) | 2 (2.8) | 1.000 | 0.72 (0.63–0.82) |
| Less than weekly | 10 (28.6) | 6 (8.3) | 0.010 | 4.27 (1.40–12.98) |
| Never | 25 (71.4) | 64 (88.9) | Ref | |
| Liver sausage (Leberwurst) | (36) | (78) | ||
| At least weekly | 7 (19.5) | 17 (21.8) | 1.000 | 0.99 (0.33–2.94) |
| Less than weekly | 16 (44.4) | 29 (37.2) | 0.654 | 1.36 (0.56–3.30) |
| Never | 13 (36.1) | 32 (41.0) | Ref | |
| Wiener sausage | (36) | (77) | ||
| At least weekly | 8 (22.2) | 22 (28.6) | 0.440 | 0.64 (0.22–1.85) |
| Less than weekly | 15 (41.7) | 32 (41.6) | 0.815 | 1.21 (0.48–3.01) |
| Never | 13 (36.1) | 23 (29.8) | Ref |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, E.; Koch, N.; Bachmann, F.; Schulz, M.; Seelow, E.; Weber, U.; Waiser, J.; Halleck, F.; Faber, M.; Bock, C.-T.; et al. Risk Factors for Hepatitis E Virus Infection and Eating Habits in Kidney Transplant Recipients. Pathogens 2023, 12, 850. https://doi.org/10.3390/pathogens12060850
Wu E, Koch N, Bachmann F, Schulz M, Seelow E, Weber U, Waiser J, Halleck F, Faber M, Bock C-T, et al. Risk Factors for Hepatitis E Virus Infection and Eating Habits in Kidney Transplant Recipients. Pathogens. 2023; 12(6):850. https://doi.org/10.3390/pathogens12060850
Chicago/Turabian StyleWu, Eva, Nadine Koch, Friederike Bachmann, Marten Schulz, Evelyn Seelow, Ulrike Weber, Johannes Waiser, Fabian Halleck, Mirko Faber, Claus-Thomas Bock, and et al. 2023. "Risk Factors for Hepatitis E Virus Infection and Eating Habits in Kidney Transplant Recipients" Pathogens 12, no. 6: 850. https://doi.org/10.3390/pathogens12060850
APA StyleWu, E., Koch, N., Bachmann, F., Schulz, M., Seelow, E., Weber, U., Waiser, J., Halleck, F., Faber, M., Bock, C.-T., Eckardt, K.-U., Budde, K., Hofmann, J., Nickel, P., & Choi, M. (2023). Risk Factors for Hepatitis E Virus Infection and Eating Habits in Kidney Transplant Recipients. Pathogens, 12(6), 850. https://doi.org/10.3390/pathogens12060850