
Resident Physicians’ Knowledge and Preparedness Regarding Human Monkeypox: A Cross-Sectional Study from Saudi Arabia
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Settings, and Subjects
2.2. Sample Size, Sampling, and Data Collection Techniques
2.3. Survey Contents
2.4. Pilot Study and Reliability of the Questionnaire
2.5. Data Analysis
2.6. Ethics
3. Results
3.1. Sociodemographic and Profession-Related Information
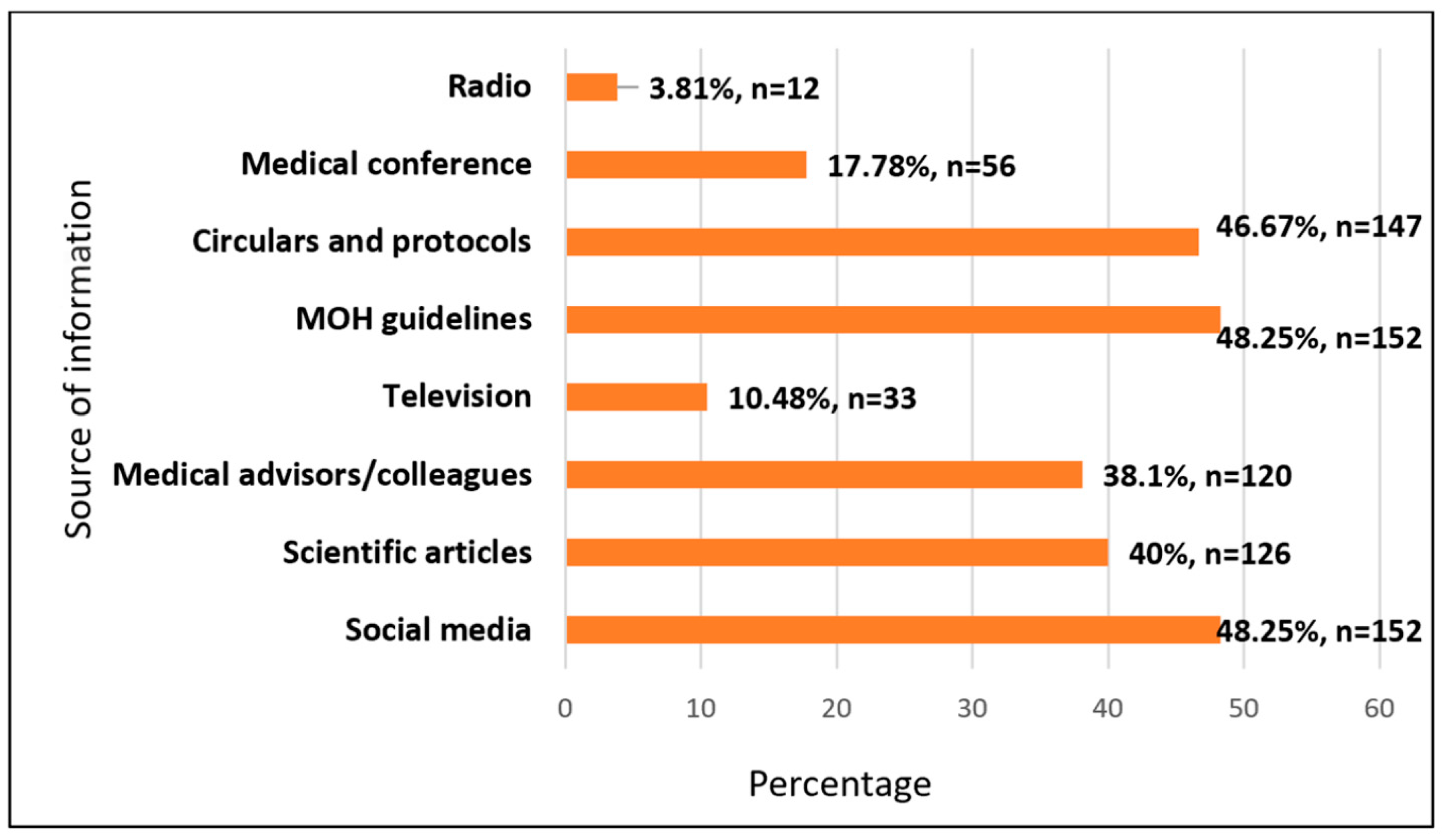
3.2. Source of Information
3.3. Knowledge about Mpox and Its Associated Factors
3.4. Confidence in the Management and Diagnosis of Monkeypox
3.5. Medical Specialties
4. Discussion
4.1. Implications of the Findings
4.2. Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pastula, D.M.; Tyler, K.L. An Overview of Monkeypox Virus and Its Neuroinvasive Potential. Ann. Neurol. 2022, 92, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Awadi, S.; Al-Shami, K.; Alkhoun, H.A.; Al-Eitan, S.F.; Alsheikh, A.M.; Saeed, A.; Al-Zoubi, R.M.; Al Zoubi, M.S. Human Monkeypox Virus in the Shadow of the COVID-19 Pandemic. J. Infect. Public Health 2023, 16, 1149–1157. [Google Scholar]
- Mitjà, O.; Ogoina, D.; Titanji, B.K.; Galvan, C.; Muyembe, J.-J.; Marks, M.; Orkin, C.M. Monkeypox. Lancet 2023, 401, 60–74. [Google Scholar] [CrossRef]
- Mpox (Monkeypox) Outbreak 2022. Available online: https://www.who.int/emergencies/situations/monkeypox-oubreak-2022 (accessed on 18 May 2023).
- Macneil, A.; Reynolds, M.G.; Braden, Z.; Carroll, D.S.; Bostik, V.; Karem, K.; Smith, S.K.; Davidson, W.; Li, Y.; Moundeli, A.; et al. Transmission of atypical varicella-zoster virus infections involving palm and sole manifestations in an area with monkeypox endemicity. Clin Infect Dis. 2009, 48, e6–e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human Monkeypox—A potential threat? A systematic review. PLOS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- Vogel, L. Making sense of monkeypox death rates. CMAJ 2022, 194, E1097. [Google Scholar] [CrossRef]
- WHO Director-General Declares the Ongoing Monkeypox Outbreak a Public Health Emergency of International Concern. Available online: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern (accessed on 18 May 2023).
- 2022-23 Mpox (Monkeypox) Outbreak: Global Trends. Available online: https://worldhealthorg.shinyapps.io/mpx_global/ (accessed on 18 May 2023).
- Mungmunpuntipantip, R.; Wiwanitkit, V. Smallpox vaccination discontinuation and monkeypox incidence in an African endemic region: A reanalysis on the relationship between the withdrawal of smallpox vaccine and subsequent morbidity. Am. J. Clin. Exp. Immunol. 2022, 11, 78–83. [Google Scholar] [PubMed]
- Sah, R.; Mohanty, A.; Padhi, B.K.; Rais, M.A.; Alotaibi, Z.A.; Alazwari, A.M.; Alghamdi, A.K.S.; Alwahbi, N.F.J.; Alshahrani, N.Z. Monkeypox deaths in 2022 outbreak across the globe: Correspondence. Ann. Med. Surg. 2023, 85, 57–58. [Google Scholar] [CrossRef]
- Flanagan, M.L.; Parrish, C.R.; Cobey, S.; Glass, G.E.; Bush, R.M.; Leighton, T.J. Anticipating the Species Jump: Surveillance for Emerging Viral Threats. Zoonoses Public Health 2012, 59, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Frutos, R.; Gavotte, L.; Serra-Cobo, J.; Chen, T.; Devaux, C. COVID-19 and emerging infectious diseases: The society is still unprepared for the next pandemic. Environ. Res. 2021, 202, 111676. [Google Scholar] [CrossRef]
- Ministry of Health Saudi Arabia. Available online: https://www.MOH.gov.sa/en/Pages/Default.aspx (accessed on 18 May 2023).
- Hasan, M.; Hossain, M.A.; Chowdhury, S.; Das, P.; Jahan, I.; Rahman, M.F.; Haque, M.M.A.; Rashid, M.U.; Khan, M.A.S.; Hossian, M. Human Monkeypox and Preparedness of Bangladesh: A Knowledge and Attitude Assessment Study among Medical Doctors. J. Infect. Public Health 2023, 16, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Al-Mahzoum, K.; Al-Tammemi, A.B.; Alkurtas, M.; Mirzaei, F.; Kareem, N.; Al-Naimat, H.; Jardaneh, L.; Al-Majali, L.; AlHadidi, A.; et al. Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare 2022, 10, 1722. [Google Scholar] [CrossRef] [PubMed]
- Salim, N.A.; Septadina, I.S.; Permata, M. Knowledge, Attitude, and Perception of Anticipating 2022 Global Human Monkeypox Infection among Internal Medicine Residents at Palembang Indonesia: An Online Survey. J. Kedokt. Dan Kesehat. Publ. Ilm. Fak. Kedokt. Univ. Sriwij. 2022, 9, 253–262. [Google Scholar] [CrossRef]
- Sobaikhi, N.H.; Alshahrani, N.Z.; Hazazi, R.S.; Al-Musawa, H.I.; Jarram, R.E.; Alabah, A.E.; Haqawi, N.F.; Munhish, F.A.; Shajeri, M.A.; Matari, M.H.; et al. Health Workers’ Knowledge and Attitude towards Monkeypox in Southwestern Saudi Arabia: A Cross-Sectional Study. Diseases 2023, 11, 81. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Alsabaani, A.A.; Ridda, I.; Rashid, H.; Alzahrani, F.; Almutairi, T.H.; Alzahrani, B.A.S.; Albeshri, A.S.S. Uptake of COVID-19 Booster Dose among Saudi Arabian Population. Medicina 2022, 58, 972. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Algethami, M.R.; Alarifi, A.M.; Alzahrani, F.; Alshehri, E.A.; Alshehri, A.M.; Sheerah, H.A.; Abdelaal, A.; Sah, R.; Rodriguez-Morales, A.J. Knowledge and Attitude Regarding Monkeypox Virus among Physicians in Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 2099. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Knowledge of human monkeypox viral infection among general practitioners: A cross-sectional study in Indonesia. Pathog. Glob. Health 2020, 114, 68–75. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Alzahrani, F.; Alarifi, A.M.; Algethami, M.R.; Alhumam, M.N.; Ayied, H.A.M.; Awan, A.Z.; Almutairi, A.F.; Bamakhrama, S.A.; Almushari, B.S.; et al. Assessment of Knowledge of Monkeypox Viral Infection among the General Population in Saudi Arabia. Pathogens 2022, 11, 904. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Assiri, A.M.; Al-Tawfiq, J.A.; Rodriguez-Morales, A.J.; Sah, R. The human monkeypox in Saudi Arabia and global tourism. Ann. Med. Surg. 2022, 82, 104686. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Lopardo, G.; Verbanaz, S.; Orduna, T.; Lloveras, S.; Azeñas-Burgoa, J.M.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Barbosa, A.N.; Diaz-Quijano, F.; et al. Latin America: Situation and Preparedness Facing the Multi-Country Human Monkeypox Outbreak. Lancet Reg. Health Am. 2022, 13, 100318. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Confidence in managing human monkeypox cases in Asia: A cross-sectional survey among general practitioners in Indonesia. Acta Trop. 2020, 206, 105450. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.R.; Grijalva, M.J. Knowledge, attitudes, and practices towards monkeypox during the 2022 outbreak: An online cross-sectional survey among clinicians in Ohio, USA. J. Infect. Public Health 2022, 15, 1459–1465. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.; Wrubel, J.; Rabow, M.W. Professional development and the informal curriculum in end-of-life care. J. Cancer Educ. 2011, 26, 444–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sah, R.; Reda, A.; Abdelaal, A.; MOHanty, A.; Siddiq, A.; Alshahrani, N.Z.; Amer, F.A.; Rodriguez-Morales, A.J. A potential monkeypox pandemic: Are we making the same mistakes as COVID-19? New Microbes New Infect. 2022, 49, 101030. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Talukder, M.; Rosen, T.; Piguet, V. Differential Diagnosis, Prevention, and Treatment of Mpox (Monkeypox): A Review for Dermatologists. Am. J. Clin. Dermatol. 2023, 1–16. [Google Scholar] [CrossRef]
- Kawsar, A.; Hussain, K.; Roberts, N. Monkeypox: Key Pointers for Dermatologists. Clin. Exp. Dermatol. 2022, 47, 2282–2284. [Google Scholar] [CrossRef]
- Sahin, T.K.; Erul, E.; Aksun, M.S.; Sonmezer, M.C.; Unal, S.; Akova, M. Knowledge and Attitudes of Turkish Physicians towards Human Monkeypox Disease and Related Vaccination: A Cross-Sectional Study. Vaccines 2022, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.; Abubakar, I.; Ihekweazu, C.; Heymann, D.; Ntoumi, F.; Blumberg, L.; Asogun, D.; Mukonka, V.; Lule, S.A.; Bates, M.; et al. Monkeypox—Enhancing public health preparedness for an emerging lethal human zoonotic epidemic threat in the wake of the smallpox post-eradication era. Int. J. Infect. Dis. 2019, 78, 78–84. [Google Scholar] [CrossRef]
- Duque, M.P.; Ribeiro, S.; Martins, J.V.; Casaca, P.; Leite, P.P.; Tavares, M.; Mansinho, K.; Duque, L.M.; Fernandes, C.; Cordeiro, R.; et al. Ongoing monkeypox virus outbreak, Portugal, April 29 to May 23 2022. Eurosurveillance 2022, 27, 2200424. [Google Scholar]


{kind=link}
{kind=link}
| Variable(s) | Frequency | Percentage |
|---|---|---|
| Age (in years) | ||
| 25–29 | 141 | 44.8 |
| 30–34 | 135 | 42.9 |
| 35–39 | 34 | 10.8 |
| 40 and more | 5 | 1.6 |
| Gender | ||
| Male | 208 | 66.0 |
| Female | 107 | 34.0 |
| Marital status | ||
| Single | 138 | 43.8 |
| Married | 177 | 56.2 |
| Level of work | ||
| R1 | 59 | 18.7 |
| R2 | 51 | 16.2 |
| R3 | 73 | 23.2 |
| R4 | 98 | 31.1 |
| R5 | 12 | 3.8 |
| GP | 22 | 7.0 |
| Medical Specialty | ||
| Dentist | 17 | 5.4 |
| Preventive Medicine | 37 | 11.8 |
| Emergency Medicine | 11 | 3.5 |
| Family medicine | 70 | 22.2 |
| General practitioner | 18 | 5.7 |
| Internal Medicine | 76 | 24.1 |
| Pediatric | 29 | 9.2 |
| Surgery | 49 | 15.6 |
| Dermatology | 8 | 2.5 |
| Where is your work center? | ||
| University KKU-Hospital | 14 | 4.4 |
| Khamis Mushait Health Sector “MOH” | 63 | 20.0 |
| Military Health Sector “AFHSR or MOI | 76 | 24.1 |
| Abha Health Sector “MOH” | 162 | 51.4 |
| Nature of your routine work in hospital/health center/clinic? | ||
| Outpatient | 65 | 20.6 |
| Inpatient and outpatient | 155 | 49.2 |
| Others | 37 | 11.7 |
| Inpatient | 24 | 7.6 |
| Administrative * | 34 | 10.8 |
| Medical practice experience in years | ||
| <1 year | 34 | 10.8 |
| 1–5 years | 193 | 61.3 |
| >5 years | 88 | 27.9 |
| Had you ever received information about Mpox during residency or medical school education? | ||
| Yes | 124 | 39.4 |
| No | 191 | 60.6 |
| Did you receive a copy of the Saudi MOH Protocol for Patients Suspected/Confirmed with Mpox? | ||
| Yes | 114 | 36.2 |
| No | 201 | 63.8 |
| When was the first time you heard information about Mpox? | ||
| Within last several days or weeks | 4 | 1.3 |
| Within last month or later | 36 | 11.4 |
| Within last 6 months or later | 260 | 82.5 |
| I did not hear about it | 15 | 4.8 |
| Did you attend any conference or lecture about Mpox? | ||
| Yes | 73 | 23.2 |
| No | 242 | 76.8 |
| Items | Response, N (%) | |
|---|---|---|
| Yes | No | |
| 1. Mpox is prevalent in middle eastern countries | 56 (17.78) | 259 (82.22) |
| 2. Mpox is prevalent in Western and Central Africa | 148 (46.98) | 167 (53.01) |
| 3. There are human Mpox cases in Saudi Arabia | 143 (45.39) | 172 (54.6) |
| 4. Is Mpox a viral disease infection? | 286 (90.79) | 29 (9.2) |
| 5. Mpox is easily transmitted via droplet contact (e.g., sneezing, coughing, etc.) | 172 (54.60) | 143 (45.39) |
| 6. Mpox could be transmitted through intimate contact | 212 (67.30) | 103 (32.69) |
| 7. Is Mpox easily transmitted human-to-human? | 189 (60) | 126 (40) |
| 8. Could Mpox be transmitted through a bite of an infected monkey? | 142 (45.07) | 173 (54.92) |
| 9. Travelers from America and Europe are the main source of imported cases of Mpox | 126 (40) | 189 (60) |
| 10. Mpox and smallpox have similar signs and symptoms | 148 (46.98) | 167 (53.01) |
| 11. Mpox and chickenpox have similar signs and symptoms? | 136 (43.17) | 179 (56.8) |
| 12. A Flu-like syndrome is one of the early signs or symptoms of human Mpox? | 206 (65.39) | 109 (34.6) |
| 13. Rashes on the skin are one of the signs or symptoms of human Mpox? | 238 (75.56) | 77 (24.44) |
| 14. Mpox is diagnosed by taking a swab sample from the lesion for a polymerase chain reaction | 191 (60.63) | 124 (39.36) |
| 15. A person does not exhibit symptoms during the incubation period | 115 (36.50) | 200 (63.49) |
| 16. Incubation period of Mpox lasts between 3–5 days | 101 (32.21) | 214 (67.93) |
| 17. Diarrhea is one of the signs or symptoms of human Mpox? | 88 (27.93) | 227 (72.06) |
| 18. Lymphadenopathy (swollen lymph nodes) is one clinical sign or symptom that could be used to differentiate Mpox and smallpox cases? | 179 (56.82) | 136 (43.17) |
| 19. There is a specific treatment for Mpox? | 67 (21.26) | 248 (78.73) |
| 20. Analgesics and antipyretics can be given to manage local pains and fever caused by Mpox | 236 (74.92) | 79 (25.07) |
| 21. Antivirals are required in the management of human Mpox patients | 151 (47.93) | 164 (52.06) |
| 22. Antibiotics are required in the management of human Mpox patients | 28 (8.89) | 287 (91.11) |
| 23. People who got chickenpox vaccine are immunized against Mpox | 102 (32.38) | 213 (67.61) |
| 24. There is a specific vaccine for Mpox? | 54 (17.14) | 261 (82.85) |
| Variables | Categories | Knowledge | Chi-Square Test/Fisher’s Exact Test | Regression Model | ||||
|---|---|---|---|---|---|---|---|---|
| Overall knowledge score | Poor | Good | p | AOR | 95% C.I. | p | ||
| 103 (32.7) | 212 (67.3) | |||||||
| Age groups | 25–29 | 59 (41.8) | 82 (58.2) | 0.01 * | Ref. | |||
| 30–34 | 37 (27.4) | 98 (72.6) | 0.59 | 0.04 | 11.36 | 0.837 | ||
| 35–39 | 6 (17.6) | 28 (82.4) | 1.05 | 0.08 | 14.34 | 0.985 | ||
| 40 and more | 1 (20.0) | 4 (80.0) | 1.33 | 0.09 | 17.58 | 0.912 | ||
| Gender | Female | 69 (33.2) | 139 (66.8) | 0.80 | Ref. | |||
| Male | 34 (31.8) | 73 (68.2) | 0.89 | 0.43 | 1.86 | 0.756 | ||
| Marital status | Married | 52 (37.7) | 86 (62.3) | 0.12 | Ref. | |||
| Single | 51 (28.8) | 126 (71.2) | 1.19 | 0.57 | 2.48 | 0.651 | ||
| Level of work | R1 | 30 (50.8) | 29 (49.2) | 0.01 * | Ref | |||
| R2 | 19 (37.3) | 32 (62.7) | 1.58 | 0.09 | 26.94 | 0.753 | ||
| R3 | 16 (21.9) | 57 (78.1) | 2.17 | 0.11 | 13.91 | 0.613 | ||
| R4 | 15 (15.3) | 83 (84.7) | 4.38 | 0.21 | 10.37 | 0.338 | ||
| R5 | 7 (58.3) | 5 (41.7) | 7.23 | 0.34 | 13.61 | 0.205 | ||
| GP | 16 (72.7) | 6 (27.3) | 4.92 | 0.18 | 18.29 | 0.349 | ||
| Medical Specialty | Dentist | 7 (41.1) | 10 (58.8) | 0.01 * | Ref. | |||
| Preventive Medicine | 3 (8.1) | 34 (91.9) | 0.624 | 0.488 | 0.797 | 0.001 * | ||
| Emergency Medicine | 2 (18.2) | 9 (81.8) | 1.134 | 0.900 | 1.429 | 0.286 | ||
| Family medicine | 18 (25.8) | 52 (74.3) | 0.902 | 0.568 | 1.433 | 0.661 | ||
| General practitioner | 14 (77.8) | 4 (22.2) | 0.934 | 0.672 | 1.297 | 0.682 | ||
| Internal Medicine | 16 (21.1) | 60 (78.9) | 1.082 | 0.812 | 1.442 | 0.589 | ||
| Pediatric | 9 (31) | 20 (69) | 0.912 | 0.537 | 1.551 | 0.735 | ||
| Surgery | 34 (69.4) | 15 (30.6) | 0.977 | 0.626 | 1.525 | 0.919 | ||
| Dermatology | 1 (12.5) | 7 (87.5) | 1.048 | 0.880 | 1.247 | 0.601 | ||
| Where is your work center? | University Health Sector | 3 (21.4) | 11 (78.6) | 0.83 | Ref. | 1 | ||
| Khamis Mushait Health Sector | 21 (33.3) | 42 (66.7) | 1.05 | 0.14 | 8.08 | 0.966 | ||
| Military Health Sector | 26 (34.2) | 50 (65.8) | 1.24 | 0.45 | 3.41 | 0.672 | ||
| Abha Health Sector | 53 (32.7) | 109 (67.2) | 1.07 | 0.49 | 2.35 | 0.866 | ||
| Nature of your routine work in hospital/health center/clinic? | Outpatient | 16 (24.6) | 49 (75.4) | 0.01 * | Ref. | 1 | ||
| Inpatient and outpatient | 65 (41.9) | 90 (58.1) | 0.71 | 0.16 | 3.13 | 0.648 | ||
| Others | 11 (29.7) | 26 (70.2) | 0.52 | 0.13 | 2.02 | 0.341 | ||
| Inpatient | 7 (29.2) | 17 (70.8) | 0.26 | 0.05 | 1.40 | 0.118 | ||
| Administrative ** | 4 (11.8) | 30 (88.2) | 0.70 | 0.12 | 4.28 | 0.700 | ||
| Medical practice experience | <1 year | 18 (52.9) | 16 (47.1) | 0.01 * | Ref. | 1 | ||
| 1–5 years | 66 (34.2) | 127 (65.8) | 1.19 | 0.28 | 5.09 | 0.808 | ||
| >5 years | 19 (21.6) | 69 (78.4) | 0.87 | 0.35 | 2.15 | 0.758 | ||
| Received information about Mpox during residency or medical school education | Yes | 31 (25.0) | 93 (75.0) | 0.02 * | Ref. | 1 | ||
| No | 72 (37.7) | 119 (62.3) | 0.96 | 0.44 | 2.09 | 0.927 | ||
| Received a copy of the Saudi MOH Protocol for Mpox management | Yes | 13 (11.4) | 101 (88.6) | 0.01 * | 4.25 | 2.49 | 5.64 | 0.001 * |
| No | 90 (44.8) | 111 (55.2) | Ref. | 1 | ||||
| First time hearing information about Mpox | I did not hear about it | 1 (33.3) | 3 (63.7) | 0.01 * | Ref. | 1 | ||
| Within last several days or weeks | 17 (47.2) | 19 (52.8) | 0.12 | 0.09 | 3.77 | 0.999 | ||
| Within last month or later | 74 (28.5) | 186 (71.5) | 1.91 | 0.32 | 11.58 | 0.480 | ||
| Within last 6 months or later | 12 (80.0) | 3 (20.0) | 3.21 | 0.65 | 15.81 | 0.152 | ||
| Attended any conferences or lectures about Mpox | Yes | 15 (20.5) | 58 (79.5) | 0.01 * | 3.34 | 2.12 | 6.96 | 0.001 * |
| No | 88 (36.4) | 154 (63.6) | Ref. | 1 | ||||
| Items | Answer | N | % |
|---|---|---|---|
| 1. Are you confident to manage Mpox cases, if any, based on your current knowledge and skills? | Yes | 87 | 27.6 |
| No | 228 | 72.4 | |
| 2. Are you confident to diagnose Mpox cases based on your current knowledge and skills? | Yes | 121 | 38.4 |
| No | 194 | 61.6 | |
| 3. Are you confident to diagnose Mpox cases based on the ability of your current facility to do diagnostic test? | Yes | 112 | 35.6 |
| No | 203 | 64.4 |
| Variables | Categories | Confidence | Chi-Square Test/Fisher’s Exact Test | Regression Model | ||||
|---|---|---|---|---|---|---|---|---|
| Overall Confidence score | Low | High | p | AOR | 95% C.I. | p | ||
| 206 (65.4) | 109 (34.6) | Lower | Upper | |||||
| Age groups | 25–29 | 102 (72.34) | 39 (27.65) | 0.018 * | Ref. | 1 | ||
| 30–34 | 86 (63.70) | 49 (36.29) | 1.44 | 0.13 | 16.40 | 0.768 | ||
| 35–39 | 15 (44.11) | 19 (55.88) | 1.54 | 0.14 | 16.42 | 0.720 | ||
| 40 and more | 3 (60) | 2 (40) | 2.05 | 0.18 | 22.98 | 0.559 | ||
| Gender | Female | 76 (71.02) | 31(28.97) | 0.132 | Ref. | 1 | ||
| Male | 130 (62.5) | 78 (37.5) | 1.41 | 0.68 | 2.92 | 0.362 | ||
| Marital status | Married | 114 (64.40) | 63 (35.59) | 0.676 | Ref. | 1 | ||
| Single | 92 (66.66) | 46 (33.33) | 1.50 | 0.75 | 3.01 | 0.251 | ||
| Level of work | R1 | 46 (77.96) | 13 (22.04) | <0.001 * | Ref. | 1 | ||
| R2 | 37 (72.54) | 14 (27.45) | 1.33 | 0.55 | 3.26 | 0.528 | ||
| R3 | 47 (64.38) | 26 (35.61) | 0.57 | 0.24 | 1.33 | 0.192 | ||
| R4 | 46 (46.93) | 52 (53.06) | 5.15 | 1.94 | 13.68 | 0.001 * | ||
| R5 | 11 (91.66) | 1 (8.33) | 1.05 | 0.79 | 1.38 | 0.748 | ||
| GP | 19 (86.36) | 3 (13.63) | 1.01 | 0.54 | 1.89 | 0.979 | ||
| Medical Specialty | Dentist | 13 (76.47) | 4 (23.52) | <0.001 * | Ref. | 1 | ||
| Preventive Medicine | 14 (37.83) | 23 (62.16) | 1.02 | 0.60 | 1.75 | 0.939 | ||
| Emergency Medicine | 5 (45.45) | 6 (54.54) | 0.15 | 0.017 | 1.34 | 0.090 | ||
| Family medicine | 42 (60) | 28 (40) | 0.82 | 0.451 | 1.47 | 0.499 | ||
| General practitioner | 15 (83.33) | 3 (16.66) | 0.99 | 0.76 | 1.29 | 0.924 | ||
| Internal Medicine | 51 (67.10) | 25 (32.89) | 0.99 | 0.88 | 1.11 | 0.854 | ||
| Pediatric | 19 (65.51) | 10 (34.48) | 0.76 | 0.47 | 1.21 | 0.245 | ||
| Surgery | 47 (95.91) | 2 (4.08) | 1.42 | 0.62 | 3.23 | 0.404 | ||
| Dermatology | 1 (12.5) | 7 (87.5) | 1.70 | 1.06 | 2.73 | 0.029 * | ||
| Where is your work center? | University Health Sector | 6 (42.85) | 8 (57.14) | 0.112 * | Ref. | 1 | ||
| Khamis Mushait Health Sector | 44 (69.84) | 19 (30.15) | 3.543 | 0.63 | 20.01 | 0.152 | ||
| Military Health Sector | 55 (72.36) | 21 (27.63) | 0.621 | 0.25 | 1.56 | 0.310 | ||
| Abha Health Sector | 101 (62.34) | 61 (37.65) | 0.605 | 0.26 | 1.41 | 0.246 | ||
| Nature of your routine work in hospital/health center/clinic? | Outpatient | 40 (61.53) | 25 (38.46) | 0.005 * | Ref. | 1 | ||
| Inpatient and outpatient | 116 (74.83) | 39 (25.16) | 1.19 | 0.41 | 3.51 | 0.744 | ||
| Others | 22 (59.45) | 15 (40.54) | 1.34 | 0.45 | 4.01 | 0.602 | ||
| Inpatient | 11 (45.83) | 13 (54.16) | 0.96 | 0.29 | 3.17 | 0.947 | ||
| Administrative ** | 17 (50) | 17 (50) | 2.26 | 1.18 | 3.89 | 0.031 * | ||
| Medical practice experience | <1 year | 29 (85.29) | 5 (14.70) | <0.001 * | Ref. | 1 | ||
| 1–5 years | 131 (67.87) | 62 (32.12) | 0.31 | 0.06 | 1.48 | 0.141 | ||
| >5 years | 46 (52.27) | 42 (47.72) | 0.57 | 0.26 | 1.26 | 0.163 | ||
| Received information about Mpox during residency or medical school education | Yes | 61 (49.19) | 63 (50.80) | Ref. | 1 | |||
| No | 145 (75.91) | 46 (24.08) | <0.001 * | 2.27 | 1.16 | 4.45 | 0.016 * | |
| Received a copy of the Saudi MOH Protocol for Mpox management | Yes | 54 (47.36) | 60 (52.63) | <0.001 * | Ref. | 1 | ||
| No | 152 (75.62) | 49 (24.37) | 1.48 | 0.75 | 2.91 | 0.261 | ||
| First time hearing information about monkeypox | I did not hear about it | 13 (86.66) | 2 (13.33) | 0.204 | Ref. | 1 | ||
| Within last several days or weeks | 2 (50) | 2 (50) | 1.09 | 0.04 | 9.93 | 0.957 | ||
| Within last month or later | 26 (72.22) | 10 (27.77) | 1.43 | 0.18 | 7.49 | 0.737 | ||
| Within last 6 months or later | 165 (63.46) | 95 (36.53) | 1.58 | 0.24 | 5.31 | 0.634 | ||
| Attended any conferences or lectures about monkeypox | Yes | 29 (39.72) | 44 (60.27) | <0.001 * | Ref. | 1 | ||
| No | 177 (73.14) | 65 (26.85) | 1.46 | 0.67 | 3.18 | 0.336 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shafei, A.M.; Al-Mosaa, K.M.; Alshahrani, N.Z.; ALAmmari, M.H.M.; Almuhlafi, M.O.O.; Draim, N.H.A.A.; Alwadie, A.M.; Alghrab, A.I. Resident Physicians’ Knowledge and Preparedness Regarding Human Monkeypox: A Cross-Sectional Study from Saudi Arabia. Pathogens 2023, 12, 872. https://doi.org/10.3390/pathogens12070872
Shafei AM, Al-Mosaa KM, Alshahrani NZ, ALAmmari MHM, Almuhlafi MOO, Draim NHAA, Alwadie AM, Alghrab AI. Resident Physicians’ Knowledge and Preparedness Regarding Human Monkeypox: A Cross-Sectional Study from Saudi Arabia. Pathogens. 2023; 12(7):872. https://doi.org/10.3390/pathogens12070872
Chicago/Turabian StyleShafei, Ali Mohammad, Khalid M. Al-Mosaa, Najm Z. Alshahrani, Mohammed Hassan Mohammed ALAmmari, Mashael Obaid Othman Almuhlafi, Nasser Hassan Awdah Al Draim, Afnan Misfer Alwadie, and Abdullah Ibrahim Alghrab. 2023. "Resident Physicians’ Knowledge and Preparedness Regarding Human Monkeypox: A Cross-Sectional Study from Saudi Arabia" Pathogens 12, no. 7: 872. https://doi.org/10.3390/pathogens12070872