
Are Kidneys Affected by SARS-CoV-2 Infection? An Updated Review on COVID-19-Associated AKI

 ,
,
Abstract
1. Introduction
2. SARS-CoV-2 Infection and Kidneys: AKI
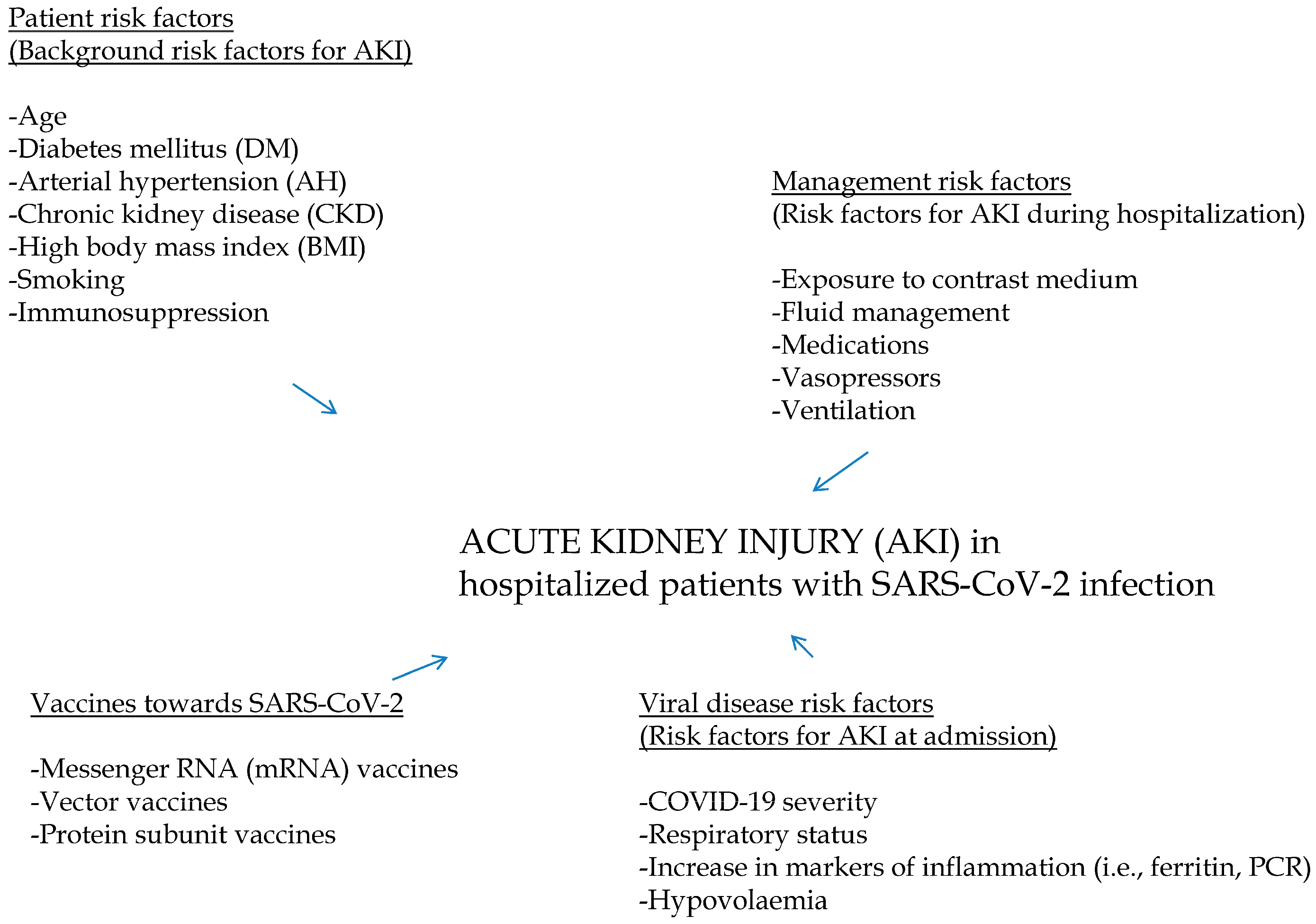
3. SARS-CoV-2 and Kidneys: Risk Factors for AKI
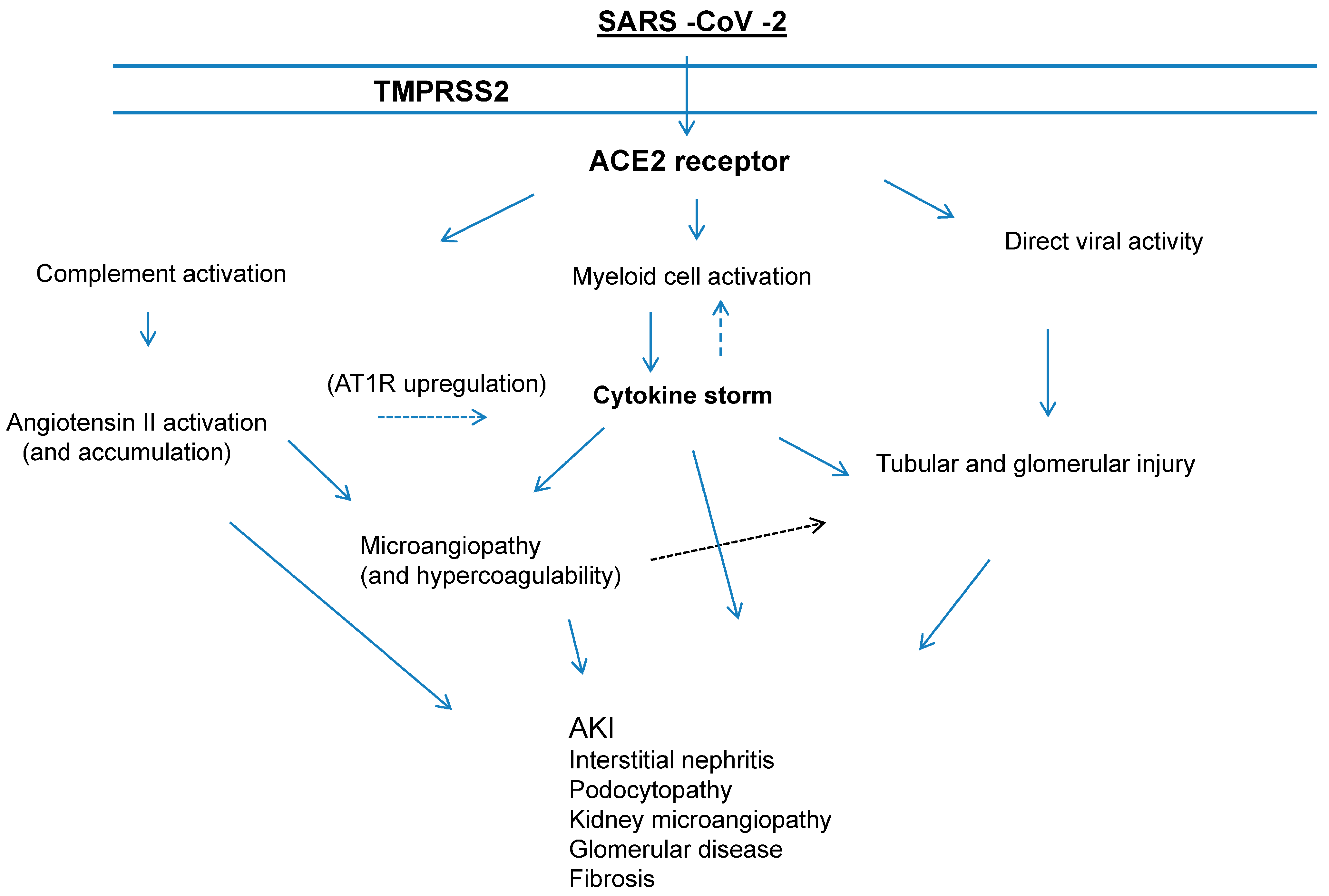
4. SARS-CoV-2 and Kidneys: AKI Pathogenesis and Direct Renal Tropism
5. SARS-CoV-2 and Kidneys: AKI Pathogenesis and ‘Cytokine Storm’
6. SARS-CoV-2 and Kidneys: AKI and Compromised Immune Response
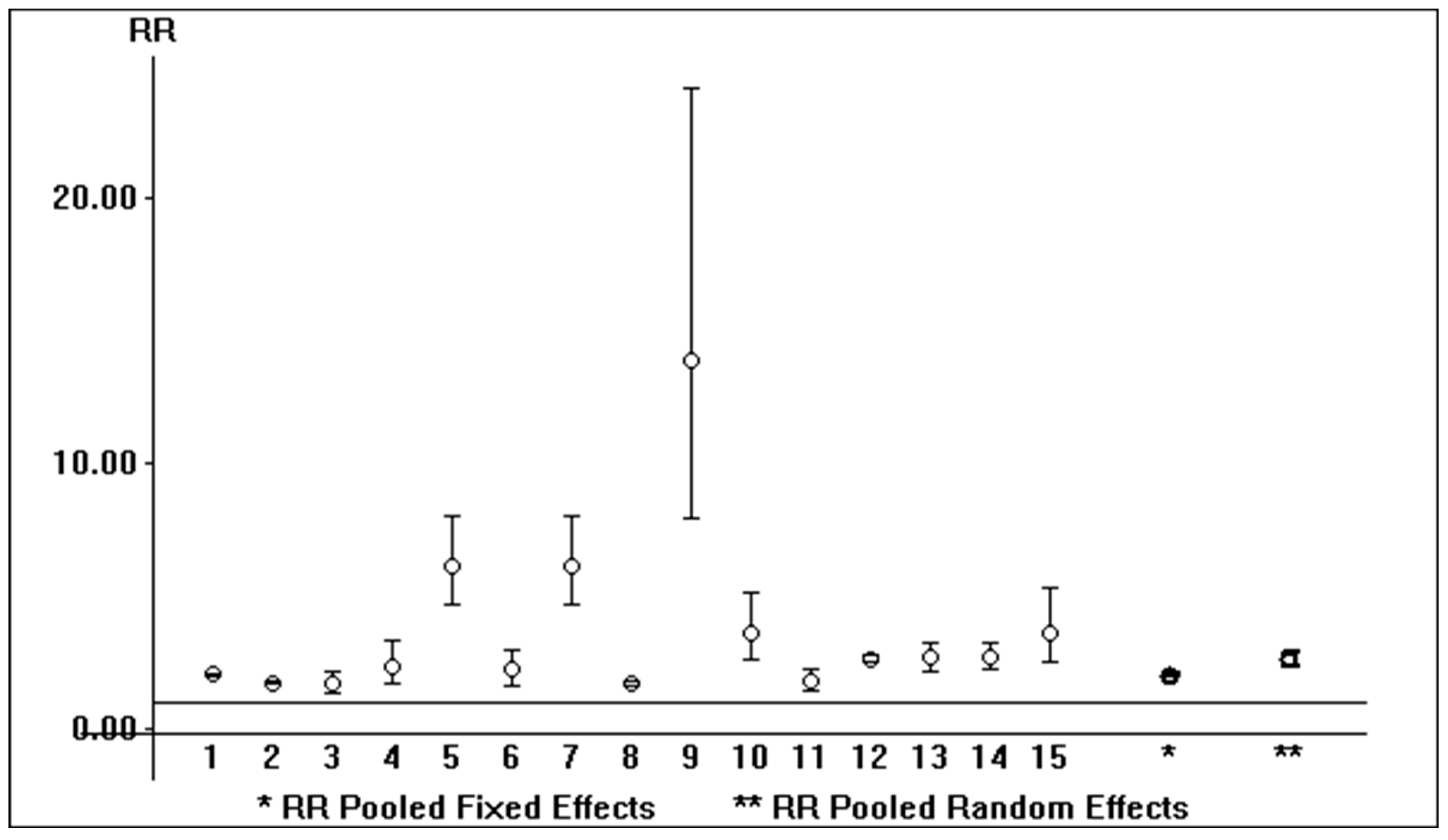
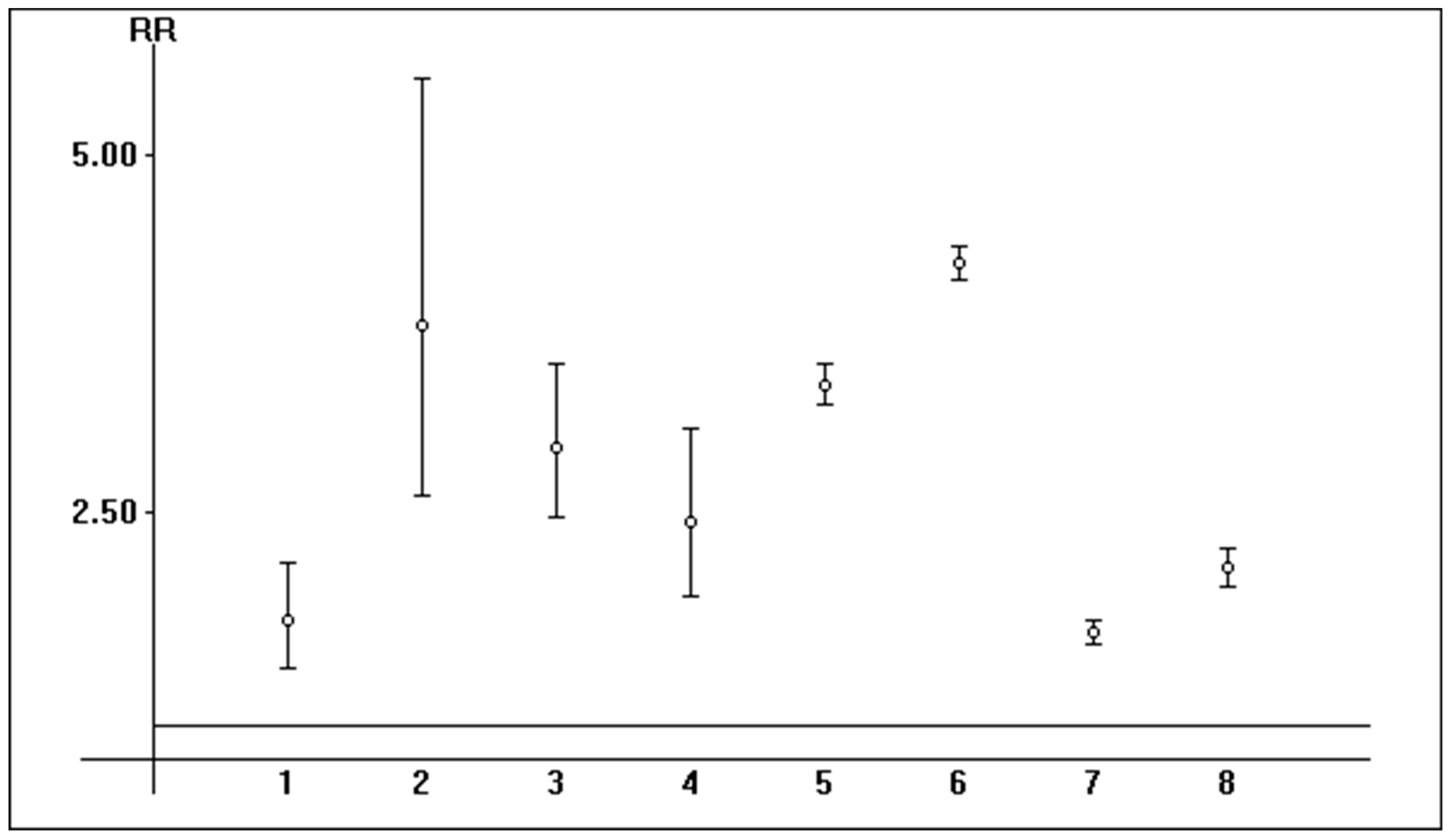
7. SARS-CoV-2 and Kidneys: Epidemiology of AKI (Pooled Analysis)
8. Kidney Disease and Long COVID
9. Conclusions
Supplementary Materials
Funding
Conflicts of Interest
Abbreviations
| ACEIs | Angiotensin converting enzymes |
| AE | Adverse events |
| AH | Arterial hypertension |
| AKI | Acute kidney injury |
| ARBs | Angiotensin receptor blockers |
| CI | Confidence intervals |
| CKD | Chronic kidney disease |
| COVID-19 | Coronavirus disease 2019 |
| COPD | Chronic obstructive pulmonary disease |
| CPAP | Continuous positive airway pressure |
| DM | Diabetes mellitus |
| eGFR | Estimated glomerular filtration rate |
| ESRD | End-stage renal disease |
| FANS | Non-steroidal anti-inflammatory drugs |
| HD | Hemodialysis |
| HFNC | High flow nasal cannula |
| ICU | Intensive care unit |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| NA | Not available |
| RAAS | Renin–angiotensin–aldosterone system |
| RRT | Renal replacement therapy |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| UTI | Urinary tract infection |
| VM | Venturi mask |
| WHO | World Health Organization |
References
- Wiersinga, W.; Rhodes, A.; Cheng, A.; Peacock, S.; Prescott, H. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Director-General’s Remarks at the Media Briefing on COVID-19 on 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 March 2020).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 1 January 2024).
- Martinez-Rojas, M.; Vega-Vega, O.; Bobadilla, N. Is the kidney a target of SARS-CoV-2? Am. J. Physiol. Renal Physiol. 2020, 318, F1454–F1462. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, X.; Chen, H.; Yan, S.; Li, D.; Li, H.; Gong, Z. Coronavirus disease 19 infection does not result in acute kidney injury: An analysis of 116 hospitalized patients from Wuhan, China. Am. J. Nephrol. 2020, 51, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.; Lely, A.; Navis, G.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Bell, S.; Forni, L.; Joannidis, M.; Koyner, J.; Liu, K.; Cantaluppi, V. Pathophysiology of COVID-19 associated acute kidney injury. Nat. Rev. Nephrol. 2021, 17, 751–764. [Google Scholar] [CrossRef] [PubMed]
- Fabrizi, F.; Alfieri, C.; Cerutti, R.; Lunghi, G.; Messa, P.G. COVID-19 and acute kidney injury: A systematic review and meta-analysis. Pathogens 2020, 9, 1052. [Google Scholar] [CrossRef]
- Mahalingasivam, V.; Su, G.; Iwagami, M.; Davids, M.; Wetmore, J.; Nitsch, D. COVID-19 and kidney disease: Insights from epidemiology to inform clinical practice. Nat. Rev. Nephrol. 2022, 18, 485–498. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Murugan, R.; Karajala-Subramanyam, V.; Lee, M.; Yende, S.; Kong, L.; Carter, M.; Angus, D.C.; Kellum, J.A. Acute kidney injury in non-severe pneumonia is associated with an increased immune response and lower survival. Kidney Int. 2010, 77, 527–535. [Google Scholar] [CrossRef]
- He, W.; Liu, X.; Hu, B.; Li, D.; Chen, L.; Li, Y.; Zhu, K.; Tu, Y.; Xiong, S.; Wang, G.; et al. Gender and ethnic disparities of acute kidney injury in COVID-19 infected patients: A literature review. Front. Cell Infect. Microbiol. 2022, 11, 778636. [Google Scholar] [CrossRef]
- Miller, S.; Brealey, J. Visualization of putative coronavirus in kidney. Kidney Int. 2020, 98, 231–232. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, function and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020, 183, 1735. [Google Scholar] [CrossRef]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin –converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef]
- Iwasaki, M.; Saito, J.; Saito, J.; Zhao, H.; Sakamoto, A.; Hirota, K.; Ma, D. Inflammation triggered by SARS-CoV-2 and ACE2 augment drives multiple organ failure of severe COVID-19: Molecular mechanisms and implications. Inflammation 2021, 44, 13–34. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Karki, R.; Kanneganti, T. The ‘cytokine storm’: Molecular mechanisms and therapeutic prospects. Trends Immunol. 2021, 42, 681–705. [Google Scholar] [CrossRef]
- Noris, M.; Benigni, A.; Remuzzi, G. The case of complement activation in COVID-19 multiorgan impact. Kidney Int. 2020, 98, 314–322. [Google Scholar] [CrossRef]
- Chowdhury, M.A.; Hossain, N.; Kashem, M.A.; Shahid, M.A.; Alam, A. Immune response in COVID-19: A review. J. Infect. Public Health 2020, 13, 1619–1629. [Google Scholar] [CrossRef]
- Casciola-Rosen, L.; Thiemann, D.R.; Andrade, F.; Zambrano, M.I.T.; Hooper, J.E.; Leonard, E.K.; Spangler, J.B.; Cox, A.L.; Machamer, C.E.; Sauer, L.; et al. IgM autoantibodies recognizing ACE2 are associated with severe COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Deng, Y.; Weng, Z.; Yang, L. Lymphopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 96, 131–135. [Google Scholar] [CrossRef]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 33. [Google Scholar] [CrossRef]
- Liu, J.; Li, S.; Liu, J.; Liang, B.; Wang, X.; Wang, H.; Li, W.; Tong, Q.; Yi, J.; Zhao, L.; et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. BioMedicine 2020, 55, 102763. [Google Scholar]
- Land, W. Role of DAMPS in respiratory virus-induced acute respiratory distress syndrome- with a preliminary reference to SARS-CoV-2 pneumonia. Genes Immun. 2021, 22, 141–160. [Google Scholar] [CrossRef]
- Xu, S.; Fu, L.; Fei, J.; Xiang, H.X.; Xiang, Y.; Tan, Z.X.; Li, M.D.; Liu, F.F.; Li, Y.; Han, M.F.; et al. Acute kidney injury at early stage as a negative prognostic indicator of patients with COVID-19: A hospital–based retrospective analysis. medRixv 2020. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef]
- Li, Q.; Ling, Y.; Zhang, J.; Li, W.; Zhang, X.; Jin, Y.; Li, L.; Fu, Q.; Huang, Y.; Lu, H.; et al. Clinical characteristics of SARS-CoV-2 infections involving 325 hospitalized patients outside Wuhan. BMC Inf. Dis. 2020. [Google Scholar] [CrossRef]
- Pei, G.; Zhang, Z.; Peng, J.; Liu, L.; Zhang, C.; Yu, C.; Ma, Z.; Huang, Y.; Liu, W.; Yao, Y.; et al. Renal involvement and early prognosis in patients with COVID-19 pneumonia. J. Am. Soc. Nephrol. 2020, 31, 1157–1165. [Google Scholar] [CrossRef]
- Fisher, M.; Neugarten, J.; Bellin, E.; Yunes, M.; Stahl, L.; Johns, T.; Abramowitz, M.; Levy, R.; Kumar, N.; Mokrzycki, M.; et al. AKI in hospitalized patients with and without COVID-19: A comparison study. J. Am. Soc. Nephrol. 2020, 31, 2145–2157. [Google Scholar] [CrossRef]
- Argenziano, M.G.; Bruce, S.L.; Slater, C.L.; Tiao, J.R.; Baldwin, M.R.; Barr, R.G.; Chang, B.P.; Chau, K.H.; Choi, J.J.; Gavin, N.; et al. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: Retrospective case series. BMJ 2020, 369, m1996. [Google Scholar] [CrossRef]
- Suleyman, G.; Fadel, R.A.; Malette, K.M.; Hammond, C.; Abdulla, H.; Entz, A.; Demertzis, Z.; Hanna, Z.; Failla, A.; Dagher, C.; et al. Clinical characteristics and morbidity associated with coronavirus disease 2019 in a series of patients in metropolitan Detroit. JAMA Netw. Open 2020, 3, e2012270. [Google Scholar] [CrossRef]
- Kohle, N.; Fluck, R.; Selby, N.; Taal, M. Acute kidney injury associated with COVID-19: A retrospective cohort study. PLoS Med. 2020, 17, e1003406. [Google Scholar]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.; et al. China Medical Treatment Expert Group for Covid-19. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Zahid, U.; Ramachandran, P.; Pitalewitz, S.; Alasadi, L.; Chakraborti, A.; Azhar, M.; Mikhalina, G.; Sherazi, A.; Narh, J.; Khattar, P.; et al. Acute kidney injury in COVID-19 patients: An inner city hospital experience and policy implications. Am. J. Nephrol. 2020, 51, 786–796. [Google Scholar] [CrossRef]
- Chan, L.; Chaudhary, K.; Saha, A.; Chauhan, K.; Vaid, A.; Zhao, S.; Paranjpe, I.; Somani, S.; Richter, F.; Miotto, R.; et al. AKI in hospitalized patients with COVID-19. J. Am. Soc. Nephrol. 2021, 32, 151–160. [Google Scholar] [CrossRef]
- Xu, H.; Garcia-Ptacek, S.; Annetorp, M.; Bruchfeld, A.; Cederholm, T.; Johnson, P.; Kivipelto, M.; Metzner, C.; Religa, D.; Eriksdotter, M. Acute kidney injury and mortality risk in older adults with COVID-19. J. Nephrol. 2021, 34, 295–304. [Google Scholar] [CrossRef]
- Ng, J.; Hirsch, J.; Hazzan, A.; Wanchoo, R.; Shah, H.; Malieckal, D.; Ross, D.; Sharma, P.; Sakhiya, V.; Fishbane, S.; et al. Northwell Nephrology COVID-19 Research Consortium. Outcomes among patients hospitalized with COVID-19 and acute kidney injury. Am. J. Kidney Dis. 2021, 77, 204–215. [Google Scholar] [CrossRef]
- Gameiro, J.; Fonseca, J.; Oliveira, J.; Marques, F.; Bernardo, J.; Costa, C.; Carreiro, C.; Braz, S.; Lopes, J. Acute kidney injury in hospitalized patients with COVID-19: A Portuguese cohort. Nefrologia 2021, 41, 689–698. [Google Scholar] [CrossRef]
- Walendy, V.; Girndt, M.; Greinert, D. COVID-19 and acute kidney injury in German hospitals 2020. PLoS ONE 2022, 17, e0264510. [Google Scholar] [CrossRef]
- Morieri, M.; Ronco, C.; Avogaro, A.; Farnia, F.; Shestakova, M.; Zaytseva, N.; Mokrysheva, N.; Akulkina, L.; Shepalina, A.; Brovko, M.; et al. In hospital risk factors for acute kidney injury and its burden in patients with SARS-CoV-2 infection: A longitudinal multinational study. Sci. Rep. 2022, 12, 3474. [Google Scholar] [CrossRef] [PubMed]
- Fabrizi, F.; Alfieri, C.; Molinari, P.; Tamborini, F.; Tangredi, M.; Sikharulidze, A.; Blasi, F.; Fracanzani, A.; Monzani, W.; Peyvandi, F.; et al. Acute kidney injury in non-intensive care unit (ICU) hospitalizations for coronavirus disease (COVID-19). Pathogens 2022, 11, 1272. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y.J.; Wilkins, K.J.; Alakwaa, F.; Liu, F.; Torre-Healy, L.A.; Krichevsky, S.; Hong, S.S.; Sakhuja, A.; Potu, C.K.; Saltz, J.H.; et al. COVID-19 associated AKI in hospitalized US patients: Temporal trends, geographical distribution, risk factors and mortality. medRxiv 2022. [Google Scholar] [CrossRef]
- Tan, B.; Tan, B.; Tan, A.; Schriver, E.; Gutierrez-Sacristan, A.; Das, P.; Yuan, W.; Hutch, M.; Barrio, N.; Jimenez, M.; et al. Long term kidney function recovery and mortality after COVID-19 associated acute kidney injury: An international multicentre observational cohort study. Lancet 2023, 55, 101724. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Han, C.; Yu, S.; Lee, H.; Kwon, S.; Kim, Y.; Lee, J.; Kim, D.; Oh, Y.; Lim, C.; et al. Trajectory of AKI and hospital mortality among patients with COVID-19. Renal Fail. 2023, 45, 2177086. [Google Scholar] [CrossRef] [PubMed]
- Shchepalina, A.; Chebotareva, N.; Akulkina, L.; Brovko, M.; Sholomova, V.; Androsova, T.; Korotchaeva, Y.; Kalmykova, D.; Tanaschuk, E.; Taranova, M.; et al. Acute kidney injury in hospitalized patients with COVID-19: Risk factors and serum biomarkers. Biomedicines 2023, 11, 1246. [Google Scholar] [CrossRef] [PubMed]
- Palomba, H.; Cubos, D.; Bozza, F.; Godinho Zampieri, F.; Gomes Romano, T. Development of a risk score for AKI onset in COVID-19 patients: COV-AKI score. BMC Nephrol. 2023, 24, 46. [Google Scholar] [CrossRef] [PubMed]
- McNicholas, B.A.; Rezoagli, E.; Simpkin, A.J.; Khanna, S.; Suen, J.Y.; Yeung, P.; Brodie, D.; Li Bassi, G.; Pham, T.; Bellani, G.; et al. Epidemiology and outcomes of early onset AKI in COVID-19-related ARDS in comparison with non-COVID-19 related ARDS: Insights from two prospective global cohort studies. Crit. Care 2023, 27, 3. [Google Scholar] [CrossRef] [PubMed]
- de Francisco, A.; Fresnedo, G. Long COVID-19 renal disease: A present medical need for nephrology. Nefrologia 2023, 43, 1–5. [Google Scholar] [CrossRef]
- Garrett, R.E.; Palacio, C.H.; Bar-Or, D. Long COVID: Is there a kidney link? Front. Med. 2023, 10, 1138644. [Google Scholar] [CrossRef]
- Aklilu, A.M.; Kumar, S.; Nugent, J.; Yamamoto, Y.; Coronel-Moreno, C.; Kadhim, B.; Faulkner, S.C.; O’connor, K.D.; Yasmin, F.; Greenberg, J.H.; et al. COVID-19 associated acute kidney injury and longitudinal kidney outcomes. JAMA Intern. Med. 2024, 184, 414–423. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Country | Sample Size, n | Male, n | Age, Years | Reference Year | Hypertension, n |
|---|---|---|---|---|---|---|
| Xu S, et al. [27] | China | 355 | 193 (54.4%) | 53.1 | 2020 | 125 (35.2%) |
| Li X, et al. [28] | China | 548 | 279 (50.9%) | 60 (48; 69) | 2020 | 166 (30.3%) |
| Li Q, et al. [29] | China | 325 | 167 (51.4%) | 51 (36; 64) | 2020 | 78 (24%) |
| Pei G, et al. [30] | China | 333 | 182 (54.7%) | 56.3 ± 13.4 | 2020 | 107 (32.2%) |
| Fisher M, et al. [31] | US | 3345 | 1776 (53.1%) | 64.4 ± 16.4 | 2020 | NA |
| Argenziano M, et al. [32] | US | 1000 | 596 (59.6%) | 63 (50; 75) | 2020 | 601 (60.1%) |
| Suleyman G, et al. [33] | US | 463 | 204 (44%) | 57.5 ± 16.8 | 2020 | 295 (63.7%) |
| Kolhe N, et al. [34] | UK | 1161 | 657 (56.6%) | 72.1 ± 15.9 | 2020 | NA |
| Guan W, et al. [35] | China | 1099 | 637 (57.9%) | 47 (35; 58) | 2020 | 165 (15%) |
| Cheng Y, et al. [36] | China | 701 | 367 (52.3%) | 63 (50; 71) | 2020 | 233 (33.4%) |
| Zahid U, et al. [37] | US | 469 | 268 (57.1%) | 64.2 ± 15.5 | 2020 | 323 (68.9%) |
| Chan L, et al. [38] | US | 3993 | 2289 (57.3%) | 64 (56; 78) | 2021 | 1527 (38.2%) |
| Xu H, et al. [39] | Sweden | 316 | 152 (48.0%) | 82.2 ± 8.5 | 2021 | 158 (50%) |
| Ng J, et al. [40] | US | 9657 | 5747 (59.5%) | 65.1 (51; 81) | 2021 | 5730 (59.3%) |
| Gameiro J, et al. [41] | Portugal | 192 | 100 (52.1%) | 72.2 ± 16.4 | 2021 | 131 (68.2%) |
| Walendy V, et al. [42] | Germany | 154,170 | 79,781 (51.8%) | NA | 2022 | 54,422 (35.3%) |
| Morieri M, et al. [43] | Italy/Russia | 939 | 497 (52.9%) | 62 ± 15.5 | 2022 | 511 (54.5%) |
| Fabrizi F, et al. [44] | Italy | 387 | 247 (63.8%) | 66 ± 15.8 | 2022 | 174 (44.9%) |
| Yoo Y, et al. [45] | US | 306,061 | 159,373 (52%) | 61.7 ± 18.8 | 2022 | 120,353 (51.8%) |
| Tan B, et al. [46] | International | 12,891 | 9611 (74.6%) | NA | 2023 | 6601 (51.2%) |
| Kim S, et al. [47] | Korea | 858 | 318 (37.1%) | 55.6 ± 20.2 | 2023 | 288 (33.6%) |
| Shchepalina A, et al. [48] | Russia | 500 | 231 (46.2%) | 73 (63; 80) | 2023 | 362 (72.4%) |
| Palomba H, et al. [49] | Brazil | 1131 | 678 (59.9%) | 52 ± 15.8 | 2023 | 722 (63.8%) |
| McNicholas B, et al. [50] | International | 1699 | 1112 (65.5%) | 56.8 | 2023 | 799 (47.0%) |
| Authors | Caucasian, n | CKD, n | Diabetes, n | AKI, n | ICU Admitted, n |
|---|---|---|---|---|---|
| Xu S, et al. [27] | NA | NA | 147 (41.4%) | 56 (15.7%) | NA |
| Li X, et al. [28] | NA | 10 (1.8%) | 83 (15.1%) | 95 (17.3%) | NA |
| Li Q, et al. [29] | NA | 4 (1.2%) | 30 (9.2%) | 19 (5.8%) | NA |
| Pei G, et al. [30] | NA | 0 | 76 (22.9%) | 35 (10.5%) | NA |
| Fisher M, et al. [31] | 275 (8.2%) | 409 (12.2%) | 906 (27.1%) | 1903 (56.9%) | 438 (13.1%) |
| Argenziano M, et al. [32] | 144 (14%) | 137 (13.7%) | 372 (37.2%) | 288 (33.9%) | 236 (23.6%) |
| Suleyman G, et al. [33] | NA | 182 (39.3%) | 178 (38.4%) | 159 (34.3%) | 141 (30.4%) |
| Kolhe N, et al. [34] | 876 (75.4%) | 224 (19.3%) | 255 (21.9%) | 304 (26.2%) | 96 (8.2%) |
| Guan W, et al. [35] | NA | 8 (0.7%) | 81 (7.4%) | 6 (0.5%) | 55 (5.0%) |
| Cheng Y, et al. [36] | NA | 14 (2%) | 100 (14.3%) | 36 (5.1%) | 73 (10.4%) |
| Zahid U, et al. [37] | 7 (1.5%) | NA | 219 (46.7%) | 128 (27.3%) | NA |
| Chan L, et al. [38] | 954 (23.9%) | 420 (10.5%) | 1019 (26%) | 1835 (46%) | 976 (24.4%) |
| Xu H, et al. [39] | NA | NA | 144 (45.5%) | 92 (29.1%) | NA |
| Ng J, et al. [40] | 3328 (34.4%) | 492 (5.1%) | 3469 (35.9%) | 3854 (39.9%) | 2409 (24.9%) |
| Gameiro J, et al. [41] | 174 (90.6%) | 38 (19.8%) | 54 (28.1%) | 106 (55.2%) | 38 (19.8%) |
| Walendy V, et al. [42] | NA | 23,380 (15.2%) | 20,504 (13.2%) | 16,773 (10.9%) | 29,329 (19%) |
| Morieri M, et al. [43] | NA | 194 (20.7%) | 292 (31.1%) | 140 (14.9%) | NA |
| Fabrizi F, et al. [44] | 387 (100%) | 40 (10.3%) | 65 (16.8%) | 119 (30.7%) | 0 |
| Yoo Y, et al. [45] | 192,482 (62.9%) | 23,380 (15.2%) NA | 70,494 (30.3%) | 126,478 (41%) | NA |
| Tan B, et al. [46] | 6215 (48.2%) | 4938 (38.3%) | NA | 6505 (50.4%) | NA |
| Kim S, et al. [47] | NA | 37 (4.3%) | 142 (16.5%) | 270 (31.5%) | 40 (4.7%) |
| Shchepalina A, et al. [48] | NA | 117 (23.4%) | 124 (24.8%) | 190 (38%) | 76 (15.2) |
| Palomba H, et al. [49] | NA | 33 (2.9%) | 269 (23.8%) | 376 (33.2%) | 1131 (100%) |
| McNicholas B, et al. [50] | NA | 0 | 509 (30.8%) | 355 (20.9%) | 1699 (100%) |
| Subgroup | Pooled AKI Risk |
|---|---|
| DM rate > 40%(n = 3) | 25% (23%; 28%) |
| DM rate < 15% (n = 5) | 11% (11%; 12%) |
| AH rate > 60% (n = 6) | 36% (34%; 38%) |
| AH rate < 25% (n = 2) | 3% (2%; 4%) |
| Age > 60 yrs (n = 14) | 41% (41%; 41%) |
| Age < 60 yrs (n = 8) | 28% (26%; 29%) |
| CKD rate > 20% (n = 4) | 49% (48%; 50%) |
| CKD rate < 10% (n = 8) | 37% (36%; 38%) |
| Reference year (2000) (n = 11) | 46% (45%; 47%) |
| Reference year (2003) (n = 5) | 33% (33%; 35%) |
| Male rate > 50% (n = 5) | 33% (32%; 37%) |
| Male rate < 50% (n = 5) | 33% (33%; 33%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabrizi, F.; Nardelli, L.; Regalia, A.; Zanoni, F.; Castellano, G. Are Kidneys Affected by SARS-CoV-2 Infection? An Updated Review on COVID-19-Associated AKI. Pathogens 2024, 13, 325. https://doi.org/10.3390/pathogens13040325
Fabrizi F, Nardelli L, Regalia A, Zanoni F, Castellano G. Are Kidneys Affected by SARS-CoV-2 Infection? An Updated Review on COVID-19-Associated AKI. Pathogens. 2024; 13(4):325. https://doi.org/10.3390/pathogens13040325
Chicago/Turabian StyleFabrizi, Fabrizio, Luca Nardelli, Anna Regalia, Francesca Zanoni, and Giuseppe Castellano. 2024. "Are Kidneys Affected by SARS-CoV-2 Infection? An Updated Review on COVID-19-Associated AKI" Pathogens 13, no. 4: 325. https://doi.org/10.3390/pathogens13040325
APA StyleFabrizi, F., Nardelli, L., Regalia, A., Zanoni, F., & Castellano, G. (2024). Are Kidneys Affected by SARS-CoV-2 Infection? An Updated Review on COVID-19-Associated AKI. Pathogens, 13(4), 325. https://doi.org/10.3390/pathogens13040325