
Dengue-Associated Hemophagocytic Lymphohistiocytosis: A Narrative Review of Its Identification and Treatment


Abstract
1. Introduction
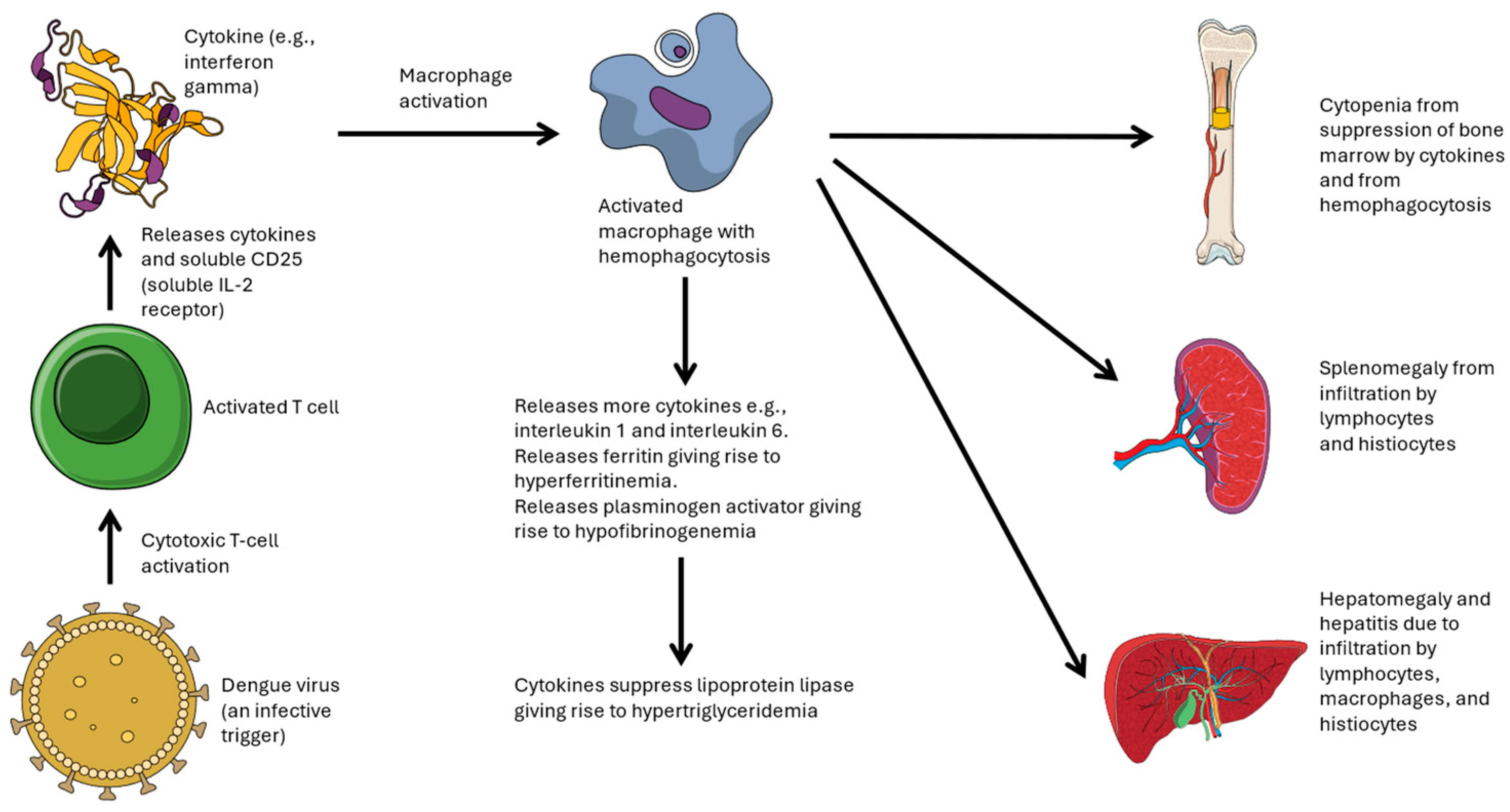
2. Pathophysiology and Presentation of Dengue-Associated HLH
3. Identification and Treatment of Dengue-Associated HLH in Adults and Children > 12 Years of Age

{kind=link}
{kind=link}
| Patient Characteristics (Reference) | Clinical Presentation and Identification of HLH | Treatment and Outcome |
|---|---|---|
| 25-year-old male (Acharya [60]) | Fever for 9 days, hepatosplenomegaly, hepatitis, pancytopenia, high ferritin (1121 mcg/L), high triglyceride (3.1 mmol/L), low fibrinogen (0.9 g/L), hemophagocytosis on bone marrow aspirate | IV dexamethasone 10 mg/m2 daily. IV etoposide twice a week for 2 weeks and once weekly for 6 weeks. Clinical recovery on day 8 of hospitalization. Complete recovery at 3 months of follow-up |
| 26-year-old male, no comorbid diseases (Arshad [63]) | Fever for 2 weeks, pancytopenia, hepatitis, high LDH, high triglyceride (3.2 mmol/L), high ferritin (24,459 mcg/L), hemophagocytosis on bone marrow aspirate | Supportive care without steroids. Death at hospitalization day 3 |
| 23-year-old female, 33-year-old man, both without comorbid conditions (Chang [51]) | Persistent and recurrent fever over >5 days, thrombocytopenia, hepatitis, high ferritin (8364–38,068 mcg/L), hemophagocytosis on bone marrow aspirate | IV dexamethasone 10 mg/m2 daily for 3–4 days, without any steroid taper. Both patients recovered fully |
| 30-year-old man, microcytic anemia of unknown cause (Cheo [49]) | Fever for 3 days, thrombocytopenia, hepatitis, high triglyceride (8.7 mmol/L), high ferritin (>40,000 mcg/L), hemophagocytosis on postmortem bone marrow | Supportive treatment without steroids. Death |
| 33-year-old female, no comorbid diseases (Chung [52]) | Fever for 3 days, splenomegaly, neutropenia, thrombocytopenia, hepatitis, high LDH (1775 U/L), high triglyceride (3.5 mmol/L), high ferritin (25,107 mcg/L) | IV dexamethasone 10 mg/m2 daily. Dexamethasone tapered over 2 weeks. Full recovery after 18 days of hospitalization |
| 21-year-old female, no comorbid diseases (De Koninck [57]) | Fever, leukopenia, thrombocytopenia, hepatitis, high ferritin (8208 mcg/L), hemophagocytosis on bone marrow aspirate | IV immunoglobulin G 1 g/kg/day body weight for 2 days. Full recovery after 14 days |
| 45-year-old female, with hypertension and diabetes mellitus (Ishak [44]) | Fever for 9 days, leukopenia, thrombocytopenia, hepatitis, high LDH (3627 U/L), high ferritin (31,013 mcg/L) | IV dexamethasone given, with improvement, hospital discharge on day 19 of illness, and normalized liver function on day 26 |
| 17, 19, 32-year-old males, all without comorbid diseases (Jamaludin [40]) | Fever for 2–5 days, anemia, thrombocytopenia, lymphopenia, hepatitis, high LDH (1054–5101 U/L), hepatomegaly, splenomegaly, high ferritin (17,432 to >40,000 mcg/L), high triglyceride (1.54–10.4 mmol/L), hemophagocytosis on bone marrow aspirate | For the first case, IV dexamethasone 10 mg/m2 daily, IV immunoglobulin 0.5 g/kg. Dexamethasone tapered over 2 weeks. For the second case, dexamethasone 4 mg TDS was administered for 2 days. For the third case, dexamethasone 4 mg TDS was administered for 1 day. All 3 patients achieved complete recovery |
| 18-year-old male, no comorbid diseases (Jha [50]) | Fever >3 weeks, hepatosplenomegaly, pancytopenia, high ferritin (10,550 mcg/L), high triglyceride (5.8 mmol/L), but no hemophagocytosis on bone marrow aspirate (i.e., false negative) | IV dexamethasone 10 mg/m2 daily (16 mg in this case) for 5 days, followed by oral dexamethasone taper over 3 weeks. Full recovery after 3 weeks |
| 33-year-old male, no comorbid diseases (Lu [64]) | Fever, thrombocytopenia, anemia, splenomegaly, hepatitis, high LDH (1243 U/L), hemophagocytosis on bone marrow aspirate (NB. No ferritin levels reported. Only 4 of the 8 HLH-2008 criteria met) | Supportive care without steroids. Complete recovery at 1 month of follow-up |
| 47-year-old male, diabetes mellitus. (Mizutani [45]) | Fever for 3 days, hepatitis, leucopenia, thrombocytopenia, high ferritin (9840 mcg/L), low fibrinogen (1.4 g/L), hemophagocytosis on bone marrow aspirate | Supportive care without steroids. Discharged after 9 days of hospitalization with complete recovery of blood counts. Remained well at 1 year of follow-up |
| 63-year-old female with asthma, chronic hepatitis B infection and hemoglobin H disease (Munshi [65]) | Fever, hepatomegaly, hepatitis, pancytopenia, high ferritin (>40,000 mcg/L), low fibrinogen (1.9 g/L), hemophagocytosis on bone marrow aspirate | Supportive care without steroids. Improvement and recovery |
| 28-year-old female, no comorbid diseases (Narayanasami [53]) | Fever for 6 days, hepatosplenomegaly, anemia, thrombocytopenia, hepatitis, high ferritin (72,100 mcg/L), hemophagocytosis on bone marrow aspirate | IV dexamethasone 10 mg/m2 daily for 3 days. Improvement with discharge after 11 days of hospitalization |
| 20-year-old male, 32-year-old male, both without comorbid conditions (Padmaprakash [58]) | Fever >7 days, hepatosplenomegaly, pancytopenia, hepatitis, high triglyceride (3–4 mmol/L), high ferritin (18,540 to >24,000 mcg/L), hemophagocytosis on bone marrow aspirate | IV immunoglobulin in both cases, IV dexamethasone in 1 case. Both survived |
| 17-year-old male, no comorbid diseases (Porel [61]) | Fever for 2 weeks, pancytopenia, hepatosplenomegaly, hepatitis, high LDH (8690 U/L), high triglyceride (3.3 mmol/L), high ferritin (1680 mcg/L), hemophagocytosis on bone marrow aspirate | Dexamethasone and etoposide following HLH-94 protocol. Significantly improved and discharged well from hospital |
| 17-year-old male, no comorbid conditions (Pradeep [54]) | Fever for >4 days, hepatosplenomegaly, hepatitis, persistent pancytopenia, high triglyceride (3.5 mmol/L), high ferritin (>3000 mcg/L), hemophagocytosis on bone marrow aspirate | IV dexamethasone 10 mg/m2 daily (17 mg/day in this patient) for 2 weeks, with steroid taper over 8 weeks. The fever settled within 24 h after starting IV dexamethasone. Complete recovery at 8 weeks follow-up |
| 24-year-old female, no comorbid diseases (Ray [55]) | Recurrent fever over 1 week, hepatosplenomegaly, anemia, leukopenia, thrombocytopenia, hepatitis, high LDH (2461 U/L), high triglyceride (6.0 mmol/L), high ferritin (2161 mcg/L), hemophagocytosis on bone marrow aspirate | IV dexamethasone 10 mg/m2 daily (16 mg/day in this patient), with steroid taper over 8 weeks, followed by dexamethasone pulses to maintain remission of HLH over weeks 9–40. Resolution and no reactivation at 6-month follow-up |
| 33-year-old man, no comorbid conditions (Ren [56]) | Fever for 9 days, hepatomegaly, thrombocytopenia, hepatitis, high ferritin (65,212 mcg/L), hemophagocytosis on bone marrow aspirate | Oral dexamethasone 20 mg daily for 2 weeks, followed by 10 mg daily for 4 days, 4 mg daily for 5 days, and then 2 mg daily for 3 days. Improved and discharged after 11 days of hospitalization. In remission at 1 month follow-up |
| 25-year-old female, 38-year-old man and 44-year-old female; all without comorbid diseases (Ribeiro [66]) | Fever, hepatosplenomegaly, leukopenia, thrombocytopenia, hepatitis, high LDH (779–1624 U/L), high ferritin (7093–23,451 mcg/L), high triglyceride (3.1–4.6 mmol/L), hemophagocytosis on bone marrow aspirate | Corticosteroids were given to all 3 patients. IV immunoglobulin given to 1 patient. All recovered after 2 weeks of treatment |
| 63-year-old female, Crohn’s disease treated with mercaptopurine and mesalamine, uterine cancer treated with hysterectomy, hypertension, hyperlipidemia, coronary artery disease, obesity, depression, previous thyroidectomy (reason not stated) (Sharp [47]) | Fever, leukopenia, thrombocytopenia, anemia, hepatitis, high LDH (727 U/L), high ferritin (>7500 mcg/L), low fibrinogen (<0.6 g/L), hemophagocytosis on bone marrow aspirate | Supportive therapy without steroids. Death at hospitalization day 12 from fulminant multiorgan failure |
| 14-year-old male, no comorbid conditions (Takkinsatian [67]) | Fever >7 days, hepatosplenomegaly, leukopenia, thrombocytopenia, high ferritin (>40,000 ng/L), low fibrinogen (1.49 g/L), hemophagocytosis on bone marrow aspirate | IV dexamethasone and IV immunoglobulin. Full recovery after 2 weeks |
| 16- to 43-year-old, 4 females, 2 males, one with previously undiagnosed diabetes mellitus (Tan [46]) | Persistent/recurrent fever >7 days, hepatomegaly, hepatitis, pancytopenia/bicytopenia, high ferritin (28,060–66,036 mcg/L), hemophagocytosis on bone marrow aspirate done for 3 patients. One patient also had high triglyceride and low fibrinogen levels | Supportive therapy without steroids in 2 patients. IV methylprednisolone in 4 patients (1 also had IV immunoglobulin G) with prednisolone taper during recovery. Recovery/improvement in 5 of 6 patients at hospital discharge. One patient died (a 43-year-old woman with previously undiagnosed diabetes mellitus) |
| 2 cases, 12 and 14 years old, 1 had beta-thalassemia major and 1 had trisomy 21 (Thadchanamoorthy [68]) | Persistent fever for >5 days, anemia, thrombocytopenia, hepatosplenomegaly, hepatitis, high LDH (1280–2106 U/L), high ferritin (6000–32,000 mcg/L), low fibrinogen (1.2 g/L), high triglyceride (2.8–3.2 mmol/L), hemophagocytosis on bone marrow aspirate | Steroid only for 1 patient. IV dexamethasone with IV immunoglobulin for 1 patient. Both recovered |
| 53-year-old male, no comorbid diseases (Wong [69]) | Fever, hepatosplenomegaly, hepatitis, anemia, thrombocytopenia, hemophagocytosis on bone marrow aspirate (NB: No ferritin levels reported. Only 4 of the 8 HLH-2008 criteria met) | “Systemic steroid” administered for 2 days prior to presentation. Complete recovery 1 week after presentation |
| 14-year-old male, 35-year-old female with morbid obesity, 56-year-old man (Yew [48]) | Fever for >3 days, bicytopenia, hepatitis, high LDH (2719 U/L), high triglyceride (3.2 mmol/L), high ferritin (35,023–93,026 mcg/L), hemophagocytosis on bone marrow aspirate | Supportive therapy without steroids for 1 patient. IV methylprednisolone 500 mg daily for 1–2 days for 2 patients. Complete recovery or improvement for all 3 patients |
4. Identification and Treatment of Dengue-Associated HLH in Young Children up to 12 Years of Age
| Patient Characteristics (Reference) | Clinical Presentation and Identification of HLH | Treatment and Outcome |
|---|---|---|
| 8-month-old male, no comorbid conditions (Arora [73]) | Recurrent fever >7 days, hepatosplenomegaly, hepatitis, high LDH (9116 U/L), bicytopenia, high ferritin (>40,000 mcg/L), low fibrinogen (0.76 g/L), high triglyceride (3.1 mmol/L), focal convulsion, embolic infarcts with diffuse leptomeningeal enhancement on MRI | IV dexamethasone 10 mg/m2 daily, IV etoposide, intrathecal methotrexate, intrathecal hydrocortisone. Death |
| 7 cases admitted to a pediatric ICU, median age 8 years, 5 (71.4%) males, no comorbid conditions (Bhattacharya [75]) | Fever for mean of 5 days, hepatomegaly, thrombocytopenia (mean platelet count 23,000/mm3), anemia (mean hemoglobin 8.1 g/dL), hepatitis, hemophagocytosis with bone marrow aspiration in all 7 cases | Steroids were given to 4 patients and all survived. No steroids given to 3 patients, with 2 deaths (28.6% mortality among all 7 cases) |
| 22 cases found from active case surveillance among hospitalized children with dengue in Puerto Rico, median age 1 year, 12 (55%) male, 3 (13.6%) were premature births, 10 (45.5%) had other chronic medical conditions (Ellis [25]) | Fever for median of 8 days, high ferritin (median 18,789 mcg/L), 17 (77.3%) had splenomegaly, 19 (86.4%) had hepatomegaly, 16 (72.7%) had anemia, 20 (90.9%) had thrombocytopenia, 17 (77.3%) had leukopenia, hemophagocytosis in 8 of 14 cases with bone marrow aspiration | Overall, 16 (72.7%) received corticosteroids, 13 (59.1%) received IV immunoglobulin, 8 (36.4%) received etoposide; 1 death out of 22 cases (4.5% case fatality rate) |
| 4-year-old female, no comorbid conditions (Gnanasambandam [72]) | Fever for 8 days, hepatomegaly, hepatitis, high triglyceride (2.8 mmol/L), thrombocytopenia, high ferritin (7500 mcg/L), low fibrinogen (1.3 g/L) | IV immunoglobulin 2 g/kg over 48 h. Recovery and hospital discharge |
| 1-week-old male, born at 33 weeks gestation, no comorbid conditions (Krishnappa [74]) | Encephalopathy, hepatomegaly, hepatitis, anemia, thrombocytopenia, low fibrinogen (1.3 g/L), high ferritin (34,718 mcg/L), low NK cell activity | IV immunoglobulin 0.5 g/kg once. IV dexamethasone 10 mg/m2 daily for 2 weeks. Improved from HLH. Had Staph hominis sepsis and Acinetobacter baumanii ventilator-associated pneumonia. Eventually recovered and discharged after 74 days of hospitalization |
| 27 cases, median 3 years old (range 4 months to 10 years) (Nandhakumar [13]) | Fever for 8 days on average, hepatitis, high ferritin (mean 26,620 mcg/L) | Overall, 18 improved with supportive care alone; 9 cases with hemodynamic instability, respiratory distress, and neurological involvement given steroids and IV immunoglobulin, with 4 deaths |
| 11 cases, 2–10 years of age, 6 male (54.5%) (Parajuli [76]) | Fever (100%), hepatomegaly (90.9%), splenomegaly (36.4%), cytopenias (90.9%), high triglyceride (18.2%), low fibrinogen (27.3%), high ferritin (mean 8311 mcg/L), hemophagocytosis (63.6%) | Six received IV dexamethasone, two received IV immunoglobulin. Five deaths (45.5%) |
| 10-year-old male, no comorbid diseases (Ray [77]) | Fever for 2 weeks, bicytopenia, hepatosplenomegaly, hepatitis, high LDH (1180 U/L), high triglyceride (3.9 mmol/L), high ferritin (2800 mcg/L) | Steroids and supportive care. Full recovery |
| 15 children, mean age 2 years, no comorbid diseases (Restrepo [26]) | Fever for >7 days (mean 10 days), hepatomegaly, anemia, hepatitis, high LDH (mean 4209 U/L), high triglyceride (mean 3.8 mmol/L) | Steroids given to 8 children (53%) with 50% survival, combined steroids and immunoglobulin given to 4 children (27%) with 25% survival (further details about disease severity not stated). Among all 15 cases, 4 deaths (27%) |
| 9 cases, mean age 10.4 years, no comorbid diseases (Singh [71]) | Splenomegaly, thrombocytopenia, hepatitis, high LDH (mean 7929 U/L), high ferritin (mean 34,593 mcg/L) | All received steroids; 2 deaths (22.2% mortality) |
| 3-year-old female, 10-year-old boy, both without comorbid conditions (Takkinsatian [67]) | Fever for >7 days, leukopenia, thrombocytopenia, hepatitis, high ferritin (>40,000 mcg/L), hemophagocytosis with bone marrow aspiration in both cases | IV dexamethasone 10 mg/m2 and IV immunoglobulin 0.5 g/kg daily. Full recovery after 1–2 weeks |
| 9-year-old female with obesity (Yew [48]) | Fever for >7 days, thrombocytopenia, hepatitis, high ferritin (97,316 mcg/L), low fibrinogen (0.95 g/L) | IV methylprednisolone 500 mg BD for 1 day. Full recovery on day 11 of illness |
5. Challenges in the Diagnosis and Treatment of Dengue-Associated HLH
6. Future Directions
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The Global Distribution and Burden of Dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Stanaway, J.D.; Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Coffeng, L.E.; Brady, O.J.; Hay, S.I.; Bedi, N.; Bensenor, I.M.; Castaneda-Orjuela, C.A.; et al. The Global Burden of Dengue: An Analysis from the Global Burden of Disease Study 2013. Lancet Infect. Dis. 2016, 16, 712–723. [Google Scholar] [CrossRef] [PubMed]
- Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Stanaway, J.D. The Global Economic Burden of Dengue: A Systematic Analysis. Lancet Infect. Dis. 2016, 16, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Capeding, M.R.; Tran, N.H.; Hadinegoro, S.R.; Ismail, H.I.; Chotpitayasunondh, T.; Chua, M.N.; Luong, C.Q.; Rusmil, K.; Wirawan, D.N.; Nallusamy, R.; et al. Clinical Efficacy and Safety of a Novel Tetravalent Dengue Vaccine in Healthy Children in Asia: A Phase 3, Randomised, Observer-Masked, Placebo-Controlled Trial. Lancet 2014, 384, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Villar, L.; Dayan, G.H.; Arredondo-Garcia, J.L.; Rivera, D.M.; Cunha, R.; Deseda, C.; Reynales, H.; Costa, M.S.; Morales-Ramirez, J.O.; Carrasquilla, G.; et al. Efficacy of a Tetravalent Dengue Vaccine in Children in Latin America. N. Engl. J. Med. 2015, 372, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Biswal, S.; Reynales, H.; Saez-Llorens, X.; Lopez, P.; Borja-Tabora, C.; Kosalaraksa, P.; Sirivichayakul, C.; Watanaveeradej, V.; Rivera, L.; Espinoza, F.; et al. Efficacy of a Tetravalent Dengue Vaccine in Healthy Children and Adolescents. N. Engl. J. Med. 2019, 381, 2009–2019. [Google Scholar] [CrossRef] [PubMed]
- Biswal, S.; Borja-Tabora, C.; Martinez Vargas, L.; Velasquez, H.; Theresa Alera, M.; Sierra, V.; Johana Rodriguez-Arenales, E.; Yu, D.; Wickramasinghe, V.P.; Duarte Moreira, E., Jr.; et al. Efficacy of a Tetravalent Dengue Vaccine in Healthy Children Aged 4–16 Years: A Randomised, Placebo-Controlled, Phase 3 Trial. Lancet 2020, 395, 1423–1433. [Google Scholar] [CrossRef]
- Kallas, E.G.; Cintra, M.A.T.; Moreira, J.A.; Patino, E.G.; Braga, P.E.; Tenorio, J.C.V.; Infante, V.; Palacios, R.; de Lacerda, M.V.G.; Batista Pereira, D.; et al. Live, Attenuated, Tetravalent Butantan-Dengue Vaccine in Children and Adults. N. Engl. J. Med. 2024, 390, 397–408. [Google Scholar] [CrossRef]
- Sridhar, S.; Luedtke, A.; Langevin, E.; Zhu, M.; Bonaparte, M.; Machabert, T.; Savarino, S.; Zambrano, B.; Moureau, A.; Khromava, A.; et al. Effect of Dengue Serostatus on Dengue Vaccine Safety and Efficacy. N. Engl. J. Med. 2018, 379, 327–340. [Google Scholar] [CrossRef]
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Durbin, A.P. Dengue Vascular Leak Syndrome: Insights into Potentially New Treatment Modalities. J. Clin. Investig. 2019, 129, 4072–4073. [Google Scholar] [CrossRef]
- Ishii, E.; Ohga, S.; Imashuku, S.; Yasukawa, M.; Tsuda, H.; Miura, I.; Yamamoto, K.; Horiuchi, H.; Takada, K.; Ohshima, K.; et al. Nationwide Survey of Hemophagocytic Lymphohistiocytosis in Japan. Int. J. Hematol. 2007, 86, 58–65. [Google Scholar] [CrossRef]
- Nandhakumar, D.; Loganatha, A.; Sivasankaran, M.; Sivabalan, S.; Munirathnam, D. Hemophagocytic Lymphohistiocytosis in Children. Indian J. Pediatr. 2020, 87, 526–531. [Google Scholar] [CrossRef]
- Simon, A.C.; Delhi Kumar, C.G.; Basu, D.; Ramesh Kumar, R. Hemophagocytic Lymphohistiocytosis in Children: Clinical Profile and Outcome. J. Pediatr. Hematol. Oncol. 2020, 42, e281–e285. [Google Scholar] [CrossRef] [PubMed]
- Autexier, C.; Greider, C.W. Mutational Analysis of the Tetrahymena Telomerase Rna: Identification of Residues Affecting Telomerase Activity In Vitro. Nucleic Acids Res. 1998, 26, 787–795. [Google Scholar] [CrossRef][Green Version]
- Riviere, S.; Galicier, L.; Coppo, P.; Marzac, C.; Aumont, C.; Lambotte, O.; Fardet, L. Reactive Hemophagocytic Syndrome in Adults: A Retrospective Analysis of 162 Patients. Am. J. Med. 2014, 127, 1118–1125. [Google Scholar] [CrossRef]
- Fukaya, S.; Yasuda, S.; Hashimoto, T.; Oku, K.; Kataoka, H.; Horita, T.; Atsumi, T.; Koike, T. Clinical Features of Haemophagocytic Syndrome in Patients with Systemic Autoimmune Diseases: Analysis of 30 Cases. Rheumatology 2008, 47, 1686–1691. [Google Scholar] [CrossRef]
- Ferreri, A.J.; Dognini, G.P.; Campo, E.; Willemze, R.; Seymour, J.F.; Bairey, O.; Martelli, M.; De Renz, A.O.; Doglioni, C.; Montalban, C.; et al. Variations in Clinical Presentation, Frequency of Hemophagocytosis and Clinical Behavior of Intravascular Lymphoma Diagnosed in Different Geographical Regions. Haematologica 2007, 92, 486–492. [Google Scholar] [CrossRef]
- Lehmberg, K.; Sprekels, B.; Nichols, K.E.; Woessmann, W.; Muller, I.; Suttorp, M.; Bernig, T.; Beutel, K.; Bode, S.F.; Kentouche, K.; et al. Malignancy-Associated Haemophagocytic Lymphohistiocytosis in Children and Adolescents. Br. J. Haematol. 2015, 170, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Nikiforow, S.; Berliner, N. The Unique Aspects of Presentation and Diagnosis of Hemophagocytic Lymphohistiocytosis in Adults. Hematol. Am. Soc. Hematol. Educ. Program. 2015, 2015, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Stepp, S.E.; Dufourcq-Lagelouse, R.; Le Deist, F.; Bhawan, S.; Certain, S.; Mathew, P.A.; Henter, J.I.; Bennett, M.; Fischer, A.; de Saint Basile, G.; et al. Perforin Gene Defects in Familial Hemophagocytic Lymphohistiocytosis. Science 1999, 286, 1957–1959. [Google Scholar] [CrossRef]
- Niece, J.A.; Rogers, Z.R.; Ahmad, N.; Langevin, A.M.; McClain, K.L. Hemophagocytic Lymphohistiocytosis in Texas: Observations on Ethnicity and Race. Pediatr. Blood Cancer 2010, 54, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Brito-Zeron, P.; Lopez-Guillermo, A.; Khamashta, M.A.; Bosch, X. Adult Haemophagocytic Syndrome. Lancet 2014, 383, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Hayden, A.; Park, S.; Giustini, D.; Lee, A.Y.; Chen, L.Y. Hemophagocytic Syndromes (Hpss) Including Hemophagocytic Lymphohistiocytosis (Hlh) in Adults: A Systematic Scoping Review. Blood Rev. 2016, 30, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E.M.; Sharp, T.M.; Perez-Padilla, J.; Gonzalez, L.; Poole-Smith, B.K.; Lebo, E.; Baker, C.; Delorey, M.J.; Torres-Velasquez, B.; Ochoa, E.; et al. Incidence and Risk Factors for Developing Dengue-Associated Hemophagocytic Lymphohistiocytosis in Puerto Rico, 2008–2013. PLoS Negl. Trop. Dis. 2016, 10, e0004939. [Google Scholar] [CrossRef] [PubMed]
- Restrepo Arias, V.C.; Salgado Garcia, D.M.; Merchan-Galvis, A.M.; Narvaez, C.F. Clinical and Laboratory Characteristics of Hemophagocytic Lymphohistiocytosis in Children with Severe Dengue during the 2019–2020 Outbreak in Southern Colombia. Pediatr. Infect. Dis. J. 2023, 42, e204–e211. [Google Scholar] [CrossRef] [PubMed]
- Che Isa, Z.; Lim, J.A.; Ain, A.M.; Othman, F.A.; Kueh, Y.C.; Tew, M.M.; Masnan, M.J.; Ibrahim, A. Clinical Profiles and Predictors of Survival in Severe Dengue Cases. Singap. Med. J. 2023. [Google Scholar] [CrossRef] [PubMed]
- Tayal, A.; Kabra, S.K.; Lodha, R. Management of Dengue: An Updated Review. Indian J. Pediatr. 2023, 90, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.J.; Chung, J.S.; Lee, J.J.; Sohn, S.K.; Choi, Y.J.; Kim, Y.K.; Yang, D.H.; Kim, H.J.; Kim, J.G.; Joo, Y.D.; et al. Treatment Outcomes with Chop Chemotherapy in Adult Patients with Hemophagocytic Lymphohistiocytosis. J. Korean Med. Sci. 2008, 23, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Arca, M.; Fardet, L.; Galicier, L.; Riviere, S.; Marzac, C.; Aumont, C.; Lambotte, O.; Coppo, P. Prognostic Factors of Early Death in a Cohort of 162 Adult Haemophagocytic Syndrome: Impact of Triggering Disease and Early Treatment with Etoposide. Br. J. Haematol. 2015, 168, 63–68. [Google Scholar] [CrossRef]
- Otrock, Z.K.; Eby, C.S. Clinical Characteristics, Prognostic Factors, and Outcomes of Adult Patients with Hemophagocytic Lymphohistiocytosis. Am. J. Hematol. 2015, 90, 220–224. [Google Scholar] [CrossRef]
- Giang, H.T.N.; Banno, K.; Minh, L.H.N.; Trinh, L.T.; Loc, L.T.; Eltobgy, A.; Tai, L.L.T.; Khan, A.; Tuan, N.H.; Reda, Y.; et al. Dengue Hemophagocytic Syndrome: A Systematic Review and Meta-Analysis on Epidemiology, Clinical Signs, Outcomes, and Risk Factors. Rev. Med. Virol. 2018, 28, e2005. [Google Scholar] [CrossRef] [PubMed]
- Kan, F.K.; Tan, C.C.; Von Bahr Greenwood, T.; Khalid, K.E.; Supramaniam, P.; Hed Myrberg, I.; Tan, L.H.; Henter, J.I. Dengue Infection Complicated by Hemophagocytic Lymphohistiocytosis: Experiences from 180 Patients with Severe Dengue. Clin. Infect. Dis. 2020, 70, 2247–2255. [Google Scholar] [CrossRef] [PubMed]
- Filipovich, A.; McClain, K.; Grom, A. Histiocytic Disorders: Recent Insights into Pathophysiology and Practical Guidelines. Biol. Blood Marrow Transpl. 2010, 16, S82–S89. [Google Scholar] [CrossRef] [PubMed]
- Hines, M.R.; von Bahr Greenwood, T.; Beutel, G.; Beutel, K.; Hays, J.A.; Horne, A.; Janka, G.; Jordan, M.B.; van Laar, J.A.M.; Lachmann, G.; et al. Consensus-Based Guidelines for the Recognition, Diagnosis, and Management of Hemophagocytic Lymphohistiocytosis in Critically Ill Children and Adults. Crit. Care Med. 2022, 50, 860–872. [Google Scholar] [CrossRef] [PubMed]
- Keenan, C.; Nichols, K.E.; Albeituni, S. Use of the JAK Inhibitor Ruxolitinib in the Treatment of Hemophagocytic Lymphohistiocytosis. Front. Immunol. 2021, 12, 614704. [Google Scholar] [CrossRef] [PubMed]
- Bergsten, E.; Horne, A.; Arico, M.; Astigarraga, I.; Egeler, R.M.; Filipovich, A.H.; Ishii, E.; Janka, G.; Ladisch, S.; Lehmberg, K.; et al. Confirmed Efficacy of Etoposide and Dexamethasone in Hlh Treatment: Long-Term Results of the Cooperative Hlh-2004 Study. Blood 2017, 130, 2728–2738. [Google Scholar] [CrossRef] [PubMed]
- Palazzi, D.L.; McClain, K.L.; Kaplan, S.L. Hemophagocytic Syndrome in Children: An Important Diagnostic Consideration in Fever of Unknown Origin. Clin. Infect. Dis. 2003, 36, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Hejblum, G.; Lambotte, O.; Galicier, L.; Coppo, P.; Marzac, C.; Aumont, C.; Fardet, L. A Web-Based Delphi Study for Eliciting Helpful Criteria in the Positive Diagnosis of Hemophagocytic Syndrome in Adult Patients. PLoS ONE 2014, 9, e94024. [Google Scholar] [CrossRef] [PubMed]
- Wan Jamaludin, W.F.; Periyasamy, P.; Wan Mat, W.R.; Abdul Wahid, S.F. Dengue Infection Associated Hemophagocytic Syndrome: Therapeutic Interventions and Outcome. J. Clin. Virol. 2015, 69, 91–95. [Google Scholar] [CrossRef]
- Henter, J.I.; Horne, A.; Arico, M.; Egeler, R.M.; Filipovich, A.H.; Imashuku, S.; Ladisch, S.; McClain, K.; Webb, D.; Winiarski, J.; et al. Hlh-2004: Diagnostic and Therapeutic Guidelines for Hemophagocytic Lymphohistiocytosis. Pediatr. Blood Cancer 2007, 48, 124–131. [Google Scholar] [CrossRef]
- Bilston, L.; Croden, J.; Taparia, M.; Karkhaneh, M.; Grossman, J.; Sun, H.L. Validation of the Hscore and the Hlh-2004 Diagnostic Criteria for the Diagnosis of Hemophagocytic Lymphohistiocytosis in a Multicenter Cohort. Eur. J. Haematol. 2022, 109, 129–137. [Google Scholar] [CrossRef]
- Mahabala, C.; Koushik, V.K.; Manjrekar, P.A.; Balanthimogru, P. Serum Soluble Interleukin-2 Receptor (Sil-2r) Is an Accurate Biomarker for Dengue-Associated Hemophagocytic Lymphohistiocytosis Syndrome Diagnosed by Hscore. Infection 2023, 51, 433–438. [Google Scholar] [CrossRef]
- Ishak, S.H.; Yaacob, L.H.; Ishak, A. Severe Dengue with Hemophagocytosis Syndrome. Malays. Fam. Physician 2020, 15, 47–49. [Google Scholar]
- Mizutani, N.; Kenzaka, T.; Nishisaki, H. Dengue Fever Complicated with Hemophagocytic Lymphohistiocytosis: A Case Report of Resolution with Steroid-Sparing Supportive Care. Trop. Med. Infect. Dis. 2023, 8, 497. [Google Scholar] [CrossRef]
- Tan, L.H.; Lum, L.C.; Omar, S.F.; Kan, F.K. Hemophagocytosis in Dengue: Comprehensive Report of Six Cases. J. Clin. Virol. 2012, 55, 79–82. [Google Scholar] [CrossRef]
- Sharp, T.M.; Gaul, L.; Muehlenbachs, A.; Hunsperger, E.; Bhatnagar, J.; Lueptow, R.; Santiago, G.A.; Munoz-Jordan, J.L.; Blau, D.M.; Ettestad, P.; et al. Fatal Hemophagocytic Lymphohistiocytosis Associated with Locally Acquired Dengue Virus Infection—New Mexico and Texas, 2012. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 49–54. [Google Scholar]
- Jasmine, Y.S.; Lee, S.L.; Kan, F.K. Infection Associated Haemophagocytic Syndrome in Severe Dengue Infection—A Case Series in a District Hospital. Med. J. Malays. 2017, 72, 62–64. [Google Scholar]
- Cheo, S.W.; Abdul Rashid, W.; Ho, C.V.; Ahmad Akhbar, R.Z.; Low, Q.J.; Rajahram, G.S. Haemophagocytic Lymphohistiocytosis Secondary to Dengue Fever: A Case Report. Hong Kong Med. J. 2021, 27, 287–289. [Google Scholar] [CrossRef]
- Jha, V.K.; Khurana, H.; Balakrishnan, A. Prolonged Fever and Pancytopenia in a Case of Severe Dengue May Be Secondary Hemophagocytic Lymphohistiocytosis. Med. J. Armed Forces India 2022, 78 (Suppl. S1), S300–S302. [Google Scholar] [CrossRef]
- Chang, C.Y.; Rajappan, M.; Zaid, M.; Ong, E.L.C. Dengue Fever Complicated by Hemophagocytic Lymphohistiocytosis: Report of 2 Cases and Bone Marrow Findings. Clin. Case Rep. 2020, 8, 3427–3431. [Google Scholar] [CrossRef]
- Chung, S.M.; Song, J.Y.; Kim, W.; Choi, M.J.; Jeon, J.H.; Kang, S.; Jung, E.; Noh, J.Y.; Cheong, H.J.; Kim, W.J. Dengue-Associated Hemophagocytic Lymphohistiocytosis in an Adult: A Case Report and Literature Review. Medicine 2017, 96, e6159. [Google Scholar] [CrossRef]
- Narayanasami, E.; Umakanth, M.; Suganthan, N. Dengue Hemorrhagic Fever Complicated with Hemophagocytic Lymphohistiocytosis in an Adult with Diabetic Ketoacidosis. Cureus 2020, 12, e10172. [Google Scholar] [CrossRef]
- Pradeep, C.; Karunathilake, P.; Abeyagunawardena, S.; Ralapanawa, U.; Jayalath, T. Hemophagocytic Lymphohistiocytosis as a Rare Complication of Dengue Haemorrhagic Fever: A Case Report. J. Med. Case Rep. 2023, 17, 224. [Google Scholar] [CrossRef]
- Ray, S.; Kundu, S.; Saha, M.; Chakrabarti, P. Hemophagocytic Syndrome in Classic Dengue Fever. J. Glob. Infect. Dis. 2011, 3, 399–401. [Google Scholar] [CrossRef]
- Ren, D.; Ong, S.W.X.; Batac, J.A.L.; Fan, B.E.; Vasoo, S. Haemophagocytic Lymphohistiocytosis in Dengue Fever. Lancet Infect. Dis. 2021, 21, 437. [Google Scholar] [CrossRef]
- De Koninck, A.S.; Dierick, J.; Steyaert, S.; Taelman, P. Hemophagocytic Lymphohistiocytosis and Dengue Infection: Rare Case Report. Acta Clin. Belg. 2014, 69, 210–213. [Google Scholar] [CrossRef]
- Padmaprakash, K.V.; Jha, V.K.; Sowmya Karantha, C.; Anurag Singh, C.; Kamal, D.; Jambunathan, P. Rescue Therapy with Intravenous Immunoglobulin in Severe Refractory Dengue: A Pilot Study. Med. J. Armed Forces India 2022, 78, 204–212. [Google Scholar] [CrossRef]
- Gambertoglio, J.G.; Frey, F.J.; Holford, N.H.; Birnbaum, J.L.; Lizak, P.S.; Vincenti, F.; Feduska, N.J.; Salvatierra, O., Jr.; Amend, W.J., Jr. Prednisone and Prednisolone Bioavailability in Renal Transplant Patients. Kidney Int. 1982, 21, 621–626. [Google Scholar] [CrossRef]
- Acharya, S.; Shukla, S.; Sontakke, T.; Vs, I.; Bagga, C.; Dronamraju, S.; Giri, A. A Case Report of Hemophagocytic Lymphohistiocytosis (HLH)—An Unusual Complication of Dengue Infection. Cureus 2022, 14, e26504. [Google Scholar] [CrossRef]
- Porel, R.; Kumar, V.; Agarwal, K.; Biswas, R.; Ojha, V.S. Secondary Hemophagocytic Lymphohistiocytosis: A Series of Three Cases. Cureus 2023, 15, e46044. [Google Scholar] [CrossRef]
- Mayurathan, P. Dengue Hemorrhagic Fever Causing Postpartum Hemorrhage and Hemophagocytic Lymphohistiocytosis in a Young Woman: A Case Report. Cureus 2024, 16, e53841. [Google Scholar] [CrossRef]
- Arshad, U.; Ahmad, S.Q.; Khan, F. Hemophagocytic Lymphohistiocytosis in a Patient with Dengue Infection. Hematol. Oncol. Stem Cell Ther. 2015, 8, 189–190. [Google Scholar] [CrossRef]
- Lu, P.L.; Hsiao, H.H.; Tsai, J.J.; Chen, T.C.; Feng, M.C.; Chen, T.P.; Lin, S.F. Dengue Virus-Associated Hemophagocytic Syndrome and Dyserythropoiesis: A Case Report. Kaohsiung J. Med. Sci. 2005, 21, 34–39. [Google Scholar] [CrossRef]
- Munshi, A.; Alsuraihi, A.; Balubaid, M.; Althobaiti, M.; Althaqafi, A. Dengue-Induced Hemophagocytic Lymphohistiocytosis: A Case Report and Literature Review. Cureus 2021, 13, e20172. [Google Scholar] [CrossRef]
- Ribeiro, E.; Kassab, S.; Pistone, T.; Receveur, M.C.; Fialon, P.; Malvy, D. Primary Dengue Fever Associated with Hemophagocytic Syndrome: A Report of Three Imported Cases, Bordeaux, France. Intern. Med. 2014, 53, 899–902. [Google Scholar] [CrossRef][Green Version]
- Takkinsatian, P.; Sowithayasakul, P.; Prommalikit, O. Dengue Associated Haemophagocytic Lymphohystiocytosis: An Often-Missed Complication of a Common Infection. Med. J. Malays. 2020, 75, 588–590. [Google Scholar]
- Thadchanamoorthy, V.; Dayasiri, K. Dengue Fever Associated Haemophagocytic Lymphohistiocytosis: A Report of Two Children. Cureus 2020, 12, e11232. [Google Scholar] [CrossRef]
- Wong, K.F.; Chan, J.K.; Chan, J.C.; Lim, W.W.; Wong, W.K. Dengue Virus Infection-Associated Hemophagocytic Syndrome. Am. J. Hematol. 1991, 38, 339–340. [Google Scholar] [CrossRef]
- Bain, B.J. Bone Marrow Biopsy Morbidity: Review of 2003. J. Clin. Pathol. 2005, 58, 406–408. [Google Scholar] [CrossRef]
- Singh, D.; Raghunathan, V.; Dhaliwal, M.; Rastogi, N.; Chadha, R.; Yadav, S.P. Soluble Interleukin-2 Receptor Level as a Marker of Hemophagocytic Lymphohistiocytosis in Children with Severe Dengue. Front. Pediatr. 2021, 9, 721857. [Google Scholar] [CrossRef]
- Gnanasambandam, J.; Geminiganesan, S.; Vilvanathan, V.; Sankaranarayanan, S.; Padmanabhan, R. Secondary Hemophagocytic Lymphohistiocytosis—A Common Ramification of Different Diseases. EJIFCC 2022, 33, 63–69. [Google Scholar] [PubMed]
- Arora, A.; Verma, S.; Khot, N.; Chalipat, S.; Agarkhedkar, S.; Kiruthiga, K.G. A Case Report on CNS Hemophagocytic Lymphohistiocytosis in an Infant with Dengue Hemorrhagic Fever. Cureus 2023, 15, e34773. [Google Scholar] [CrossRef]
- Krishnappa, A.; Munusamy, J.; Ray, S.; Rameshbabu, M.; Bhatia, P.; Roy, P.S.; Sundaram, V.; Kumar, P. Neonatal Dengue with HLH: Perks of Early Diagnosis and Management. J. Pediatr. Hematol. Oncol. 2021, 43, e770–e773. [Google Scholar] [CrossRef]
- Bhattacharya, D.; Angurana, S.K.; Nallasamy, K.; Iyer, R.; Jayashree, M. Severe Dengue and Associated Hemophagocytic Lymphohistiocytosis in PICU. Indian J. Pediatr. 2019, 86, 1094–1098. [Google Scholar] [CrossRef]
- Parajuli, B.; Angurana, S.K.; Awasthi, P.; Nallasamy, K.; Baranwal, A.; Bansal, A.; Bansal, D.; Rawat, A.; Varma, N.; Jayashree, M. Hemophagocytic Lymphohistiocytosis in a Picu of a Developing Economy: Clinical Profile, Intensive Care Needs, Outcome, and Predictors of Mortality. Pediatr. Crit. Care Med. 2021, 22, e44–e57. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.; Kumar, M.; Mahajan, N.; Khatri, A. Paediatric Hemophagocytic Lymphohistiocytosis: A Case Series with a Diverse Spectrum from a Resource-Limited Setting. Cureus 2023, 15, e45140. [Google Scholar] [CrossRef]
- Balis, F.M.; Lester, C.M.; Chrousos, G.P.; Heideman, R.L.; Poplack, D.G. Differences in Cerebrospinal Fluid Penetration of Corticosteroids: Possible Relationship to the Prevention of Meningeal Leukemia. J. Clin. Oncol. 1987, 5, 202–207. [Google Scholar] [CrossRef]
- Spoorenberg, S.M.; Deneer, V.H.; Grutters, J.C.; Pulles, A.E.; Voorn, G.P.; Rijkers, G.T.; Bos, W.J.; van de Garde, E.M. Pharmacokinetics of Oral vs. Intravenous Dexamethasone in Patients Hospitalized with Community-Acquired Pneumonia. Br. J. Clin. Pharmacol. 2014, 78, 78–83. [Google Scholar] [CrossRef]
- Carter, S.J.; Tattersall, R.S.; Ramanan, A.V. Macrophage Activation Syndrome in Adults: Recent Advances in Pathophysiology, Diagnosis and Treatment. Rheumatology 2019, 58, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Cleves, D.; Lotero, V.; Medina, D.; Perez, P.M.; Patino, J.A.; Torres-Canchala, L.; Olaya, M. Pediatric Hemophagocytic Lymphohistiocytosis: A Rarely Diagnosed Entity in a Developing Country. BMC Pediatr. 2021, 21, 411. [Google Scholar] [CrossRef]
- Cerqueira, F.P.; Jesus, A.M.C.; Cotrim, M.D. Adaptive Design: A Review of the Technical, Statistical, and Regulatory Aspects of Implementation in a Clinical Trial. Ther. Innov. Regul. Sci. 2020, 54, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Jordan, M.B.; Allen, C.; Cesaro, S.; Rizzari, C.; Rao, A.; Degar, B.; Garrington, T.P.; Sevilla, J.; Putti, M.C.; et al. Emapalumab in Children with Primary Hemophagocytic Lymphohistiocytosis. N. Engl. J. Med. 2020, 382, 1811–1822. [Google Scholar] [CrossRef] [PubMed]
- Dufranc, E.; Del Bello, A.; Belliere, J.; Kamar, N.; Faguer, S.; Taidi Study Group. IIl6-R Blocking with Tocilizumab in Critically Ill Patients with Hemophagocytic Syndrome. Crit. Care 2020, 24, 166. [Google Scholar] [CrossRef] [PubMed]
- Baverez, C.; Grall, M.; Gerfaud-Valentin, M.; De Gail, S.; Belot, A.; Perpoint, T.; Weber, E.; Reynaud, Q.; Seve, P.; Jamilloux, Y. Anakinra for the Treatment of Hemophagocytic Lymphohistiocytosis: 21 Cases. J. Clin. Med. 2022, 11, 5799. [Google Scholar] [CrossRef]
- Ge, J.; Zhang, Q.; Ma, H.; Wang, D.; Zhao, Y.; Zhu, T.; Wang, W.; Zhou, C.; Wei, A.; Lian, H.; et al. Ruxolitinib-Based Regimen in Children with Primary Hemophagocytic Lymphohistiocytosis. Haematologica 2024, 109, 458–465. [Google Scholar] [CrossRef]


| Management Step | Initial Actions | Further Actions |
|---|---|---|
| Diagnosis | Consider HLH routinely in all cases of severe dengue. In addition, suspect HLH based on the presence of any of the following in a patient with dengue: (1) prolonged or recurrent fever of >7 days; (2) anemia without intravascular hemolysis or massive bleeding | Send blood tests for triglycerides, fibrinogen, and ferritin. Send blood tests for NK-cell-activity and high-soluble interleukin-2-receptor if available. Perform bone marrow aspirate for hemophagocytosis if possible. The presence of at least 5 of the 8 HLH-2004 criteria confirms HLH *. Rule out other associations of HLH (other infections, autoimmune diseases, and malignancy) |
| Treatment | Maintain adequate hydration. Correct anemia. Correct thrombocytopenia if bleeding. Supportive care for organ dysfunction. If bacterial co-infection is suspected, then obtain blood cultures and administer broad-spectrum antibiotics promptly | Consider IV methylprednisolone 1 g/kg or IV dexamethasone 10 mg/m2 daily for 3–4 days or more, contingent on improvement of clinical and laboratory parameters. Steroids may be oral and tapered over 2 or more weeks, contingent on improvement of clinical and laboratory parameters. Consider IV immunoglobulin and/or etoposide as rescue therapy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
See, K.C. Dengue-Associated Hemophagocytic Lymphohistiocytosis: A Narrative Review of Its Identification and Treatment. Pathogens 2024, 13, 332. https://doi.org/10.3390/pathogens13040332
See KC. Dengue-Associated Hemophagocytic Lymphohistiocytosis: A Narrative Review of Its Identification and Treatment. Pathogens. 2024; 13(4):332. https://doi.org/10.3390/pathogens13040332
Chicago/Turabian StyleSee, Kay Choong. 2024. "Dengue-Associated Hemophagocytic Lymphohistiocytosis: A Narrative Review of Its Identification and Treatment" Pathogens 13, no. 4: 332. https://doi.org/10.3390/pathogens13040332
APA StyleSee, K. C. (2024). Dengue-Associated Hemophagocytic Lymphohistiocytosis: A Narrative Review of Its Identification and Treatment. Pathogens, 13(4), 332. https://doi.org/10.3390/pathogens13040332