
Predictor Variables in the Spread of Chagas Disease in Rural Areas



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
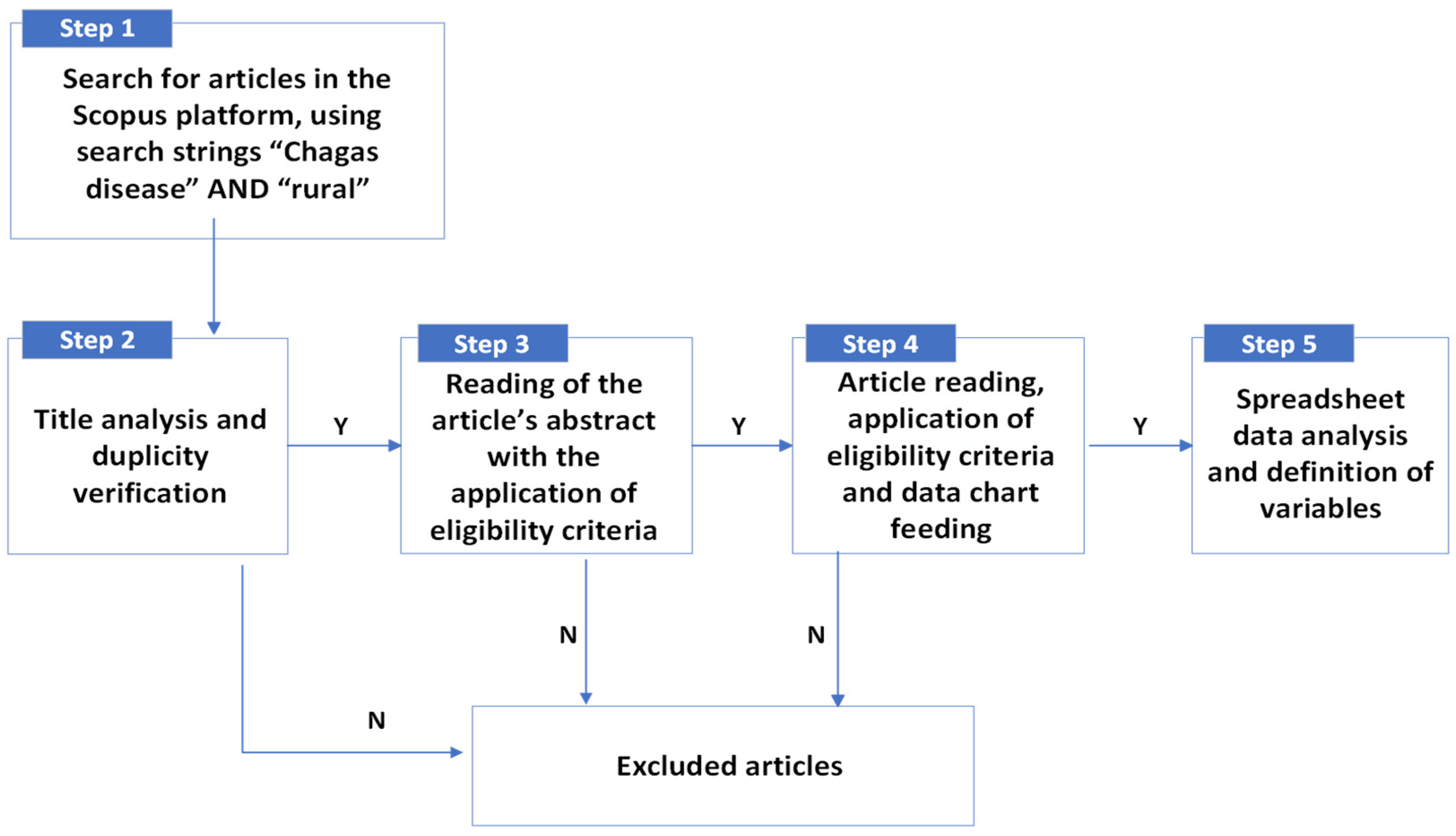
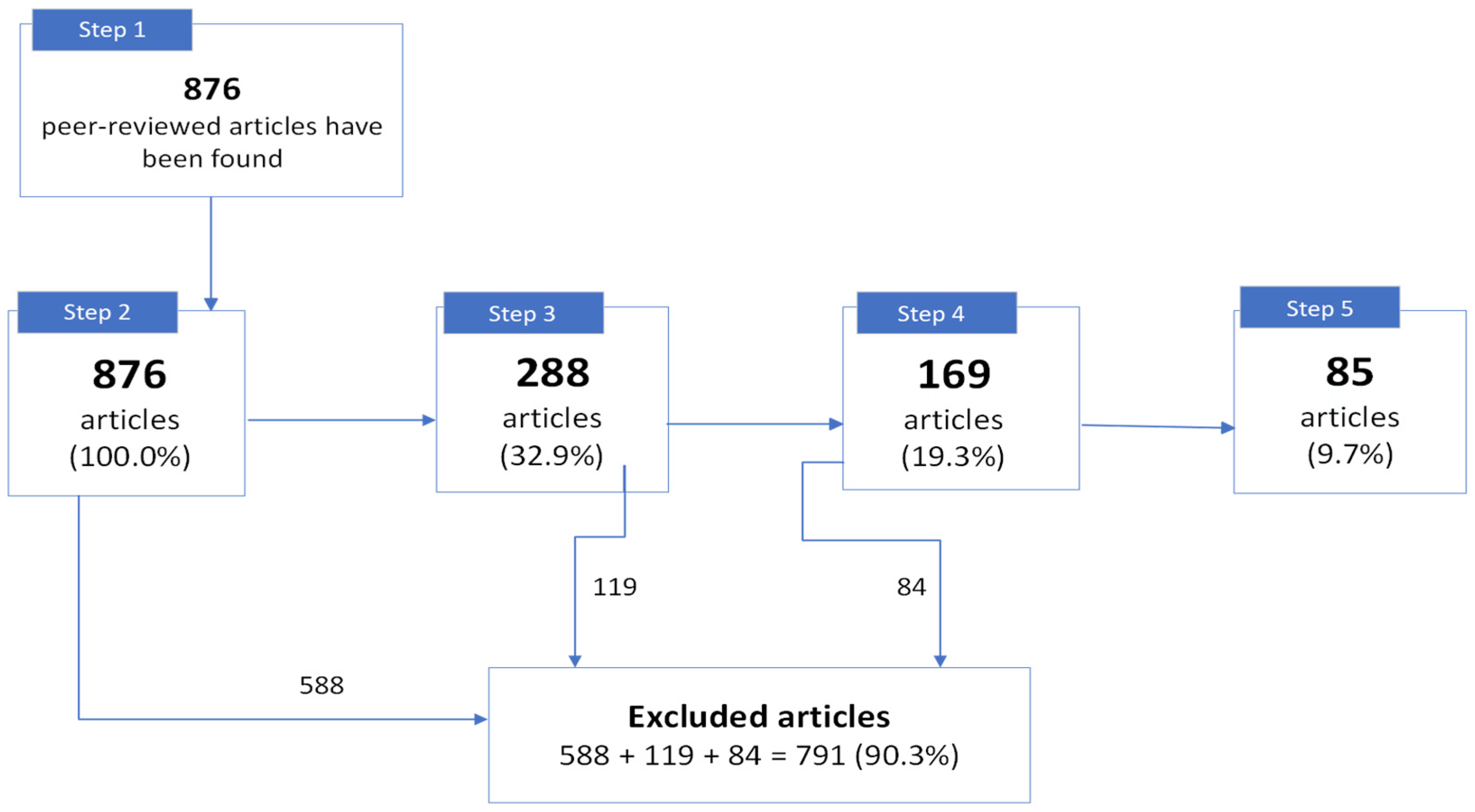
2.1. Bibliographic Search
2.2. Selection of Articles by Criteria
- (A) Adequate—discuss the occurrence and spread of CD, related or not to the presence and infection by T. cruzi in triatomines and/or animals;
- (PA) Possibly Adequate—might present variables which influence in the occurrence and spread of CD, related or not to the presence and infection by T. cruzi in triatomines and/or animals;
- (I) Inadequate—discuss the treatment and/or the physiobiological and clinical consequences of CD; they study the ecology of triatomines or their behavior in labs; they dissert about other diseases;
- (D) Duplicate articles.
- Inclusion criteria: (1) CD seroprevalence in humans, (2) infection by T. cruzi in triatomines, (3) infection by T. cruzi in animals;
- Exclusion criteria: (4) regarded other diseases; neglected tropical diseases in general; diagnostics and clinical treatments of CD; laboratorial studies; genotyping and/or ecology of triatomines without contribution for the analysis of risk variables for CD; diagnoses methodologies for CD; academic biographies; perception and intervention works; cases of individuals inhabiting only in urban area; (5) duplicated articles; and (6) without access to the article or abstract.
2.3. Data Analysis
3. Results and Discussion
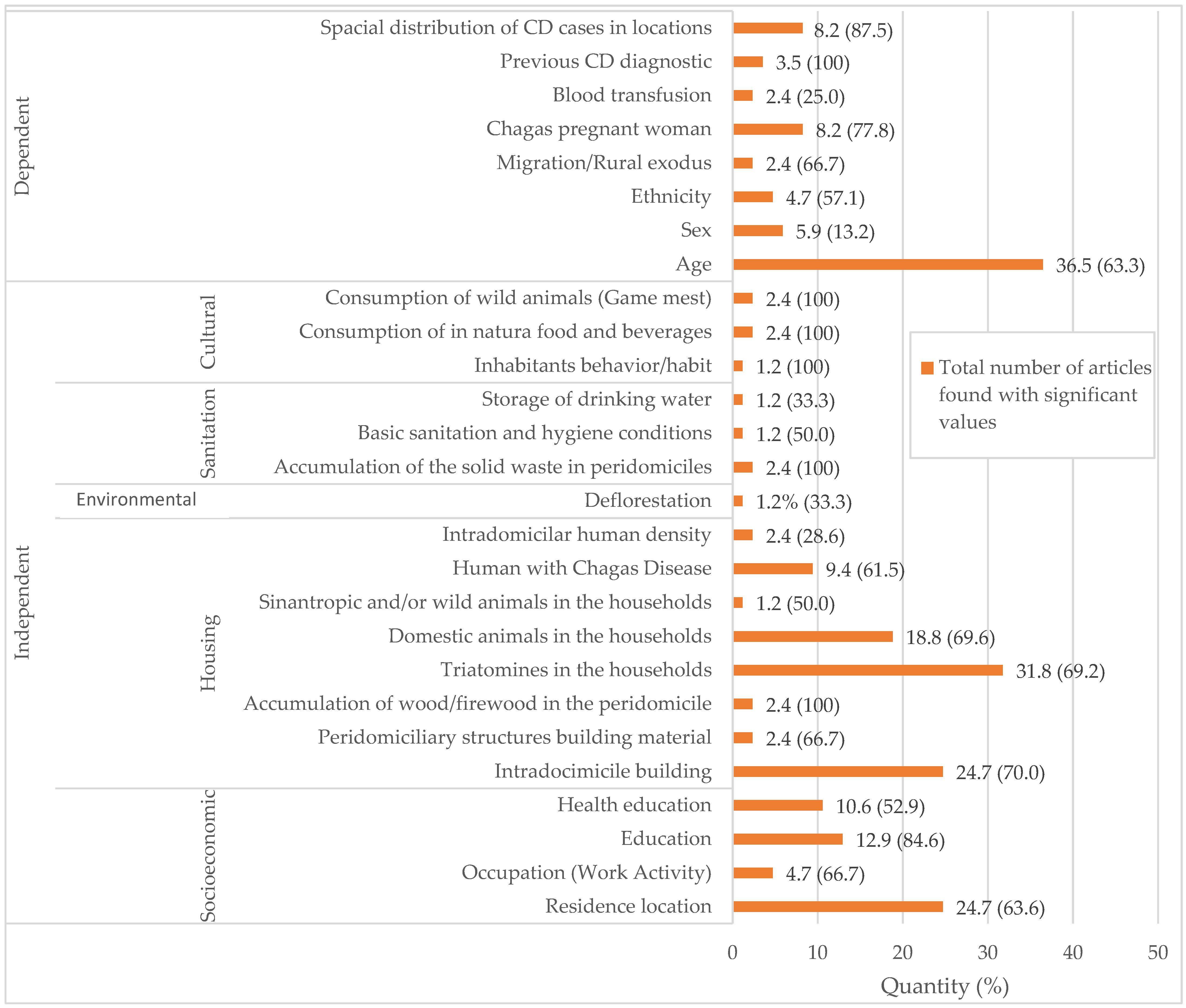
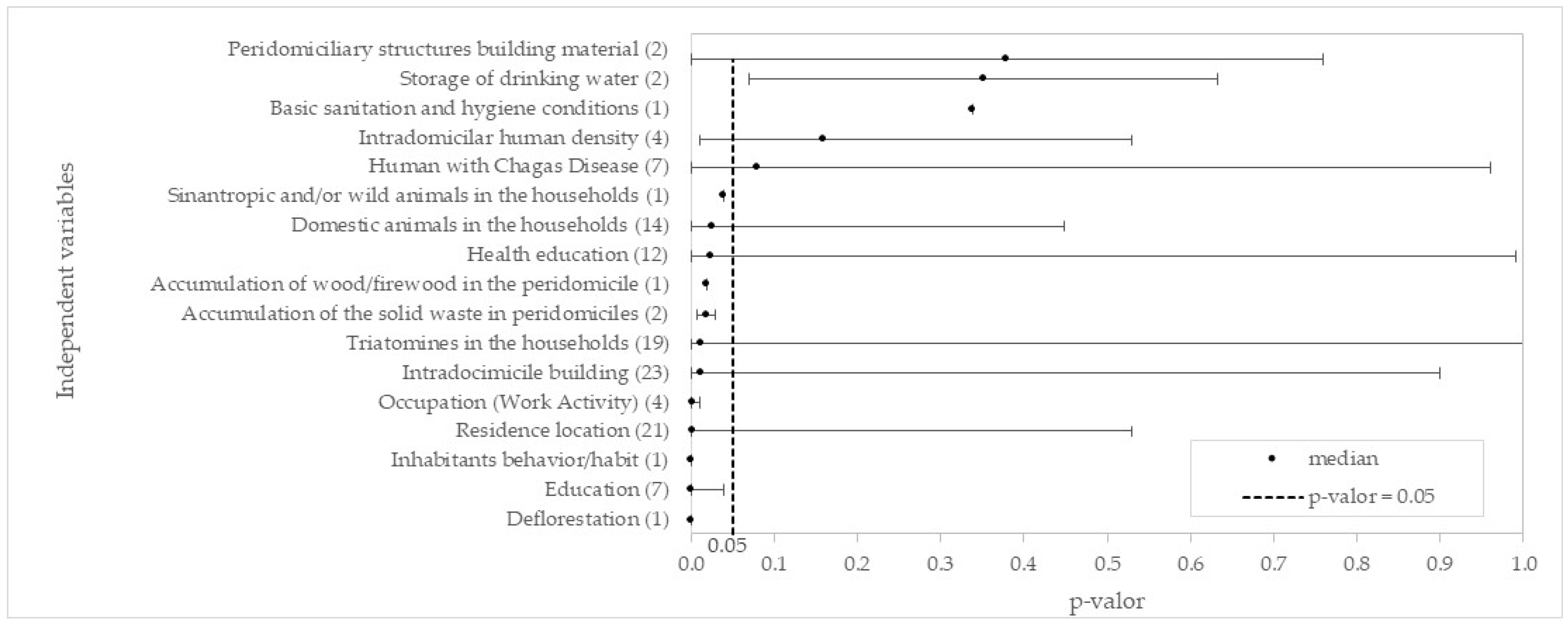
3.1. Independent Predictor Variables
3.1.1. Socioeconomic Variable
- ➢
- RESIDENCE LOCATION
- ➢
- OCCUPATION (WORK ACTIVITY)
- ➢
- EDUCATION
- ➢
- HEALTH EDUCATION
3.1.2. Housing Variable
- ➢
- INTRADOMICILE BUILDING
- ➢
- PERIDOMICILIARY STRUCTURE BUILDING MATERIAL
- ➢
- ACCUMULATION OF WOOD/FIREWOOD IN THE PERIDOMICILE
- ➢
- TRIATOMINES IN THE HOUSEHOLDS
- ➢
- DOMESTIC ANIMALS IN THE HOUSEHOLDS
- ➢
- SINANTROPIC AND/OR WILD ANIMALS IN THE HOUSEHOLDS
- ➢
- HUMANS WITH CHAGAS DISEASE
- ➢
- INTRADOMICILIAR HUMAN DENSITY
3.1.3. Environmental Variable
- ➢
- DEFORESTATION
3.1.4. Sanitation Variable
- ➢
- ACCUMULATION OF SOLID WASTE IN PERIDOMICILES
- ➢
- STORAGE OF DRINKING WATER
- ➢
- BASIC SANITATION AND HYGIENE CONDITIONS
3.1.5. Cultural Variable
- ➢
- INHABITANT BEHAVIOR/HABIT
- ➢
- CONSUMPTION OF IN NATURA FOOD AND BEVERAGES
- ➢
- CONSUMPTION OF WILD ANIMALS (GAME MEAT)
3.2. Dependent Predictor Variables
- ➢
- AGE
- ➢
- SEX
- ➢
- ETHNICITY
- ➢
- CHAGASIC PREGNANT WOMAN
- ➢
- BLOOD TRANSFUSION
- ➢
- PREVIOUS CD DIAGNOSIS
- ➢
- MIGRATION/RURAL EXODUS
- ➢
- SPATIAL DISTRIBUTION OF CD CASES IN LOCATIONS
4. Final Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kropf, S.P. Carlos Chagas and the debates and controversies surrounding the disease of Brazil (1909–1923). Hist. Ciênc. Saúde-Manguinhos 2009, 16, 205–227. [Google Scholar] [CrossRef]
- dos Santos, J.P.; Silva Junior, R.; Ricardo-Silva, A.H.; Verly, T.; Britto, C.; Evangelista, B.B.C.; Rocha-Silva, L.; da Silva, D.F.M.; Oliveira, R.A.; Pereira, E.; et al. Assessing the entomo-epidemiological situation of Chagas disease in rural communities in the state of Piauí, Brazilian semi-arid region. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Martinez, E. World Health Organization—WHO. Chagas Disease (Also Known as American Trypanosomiasis). 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/chagas-disease-(american-trypanosomiasis) (accessed on 17 February 2024).
- de Meis, J.; Castro, R.S.S. Manual para Diagnóstico em Doença de Chagas para Microscopistas de base no Estado do Pará, 1st ed.; Biblioteca de Ciências Biomédicas/ICICT/FIOCRUZ-RJ: Rio de Janeiro, Brazil, 2017; 110p, Available online: http://chagas.fiocruz.br/wp-content/uploads/2021/11/Manual-para-o-diagnostico-em-Doenca-de-Chagas.pdf (accessed on 17 February 2024).
- Departamento de Articulação Estratégica de Vigilância em Saúde, Secretaria de Vigilância em Saúde, Ministério da Saúde. Guia de Vigilância em Saúde, 5th ed.; Ministério da Saúde: Brasília, Brazil, 2022; 126p. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_saude_5ed_rev_atual.pdf (accessed on 17 February 2024).
- Jurberg, J.; Rodrigues, J.M.S.; Moreira, F.F.F.; Dale, C.; Cordeiro, I.R.S.; Lamas Junior, V.D.; Galvão, C.; Rocha, D.S. Atlas Iconográfico dos Triatomíneos do Brasil: Vetores da Doença de Chagas; Instituto Oswaldo Cruz: Rio de Janeiro, Brazil, 2014. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/publicacoes-svs/doenca-de-chagas/atlas-iconografico-dos-triatomineos-do-brasil-vetores-da-doenca-de-chagas.pdf/view (accessed on 17 February 2024).
- Ruiz-Guevara, R.; Muñoz-Calderón, A.; Alarcón de Noya, B.; Redondo, C.; Pulido, L.; Beitia, Y.; Mauriello, L.; Rojas, D.; Muñoz, J.; Navarro, E.; et al. Brote familiar de enfermedad de Chagas por transmisión oral en Yaguapita, estado Miranda, Venezuela. Bol. Malariol. Salud Amb. 2017, 57, 45–57. Available online: http://iaes.edu.ve/iaespro/ojs/index.php/bmsa/article/view/61 (accessed on 17 February 2024).
- Superintendência do Controle de Endemias—SUCEN. Guia de Triatomíneos do Estado de São Paulo. Departamento de Combate a Vetores. São Paulo. 2020. Available online: http://www.saude.sp.gov.br/resources/sucen/homepage/downloads/arquivos-de-chagas/guia_dos_triatomineos_do_estado_de_sao_paulo_final.pdf (accessed on 17 February 2024).
- Ramos-Ligonio, A.; López-Monteon, A.; Guzmán-Gómez, D.; Rosales-Encina, J.L.; Limón-Flores, Y.; Dumonteil, E. Identification of a hyperendemic area for Trypanosoma cruzi infection in central Veracruz, Mexico. Am. J. Trop. Med. Hyg. 2010, 83, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Beatty, N.L.; Klotz, S.A. Autochthonous Chagas Disease in the United States: How are People Getting Infected? Am. J. Trop. Med. Hyg. 2020, 103, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Navarro, M.; Reguero, L.; Subirà, C.; Blázquez-Pérez, A.; Requena-Méndez, A. Estimating chagas disease prevalence and number of underdiagnosed, and undertreated individuals in Spain. Travel Med. Infect. Dis. 2022, 47, 102248. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, I.M.I.; Miura, S.; Maeda, T.; Imai, K.; Smith, C.; Velasquez, C.V.; Honda, S.; Hirayama, K. Analysis of the Chagas disease situation in Japan: A cross sectional study and cost-effectiveness analysis of a Chagas disease screening program. Lancet Reg. Health West. Pac. 2023, 31, 100574. [Google Scholar] [CrossRef] [PubMed]
- Madeira, F.P.; de Jesus, A.C.; da Silva Moraes, M.H.; Barroso, N.F.; de Souza Castro, G.V.; Ribeiro, M.A.L.; Mendes, J.E.T.; Camargo, L.M.A.; de Oliveira Meneguetti, D.U.; Bernarde, P.S. Chagas Disease in the Western Brazilian Amazon: Epidemiological Overview from 2007 to 2018. J. Hum. Growth Dev. 2021, 31, 84–92. [Google Scholar] [CrossRef]
- Dale, C.; Paschoaletto, L.; Costa, J. O Complexo Triatoma Brasilienses: Atualizações sobre o Principal Vetor da Doença de Chagas No Nordeste Brasileiro, 1st ed.; Fundação Oswaldo Cruz: Rio de Janeiro, Brazil, 2019; 33p, Available online: https://www.fiocruz.br/ioc/media/Cartilha_Triatoma_brasiliensis_2019.pdf (accessed on 17 February 2024).
- Granados, P.S.; Pacheco, G.J.; Evangelina, N.P.; Betancourt, J.; Fulton, L. Assessing the effectiveness of Chagas disease education for healthcare providers in the United States. BMC Infect. Dis. 2020, 20, 6. [Google Scholar] [CrossRef]
- Imai, K.; Maeda, T.; Sayama, Y.; Mikita, K.; Fujikura, Y.; Misawa, K.; Nagumo, M.; Iwata, O.; Ono, T.; Kurane, I.; et al. Mother-to-Child Transmission of Congenital Chagas Disease, Japan. Emerg. Infect. Dis. 2014, 20, 146–148. [Google Scholar] [CrossRef]
- Lannes-Vieira, J. Portal da Doença de Chagas. Disease. Laboratory of Interactions Biology. Instituto Oswaldo Cruz/Fiocruz. 2017. Available online: https://chagas.fiocruz.br/sessao/doenca/ (accessed on 17 February 2024).
- Perissato, I.L.; Santos, K.A.R.; Oliveira, A.M.M.; Limongi, J.E. Doença de Chagas e a seguridade social: Caracterização da doença no sistema previdenciário e assistencial brasileiro, 2004–2016. Epidemiol. Serv. Saúde 2022, 31, e2021777. [Google Scholar] [CrossRef]
- Rios, L.; Campos, E.E.; Menon, R.; Zago, M.P.; Garg, N.J. Epidemiology and pathogenesis of maternal-fetal transmission of Trypanosoma cruzi and a case for vaccine development against congenital Chagas disease. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2020, 1866, 165591. [Google Scholar] [CrossRef]
- Cantey, P.T.; Stramer, S.L.; Townsend, R.L.; Kamel, H.; Ofafa, K.; Todd, C.W.; Currier, M.; Hand, S.; Varnado, W.; Dotson, E.; et al. The United States Trypanosoma cruzi Infection Study: Evidence for vector-borne transmission of the parasite that causes Chagas disease among United States blood donos. Transfusion 2012, 52, 1922–1930. [Google Scholar] [CrossRef]
- Lynn, M.K.; Bossak, B.H.; Sandifer, P.A.; Watson, A.; Nolan, M.S. Contemporary autochthonous human Chagas disease in the USA. Acta Trop. 2020, 205, 105361. [Google Scholar] [CrossRef] [PubMed]
- Moo-Millan, J.I.; Arnal, A.; Pérez-Carrillo, S.; Hernandez-Andrade, A.; Ramírez-Sierra, M.J.; Rosado-Vallado, M.; Dumonteil, E.; Waleckx, E. Disentangling Trypanosoma cruzi transmission cycle dynamics through the identification of blood meal sources of natural populations of Triatoma dimidiata in Yucatán, Mexico. Parasites Vectors 2019, 12, 572. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-Gómez, D.; Salas-González, G.; López-Monteon, A.; Welsh-Rodríguez, C.M.; Torres-Montero, J.; Dumonteil, E.; Waleckx, E.; Ramos-Ligonio, A. Risk factors for infestation by Triatoma dimidiata in a rural locality of Veracruz, Mexico, with active transmission of Trypanosoma cruzi: Weather and rain as factors. Trop. Med. Int. Health 2021, 26, 916–926. [Google Scholar] [CrossRef]
- Zamora-Ledesma, S.; Hernández-Camacho, N.; Sánchez-Moreno, M.; Ruiz-Piña, H.; Villagrán-Herrera, M.E.; Marín-Sánchez, C.; Carrillo-Angeles, I.G.; Jones, R.W.; Camacho-Macías, B. Seropositivity for Trypanosoma cruzi and Leishmania mexicana in dogs from a metropolitan region of Central Mexico. Vet. Parasitol. Reg. Stud. Rep. 2020, 22, 100459. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.K.; Yoshioka, K.; Hashimoto, K.; Caranci, A.; Gottdenker, N.; Monroy, C.; Saldaña, A.; Rodrigues, S.; Dorn, P.; Zúniga, C. Chagas Disease Epidemiology in Central America: An Update. Curr. Trop. Med. Rep. 2019, 6, 92–105. [Google Scholar] [CrossRef]
- Dorn, P.L.; Monroy, M.C.; Stevens, L. Sustainable, integrated control of native vectors: The case of Chagas disease in Central America. Front. Trop. Dis. 2022, 3, 971000. [Google Scholar] [CrossRef]
- Escobio, P.F.; Ribas, J.; Morillo, M.G.; Rodríguez-Ramírez, G.; Vicens-Ferrer, J.; Esteva, M. Prevalence of Chagas disease in the Bolivian population of Majorca (Spain). Gac. Sanit. 2015, 29, 288–291. [Google Scholar] [CrossRef]
- Hopkins, T.; Gonçalves, R.; Mamani, J.; Courtenay, O.; Bern, C. Chagas disease in the Bolivian Chaco: Persistent transmission indicated by childhood seroscreening study. Int. J. Infect. Dis. 2019, 86, 175–177. [Google Scholar] [CrossRef] [PubMed]
- de Santana Aquino, M.S.; Ferreira, A.L.D.S.; dos Santos, L.V.B.; Campos, J.H.F.; de Sena, L.L.J.; Mendonça, V.J. Seroprevalence of Chagas disease in rural communities at Campinas do Piauí city, Brazil. Trop. Med. Int. Health 2021, 26, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, M.R.; Rouset, F.; Carrasco, O.F.; Murillo, D.E.; Costales, J.A.; Brenière, S.F. Congenital chagas disease in the ecuadorian Amazon: Maternal screening at delivery and evaluation of risk factors associated with vector exposure. Am. J. Trop. Med. Hyg. 2019, 101, 1350–1358. [Google Scholar] [CrossRef] [PubMed]
- Díaz, A.L.M.; Sigua, F.P.; Otálora, A.S.; Pedraza Bernal, A.M. Seroprevalence of Chagas disease in rural communities at Campinas do Piauí city, Brazil. J. Parasit. Dis. 2021, 45, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Alarcón de Noya, B.A.; de Colmenares, C.; Díaz-Bello, Z.; Ruiz-Guevara, R.; Medina, K.; Muñoz-Calderón, A.; Mauriello, L.; Cabrera, E.; Montiel, L.; Losada, S.; et al. Orally-transmitted Chagas disease: Epidemiological, clinical, serological and molecular outcomes of a school microepidemic in Chichiriviche de la Costa, Venezuela. Parasite Epidemiol. Control 2016, 1, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Antik, A.; Hidalgo, G.; Anders, M.; Piñero, F.; Krogh, D.H.; Tagliafichi, V.; Silva, M.; Mendizabal, M.; Antinucci, F.; Brutti, J.; et al. 348.3: Prevalence of Chagas Disease in Deceased Donors From Argentina. Transplantation 2022, 106, S362. [Google Scholar] [CrossRef]
- Ventura-García, L.; Roura, M.; Pell, C.; Posada, E.; Gascón, J.; Aldasoro, E.; Pool, R. Socio-cultural aspects of Chagas disease: A systematic review of qualitative research. PLoS Negl. Trop. Dis. 2013, 7, e2410. [Google Scholar] [CrossRef]
- PAHO. Pan-American Health Organization. Less than 10% of People with Chagas Receive a Diagnosis; PAHO: Brasília, Brasil, 2023; Available online: https://www.paho.org/en/news/13-4-2023-less-10-people-chagas-receive-diagnosis (accessed on 17 February 2024).
- Departamento de Imunização e Doenças Transmissíveis, Secretaria de Vigilância em Saúde, Ministério da Saúde. Boletim Epidemiológico: Doença de Chagas; Ministério da Saúde: Brasília, Brazil, 2021; 36p. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2021/boletim_especial_chagas_14abr21_b.pdf (accessed on 17 February 2024).
- do Nascimento, L.P.G.R.; Nogueira, L.M.V.; Rodrigues, I.L.A.; André, S.R.; da Graça, V.V.; Monteiro, N.J. Prevalence of chagas disease associated with the mode of infection. Cogitare Enferm. 2021, 26, e7395. [Google Scholar] [CrossRef]
- Magalhães, L.; Silveira, H.; Prestes, S.; Magalhães, L.K.C.; Santana, R.A.; Ramasawmy, R.; Oliveira, J.; Roque, C.C.R.; Silva Junior, R.C.A.; Fé, N.; et al. Bioecological aspects of triatomines and marsupials as wild Trypanosoma cruzi reservoirs in urban, peri-urban and rural areas in the Western Brazilian Amazon. Med. Vet. Entomol. 2021, 35, 389–399. [Google Scholar] [CrossRef]
- de Souza Assis, S.N.; Lima, R.A.; Campos, M.C.C. Impact of deforestation on the incidence of chagas disease in the Brazilian Amazon. R. Gest. Sust. Ambient. 2022, 11, 279–297. [Google Scholar] [CrossRef]
- Cardinal, M.V.; Sartor, P.A.; Gaspe, M.S.; Enriquez, G.F.; Colaianni, I.; Gürtler, R.E. High levels of human infection with Trypanosoma cruzi associated with the domestic density of infected vectors and hosts in a rural area of northeastern Argentina. Parasites Vectors 2018, 11, 492. [Google Scholar] [CrossRef]
- Cantillo-Barraza, O.; Bedoya, S.C.; Xavier, S.C.C.; Zuluaga, S.; Salazar, B.; Vélez-Mira, A.; Carrillo, L.M.; Triana-Chávez, O. Trypanosoma cruzi infection in domestic and synanthropic mammals such as potential risk of sylvatic transmission in a rural area from north of Antioquia, Colombia. Parasite Epidemiol. Control 2020, 11, e00171. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.; Leone, J.L.; Vigliano, C.A. Chagas disease: Historic perspective. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165689. [Google Scholar] [CrossRef]
- Fundação Nacional de Saúde, Ministério da Saúde. Programa de Saneamento Rural, 1st ed.; Ministério da Saúde: Brasília, Brazil, 2019; 266p. Available online: http://www.funasa.gov.br/documents/20182/38564/MNL_PNSR_2019.pdf/08d94216-fb09-468e-ac98-afb4ed0483eb (accessed on 17 February 2024).
- Leite, L.S.; Scalize, P.S.; Hora, K.E.R. Habitação e Habitabilidade Rurais. Revista Ibero-Am. de Ciências Ambient. 2022, 13, 195–207. [Google Scholar] [CrossRef]
- Sandoval, E.M.; Marco, A.S.; Guzmán-Bracho, C.; Huante, R. Factores asociados con enfermedad de Chagas en zonas rurales de Guerrero, México. In Uma Mirada al Desarorollo Rural desde Realidades Locales, 1st ed.; Romero, D.M.Q., Velasco, R.L., Espinosa, R.R., Eds.; Universidad Autónoma Chapingo: Guerrero, México, 2022; pp. 230–251. Available online: http://ri.uagro.mx/bitstream/handle/uagro/3407/LIBC_10881_2022.pdf?sequence=1&isAllowed=y#page=231 (accessed on 17 February 2024).
- Dye-Braumuller, K.C.; Gorchakov, R.; Gunter, S.M.; Nielsen, D.H.; Roachell, W.D.; Wheless, A.; Debboun, M.; Murray, K.O.; Nolan, M.S. Identification of Triatomines and Their Habitats in a Highly Developed Urban Environment. Vector-Borne Zoonotic Dis. 2019, 19, 265–273. [Google Scholar] [CrossRef]
- Gaspe, M.S.; Fernández, M.D.P.; Cardinal, M.V.; Enriquez, G.F.; Rodríguez-Planes, L.I.; Macchiaverna, N.P.; Gürtler, R.E. Urbanisation, risk stratification and house infestation with a major vector of Chagas disease in an endemic municipality of the Argentine, Chaco. Parasites Vectors 2020, 13, 316–329. [Google Scholar] [CrossRef] [PubMed]
- Batista, P.H.; Lima, S.d.C. Aspectos socioambientais e vetores da doença de Chagas em assentamentos de reforma agrária no município de Uberlândia (MG), Brasil. Hygeia 2009, 5, 57–91. [Google Scholar] [CrossRef]
- Zamora, D.M.B.; Hernández, M.M.; Torres, N.; Zúniga, C.; Sosa, W.; Abrego, V.; Escobar, M.C.M. Information to act: Household characteristics are predictors of domestic infestation with the Chagas vector Triatoma dimidiata in central America. Am. J. Trop. Med. Hyg. 2015, 93, 97–107. [Google Scholar] [CrossRef]
- Donthu, N.; Kumar, S.; Mukherjee, D.; Pandey, N.; Lim, W.M. How to conduct a bibliometric analysis: An overview and guidelines. J. Bus. Res. 2021, 133, 285–296. [Google Scholar] [CrossRef]
- Fernández, M.D.P.; Gaspe, M.S.; Gürtler, R.E. Inequalities in the social determinants of health and Chagas disease transmission risk in indigenous and creole households in the Argentine Chaco. Parasites Vectors 2019, 12, 184–201. [Google Scholar] [CrossRef]
- Hernández-Romano, P.; Cámara-Contreras, M.; Bravo-Sarmiento, E.; Lõpez-Balderas, N. Prevalence of Trypanosoma cruzi antibodies in blood donors from Veracruz State, Mexico. Transfusion 2015, 55, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Santana, M.D.A.; Leal, A.R.D.S.; de Sousa, R.L.T.; dos Santos, L.V.B.; Mascarenhas, M.D.M.; Rodrigues, M.T.P.; Mendonça, V.J. Epidemiological aspects of Chagas disease in the state of Piauí (Northeast Brazil) in the period 2010–2019. Acta Trop. 2022, 228, 106338. [Google Scholar] [CrossRef] [PubMed]
- Fidalgo, A.S.O.B.V.; da Costa, A.C.; Ramos Júnior, A.N.; Leal, L.K.A.M.; Martins, A.M.C.; Silva Filho, J.D.D.; Ferreira, A.F.; Nunes, F.M.M.; Marinho Júnior, F.A.A.; Lacerda, J.M.; et al. Seroprevalence and risk factors of chagas disease in a rural population of the quixeré municipality, Ceará, Brazil. Rev. Soc. Bras. Med. Trop. 2021, 54, e0247-2020. [Google Scholar] [CrossRef] [PubMed]
- Colussi, C.; Stafuza, M.; Nepote, M.; Mendicino, D. Seroprevalence of Chagas disease in urban and rural indigenous populations of the south of Gran Chaco. Rev. Soc. Bras. Med. Trop. 2022, 55, e0479-2021. [Google Scholar] [CrossRef] [PubMed]
- Mordini, O.D.; Bavio, E.; Beloscar, J.; Tognoni, G.; Sosa, F.J.; Reyes, O.; Pairone, E.; Lacunza, D.; Manzur, R.; Redondo, M.; et al. Enfermedad de Chagas en Argentina. “Registro Nacional de enfermedad de Chagas de la Federación Argentina de Cardiología”. Estudio RENECH. Rev. Fed. Arg. Cardiol. 2016, 45, 84–92. Available online: https://www.researchgate.net/publication/306193531_Chagas_disease_in_Argentina_National_registry_of_chagas_disease_of_the_'Federacion_Argentina_de_Cardiologia'_RENECH_study (accessed on 17 February 2024).
- Sánchez-Guillén, M.C.; Barnabé, C.; Guégan, J.F.; Tibayrenc, M.; Velásquez-Rojas, M.; Martínez-Munguía, J.; Salgado-Rosas, H.; Torres-Rasgado, E.; Rosas-Ramírez, M.I.; Pérez-Fuentes, R. High prevalence anti-Trypanosoma cruzi antibodies, among blood donors in the State of Puebla, a non-endemic area of Mexico. Mem. Inst. Oswaldo Cruz 2002, 97, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Winter, A.C.; Menegotto, L.M.D.O.; Zucchetti, D.T. Vulnerabilidade social e educação: Uma reflexão na perspectiva da importância da intersetorialidade. Conhecimento Divers 2019, 11, 165–183. [Google Scholar] [CrossRef]
- Cucunubá, Z.M.; Flórez, A.C.; Cárdenas, Á.; Pavía, P.; Montilla, M.; Aldana, R.; Villamizar, K.; Ríos, L.C.; Nicholls, R.S.; Puerta, C.J. Prevalence and risk factors for chagas disease in pregnant women in Casanare, Colombia. Am. J. Trop. Med. Hyg. 2012, 87, 837–842. [Google Scholar] [CrossRef]
- Mastrolonardo, V.; Ramos, D.; Paravisini, I.; Morales, J.; Carrasco, H.; Huang, S.L.; Lemma, C. Trypanosomiasis in pregnancy [Tripanosomiasis en el embarazo]. Rev. Obstet. Ginecol. Venez. 2013, 73, 149–156. Available online: http://ve.scielo.org/scielo.php?script=sci_arttext&pid=S0048-77322013000300002&lng=es&nrm=iso&tlng=es (accessed on 17 March 2023).
- Montes-Rincón, L.M.; Galaviz-Silva, L.; González-Bravo, F.E.; Molina-Garza, Z.J. Trypanosoma cruzi seroprevalence in pregnant women and screening by PCR and microhaematocrit in newborns from Guanajuato, Mexico. Acta Trop. 2016, 164, 100–106. [Google Scholar] [CrossRef]
- Cardoso, L.P.; Paiva, T.R.; Nogueira, L.M.V.; Guimarães, R.J.P.S.E.; Rodrigues, I.L.A.; André, S.R. Spatial distribution of Chagas disease and its correlation with health services. Rev. Esc. Enferm. USP 2020, 54, e03565. [Google Scholar] [CrossRef] [PubMed]
- Sousa Júnior, A.S.; Palácios, V.R.C.M.; Miranda, C.S.; da Costa, R.J.F.; Catete, C.P.; Chagasteles, E.J.; Pereira, A.L.R.R.; Gonçalves, N.V. Space-temporal analysis of chagas disease and its environmental and demographic risk factors in the municipality of Barcarena, Pará, Brazil. Rev. Bras. Epidemiol. 2017, 20, 742–755. [Google Scholar] [CrossRef]
- García-Jordán, N.; Berrizbeitia, M.; Rodríguez, J.; Concepción, J.L.; Cáceres, A.; Quiñones, W. Seroprevalence of Trypanosoma cruzi infection in the rural population of Sucre state, Venezuela. Cad. Saúde Pública 2017, 33, e00050216. [Google Scholar] [CrossRef]
- Cruz, D.S.; de Souza, N.N.; Rafael, A.F.; Damasceno, R.F.; Ribeiro, A.L.P.; de Oliveira, L.C.; Sabino, E.C.; Ghilardi, F.R.; Neto, O.C.C.; Ferreira, A.M.; et al. Serological screening for Chagas disease in an endemic region of northern Minas Gerais, Brazil: The sami-trop project. Rev. Inst. Med. Trop. 2021, 63, e67. [Google Scholar] [CrossRef]
- Sampaio, G.H.F.; da Silva, A.N.B.; Brito, C.R.D.N.; Honorato, N.R.M.; Oliveira, L.M.; da Câmara, A.C.J.; Galvão, L.M.D.C. Epidemiological profile of acute chagas disease in individuals infected by oral transmission in Northern Brazil. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200088. [Google Scholar] [CrossRef]
- Sánchez-Lerma, L.; Pavas-Escobar, N.; Pérez-Gutiérrez, N.; González-Robayo, M.; Campo-Palacio, S. Seroprevalence of infection with Trypanosoma cruzi and associated factors in a population of Cumaral, Meta, Colombia. Rev. Habanera de Cienc. Med. 2021, 20, e3193. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1729-519X2021000100012 (accessed on 17 February 2022).
- de Oliveira, G.F.; Ribeiro, M.A.L.; Castro, G.V.S.; Menezes, A.L.R.; Lima, R.A.; Silva, R.P.M.; Meneguetti, D.U.O. Retrospective study of the epidemiological overview of the transmission of Chagas disease in the State of Acre, South-Western Amazonia, from 2009 to 2016. J. Hum. Growth Dev. 2018, 28, 329–336. [Google Scholar] [CrossRef]
- Delgado, S.; Neyra, R.C.; Machaca, V.R.Q.; Juárez, J.A.; Chu, L.C.; Verastegui, M.R.; Apaza, G.M.M.; Bocángel, C.D.; Tustin, A.W.; Sterling, C.R.; et al. A history of Chagas disease transmission, control, and re-emergence in peri-rural La Joya, Peru. PLoS Negl. Trop. Dis. 2011, 5, e970. [Google Scholar] [CrossRef]
- Sangenis, L.H.C.; Saraiva, R.M.; Georg, I.; de Castro, L.; dos Santos Lima, V.; Roque, A.L.R.; das Chagas Xavier, S.C.; Santos, L.C.; Fernandes, F.A.; Sarquis, O.; et al. Autochthonous transmission of Chagas disease in Rio de Janeiro State, Brazil: A clinical and eco-epidemiological study. BMC Infect. Dis. 2015, 15, 12. [Google Scholar] [CrossRef]
- Zabala, N.D.C.; Berrizbeitia, M.; Jorquera, A.; Rodríguez, J.; Romero, L. Trypanosoma cruzi infection in puerperal women and their neonates at Barcelona, Anzoategui State, Venezuela. Biomédica 2019, 39, 769–784. [Google Scholar] [CrossRef]
- Benítez-Villa, G.E.; López-Monteon, A.; Waleckx, E.; Dumonteil, E.; Márquez-Fernández, A.J.; Rovirosa-Hernández, M.J.; Orduña-García, F.; Guzmán-Gómez, D.; Ramos-Ligonio, A. Presence of Anti-T. cruzi Antibodies in Inhabitants and Dogs of Two Rural Settlements in the Sierra de Los Tuxtlas, Veracruz, Mexico. Acta Parasitol. 2022, 67, 1136–1144. [Google Scholar] [CrossRef]
- Abad-Franch, F.; Lima, M.M.; Sarquis, O.; Gurgel-Gonçalves, R.; Sánchez-Martín, M.; Calzada, J.; Saldaña, A.; Monteiro, F.A.; Palomeque, F.S.; Santos, W.S.; et al. On palms, bugs, and Chagas disease in the Americas. Acta Trop. 2015, 151, 126–141. [Google Scholar] [CrossRef] [PubMed]
- Coura, J.R.; Barrett, T.V.; Naranjo, M.A. Human populations attacked by wild Triatominae in the Amazonas: A new form of transmission of Chagas disease? Rev. Soc. Bras. Med. Trop. 1994, 27, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Borges-Pereira, J.; de Castro, J.A.F.; Silva, A.G.; Zauza, P.L.; Bulhões, T.P.; Gonçalves, M.E.; de Almeida, E.S.; Salmito, M.D.A.; Pereira, L.R.M.; Alves Filho, F.I.; et al. Seroprevalence of Chagas disease infection in the State of Piauí, 2002. Rev. Soc. Bras. Med. Trop. 2006, 39, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Aras, R.; Veiga, M.; Gomes, I.; Mota, G.; Rodrigues, B.; Rabelo, R.; Guzman-Bracho, C.; Melo, A. Prevalence of chagas’ disease in Mulungu do Morro northeastern Brazil. Arq. Bras. Cardiol. 2002, 78, 441–443. [Google Scholar] [CrossRef] [PubMed]
- Bar, M.E.; Oscherov, E.B.; Damborsky, M.P.; Borda, M. Transversal study on Chagas’ disease in an endemic area of Corrientes Province, Argentina. Bol. Malariol. Salud Amb. 2010, 50, 207–217. Available online: http://ve.scielo.org/scielo.php?script=sci_arttext&pid=S1690-46482010000200005&lng=en&nrm=iso (accessed on 17 February 2024).
- Brito, C.R.N.; Sampaio, G.H.F.; da Câmara, A.C.J.; Nunes, D.F.; de Azevedo, P.R.M.; Chiari, E.; Galvão, L.M.C. Seroepidemiology of Trypanosoma cruzi infection in the semiarid rural zone of the State of Rio Grande do Norte, Brazil. Rev. Soc. Bras. Med. Trop. 2012, 45, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Segura, E.L.; Escobar-Mesa, A.; Salazar-Schettino, P.M.; Rojas-Wastavino, G.E.; Cabrera-Bravo, M.; Bucio-Torres, M.I.; Guevara-Gómez, Y.; García-De La Torre, G.S. Epidemiología de la enfermedad de Chagas en el estado de Veracruz. Salud Publ. Méx. 2005, 47, 201–208. Available online: https://saludpublica.mx/index.php/spm/article/view/6610/8172 (accessed on 17 March 2023). [CrossRef]
- da Silva, R.A.; Goldenberg, P. Chagas’ disease in Porto Letícia, São Paulo: A comparative study in the Pontal the Paranapanema. Rev. Soc. Bras. Med. Trop. 2008, 41, 621–627. [Google Scholar] [CrossRef]
- Tobar, I.B.; Parra, F.; Pérez, C.N.; Rodríguez-Bonfante, C.; Useche, F.; Bonfante-Cabarcas, R. Prevalence of Trypanosoma cruzi antibodies and inflammatory markers in uncompensated heart failure. Rev. Soc. Bras. Med. Trop. 2011, 44, 691–696. [Google Scholar] [CrossRef]
- Bonfante-Cabarcas, R.; Rodríguez-Bonfante, C.; Vielma, B.O.; García, D.; Saldivia, A.M.; Aldana, E.; Curvelo, J.L.C. Seroprevalence for Trypanosoma cruzi infection and associated factors in an endemic area of Venezuela. Cad. Saúde Pública 2011, 27, 1917–1929. [Google Scholar] [CrossRef] [PubMed]
- Gamboa-León, R.; Ramirez-Gonzalez, C.; Pacheco-Tucuch, F.S.; O’shea, M.; Rosecrans, K.; Pippitt, J.; Dumonteil, E.; Buekens, P. Seroprevalence of Trypanosoma cruzi among mothers and children in rural Mayan communities and associated reproductive outcomes. Am. J. Trop. Med. Hyg. 2014, 91, 348–353. [Google Scholar] [CrossRef] [PubMed]
- de Godoy, I.; Meira, D.A. Seroprevalence of Chagas infection among inhabitants of municipalities in the Botucatu region, State of São Paulo. Rev. Soc. Bras. Med. Trop. 2007, 40, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Mott, K.E.; Muniz, T.M.; Lehman Junior, J.S.; Hoff, R.; Morrow Junior, R.H.; de Oliveira, T.S.; Sherlock, I.; Draper, C.C. House construction, triatomine distribution, and household distribution of seroreactivity to Trypanosoma cruzi in a rural community in northeast Brazil. Am. J. Trop. Med. Hyg. 1978, 27, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Gürtler, R.E.; Wisnivesky-Colli, C.; Solarz, N.D.; Lauricella, M.; Bujas, M.A. Dynamics of transmission of Trypanosoma cruzi in a rural area of Argentina: II. Household infection patterns among children and dogs relative to the density of infected Triatoma infestans. Bull. Pan Am. Health Organ. 1987, 21, 280–292. Available online: https://iris.paho.org/handle/10665.2/27750 (accessed on 18 March 2023). [PubMed]
- Paulone, I.; Chuit, R.; Perez, A.C.; Canale, D.; Segura, E.L. The status of transmission of Trypanosoma cruzi in an endemic area of Argentina prior to control attempts, 1985. Ann. Trop. Med. Parasitol. 1991, 85, 489–497. [Google Scholar] [CrossRef]
- Rivera, T.; Palma-Guzman, R.; Morales, W. Seroepidemiological and clinical study of Chagas’ disease in Nicaragua. Rev. Inst. Med. Trop. 1995, 37, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Zulantay, I.; Bozán, F.; Salas, C.; Zilleruelo, N.; Osuna, A.; Gil, L.C.; Rodríguez, J.; Rojas, A.; Egea, J.L.; Apt, W. Chronic Chagas disease. Absence of intradomiciliary Triatoma infestans and persistence of circulating post-therapy Trypanosoma cruzi. Parasitol. Latinoam. 2004, 59, 93–98. [Google Scholar] [CrossRef]
- Hoyos, R.; Pacheco, L.; Agudelo, L.A.; Zafra, G.; Blanco, P.; Triana, O. Seroprevalence of chagas disease and associated risk factors in a population of Morroa, Sucre. Biomédica 2007, 27, 130–136. [Google Scholar] [CrossRef]
- Black, C.L.; Ocaña-Mayorga, S.; Riner, D.K.; Costales, J.A.; Lascano, M.S.; Arcos-Terán, L.; Preisser, J.S.; Seed, J.R.; Grijalva, M.J. Seroprevalence of Trypanosoma cruzi in rural Ecuador and clustering of seropositivity within households. Am. J. Trop. Med. Hyg. 2009, 81, 1035–1040. [Google Scholar] [CrossRef]
- Cruz, O.A.; De La Pena, J.E.; Castrejón, O.V.; Bracho, C.G. Chagas disease seroprevalence in Tamazunchale, San Luis Potosí. Enf. Inf. Microbiol. 2009, 29, 107–110. Available online: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=26750 (accessed on 18 March 2023).
- Ostermayer, A.L.; Passos, A.D.C.; Silveira, A.C.; Ferreira, A.W.; Macedo, V.; Prata, A.R. The national Survey of seroprevalence for evaluation of the control of Chagas disease in Brazil (2001–2008). Rev. Soc. Bras. Med. Trop. 2011, 44, 108–121. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.M.; Carvalho-Costa, F.A.; Toma, H.K.; Borges-Pereira, J.; de Oliveira, T.G.; Sarquis, O. Chagas disease and housing improvement in northeastern Brazil: A cross-sectional survey. Parasitol. Res. 2015, 114, 1687–1692. [Google Scholar] [CrossRef]
- Paz, O.M.; Díaz-Suárez, O.; Atencio, R.; Rivero-Rodríguez, Z.; Terán, M.R.R.; Bracho, A.; Soler, M.; Suárez, M. Seroprevalencia y factores de riesgo asociados a infección por Trypanosoma cruzi y Toxoplasma gondii en la comunidad Saimadoyi, Sierra de Perijá, estado Zulia. Kasmera 2017, 45, 33–43. Available online: https://produccioncientificaluz.org/index.php/kasmera/article/view/22834/22750 (accessed on 18 March 2023).
- Zumaquero-Ríos, L.; Sarracent-Pérez, J.; Sandoval-Ruiz, C.; Aldana-Arnas, R.M.; López-Monteon, A.; Torres-Montero, J.; Guzmán-Gómez, D.; Ramos-Ligonio, A. Presence of Seropositive Patients to Trypanosoma cruzi in a Municipality of the Mixtec Sierra of the State of Puebla: A Preliminary Study. Acta Parasitol. 2020, 65, 19–26. [Google Scholar] [CrossRef]
- Gutierrez, F.R.S.; Trujillo Güiza, M.L.; Escobar Martínez, M.D.C. Prevalence of Trypanosoma cruzi Infection among People Aged 15 to 89 Years Inhabiting the Department of Casanare (Colombia). PLoS Negl. Trop. Dis. 2013, 7, e2113. [Google Scholar] [CrossRef] [PubMed]
- Serrano, O.; Mendoza, F.; Suárez, B.; Soto, A. Seroepidemiology of Chagas disease in two rural populations in the municipality of Costa de Oro, at Aragua State, northern Venezuela. Biomédica 2008, 28, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Sarquis, O.; Sposina, R.; de Oliveira, T.G.; Cord, J.R.M.; Cabello, P.H.; Borges-Pereira, J.; Lima, M.M. Aspects of peridomiciliary ecotopes in rural areas of Northeastern Brazil associated to triatomine (Hemiptera, Reduviidae) infestation, vectors of Chagas disease. Mem. Inst. Oswaldo Cruz 2006, 101, 143–147. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, A.L.S.S.; Zicker, F.; Silva, I.G.; Souza, J.M.P.; Martelli, C.M.T. Risk factors for Trypanosoma cruzi infection among children in central Brazil: A case-control study in vector control settings. Am. J. Trop. Med. Hyg. 1995, 52, 183–187. [Google Scholar] [CrossRef]
- Bar, M.E.; Oscherov, E.B.; Damborsky, M.P.; Alvarez, B.M.; Mizdraji, G.; Avalos, G.; Porcel, E. Domestic infestation by Triatoma infestans and prevalence of Trypanosoma cruzi seropositives in a rural area of the Argentinian northeast. Rev. Soc. Bras. Med. Trop. 1996, 29, 549–555. [Google Scholar] [CrossRef]
- Oscherov, E.B.; Bar, M.E.; Damborsky, M.P.; Milano, A.M.F.; Avalos, G.; Borda, M.A. Chagas’ disease epidemiology in the province of General Paz, Argentina. Rev. Saúde Pública 2003, 37, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Fernández, M.D.P.; Gaspe, M.S.; Sartor, P.; Gürtler, R.E. Human Trypanosoma cruzi infection is driven by eco-social interactions in rural communities of the Argentine Chaco. J. Infect. Public Health 2019, 11, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Cardinal, M.V.; Enriquez, G.F.; Macchiaverna, N.P.; Argibay, H.D.; Fernández, M.P.; Alvedro, A.; Gaspe, M.S.; Gürtler, R.E. Long-term impact of a ten-year intervention program on human and canine Trypanosoma cruzi infection in the argentine chaco. PLoS Negl. Trop. Dis. 2021, 15, e0009389. [Google Scholar] [CrossRef] [PubMed]
- Gürtler, R.E.; Cecere, M.C.; Lauricella, M.A.; Petersen, R.M.; Chuit, R.; Segura, E.L.; Cohen, J.E. Incidence of Trypanosoma cruzi infection among children following domestic reinfestation after insecticide spraying in rural northwestern Argentina. Am. J. Trop. Med. Hyg. 2005, 73, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Gürtler, R.E.; Chuit, R.; Cécere, M.C.; Castañera, M.B.; Cohen, J.E.; Segura, E.L. Household prevalence of seropositivity for Trypanosoma cruzi in three rural villages in northwest Argentina: Environmental, demographic, and entomologic associations. Am. J. Trop. Med. Hyg. 1998, 59, 741–749. [Google Scholar] [CrossRef]
- Saldaña, A.; Pineda, V.; Martinez, I.; Santamaria, G.; Santamaria, A.M.; Miranda, A.; Calzada, J.E. A new endemic focus of Chagas disease in the northern region of Veraguas Province, Western Half Panama, Central America. PLoS ONE 2012, 7, e34657. [Google Scholar] [CrossRef] [PubMed]
- Sousa, O.E.; Johnson, C.M. Prevalence of Trypanosoma cruzi and Trypanosoma rangeli in triatomines (hemiptera:reduviidae) collected in the Republic of Panama. Am. J. Trop. Med. Hyg. 1973, 22, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Monteon, V.; Alducin, C.; Hernández, J.; Ramos-Ligonio, A.; Lopez, R. High frequency of human blood in Triatoma dimidiata Captured inside dwellings in a rural community in the Yucatan Peninsula, Mexico, but low antibody seroprevalence and electrocardiographic findings compatible with Chagas disease in humans. Am. J. Trop. Med. Hyg. 2013, 88, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Baeck, I.M.; Mando, P.; Virasoro, B.M.; Martinez, A.; Zarate, S.; Valentini, R.; Saubidet, I.L. Prevalence of Chagas Disease and Associated Factors in an Endemic Area of Northeastern Argentina. Am. J. Trop. Med. Hyg. 2022, 107, 146–150. [Google Scholar] [CrossRef]
- Newton-Sanchez, O.A.; Melnikov, V.; Nava-Zavala, A.H.; Zavala-Cerna, M.G.; Guzman-Bracho, C.; Delgado-Enciso, I.; Rojas-Larios, F.; Martinez-Rizo, A.B.; Lopez-Lemus, U.A.; Espinoza-Gomez, F. Presence of Acute Chagas Disease among Febrile Patients in the Western Coast of Mexico. Vector-Borne Zoonotic Dis. 2020, 20, 657–663. [Google Scholar] [CrossRef]
- Añez, N.; Crisante, G.; Rojas, A.; Dávila, D. Brote de enfermedad de Chagas agudo de posible transmisión oral en Mérida, Venezuela. Bol. Malariol. Salud Amb. 2013, 53, 1–11. Available online: http://ve.scielo.org/scielo.php?script=sci_arttext&pid=S1690-46482013000100001&lng=es&nrm=iso (accessed on 18 March 2023).
- Ceretta, G.F.; Silva, F.K.; Rocha, A.C. Environmental Management and the problem of household waste in the rural area of São João-PR. Revista ADMpg Gestão Estratégica 2013, 6, 17–25. Available online: https://revistas.uepg.br/index.php/admpg/article/view/14012/209209211131 (accessed on 18 March 2023).
- Straceione, M.M.; Printes, R.B. Desafios na Gestão Intercultural de Resíduos Sólidos em Aldeias Mbya Guarani no Centro sul do Rio Grande do Sul. Graduation, Universidade Estadual do Rio Grande do Sul (UERGS), Rio Grande do Sul—Brazil. 2021. Available online: https://repositorio.uergs.edu.br/xmlui/handle/123456789/1965 (accessed on 18 March 2023).
- Ferreira-Silva, M.M.; Pereira, G.A.; Lages-Silva, E.; Moraes-Souza, H. Socioepidemiological screening of serologically ineligible blood donors due to Chagas disease for the definition of inconclusive cases. Mem. Inst. Oswaldo Cruz 2010, 105, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Lucas, R.M.O.; Barba, M.C.P. Prevalence of American Tripanosomiasis in Pregnant Women from a Health Area of Valencia, Spain. 2005-2007. Rev. Esp. Salud Publica 2009, 83, 543–555. Available online: http://hdl.handle.net/20.500.12466/1436 (accessed on 18 March 2023). [PubMed]
- Fundação João Pinheiro. Metodologia do Déficit Habitacional e da Inadequação de Domicílios no Brasil—2016–2019; Fundação João Pinheiro: Belo Horizonte, Brazil, 2021; 80p. Available online: https://fjp.mg.gov.br/metodologia-do-deficit-habitacional-e-inadequacao-de-domicilios-no-brasil-2016-2019 (accessed on 18 March 2023).
- Barros, F.N.L.; Vieira, J.S.C.; Sampaio Júnior, F.D.; Lima, J.S.; Nobre, A.V.; Barrozo, P.H.M.; Paiva, J.R.; Cavalcante, G.G.; Scofield, A. Trypanosoma cruzi infection in triatomines (Hemiptera:Reduviidae) from rural areas of the state of Pará, Brazil. Zoonoses Public Health 2021, 68, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.L.; Hoyos, L.; Cabido, M.; Catalá, S.S.; Gorla, D.E. Exploring the association between Trypanosoma cruzi infection in rural communities and environmental changes in the Southern Gran Chaco. Mem. Inst. Oswaldo Cruz 2012, 107, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Traviezo, L.E.; Bonfante-Garrido, R. Seroepidemiological study on Chagas disease in the locality of Caballito, Simon Planas Municipality, Lara State, Venezuela. Parasitol. Latinoam. 2004, 59, 46–50. [Google Scholar] [CrossRef]
- Añez, N.; Rojas, A.; Crisante, G.; Parra, J.; Vivas, D.; Parada, H. Enfermedad de Chagas en el estado Táchira: Reporte de un nuevo brote por transmisión oral de Trypanosoma cruzi en el occidente de Venezuela. Bol. Malariol. Salud Amb. 2018, 58, 46–56. Available online: http://iaes.edu.ve/iaespro/ojs/index.php/bmsa/article/view/58 (accessed on 18 March 2023).
- Silva, B.A.M.; dos Santos, F.S.; Costa, V.B.N.; Ferreira, R.R.; de Oliveira, S. Perfil de transmissão da Doença de Chagas no Brasil: 2008 a 2020. Rev. Presença 2021, 7, 22–42. Available online: https://revistapresenca.celsolisboa.edu.br/index.php/numerohum/article/view/354 (accessed on 18 March 2023).
- Sangenis, L.H.C.; Nielebock, M.A.P.; Santos, C.S.; Silva, M.C.C.; Bento, G.M.R. Chagas disease transmission by consumption of game meat: Systematic review. Rev. Bras. Epidemiol. 2016, 19, 803–811. [Google Scholar] [CrossRef]
- Wisnivesky-Colli, C.; Ruiz, A.M.; Gurtler, R.E.; Solarz, N.D.; Lazzari, J.; Ledesma, O.; Bujas, M.A.; de Rissio, A.M.; Marteleur, A.; Segura, E.L. Dynamics of transmission of Trypanosoma cruzi in a rural area of Argentina. IV. Serologic, parasitologic and electrocardiographic study of the human population. Medicina 1989, 49, 341–350. Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=PuyMFry8ww4C&oi=fnd&pg=PA341&dq=Dynamics+of+transmission+of+Trypanosoma+cruzi+in+a+rural+area+of+Argentina.+IV.+Serologic,+parasitologic+and+electrocardi-ographic+study+of+the+human+population&ots=gdmoinl3aT&sig=YLXra8nPfILbnuxrEGDInss2E0w#v=onepage&q=Dynamics%20of%20transmission%20of%20Trypanosoma%20cruzi%20in%20a%20rural%20area%20of%20Argentina.%20IV.%20Serologic%2C%20parasitologic%20and%20electrocardi-ographic%20study%20of%20the%20human%20population&f=false (accessed on 18 March 2023).
- Bar, M.E.; Oscherov, E.B.; Damborsky, M.P.; Varela, M.E.; Mizdraji, G.; Porcel, E. Triatomismo del Departamento San Luis del Palmar de la provincia de Corrientes, Argentina. Medicina 1992, 52, 193–201. Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=jIHzwkqXDhIC&oi=fnd&pg=PA193&dq=Triatomismo+del+Departamento+San+Luis+del+Palmar+de+la+provincia+de+Corrientes,+Argentina.&ots=d0dV7JXHfQ&sig=YtPhCcmyTzETb6BnT4Dk2gUm1_8#v=onepage&q=Triatomismo%20del%20Departamento%20San%20Luis%20del%20Palmar%20de%20la%20provincia%20de%20Corrientes%2C%20Argentina.&f=false (accessed on 18 March 2023). [PubMed]
- Passos, A.D.C.; Nogueira, J.L.; de Castro Figueiredo, J.F.; Gomes, U.A.; Dal-Fabbro, A.L. Evolution of seropositivity for Chagas’ disease in a rural community in Brazil. Rev. Panam. Salud Publica 1997, 2, 247–252. [Google Scholar] [CrossRef]
- Monteón, V.M.; Reyes-López, P.A.; Sosa-Palacio, A.; León-Tello, G.; Martínez-Murguía, J.; Sosa-Jurado, F. Heterogeneous distribution of the prevalence of anti-Trypanosoma cruzi antibodies among blood donors in the State of Puebla, Mexico. Salud Publica Mex. 2005, 47, 116–125. [Google Scholar] [CrossRef]
- Rodríguez-Bonfante, C.; Amaro, A.; García, M.; Wohlert, L.E.M.; Guillen, P.; García, R.A.; Álvarez, N.; Díaz, M.; Cárdenas, E.; Castillo, S.; et al. Epidemiología de la enfermedad de Chagas en el municipio Andrés Eloy Blanco, Lara, Venezuela: Infestación triatomínica y seroprevalencia en humanos. Cad. Saúde Pública 2007, 23, 1133–1140. [Google Scholar] [CrossRef]
- Borges-Pereira, J.; Sarquis, O.; Zauza, P.L.; Britto, C.; Lima, M.M. Epidemiology of Chagas disease in four rural localities in Jaguaruana, State of Ceará. Seroprevalence of infection, parasitemia and clinical characteristics. Rev. Soc. Bras. Med. Trop. 2008, 41, 345–351. [Google Scholar] [CrossRef]
- Moreno, M.L.; Moretti, E.; Basso, B.; Céspedes, M.F.; Catalá, S.S.; Gorla, D.E. Seroprevalence of Trypanosoma cruzi infection and vector control activities in rural communities of the southern Gran Chaco (Argentina). Acta Trop. 2010, 113, 257–262. [Google Scholar] [CrossRef]
- Chippaux, J.P.; Postigo, J.R.; Santalla, J.A.; Schneider, D.; Brutus, L. Epidemiological evaluation of Chagas disease in a rural area of southern Bolivia. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 578–584. [Google Scholar] [CrossRef]
- Alroy, K.A.; Huang, C.; Gilman, R.H.; Quispe-Machaca, V.R.; Marks, M.A.; Ancca-Juarez, J.; Hillyard, M.; Verastegui, M.; Sanchez, G.; Cabrera, L.; et al. Prevalence and Transmission of Trypanosoma cruzi in People of Rural Communities of the High Jungle of Northern Peru. PLoS Negl. Trop. Dis. 2015, 9, e0003779. [Google Scholar] [CrossRef]
- Baruffa, G.; Alcantara Filho, A. Serologic prevalence of Chagas disease in the southern area of the state of Rio Grande do Sul (Brasil). Rev. Inst. Med. Trop. 1977, 19, 117–123. Available online: https://www.revistas.usp.br/rimtsp/article/download/197845/182022 (accessed on 18 March 2023).
- Goldsmith, R.S.; Zárate, R.J.; Zárate, L.G.; Kagan, I.; Jacobson, L.B. Clinical and epidemiologic studies of Chagas’ disease in rural communities in Oaxaca State, Mexico, and a seven-year follow-up: I. Cerro del Aire. Bull. Pan Am. Health Organ. 1985, 19, 120–138. Available online: https://iris.paho.org/handle/10665.2/27295 (accessed on 18 March 2023).
- Becerril-Flores, M.A.; Valle-De La Cruz, A. Descripción de la Enfermedad de Chagas en el Valle de Iguala Guerrero, México. Gac. Med. Mex. 2003, 139, 539–544. Available online: https://www.medigraphic.com/pdfs/gaceta/gm-2003/gm036c.pdf (accessed on 18 March 2023). [PubMed]
- Vargas, C.C.; Narváez, A.O.; Aroca, J.M.; Shiguango, G.; Robles, L.M.; Herrera, C.; Dumonteil, E. Seroprevalence of Trypanosoma cruzi infection in schoolchildren and in pregnant women from an Amazonian Region in Orellana Province, Ecuador. Am. J. Trop. Med. Hyg. 2015, 93, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Correia, J.R.; Ribeiro, S.C.S.; de Araújo, L.V.F.; Santos, M.C.; Rocha, T.R.; Viana, E.A.S.; Cairesp, P.T.P.R.C.; Corrêa, S.M.C.; Pinheiro, T.G.; Carvalho, L.C. Chagas disease: Clinical, epidemiological and pathophysiological aspects. Electron. J. Collect. Health 2021, 13, e6502. [Google Scholar] [CrossRef]
- Goldsmith, R.S. Estudios clinicos y epidemiologicos sobre la enfermedad de Chagas en comunidades rurales de Oaxaca, Mexico un estudio de ocho anos de seguimiento: II. Chila. Bol. Of. Sanit. Panam. 1992, 113, 97–108. Available online: https://iris.paho.org/bitstream/handle/10665.2/16459/v113n2p97.pdf?sequence=1 (accessed on 18 March 2023).
- Ferreira, I.L.M.; Silva, T.P.T. Transmission elimination of Chagas’ disease by Triatoma infestans in Brazil: An historical fact. Rev. Soc. Bras. Med. Trop. 2006, 39, 507–509. [Google Scholar] [CrossRef]
- Paz-Bailey, G.; Monroy, C.; Rodas, A.; Rosales, R.; Tabaru, R.; Davies, C.; Lines, J. Incidence of Trypanosoma cruzi infection in two Guatemalan communities. Trans. R. Soc. Trop. Med. Hyg. 2002, 96, 48–52. [Google Scholar] [CrossRef]
- Lucero, R.H.; Brusés, B.L.; Cura, C.I.; Formichelli, L.B.; Juiz, N.; Fernández, G.J.; Bisio, M.; Deluca, G.D.; Besuschio, S.; Hernández, D.O.; et al. Chagas’ disease in Aboriginal and Creole communities from the Gran Chaco Region of Argentina: Seroprevalence and molecular parasitological characterization. Infect. Genet. Evol. 2016, 41, 84–92. [Google Scholar] [CrossRef]
- Salvatella, R.; Rosa, R.; Gonzalez, M.; Basmadjián, Y.; Combol, A.; Benavidez, U.; Mancebo, R.; Fernandez, N.; Calegari, L. Seroprevalencia de la infección por Trypanosoma cruzi en escolares de seis y doce años de edad de tres departamentos endémicos de Uruguay. Bol. Chil. Parasitol. 1999, 54, 51–56. [Google Scholar] [CrossRef]
- Melendez, F.; Bachler, G.; Colvin, A.; Mejías, G.; Gutiérrez, C.; Rojas, A.; García, A.L.; Contreras, M.C.; Schenone, H.; Lorca, M. Comparison of Trypanosoma cruzi infection in less than 10 years old children from the V Región, Chile, 1982–1995. Bol. Chil. Parasitol. 2000, 55, 27–30. [Google Scholar] [CrossRef]
- Russomando, G.; Cousiño, B.; Sanchez, Z.; Franco, L.X.; Nara, E.M.; Chena, L.; Martínez, M.; Galeano, M.E.; Benitez, L. Chagas disease: National survey of seroprevalence in children under five years of age conducted in 2008. Mem. Inst. Oswaldo Cruz 2017, 112, 348–353. [Google Scholar] [CrossRef]
- Ticona, C.A.M.; Benzaquen, E.C.; Juárez, J.A.; Díaz, J.S.; Choque, A.T.; Talavera, R.V.; Álvarez, J.L.R.; Díaz, J.S.; Chirinos, S.V.; Pérez, R.S. The prevalence of Chagas’ disease in puerperal women and congenital transmission in an endemic area of Peru. Rev. Panam. Salud Publica 2005, 17, 147–153. [Google Scholar] [CrossRef]
- Conners, E.E.; Ordõez, T.L.; Cordon-Rosales, C.; Casanueva, C.F.; Miranda, S.M.; Brouwer, K.C. Chagas disease infection among migrants at the Mexico/Guatemala border. Am. J. Trop. Med. Hyg. 2017, 97, 1134–1140. [Google Scholar] [CrossRef]
- Monteón-Padilla, V.M.; Hernández-Becerril, N.; Guzmán-Bracho, C.; Rosales-Encina, J.L.; Reyes-López, P.A. American trypanosomiasis (Chagas’ disease) and blood banking in Mexico City: Seroprevalence and Its potential transfusional transmission risk. Arch. Med. Res. 1999, 30, 393–398. [Google Scholar] [CrossRef]
- Guimarães, R.J.P.S.; Sousa Junior, A.S.; Pinheiro, A.F.; Dias, R.S.; Dias, F.A.; Neves, A.L.L.; Vale, I.S.S.; Palacios, M.C.; Veiga, N.G. Geoprocessamento aplicado à análise ecoepidemiológica da doença de Chagas nos municípios de Abaetetuba e Barcarena, no Estado do Pará, Brasil, entre 2000–2011. Rev. SELPER 2012, 34, 30–35. Available online: https://d1wqtxts1xzle7.cloudfront.net/53625601/selper_34-2_2012_Chagas.pdf?1498142447=&response-content-disposition=inline%3B+filename%3DGeoprocessamento_aplicado_a_analise_ecoe.pdf&Expires=1708282128&Signature=EbuN6xwMnxBfwNeCAxkQj2aa4OnUjv~qwY1L3aFkQhIXZweWjrVIfoe1GDtiUywzINwLl-BDoOvJUXyMqe1uCRsUuhO3mtOdxIMOS~iLaq2PEP8iCu67POWx2bBh65z-kqTynb-4jDyHaTz0IW5yjnP0TNJ~6-5Uh3nEd28H0zbT9l1zoKql~4ll7xL-Vi5KsuP0kuoCwMBlCAQV9bl83~VwgTn5gDFIQSh-RipY6PlpyDBSSyO6G5cBigMnH9UHxsmroBktggIwzmGLZqXj9F9J7JsHWbUgORDLnYA9UGUImsO2nOrphYHS-Z80aTyOf9qJrfl5AlCKGNUxqtRZKw__&Key-Pair-Id=APKAJLOHF5GGSLRBV4ZA (accessed on 18 February 2024).
- Di Iorio, O.; Gürtler, R.E. Seasonality and temperature-dependent flight dispersal of Triatoma infestans (Hemiptera: Reduviidae) and other vectors of Chagas disease in Western Argentina. J. Med. Entomol. 2017, 54, 1285–1292. [Google Scholar] [CrossRef]
- Dantas, E.S.; Gurgel-Gonçalves, R.; Maciel-De-Freitas, R.; Monteiro, F.A. Simultaneous external and internal marking of Triatoma sordida nymphs: Trace element efficacy and microgeographic dispersal in a peridomestic Brazilian Cerrado rural household. Parasites Vectors 2022, 15, 325–332. [Google Scholar] [CrossRef] [PubMed]
- de Arias, A.R.; Messenger, L.A.; Rolon, M.; Veja, M.C.; Acosta, N.; Villalba, C.; Marcet, P.L. Dynamics of Triatoma infestans populations in the Paraguayan Chaco: Population genetic analysis of household reinfestation following vector control. PLoS ONE 2022, 17, e0263465. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Sousa Leite, L.; de Rezende Feres, V.C.; Scalize, P.S. Predictor Variables in the Spread of Chagas Disease in Rural Areas. Pathogens 2024, 13, 394. https://doi.org/10.3390/pathogens13050394
de Sousa Leite L, de Rezende Feres VC, Scalize PS. Predictor Variables in the Spread of Chagas Disease in Rural Areas. Pathogens. 2024; 13(5):394. https://doi.org/10.3390/pathogens13050394
Chicago/Turabian Stylede Sousa Leite, Liziana, Valéria Christina de Rezende Feres, and Paulo Sérgio Scalize. 2024. "Predictor Variables in the Spread of Chagas Disease in Rural Areas" Pathogens 13, no. 5: 394. https://doi.org/10.3390/pathogens13050394
APA Stylede Sousa Leite, L., de Rezende Feres, V. C., & Scalize, P. S. (2024). Predictor Variables in the Spread of Chagas Disease in Rural Areas. Pathogens, 13(5), 394. https://doi.org/10.3390/pathogens13050394