
Prevalence of Blastocystis spp. and Other Gastrointestinal Pathogens Among Patients Admitted to Research Hospitals in Campania Region, Italy

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Direct Microscopic Fresh Examination of Fecal Samples
2.3. Microscopic Examination After Ridley’s Concentration Method
2.4. Detection of Bacterial Co-Infections
2.4.1. Clostridium Difficile Detection by GDH Immuno-Chromatographic Test: Tox A and Tox B
2.4.2. Helicobacter Pylori Antigen Detection by Immuno-Chromatographic Test
2.4.3. Salmonella spp. Detection
2.5. Detection of Viral Co-Infections
2.6. Fungal Co-Infections by DNA Identification
2.7. Parasitic Co-Infections by Immuno-Chromatographic Tests and Molecular Confirmation
2.8. DNA Extraction, PCR Amplification, and Microarray
2.9. Statistical Analysis
3. Results
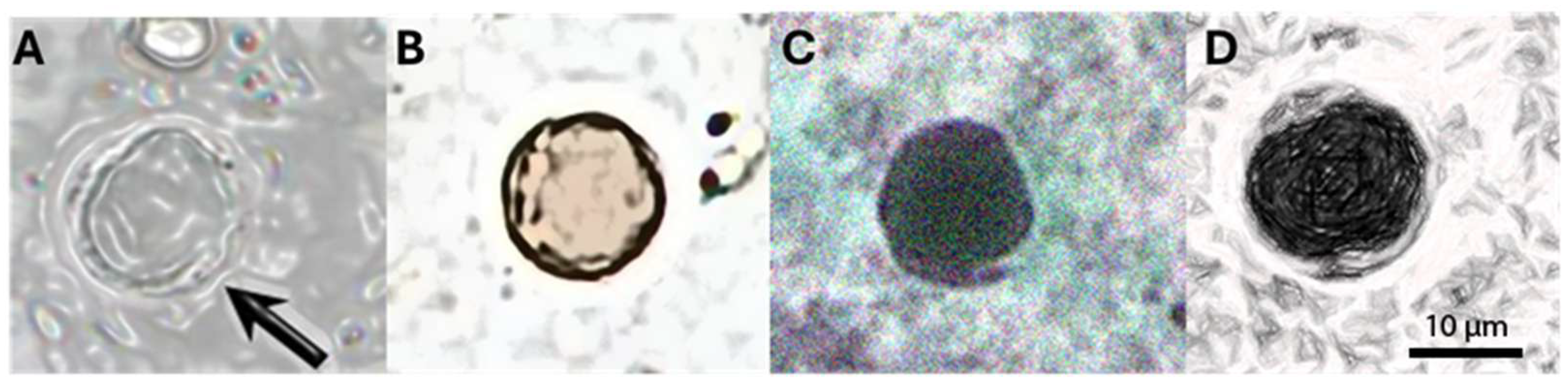
3.1. Prevalence of Blastocystis spp. by Microscopic Detection
3.2. Detection of Co-Infecting Pathogens
3.2.1. Bacterial Co-Infection
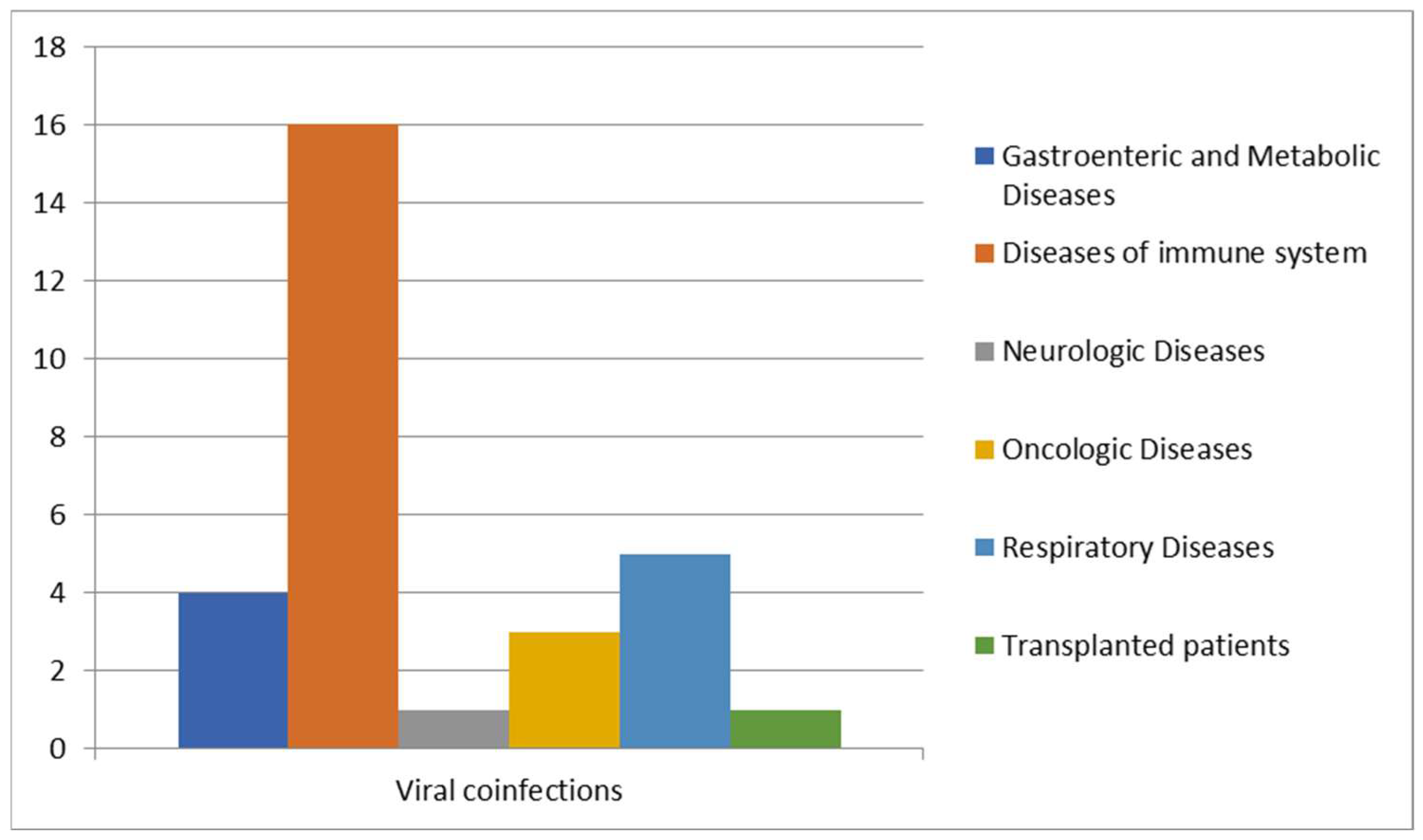
3.2.2. Viral Co-Infections
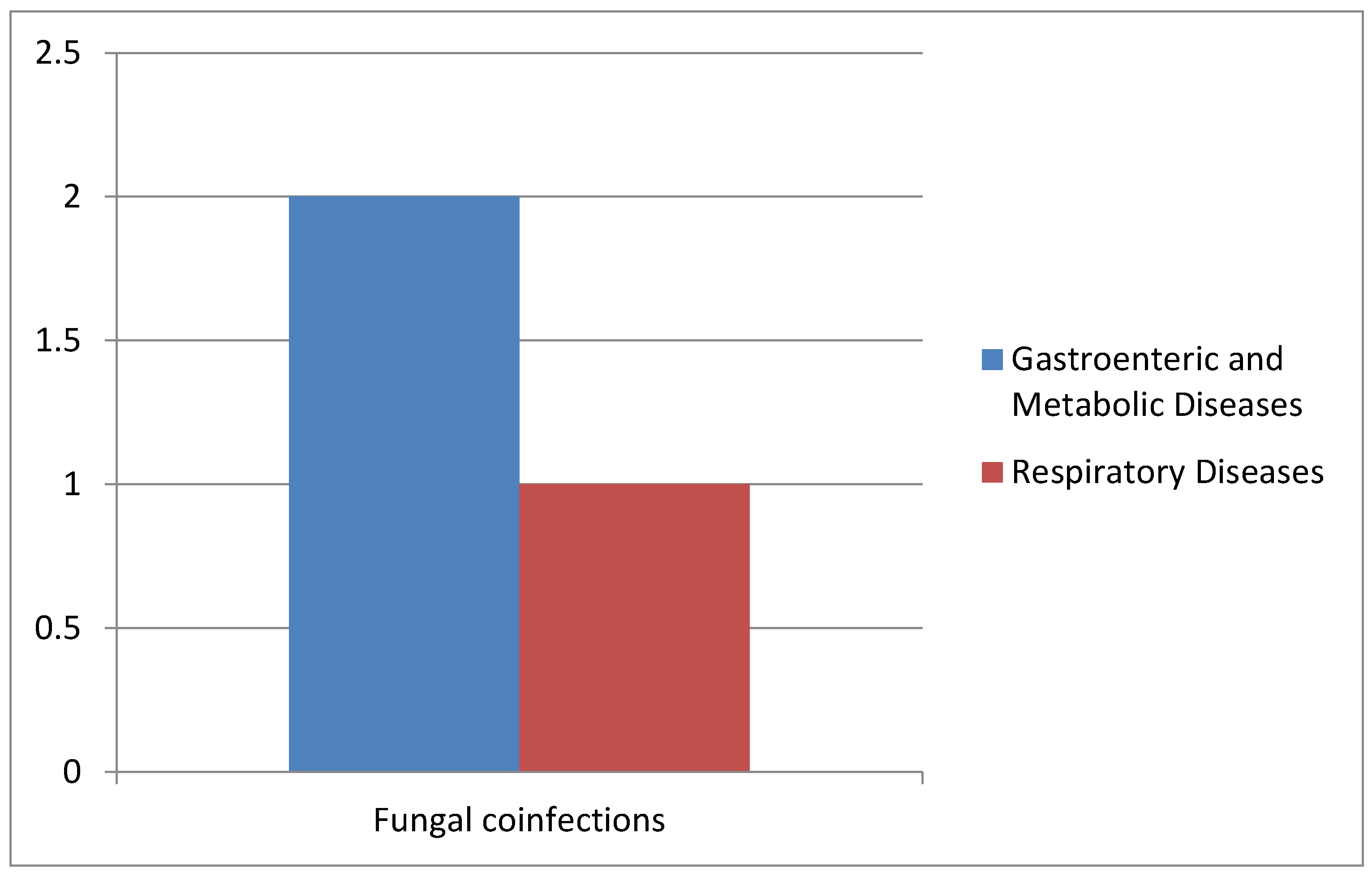
3.2.3. Fungal Co-Infections
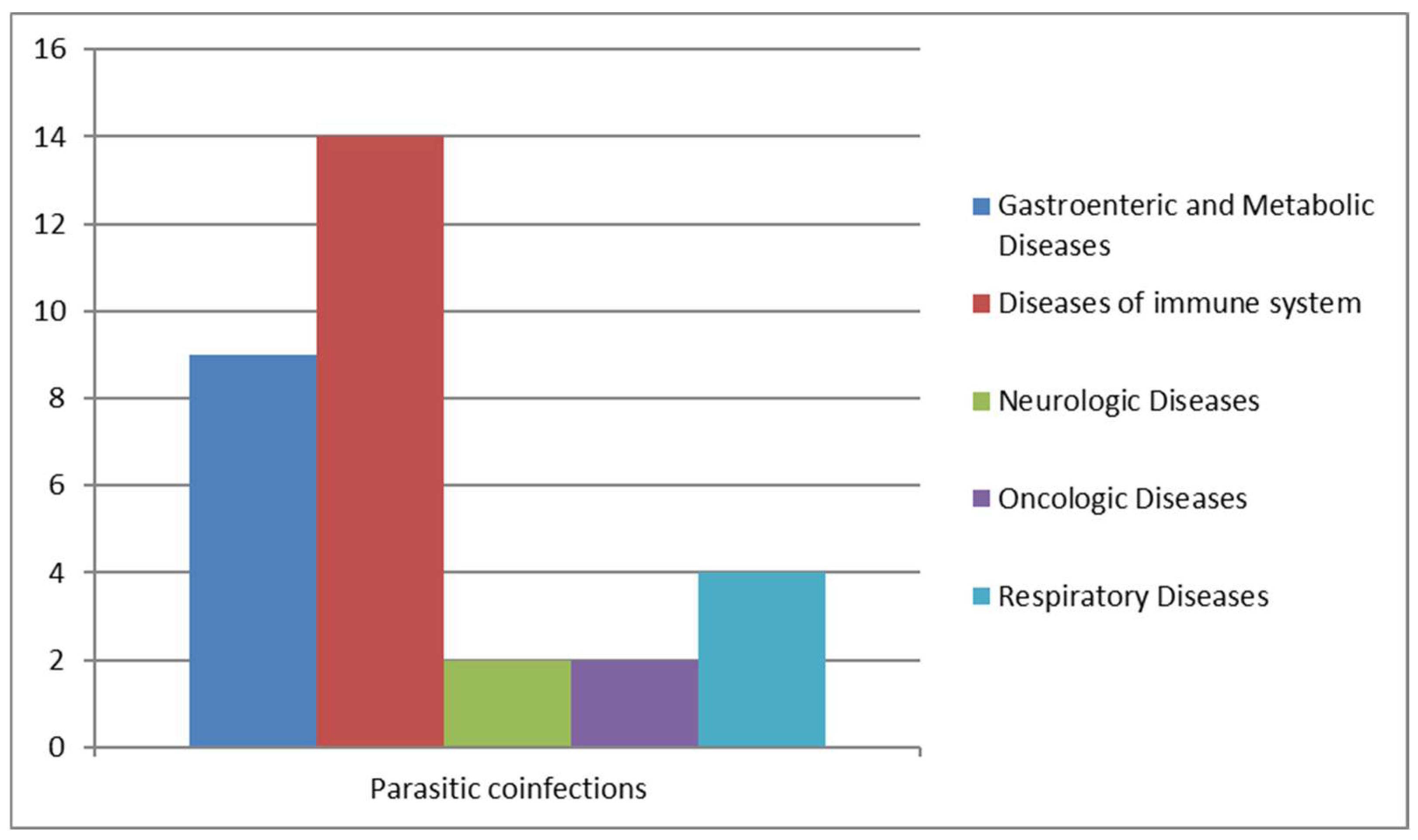
3.2.4. Parasitic Co-Infections
3.2.5. Prevalence of Blastocystis spp.
3.2.6. Molecular Analysis to Characterize Blastocystis spp.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lepczynska, M.; Bialkowska, J.; Dzika, E.; Piskorz-Ogorek, K.; Korycinska, J. Blastocystis: How do specific diets and human gut microbiota affect its development and pathogenicity? Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1531–1540. [Google Scholar] [CrossRef]
- Stenzel, D.J.; Boreham, P.F. Blastocystis hominis revisited. Clin. Microbiol. Rev. 1996, 9, 563–584. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.S. New insights on classification, identification, and clinical relevance of Blastocystis spp. Clin. Microbiol. Rev. 2008, 21, 639–665. [Google Scholar] [CrossRef]
- Ajjampur, S.S.; Tan, K.S. Pathogenic mechanisms in Blastocystis spp.—Interpreting results from in vitro and in vivo studies. Parasitol. Int. 2016, 65, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.S.; Mirza, H.; Teo, J.D.; Wu, B.; Macary, P.A. Current Views on the Clinical Relevance of Blastocystis spp. Curr. Infect. Dis. Rep. 2010, 12, 28–35. [Google Scholar] [CrossRef]
- Kosik-Bogacka, D.; Lepczynska, M.; Kot, K.; Szkup, M.; Lanocha-Arendarczyk, N.; Dzika, E.; Grochans, E. Prevalence, subtypes and risk factors of Blastocystis spp. infection among pre- and perimenopausal women. BMC Infect. Dis. 2021, 21, 1125. [Google Scholar] [CrossRef]
- Parija, S.C. Neglected tropical diseases. Trop. Parasitol. 2022, 12, 67–68. [Google Scholar] [CrossRef]
- Stensvold, C.R.; Clark, C.G. Pre-empting Pandora’s Box: Blastocystis Subtypes Revisited. Trends Parasitol. 2020, 36, 229–232. [Google Scholar] [CrossRef]
- Mohammadpour, I.; Bozorg-Ghalati, F.; Gazzonis, A.L.; Manfredi, M.T.; Motazedian, M.H.; Mohammadpour, N. First molecular subtyping and phylogeny of Blastocystis sp. isolated from domestic and synanthropic animals (dogs, cats and brown rats) in southern Iran. Parasit. Vectors 2020, 13, 365. [Google Scholar] [CrossRef]
- Stensvold, C.R.; Tan, K.S.W.; Clark, C.G. Blastocystis. Trends Parasitol. 2020, 36, 315–316. [Google Scholar] [CrossRef]
- Khaled, S.; Gantois, N.; Ly, A.T.; Senghor, S.; Even, G.; Dautel, E.; Dejager, R.; Sawant, M.; Baydoun, M.; Benamrouz-Vanneste, S.; et al. Prevalence and Subtype Distribution of Blastocystis sp. in Senegalese School Children. Microorganisms 2020, 8, 1408. [Google Scholar] [CrossRef] [PubMed]
- Beghini, F.; Pasolli, E.; Truong, T.D.; Putignani, L.; Caccio, S.M.; Segata, N. Large-scale comparative metagenomics of Blastocystis, a common member of the human gut microbiome. ISME J. 2017, 11, 2848–2863. [Google Scholar] [CrossRef]
- Sanchez-Aguillon, F.; Lopez-Escamilla, E.; Velez-Perez, F.; Martinez-Flores, W.A.; Rodriguez-Zulueta, P.; Martinez-Ocana, J.; Martinez-Hernandez, F.; Romero-Valdovinos, M.; Maravilla, P. Parasitic infections in a Mexican HIV/AIDS cohort. J. Infect. Dev. Ctries. 2013, 7, 763–766. [Google Scholar] [CrossRef]
- Albrecht, H.; Stellbrink, H.J.; Koperski, K.; Greten, H. Blastocystis hominis in human immunodeficiency virus-related diarrhea. Scand. J. Gastroenterol. 1995, 30, 909–914. [Google Scholar] [CrossRef]
- Bednarska, M.; Jankowska, I.; Pawelas, A.; Piwczynska, K.; Bajer, A.; Wolska-Kusnierz, B.; Wielopolska, M.; Welc-Faleciak, R. Prevalence of Cryptosporidium, Blastocystis, and other opportunistic infections in patients with primary and acquired immunodeficiency. Parasitol. Res. 2018, 117, 2869–2879. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Tay, H.; Peng, G.; Lee, J.W.J.; Tan, K.S.W. Prevalence and molecular subtyping of Blastocystis in patients with Clostridium difficile infection, Singapore. Parasit. Vectors 2021, 14, 277. [Google Scholar] [CrossRef]
- Pomari, E.; Ursini, T.; Silva, R.; Leonardi, M.; Ligozzi, M.; Angheben, A. Concomitant Infection of Helicobacter pylori and Intestinal Parasites in Adults Attending a Referral Centre for Parasitic Infections in North Eastern Italy. J. Clin. Med. 2020, 9, 2366. [Google Scholar] [CrossRef] [PubMed]
- Pielok, L.A.; Swarcewicz, J.; Frackowiak, K.; Lisiecka, M. Cryptosporidium spp. and Blastocystis spp. coinfection as a reason of an acute diarrhea in a young healthy veterinary Polish student—Case report. Ann. Agric. Environ. Med. 2022, 29, 592–594. [Google Scholar] [CrossRef]
- Sanchez, A.; Munoz, M.; Gomez, N.; Tabares, J.; Segura, L.; Salazar, A.; Restrepo, C.; Ruiz, M.; Reyes, P.; Qian, Y.; et al. Molecular Epidemiology of Giardia, Blastocystis and Cryptosporidium among Indigenous Children from the Colombian Amazon Basin. Front. Microbiol. 2017, 8, 248. [Google Scholar] [CrossRef]
- Matovelle, C.; Tejedor, M.T.; Monteagudo, L.V.; Beltran, A.; Quilez, J. Prevalence and Associated Factors of Blastocystis sp. Infection in Patients with Gastrointestinal Symptoms in Spain: A Case-Control Study. Trop. Med. Infect. Dis. 2022, 7, 226. [Google Scholar] [CrossRef]
- AMCLI. Available online: https://www.amcli.it/wp-content/uploads/2024/02/2022-25_PARASSITOSI-INTESTINALI.pdf (accessed on 12 December 2024).
- Wormser, G.P.; Hanna, B.A. Manual of Clinical Microbiology, 8th Edition. Edited by Patrick R. Murray, Ellen Jo Baron, James H. Jorgensen, Michael A. Pfaller, and Robert H. Yolken Washington, D.C.: American Society for Microbiology Press, 2003. 2322 pp. $189.95 (cloth). Clin. Infect. Dis. 2004, 38, 1199–1200. [Google Scholar] [CrossRef]
- Zhang, S.X.; Kang, F.Y.; Chen, J.X.; Tian, L.G.; Geng, L.L. Risk factors for Blastocystis infection in HIV/AIDS patients with highly active antiretroviral therapy in Southwest China. Infect. Dis. Poverty 2019, 8, 89. [Google Scholar] [CrossRef]
- Duda, A.; Kosik-Bogacka, D.; Lanocha-Arendarczyk, N.; Kolodziejczyk, L.; Lanocha, A. The prevalence of Blastocystis hominis and other protozoan parasites in soldiers returning from peacekeeping missions. Am. J. Trop. Med. Hyg. 2015, 92, 805–806. [Google Scholar] [CrossRef]
- Parija, S.C.; Jeremiah, S. Blastocystis: Taxonomy, biology and virulence. Trop. Parasitol. 2013, 3, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Hafeez, E.H.; Sanadeki, M.M.; Abdelgelil, N.H.; Shaban, N.M.; Abd Rabou, R.A.M. Is co-infection of intestinal parasites with COVID-19 virus infection affecting its severity? Minia J. Med. Res. 2023, 34, 113–122. [Google Scholar] [CrossRef]
- Audebert, C.; Even, G.; Cian, A.; Blastocystis Investigation, G.; Loywick, A.; Merlin, S.; Viscogliosi, E.; Chabe, M. Colonization with the enteric protozoa Blastocystis is associated with increased diversity of human gut bacterial microbiota. Sci. Rep. 2016, 6, 25255. [Google Scholar] [CrossRef]
- Leung, J.M.; Davenport, M.; Wolff, M.J.; Wiens, K.E.; Abidi, W.M.; Poles, M.A.; Cho, I.; Ullman, T.; Mayer, L.; Loke, P. IL-22-producing CD4+ cells are depleted in actively inflamed colitis tissue. Mucosal Immunol. 2014, 7, 124–133. [Google Scholar] [CrossRef]
- El Safadi, D.; Gaayeb, L.; Meloni, D.; Cian, A.; Poirier, P.; Wawrzyniak, I.; Delbac, F.; Dabboussi, F.; Delhaes, L.; Seck, M.; et al. Children of Senegal River Basin show the highest prevalence of Blastocystis sp. ever observed worldwide. BMC Infect. Dis. 2014, 14, 164. [Google Scholar] [CrossRef]
- Jones, M.S.; Whipps, C.M.; Ganac, R.D.; Hudson, N.R.; Boorom, K. Association of Blastocystis subtype 3 and 1 with patients from an Oregon community presenting with chronic gastrointestinal illness. Parasitol. Res. 2009, 104, 341–345. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AOU of University Hospital of Campania “Luigi Vanvitelli” | ||
|---|---|---|
| Sex | Age | Species |
| Male | 72 | Helicobacter pylori |
| Male | 14 | Clostridium difficile |
| Male | 9 | Enterobacteriaceae |
| Female | 64 | Helicobacter pylori; Clostridium difficile |
| Female | 4 | Salmonella spp. |
| Female | 25 | Escherichia coli Extended-Spectrum-β-Lactamase |
| Female | 65 | Enterobacteriaceae |
| Female | 46 | Enterobacteriaceae |
| Female | 4 | Enterobacteriaceae; Klebsiella pneumoniae |
| Male | 61 | Enterobacteriaceae |
| Male | 59 | Enterobacteriaceae; Clostridium difficile |
| Female | 76 | Clostridium difficile |
| Male | 14 | Enterobacteriaceae; Campylobacter |
| Male | 6 | Enterobacteriaceae |
| Male | 67 | Enterobacteriaceae |
| Female | 55 | Enterobacteriaceae |
| Cotugno Hospital | ||
| Female | 41 | Helicobacter pylori |
| Female | 36 | Enterobacteriaceae |
| Female | 36 | Plesiomonas shigelloides |
| Male | 38 | Treponema pallidum |
| University Hospital of Campania “Luigi Vanvitelli” | ||
|---|---|---|
| Sex | Age | Species |
| Male | 72 | HAV; HBV |
| Male | 14 | HAV |
| Male | 59 | HBV |
| Male | 4 | Adenovirus; CMV; HBV |
| Female | 45 | HSV-1; HSV-2; RuV |
| Female | 4 | EBV; influenzas A and B |
| Male | 58 | CMV |
| Male | 64 | HAV |
| Female | 25 | Coxsackie |
| Female | 4 | HSV-1; HSV-2; RuV |
| Male | 30 | HBV |
| Male | 42 | HBV |
| Cotugno Hospital | ||
| Female | 36 | EBV/SARS-CoV-2 |
| Male | 53 | HIV |
| Male | 43 | HBV |
| Male | 60 | HIV |
| Female | 61 | CMV; SARS-CoV-2 |
| Female | 59 | CMV |
| Female | 44 | HBV |
| Female | 18 | EBV |
| Female | 38 | HIV |
| Female | 39 | HIV |
| Male | 18 | HBV; CMV |
| Male | 18 | HIV; CMV |
| Female | 36 | HBV |
| Male | 37 | HIV |
| Male | 51 | CMV; HAV; HBV |
| Male | 14 | HBC |
| Female | 43 | HAV; HIV |
| University Hospital of Campania “Luigi Vanvitelli” | ||
|---|---|---|
| Sex | Age | Species |
| Male | 74 | Candida spp. |
| Female | 10 | Candida spp. |
| Cotugno Hospital | ||
| Male | 58 | Pnuemocystis jirovecii |
| University Hospital of Campania “Luigi Vanvitelli” | ||
|---|---|---|
| Sex | Age | Species |
| Male | 33 | Chilomastix mesnili |
| Male | 33 | Dientamoeba fragilis |
| Female | 39 | Giardia duodenalis |
| Female | 46 | Entamoeba histolytica/dispar |
| Male | 30 | Schistosoma mansoni |
| Cotugno Hospital | ||
| Female | 57 | Entamoeba histolytica/dispar, Endolimax nana, and Entamoeba coli |
| Female | 44 | Entamoeba histolytica/dispar |
| Female | 46 | Entamoeba histolytica/dispar |
| Male | 39 | Giardia duodenalis |
| Male | 52 | Giardia duodenalis |
| Male | 38 | Entamoeba histolytica/dispar |
| Male | 38 | Giardia intestinalis, Chilomastix mesnili, and Dientamoeba fragilis |
| Male | 40 | Giardia duodenalis |
| Male | 50 | Dientamoeba fragilis |
| Male | 69 | Dientamoeba fragilis |
| Male | 61 | Enterocytozoon bieneusi and Giardia intestinalis |
| Male | 47 | Entamoeba histolytica/dispar |
| Male | 30 | Schistosoma mansoni |
| Male | 18 | Schistosoma mansoni |
| Male | 64 | Dientamoeba fragilis |
| Age of Patients with Co-Infections | ||||
|---|---|---|---|---|
| Age groups | No. total of positive With co-infections | No. of positive With co-infections for age | Incidence (%) | p value |
| 0–20 | 75 | 16 | 21 | 0.708 |
| 21–40 | 75 | 22 | 29 | 0.804 |
| 41–60 | 75 | 23 | 31 | 0.048 |
| 61–80 | 75 | 14 | 19 | 0.420 |
| Characteristics | Total No. of Positives Examined for Blastocystis spp. | No. of Positives with Co-Infections | Incidence (%) | p-Value |
|---|---|---|---|---|
| Gender | ||||
| Male | 78 | 44 | 59 | 0.099 |
| Female | 43 | 31 | 41 | 0.548 |
| Ethnicity | ||||
| Ghana | 5 | 5 | 4 | N/A |
| India | 6 | 4 | 5 | N/A |
| Morocco | 4 | 3 | 3 | N/A |
| Italy | 106 | 106 | 88 | N/A |
| Form of Blastocystis (n =121) | ||||
| Granular | 33 | 27 | <0.005 | |
| Vacuolar | 88 | 73 | <0.005 | |
| Positive Samples | Negative Samples | % Agreement | |
|---|---|---|---|
| Fresh exam and exam after the Ridley concentration | 110 | 11 | 91 |
| Giemsa staining | 45 | 76 | 37.2 |
| Molecular analysis | 121 | 0 | 100 |
| Sensitivity | Specificity | ||
| Standard reference technique (O&P) | 87% | 100% | Standard reference technique (O&P) |
| Molecular analysis | 100% | 100% | Molecular analysis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ascierto, M.; Chianese, A.; Foglia, F.; Finamore, E.; Petrullo, L.; Zannella, C.; De Filippis, A.; Coppola, M.G.; Galdiero, M. Prevalence of Blastocystis spp. and Other Gastrointestinal Pathogens Among Patients Admitted to Research Hospitals in Campania Region, Italy. Pathogens 2025, 14, 425. https://doi.org/10.3390/pathogens14050425
Ascierto M, Chianese A, Foglia F, Finamore E, Petrullo L, Zannella C, De Filippis A, Coppola MG, Galdiero M. Prevalence of Blastocystis spp. and Other Gastrointestinal Pathogens Among Patients Admitted to Research Hospitals in Campania Region, Italy. Pathogens. 2025; 14(5):425. https://doi.org/10.3390/pathogens14050425
Chicago/Turabian StyleAscierto, Marianna, Annalisa Chianese, Francesco Foglia, Emiliana Finamore, Luciana Petrullo, Carla Zannella, Anna De Filippis, Maria Grazia Coppola, and Massimiliano Galdiero. 2025. "Prevalence of Blastocystis spp. and Other Gastrointestinal Pathogens Among Patients Admitted to Research Hospitals in Campania Region, Italy" Pathogens 14, no. 5: 425. https://doi.org/10.3390/pathogens14050425
APA StyleAscierto, M., Chianese, A., Foglia, F., Finamore, E., Petrullo, L., Zannella, C., De Filippis, A., Coppola, M. G., & Galdiero, M. (2025). Prevalence of Blastocystis spp. and Other Gastrointestinal Pathogens Among Patients Admitted to Research Hospitals in Campania Region, Italy. Pathogens, 14(5), 425. https://doi.org/10.3390/pathogens14050425