
Review and Analysis of Platform-Related Performance of Rehabilitation Lower Limb Exoskeletons

 ,
, 
Abstract
:1. Introduction
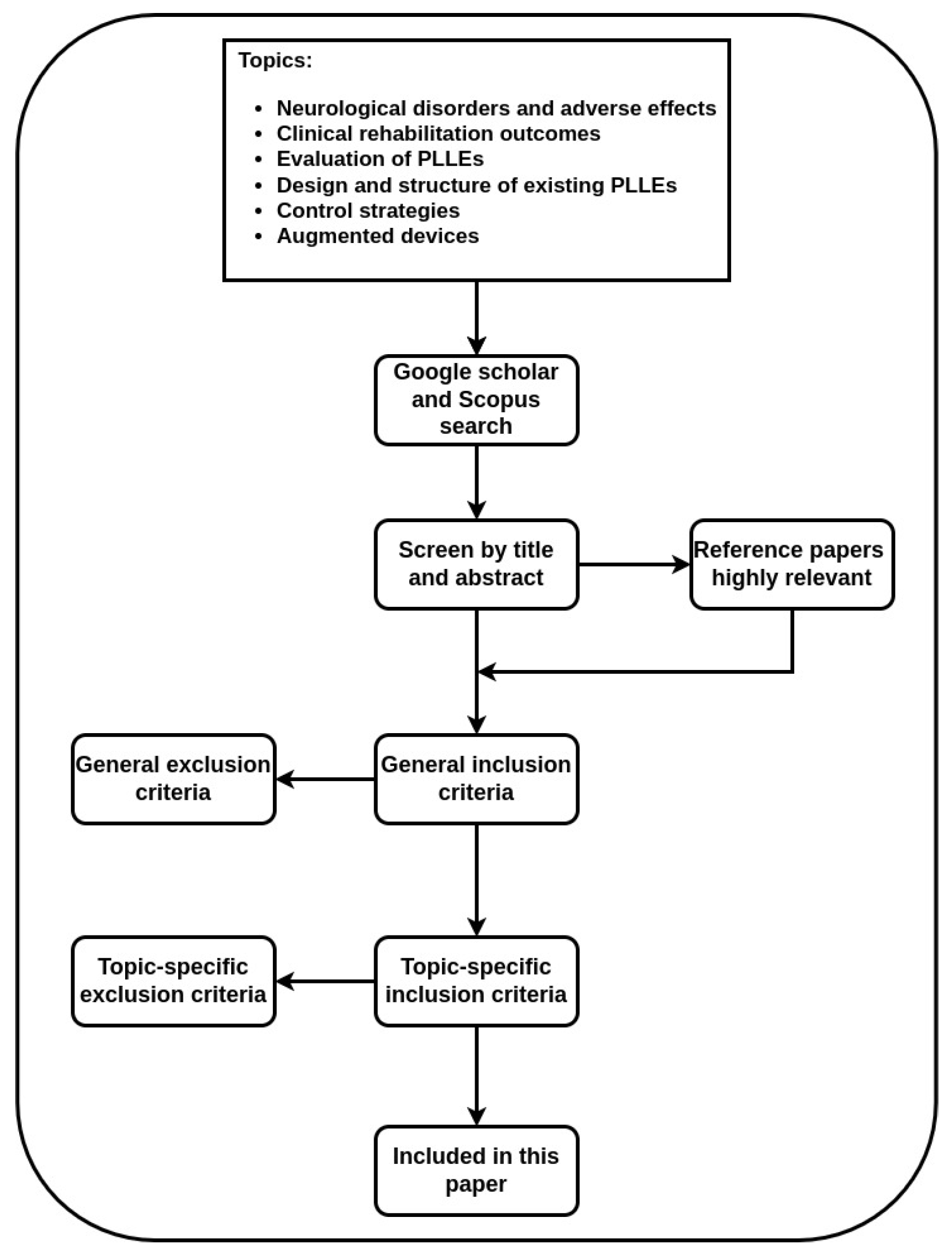
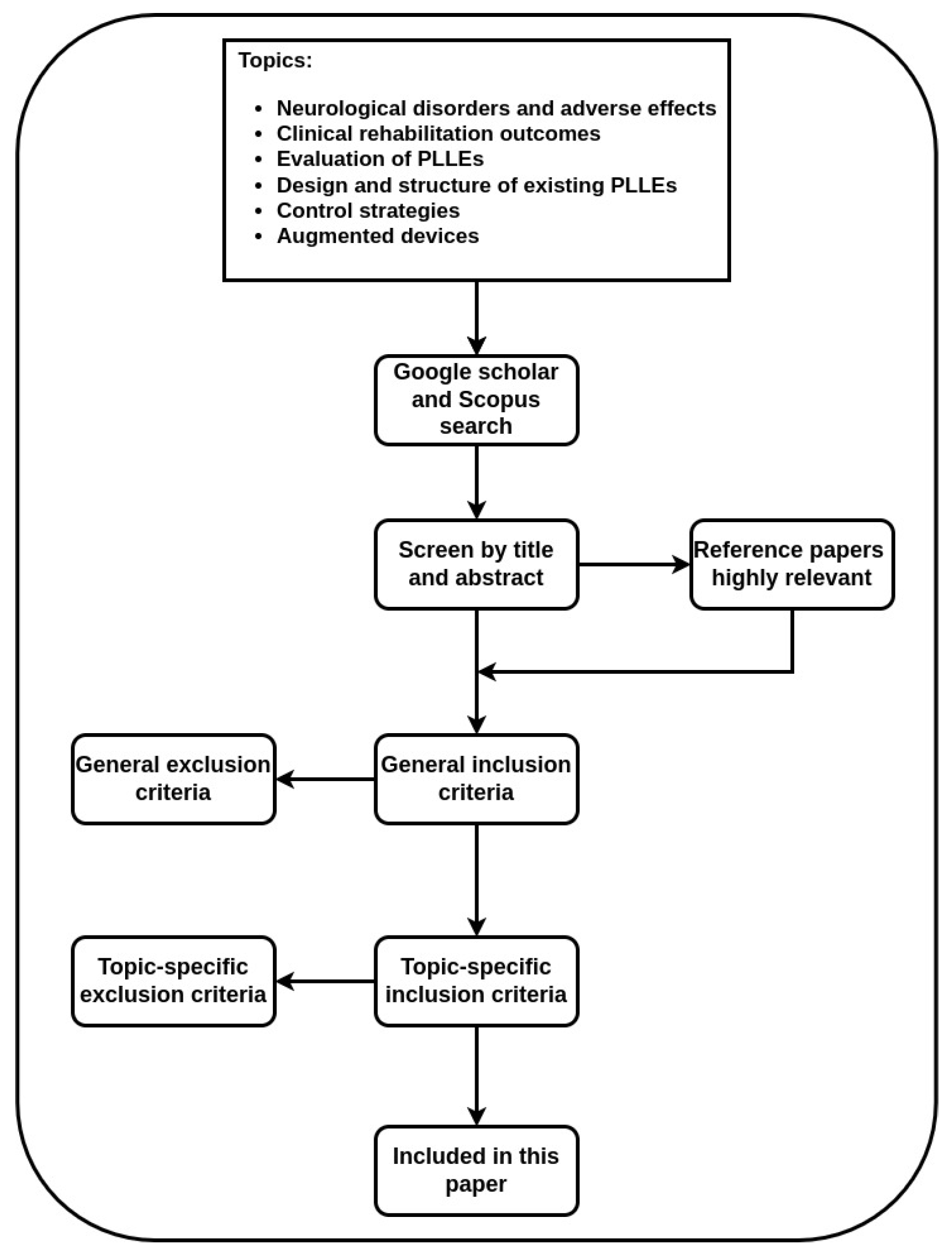
2. Search Methodology and Classification Method
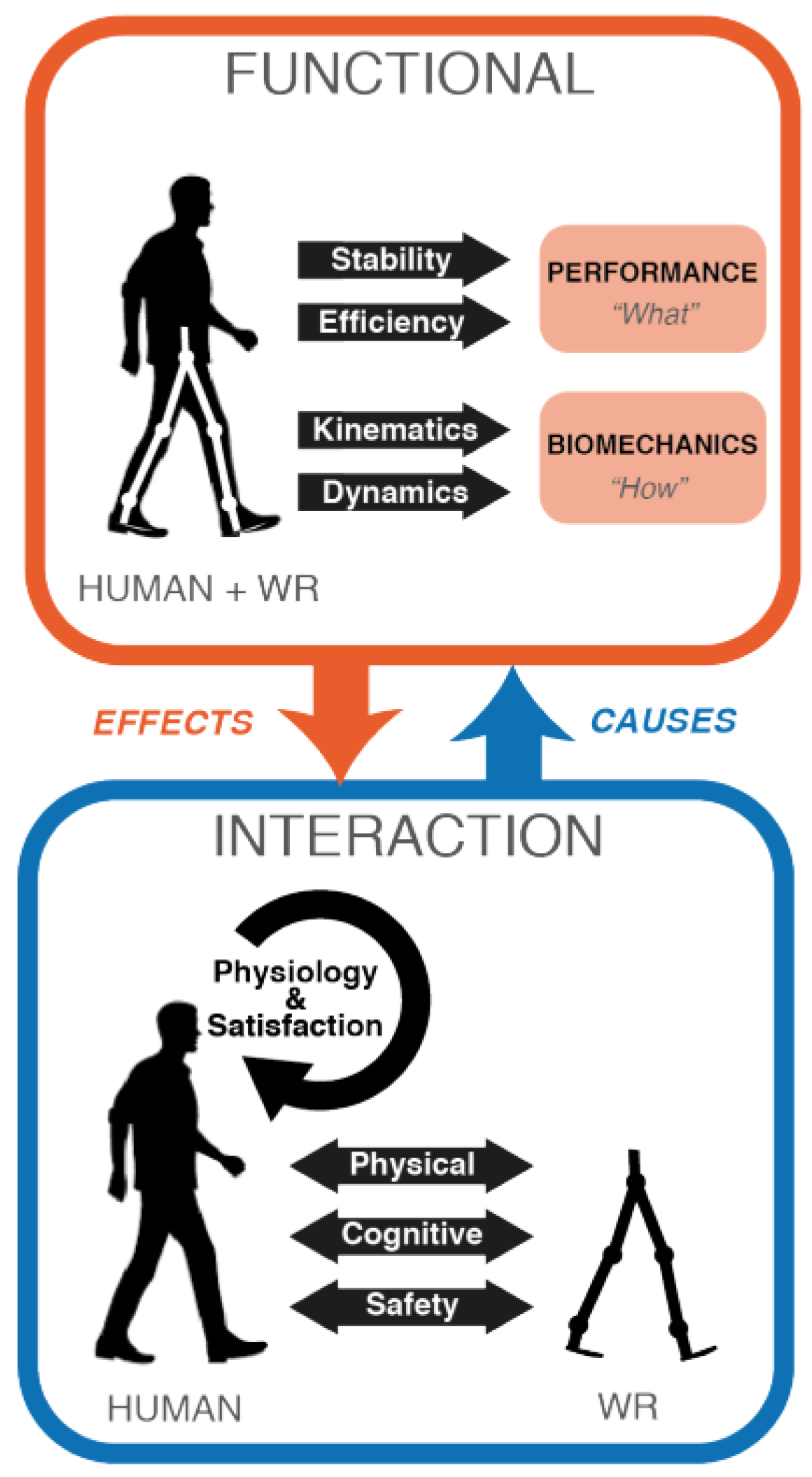
3. Performance Evaluation Criteria
3.1. Criteria Selection
- Gait rehabilitation (GAR);
- Balance maintenance (BAM);
- Decision making (DEM);
- Locomotion modes (LOM);
- Safety, ergonomy and clinical use (SEC).
Robot-Assisted Rehabilitation and Target Population
3.2. Selected Performance Criteria
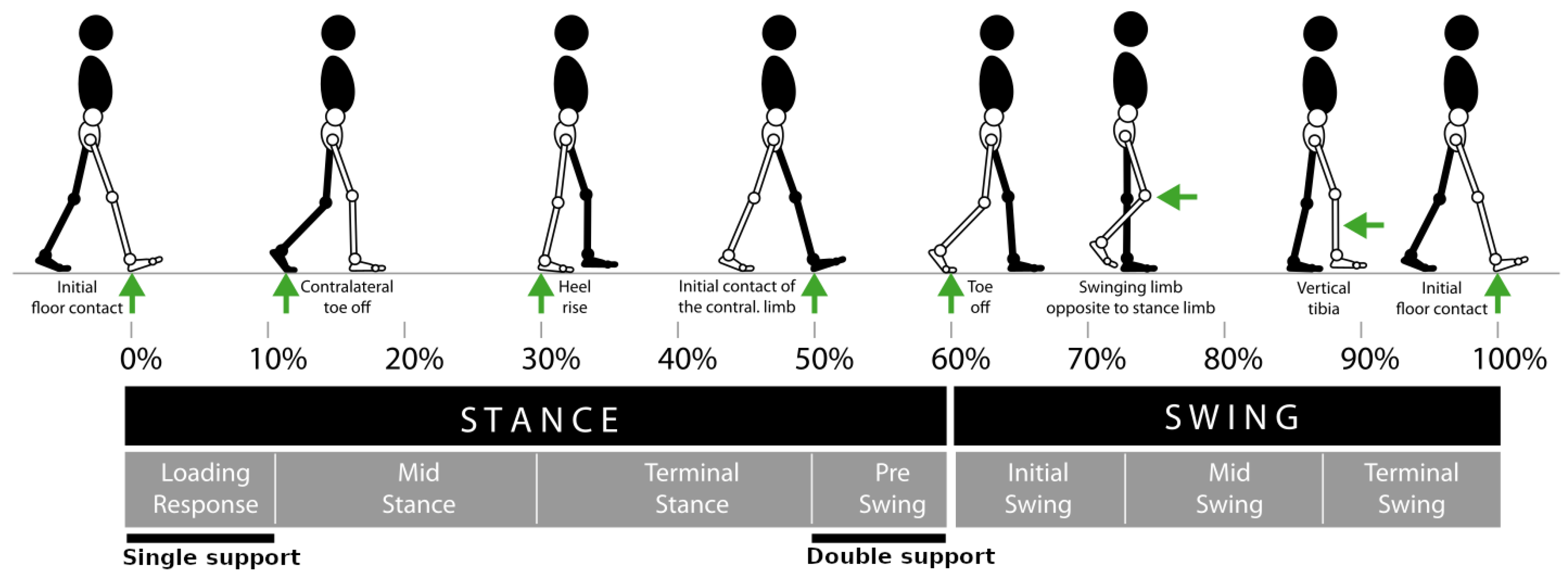
3.2.1. Gait Rehabilitation (GAR)
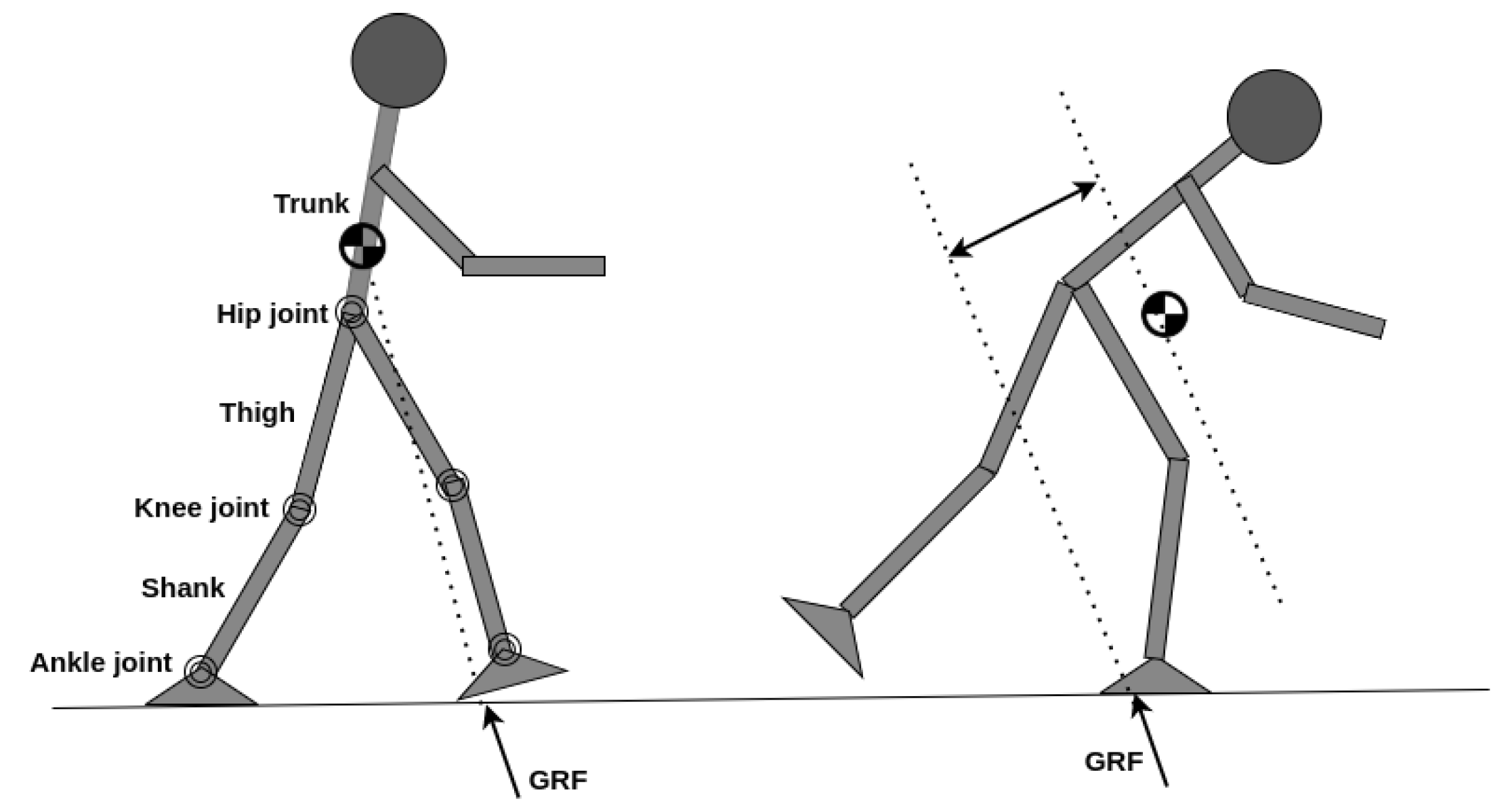
3.2.2. Balance Maintenance (BAM)
3.2.3. Locomotion Modes (LOM)
3.2.4. Decision Making (DEM)
3.2.5. Safety, Ergonomics and Clinical Use (SEC)
4. Platform-Related Apparatus
4.1. Lower limb Exoskeletons
4.2. Control Algorithms and Strategies
4.2.1. Assistive Controllers
- Trajectory-based (position, velocity);
- Force/flow field;
- Impedance and admittance;
- Virtual constraints.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strategy | Ref. | Method | Description |
|---|---|---|---|
| Assistive | [121] | Impedance | Implemented an adaptive impedance controller by introducing an adaptive control law that considers interaction torque of human–exoskeleton. A radial basis function neural network was adopted to approximate the uncertain dynamic. |
| [114] | Tracking | Developed a parameter identification system for both human and exoskeleton and adopted linear quadratic programming method for trajectory tracking. | |
| [118] | AAN | A velocity field in task space was constructed to determine motion velocity limits at any configuration, and implemented a force field controller in joint space, embedding a tunnel for position tracking and control. | |
| [120] | Torque field | Proposed a torque field controller to guarantee coordination between limb joints and also allows the user to vary step length and time. | |
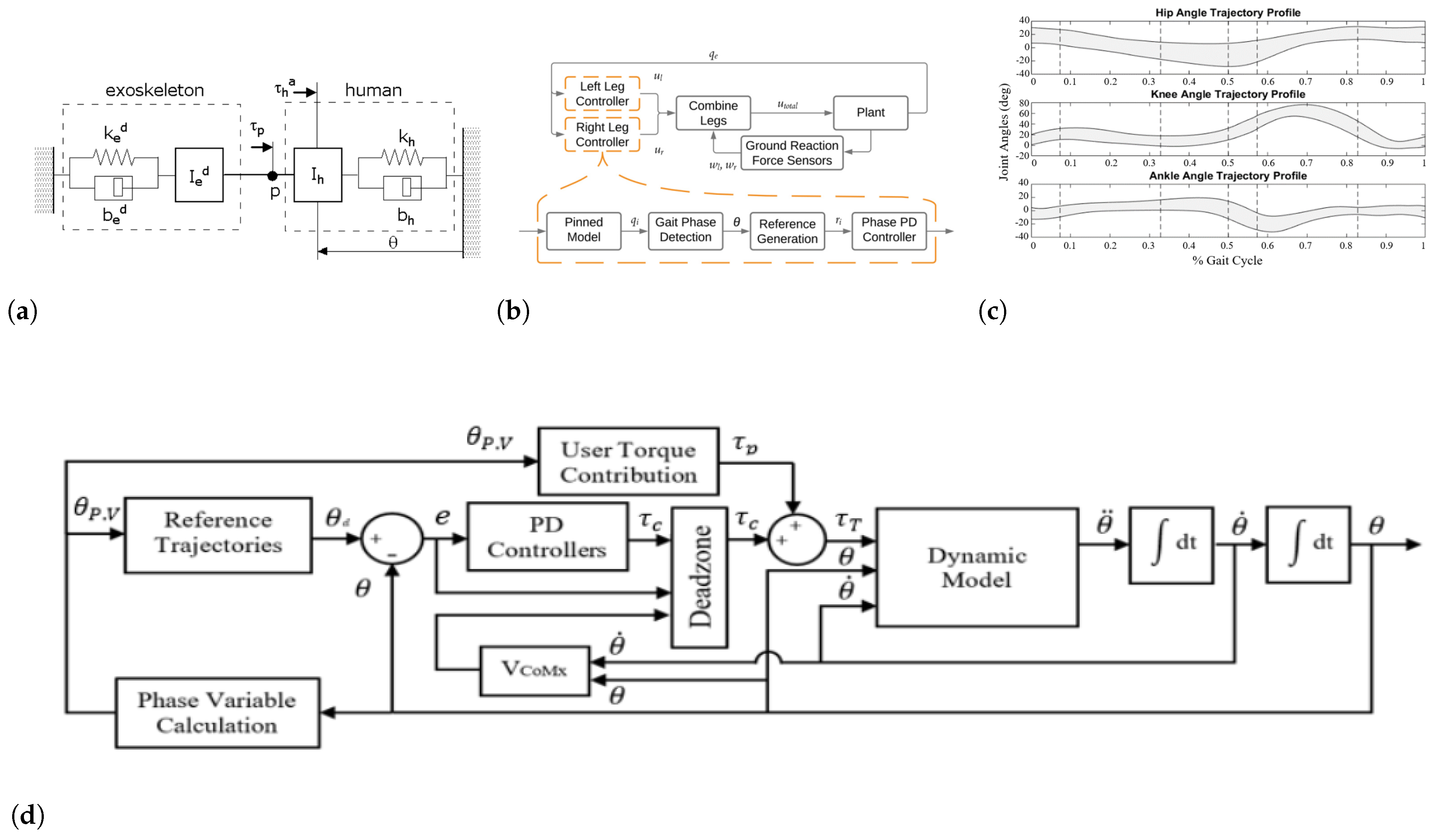
| [108] | Virtual constraints | Proposed a virtual constraint model to generate trajectories autonomously and to ensure stability of the user. This work adopted also AAN method to allow the user to deviate from desired trajectories within a deadzone that is defined according to velocity of CoM. | |
| Volitional | [122] | BMI | Implemented a control framework to feed human detected intentions to the PLLE considering safety issues. This work successfully detects six different intentions. |
| [123] | HMI | This work combined EEG and EMG signals to detect three movement classes of human intentions. | |
| Autonomous | [124] | Synergy | An adaptive synergy-based control is developed to realize impedance adjustment on affected leg following the kinesiological information of healthy leg. |
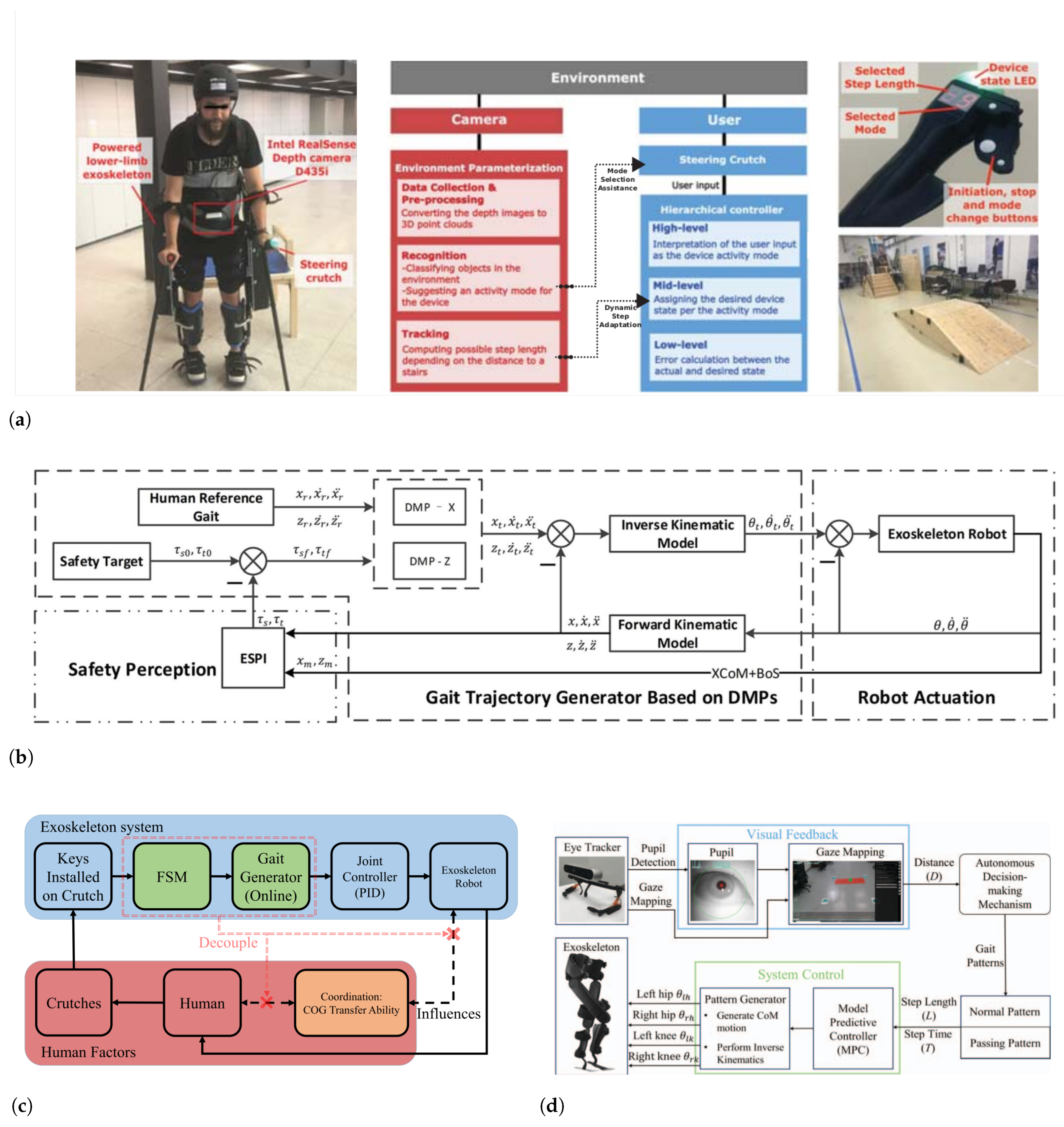
| [125] | Balancing | A safety index based on extrapolated CoM of human–exoskeleton model together with dynamic movement primitives is presented to promote BAM and control of exoskeleton. | |
| [126] | CoG transfer | It presents a control scheme capable of minimizing the reliance on pilot for transferring centre of gravity. It also provides an online trajectory planning considering CoG transfer and safety. |
4.2.2. Challenge-Based Controllers
4.2.3. Volitional Controllers
4.2.4. Autonomous Controllers
4.3. Augmented Devices and Sensors
4.3.1. Functional Electrical Stimulation (FES)
4.3.2. Sensors
4.3.3. EEG/EMG Sensors
4.3.4. Smart Crutches (SMC)
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Federici, S.; Meloni, F.; Bracalenti, M.; De Filippis, M.L. The effectiveness of powered, active lower limb exoskeletons in neurorehabilitation: A systematic review. NeuroRehabilitation 2015, 37, 321–340. [Google Scholar] [PubMed]
- Lajeunesse, V.; Vincent, C.; Routhier, F.; Careau, E.; Michaud, F. Exoskeletons’ design and usefulness evidence according to a systematic review of lower limb exoskeletons used for functional mobility by people with spinal cord injury. Disabil. Rehabil. Assist. Technol. 2016, 11, 535–547. [Google Scholar] [PubMed]
- Lerner, Z.F.; Damiano, D.L.; Bulea, T.C. A lower-extremity exoskeleton improves knee extension in children with crouch gait from cerebral palsy. Sci. Transl. Med. 2017, 9, eaam9145. [Google Scholar]
- Benson, I.; Hart, K.; Tussler, D.; van Middendorp, J.J. Lower-limb exoskeletons for individuals with chronic spinal cord injury: Findings from a feasibility study. Clin. Rehabil. 2016, 30, 73–84. [Google Scholar] [PubMed]
- Dollar, A.M.; Herr, H. Lower Extremity Exoskeletons and Active Orthoses: Challenges and State-of-the-Art. IEEE Trans. Robot. 2008, 24, 144–158. [Google Scholar] [CrossRef]
- Pandy, M.G.; Andriacchi, T.P. Muscle and joint function in human locomotion. Annu. Rev. Biomed. Eng. 2010, 12, 401–433. [Google Scholar]
- Stanev, D.; Moustakas, K. Modeling musculoskeletal kinematic and dynamic redundancy using null space projection. PLoS ONE 2019, 14, e0209171. [Google Scholar]
- Babič, J.; Laffranchi, M.; Tessari, F.; Verstraten, T.; Novak, D.; Šarabon, N.; Ugurlu, B.; Peternel, L.; Torricelli, D.; Veneman, J.F. Challenges and solutions for application and wider adoption of wearable robots. Wearable Technol. 2021, 2, e14. [Google Scholar]
- Bunge, L.R.; Davidson, A.J.; Helmore, B.R.; Mavrandonis, A.D.; Page, T.D.; Schuster-Bayly, T.R.; Kumar, S. Effectiveness of powered exoskeleton use on gait in individuals with cerebral palsy: A systematic review. PLoS ONE 2021, 16, e0252193. [Google Scholar]
- Nedergård, H.; Arumugam, A.; Sandlund, M.; Bråndal, A.; Häger, C.K. Effect of robotic-assisted gait training on objective biomechanical measures of gait in persons post-stroke: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2021, 18, 64. [Google Scholar]
- Shackleton, C.; Evans, R.; Shamley, D.; West, S.; Albertus, Y. Effectiveness of over-ground robotic locomotor training in improving walking performance, cardiovascular demands, secondary complications and user-satisfaction in individuals with spinal cord injuries: A systematic review. J. Rehabil. Med. 2019, 51, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Harvey, L.; Thomas, S.; Elsner, B. Is body-weight-supported treadmill training or robotic-assisted gait training superior to overground gait training and other forms of physiotherapy in people with spinal cord injury? A systematic review. Spinal Cord 2017, 55, 722–729. [Google Scholar] [PubMed]
- Yeung, L.F.; Lau, C.C.; Lai, C.W.; Soo, Y.O.; Chan, M.L.; Tong, R.K. Effects of wearable ankle robotics for stair and over-ground training on sub-acute stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 19. [Google Scholar] [PubMed]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 5, CD006185. [Google Scholar]
- Esquenazi, A.; Talaty, M.; Jayaraman, A. Powered exoskeletons for walking assistance in persons with central nervous system injuries: A narrative review. PM&R 2017, 9, 46–62. [Google Scholar]
- Wang, T.; Zhang, B.; Liu, C.; Liu, T.; Han, Y.; Wang, S.; Ferreira, J.P.; Dong, W.; Zhang, X. A Review on the Rehabilitation Exoskeletons for the Lower Limbs of the Elderly and the Disabled. Electronics 2022, 11, 388. [Google Scholar]
- Kalita, B.; Narayan, J.; Dwivedy, S.K. Development of active lower limb robotic-based orthosis and exoskeleton devices: A systematic review. Int. J. Soc. Robot. 2021, 13, 775–793. [Google Scholar]
- Shi, D.; Zhang, W.; Zhang, W.; Ding, X. A review on lower limb rehabilitation exoskeleton robots. Chin. J. Mech. Eng. 2019, 32, 74. [Google Scholar]
- del Carmen Sanchez-Villamañan, M.; Gonzalez-Vargas, J.; Torricelli, D.; Moreno, J.C.; Pons, J.L. Compliant lower limb exoskeletons: A comprehensive review on mechanical design principles. J. Neuroeng. Rehabil. 2019, 16, 55. [Google Scholar]
- Huo, W.; Mohammed, S.; Moreno, J.C.; Amirat, Y. Lower limb wearable robots for assistance and rehabilitation: A state of the art. IEEE Syst. J. 2014, 10, 1068–1081. [Google Scholar] [CrossRef]
- Pamungkas, D.S.; Caesarendra, W.; Soebakti, H.; Analia, R.; Susanto, S. Overview: Types of lower limb exoskeletons. Electronics 2019, 8, 1283. [Google Scholar] [CrossRef]
- Contreras-Vidal, J.L.; Bhagat, N.A.; Brantley, J.; Cruz-Garza, J.G.; He, Y.; Manley, Q.; Nakagome, S.; Nathan, K.; Tan, S.H.; Zhu, F.; et al. Powered exoskeletons for bipedal locomotion after spinal cord injury. J. Neural Eng. 2016, 13, 031001. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.G.; Ma, X.F.; Huo, B.; Zhang, Y.D.; Yu, X.Y. Recent advances on lower limb exoskeleton rehabilitation robot. Recent Patents Eng. 2017, 11, 194–207. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, A.; Lobo-Prat, J.; Font-Llagunes, J.M. Systematic review on wearable lower-limb exoskeletons for gait training in neuromuscular impairments. J. Neuroeng. Rehabil. 2021, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Yan, T.; Cempini, M.; Oddo, C.M.; Vitiello, N. Review of assistive strategies in powered lower-limb orthoses and exoskeletons. Robot. Auton. Syst. 2015, 64, 120–136. [Google Scholar] [CrossRef]
- Baud, R.; Manzoori, A.R.; Ijspeert, A.; Bouri, M. Review of control strategies for lower-limb exoskeletons to assist gait. J. Neuroeng. Rehabil. 2021, 18, 119. [Google Scholar] [CrossRef]
- Li, W.Z.; Cao, G.Z.; Zhu, A.B. Review on Control Strategies for Lower Limb Rehabilitation Exoskeletons. IEEE Access 2021, 9, 123040–123060. [Google Scholar] [CrossRef]
- Tucker, M.R.; Olivier, J.; Pagel, A.; Bleuler, H.; Bouri, M.; Lambercy, O.; Millán, J.d.R.; Riener, R.; Vallery, H.; Gassert, R. Control strategies for active lower extremity prosthetics and orthotics: A review. J. Neuroeng. Rehabil. 2015, 12, 1. [Google Scholar] [CrossRef]
- Riener, R. The Cybathlon promotes the development of assistive technology for people with physical disabilities. J. Neuroeng. Rehabil. 2016, 13, 49. [Google Scholar] [CrossRef]
- Pinto-Fernandez, D.; Torricelli, D.; del Carmen Sanchez-Villamanan, M.; Aller, F.; Mombaur, K.; Conti, R.; Vitiello, N.; Moreno, J.C.; Pons, J.L. Performance evaluation of lower limb exoskeletons: A systematic review. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1573–1583. [Google Scholar] [CrossRef]
- Torricelli, D.; Pons, J.L. Eurobench: Preparing robots for the real world. In Proceedings of the International Symposium on Wearable Robotics; Springer: Berlin/Heidelberg, Germany, 2018; pp. 375–378. [Google Scholar]
- Torricelli, D.; Rodriguez-Guerrero, C.; Veneman, J.F.; Crea, S.; Briem, K.; Lenggenhager, B.; Beckerle, P. Benchmarking wearable robots: Challenges and recommendations from functional, user experience, and methodological perspectives. Front. Robot. AI 2020, 7, 168. [Google Scholar] [CrossRef] [PubMed]
- Torricelli, D.; Del Ama, A.J.; Gonzalez, J.; Moreno, J.; Gil, A.; Pons, J.L. Benchmarking lower limb wearable robots: Emerging approaches and technologies. In Proceedings of the 8th ACM International Conference on PErvasive Technologies Related to Assistive Environments, Corfu, Greece, 1–3 July 2015; pp. 1–4. [Google Scholar]
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 46. [Google Scholar] [PubMed]
- Ma, V.Y.; Chan, L.; Carruthers, K.J. Incidence, prevalence, costs, and impact on disability of common conditions requiring rehabilitation in the United States: Stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, osteoarthritis, rheumatoid arthritis, limb loss, and back pain. Arch. Phys. Med. Rehabil. 2014, 95, 986–995. [Google Scholar] [PubMed]
- Adams, R.; Gandevia, S.; Skuse, N. The distribution of muscle weakness in upper motoneuron lesions affecting the lower limb. Brain 1990, 113, 1459–1476. [Google Scholar] [CrossRef]
- Da Vies, J.; Mayston, M.; Newham, D. Electrical and mechanical output of the knee muscles during isometric and isokinetic activity in stroke and healthy adults. Disabil. Rehabil. 1996, 18, 83–90. [Google Scholar] [CrossRef]
- Harris, M.; Polkey, M.; Bath, P.M.; Moxham, J. Quadriceps muscle weakness following acute hemiplegic stroke. Clin. Rehabil. 2001, 15, 274–281. [Google Scholar] [CrossRef]
- McComas, A.; Sica, R.; Upton, A.; Aguilera, N. Functional changes in motoneurones of hemiparetic patients. J. Neurol. Neurosurg. Psychiatry 1973, 36, 183–193. [Google Scholar]
- Clark, D.J.; Ting, L.H.; Zajac, F.E.; Neptune, R.R.; Kautz, S.A. Merging of healthy motor modules predicts reduced locomotor performance and muscle coordination complexity post-stroke. J. Neurophysiol. 2010, 103, 844–857. [Google Scholar] [CrossRef]
- Ting, L.H.; McKay, J.L. Neuromechanics of muscle synergies for posture and movement. Curr. Opin. Neurobiol. 2007, 17, 622–628. [Google Scholar]
- Hidler, J.; Carroll, M.; Federovich, E.; Lacsamana, C. Loss of differential muscle control leads to weakness and discoordination in individuals with acute hemiparetic stroke. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No. 03CH37439), Cancun, Mexico, 17–21 September 2003; IEEE: New York, NY, USA, 2003; Volume 2, pp. 1468–1470. [Google Scholar]
- Dobkin, B.H. Rehabilitation after stroke. N. Engl. J. Med. 2005, 352, 1677–1684. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Cacciola, A.; Berté, F.; Manuli, A.; Leo, A.; Bramanti, A.; Naro, A.; Milardi, D.; Bramanti, P. Robotic gait rehabilitation and substitution devices in neurological disorders: Where are we now? Neurol. Sci. 2016, 37, 503–514. [Google Scholar] [PubMed]
- Hornby, T.G.; Reisman, D.S.; Ward, I.G.; Scheets, P.L.; Miller, A.; Haddad, D.; Fox, E.J.; Fritz, N.E.; Hawkins, K.; Henderson, C.E.; et al. Clinical practice guideline to improve locomotor function following chronic stroke, incomplete spinal cord injury, and brain injury. J. Neurol. Phys. Ther. 2020, 44, 49–100. [Google Scholar] [PubMed]
- Torricelli, D.; Gonzalez, J.; Weckx, M.; Jiménez-Fabián, R.; Vanderborght, B.; Sartori, M.; Dosen, S.; Farina, D.; Lefeber, D.; Pons, J.L. Human-like compliant locomotion: State of the art of robotic implementations. Bioinspiration Biomimetics 2016, 11, 051002. [Google Scholar] [CrossRef] [PubMed]
- Andrews, K.; Brocklehurst, J.; Richards, B.; Laycock, P. The rate of recovery from stroke-and its measurement. Int. Rehabil. Med. 1981, 3, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Skilbeck, C.E.; Wade, D.T.; Hewer, R.L.; Wood, V.A. Recovery after stroke. J. Neurol. Neurosurg. Psychiatry 1983, 46, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Cifu, D.X.; Stewart, D.G. Factors affecting functional outcome after stroke: A critical review of rehabilitation interventions. Arch. Phys. Med. Rehabil. 1999, 80, S35–S39. [Google Scholar] [CrossRef]
- Krakauer, J.W. Motor learning: Its relevance to stroke recovery and neurorehabilitation. Curr. Opin. Neurol. 2006, 19, 84–90. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Lee, T.D.; Winstein, C.; Wulf, G.; Zelaznik, H.N. Motor Control and Learning: A Behavioral Emphasis; Human Kinetics: Windsor, ON, Canada, 2018. [Google Scholar]
- Winstein, C.; Wing, A.; Whitall, J. Motor control and learning principles for rehabilitation of upper limb movements after brain injury. Handb. Neuropsychol. 2003, 9, 79–138. [Google Scholar]
- Shea, J.B.; Morgan, R.L. Contextual interference effects on the acquisition, retention, and transfer of a motor skill. J. Exp. Psychol. Hum. Learn. Mem. 1979, 5, 179. [Google Scholar] [CrossRef]
- Hanlon, R.E. Motor learning following unilateral stroke. Arch. Phys. Med. Rehabil. 1996, 77, 811–815. [Google Scholar] [CrossRef]
- Van Peppen, R.P.; Kwakkel, G.; Wood-Dauphinee, S.; Hendriks, H.J.; Van der Wees, P.J.; Dekker, J. The impact of physical therapy on functional outcomes after stroke: What’s the evidence? Clin. Rehabil. 2004, 18, 833–862. [Google Scholar] [PubMed]
- Langhammer, B.; Stanghelle, J.K. Bobath or motor relearning programme? A comparison of two different approaches of physiotherapy in stroke rehabilitation: A randomized controlled study. Clin. Rehabil. 2000, 14, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Pennycott, A.; Wyss, D.; Vallery, H.; Klamroth-Marganska, V.; Riener, R. Towards more effective robotic gait training for stroke rehabilitation: A review. J. Neuroeng. Rehabil. 2012, 9, 65. [Google Scholar] [CrossRef]
- Riener, R.; Lünenburger, L.; Colombo, G. Human-centered robotics applied to gait training and assessment. J. Rehabil. Res. Dev. 2006, 43, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Heins, S.; Dehem, S.; Montedoro, V.; Dehez, B.; Edwards, M.; Stoquart, G.; Rocca, F.; De Deken, P.H.; Mancas, M.; Lejeune, T. Robotic-assisted serious game for motor and cognitive post-stroke rehabilitation. In Proceedings of the 2017 IEEE 5th International Conference on Serious Games and Applications for Health (SeGAH), Perth, WA, Australia, 2–4 April 2017; IEEE: New York, NY, USA, 2017; pp. 1–8. [Google Scholar]
- Metzger, J.C.; Lambercy, O.; Califfi, A.; Dinacci, D.; Petrillo, C.; Rossi, P.; Conti, F.M.; Gassert, R. Assessment-driven selection and adaptation of exercise difficulty in robot-assisted therapy: A pilot study with a hand rehabilitation robot. J. Neuroeng. Rehabil. 2014, 11, 154. [Google Scholar]
- Choi, Y.; Qi, F.; Gordon, J.; Schweighofer, N. Performance-based adaptive schedules enhance motor learning. J. Mot. Behav. 2008, 40, 273–280. [Google Scholar] [CrossRef]
- Goswami, A.; Kallem, V. Rate of change of angular momentum and balance maintenance of biped robots. In Proceedings of the IEEE International Conference on Robotics and Automation, ICRA’04, New Orleans, LA, USA, 26 April–1 May 2004; IEEE: New York, NY, USA, 2004; Volume 4, pp. 3785–3790. [Google Scholar]
- Kuo, A.D.; Zajac, F.E. Human standing posture: Multi-joint movement strategies based on biomechanical constraints. Prog. Brain Res. 1993, 97, 349–358. [Google Scholar]
- Townsend, M.A. Biped gait stabilization via foot placement. J. Biomech. 1985, 18, 21–38. [Google Scholar] [CrossRef]
- Hamza, M.F.; Ghazilla, R.A.R.; Muhammad, B.B.; Yap, H.J. Balance and stability issues in lower extremity exoskeletons: A systematic review. Biocybern. Biomed. Eng. 2020, 40, 1666–1679. [Google Scholar]
- MacKinnon, C.D.; Winter, D.A. Control of whole body balance in the frontal plane during human walking. J. Biomech. 1993, 26, 633–644. [Google Scholar] [CrossRef]
- Vukobratovic, M.; Borovac, B.; Surla, D.; Stokic, D. Biped Locomotion: Dynamics, Stability, Control and Application; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012; Volume 7. [Google Scholar]
- Vaughan, C.L.K. The Biomechanics of Human Locomotion. 2009. Available online: https://open.uct.ac.za/handle/11427/3491 (accessed on 26 July 2023).
- Bruijn, S.M.; Meijer, O.G.; Beek, P.J.; Van Dieen, J.H. The effects of arm swing on human gait stability. J. Exp. Biol. 2010, 213, 3945–3952. [Google Scholar] [CrossRef] [PubMed]
- Vallery, H.; Bögel, A.; O’ Brien, C.; Riener, R. Cooperative control design for robot-assisted balance during gait. De Gruyter (O) 2012, 60, 715–720. [Google Scholar] [CrossRef]
- Zhang, F.; Liu, M.; Huang, H. Effects of locomotion mode recognition errors on volitional control of powered above-knee prostheses. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 23, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Alingh, J.; Fleerkotte, B.; Groen, B.; Rietman, J.; Weerdesteyn, V.; van Asseldonk, E.; Geurts, A.; Buurke, J. Effect of assist-as-needed robotic gait training on the gait pattern post stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 26. [Google Scholar] [CrossRef]
- Cai, L.L.; Fong, A.J.; Liang, Y.; Burdick, J.; Edgerton, V.R. Assist-as-needed training paradigms for robotic rehabilitation of spinal cord injuries. In Proceedings of the 2006 IEEE International Conference on Robotics and Automation, ICRA 2006, Orlando, FL, USA, 15–19 May 2006; IEEE: New York, NY, USA, 2006; pp. 3504–3511. [Google Scholar]
- Li, Z.; Zhao, K.; Zhang, L.; Wu, X.; Zhang, T.; Li, Q.; Li, X.; Su, C.Y. Human-in-the-loop control of a wearable lower limb exoskeleton for stable dynamic walking. IEEE/ASME Trans. Mechatronics 2020, 26, 2700–2711. [Google Scholar] [CrossRef]
- Zhang, J.; Fiers, P.; Witte, K.A.; Jackson, R.W.; Poggensee, K.L.; Atkeson, C.G.; Collins, S.H. Human-in-the-loop optimization of exoskeleton assistance during walking. Science 2017, 356, 1280–1284. [Google Scholar] [CrossRef]
- Meyer, J.T.; Schrade, S.O.; Lambercy, O.; Gassert, R. User-centered design and evaluation of physical interfaces for an exoskeleton for paraplegic users. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; IEEE: New York, NY, USA, 2019; pp. 1159–1166. [Google Scholar]
- Rajasekaran, V.; Aranda, J.; Casals, A. Compliant gait assistance triggered by user intention. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; IEEE: New York, NY, USA, 2015; pp. 3885–3888. [Google Scholar]
- Suzuki, K.; Kawamura, Y.; Hayashi, T.; Sakurai, T.; Hasegawa, Y.; Sankai, Y. Intention-based walking support for paraplegia patient. In Proceedings of the 2005 IEEE International Conference on Systems, Man and Cybernetics, Waikoloa, HI, USA, 12 October 2005; IEEE: New York, NY, USA, 2005; Volume 3, pp. 2707–2713. [Google Scholar]
- Kawamoto, H.; Hayashi, T.; Sakurai, T.; Eguchi, K.; Sankai, Y. Development of single leg version of HAL for hemiplegia. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; IEEE: New York, NY, USA, 2009; pp. 5038–5043. [Google Scholar]
- Ferris, D.P.; Huang, H.J.; Kao, P.C. Moving the arms to activate the legs. Exerc. Sport Sci. Rev. 2006, 34, 113–120. [Google Scholar] [CrossRef]
- Stephenson, J.L.; Lamontagne, A.; De Serres, S.J. The coordination of upper and lower limb movements during gait in healthy and stroke individuals. Gait Posture 2009, 29, 11–16. [Google Scholar] [CrossRef]
- Hassan, M.; Kadone, H.; Suzuki, K.; Sankai, Y. Exoskeleton robot control based on cane and body joint synergies. In Proceedings of the 2012 IEEE/RSJ International Conference on Intelligent Robots and Systems, Vilamoura-Algarve, Portugal, 7–12 October 2012; pp. 1609–1614. [Google Scholar]
- Li, Y.; Sun, H.; Wang, C.; Yang, Y.; Fan, C.; Zhang, Z.; Rui, Y. Key Technologies of Lower Limb Power-Assisted Exoskeleton Robots: A Review. In Proceedings of the 2021 6th International Conference on Control, Robotics and Cybernetics (CRC), Shanghai, China, 9–11 October 2021; IEEE: New York, NY, USA, 2021; pp. 25–31. [Google Scholar]
- Mickelborough, J.; Van Der Linden, M.; Tallis, R.; Ennos, A. Muscle activity during gait initiation in normal elderly people. Gait Posture 2004, 19, 50–57. [Google Scholar] [CrossRef]
- Novak, D.; Reberšek, P.; De Rossi, S.M.M.; Donati, M.; Podobnik, J.; Beravs, T.; Lenzi, T.; Vitiello, N.; Carrozza, M.C.; Munih, M. Automated detection of gait initiation and termination using wearable sensors. Med. Eng. Phys. 2013, 35, 1713–1720. [Google Scholar] [CrossRef]
- Bessler, J.; Prange-Lasonder, G.B.; Schaake, L.; Saenz, J.F.; Bidard, C.; Fassi, I.; Valori, M.; Bach Lassen, A.; Buurke, J.H. Safety assessment of rehabilitation robots: A review identifying safety skills and current knowledge gaps. Front. Robot. AI 2021, 8, 33. [Google Scholar] [CrossRef]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2018, 9, CD006876. [Google Scholar] [CrossRef]
- Bessler, J.; Prange-Lasonder, G.B.; Schulte, R.V.; Schaake, L.; Prinsen, E.C.; Buurke, J.H. Occurrence and type of adverse events during the use of stationary gait robots—A systematic literature review. FRontiers Robot. AI 2020, 7, 557606. [Google Scholar] [CrossRef]
- He, Y.; Eguren, D.; Luu, T.P.; Contreras-Vidal, J.L. Risk management and regulations for lower limb medical exoskeletons: A review. Med. Devices 2017, 10, 89. [Google Scholar] [CrossRef]
- Rocon, E.; Ruiz, A.; Raya, R.; Schiele, A.; Pons, J.L.; Belda-Lois, J.; Poveda, R.; Vivas, M.; Moreno, J. Human-robot physical interaction. Wearable Robot. Biomechatron. Exoskelet. 2008, 127–163. [Google Scholar]
- Chaichaowarat, R.; Macha, V.; Wannasuphoprasit, W. Passive knee exoskeleton using brake torque to assist stair ascent. In Proceedings of the 2020 IEEE REGION 10 CONFERENCE (TENCON), Osaka, Japan, 16–19 November 2020; IEEE: New York, NY, USA, 2020; pp. 1165–1170. [Google Scholar]
- Ármannsdóttir, A.L.; Beckerle, P.; Moreno, J.C.; van Asseldonk, E.H.; Manrique-Sancho, M.T.; Del-Ama, A.J.; Veneman, J.F.; Briem, K. Assessing the involvement of users during development of lower limb wearable robotic exoskeletons: A survey study. Hum. Factors 2020, 62, 351–364. [Google Scholar] [CrossRef]
- Harman, E.; Hoon, K.; Frykman, P.; Pandorf, C. The Effects of Backpack Weight on the Biomechanics of Load Carriage; Technical Report; Army Research Inst of Environmental Medicine Natick Ma Military Performancediv: Natick, MA, USA, 2000. [Google Scholar]
- Kitatani, R.; Ohata, K.; Takahashi, H.; Shibuta, S.; Hashiguchi, Y.; Yamakami, N. Reduction in energy expenditure during walking using an automated stride assistance device in healthy young adults. Arch. Phys. Med. Rehabil. 2014, 95, 2128–2133. [Google Scholar] [CrossRef]
- Pröbsting, E.; Kannenberg, A.; Zacharias, B. Safety and walking ability of KAFO users with the C-Brace® Orthotronic Mobility System, a new microprocessor stance and swing control orthosis. Prosthetics Orthot. Int. 2017, 41, 65–77. [Google Scholar] [CrossRef]
- AlterG, Inc. Bionic Leg User Manual. 2015. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwiZ4Or6l5-CAxW9slYBHZeXDp0QFnoECBUQAQ&url=https%3A%2F%2Falterg.com%2Fwp-content%2Fuploads%2F2022%2F08%2FAlterG-M-F320-User-Man-114422-00-Rev-C.pdf&usg=AOvVaw1pLx3T8QMD1QjeJyEBjt2k&opi=89978449 (accessed on 25 July 2023).
- Puyuelo-Quintana, G.; Cano-De-La-Cuerda, R.; Plaza-Flores, A.; Garces-Castellote, E.; Sanz-Merodio, D.; Goñi-Arana, A.; Marín-Ojea, J.; García-Armada, E. A new lower limb portable exoskeleton for gait assistance in neurological patients: A proof of concept study. J. Neuroeng. Rehabil. 2020, 17, 60. [Google Scholar] [CrossRef]
- Birch, N.; Graham, J.; Priestley, T.; Heywood, C.; Sakel, M.; Gall, A.; Nunn, A.; Signal, N. Results of the first interim analysis of the RAPPER II trial in patients with spinal cord injury: Ambulation and functional exercise programs in the REX powered walking aid. J. Neuroeng. Rehabil. 2017, 14, 60. [Google Scholar] [CrossRef]
- Bionics, E. Ekso GT Lower Limb Exoskeleton. 2022. Available online: https://www.eksobionics.com/ (accessed on 28 July 2023).
- Laffranchi, M.; D’Angella, S.; Vassallo, C.; Piezzo, C.; Canepa, M.; De Giuseppe, S.; Di Salvo, M.; Succi, A.; Cappa, S.; Cerruti, G.; et al. User-Centered design and development of the modular TWIN lower limb exoskeleton. Front. Neurorobot. 2021, 15, 709731. [Google Scholar] [CrossRef]
- Parker Hannifin Corporation Indego Lower Limb Exoskeleton. 2022. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwiMv6CjmJ-CAxWzlFYBHYLnAIQQFnoECBYQAQ&url=https%3A%2F%2Fwww.medtechdive.com%2Fnews%2Fekso-bionics-parker-hannifin-sells-indego-exoskeleton%2F638167%2F&usg=AOvVaw3KABjpFrVvWrvzOAn6CyQg&opi=89978449 (accessed on 28 July 2023).
- Zoss, A.B.; Kazerooni, H.; Chu, A. Biomechanical design of the Berkeley lower extremity exoskeleton (BLEEX). IEEE/ASME Trans. Mechatronics 2006, 11, 128–138. [Google Scholar]
- Crabtree, C.A.; Higginson, J.S. Modeling neuromuscular effects of ankle foot orthoses (AFOs) in computer simulations of gait. Gait Posture 2009, 29, 65–70. [Google Scholar]
- Miyazaki, S.; Yamamoto, S.; Kubota, T. Effect of ankle-foot orthosis on active ankle moment in patients with hemiparesis. Med. Biol. Eng. Comput. 1997, 35, 381–385. [Google Scholar] [CrossRef]
- Geyer, H.; Seyfarth, A.; Blickhan, R. Compliant leg behaviour explains basic dynamics of walking and running. Proc. R. Soc. B Biol. Sci. 2006, 273, 2861–2867. [Google Scholar]
- Aguirre-Ollinger, G.; Colgate, J.E.; Peshkin, M.A.; Goswami, A. Active-impedance control of a lower-limb assistive exoskeleton. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; IEEE: New York, NY, USA, 2007; pp. 188–195. [Google Scholar]
- Goo, A.; Laubscher, C.A.; Sawicki, J.T. Hybrid Zero Dynamics Control of an Underactuated Lower-Limb Exoskeleton for Gait Guidance. J. Dyn. Syst. Meas. Control. 2022, 144, 061008. [Google Scholar]
- Campbell, S.M.; Diduch, C.P.; Sensinger, J.W. Autonomous assistance-as-needed control of a lower limb exoskeleton with guaranteed stability. IEEE Access 2020, 8, 51168–51178. [Google Scholar] [CrossRef]
- Huang, R.; Cheng, H.; Chen, Y.; Chen, Q.; Lin, X.; Qiu, J. Optimisation of reference gait trajectory of a lower limb exoskeleton. Int. J. Soc. Robot. 2016, 8, 223–235. [Google Scholar]
- Tian, J.; Yuan, L.; Xiao, W.; Ran, T.; He, L. Trajectory following control of lower limb exoskeleton robot based on Udwadia–Kalaba theory. J. Vib. Control 2021, 28, 3383–3396. [Google Scholar]
- Amiri, M.S.; Ramli, R.; Ibrahim, M.F. Hybrid design of PID controller for four DoF lower limb exoskeleton. Appl. Math. Model. 2019, 72, 17–27. [Google Scholar]
- Narayan, J.; Kalani, A.; Dwivedy, S.K. Reference trajectory based Jacobian transpose control of a novel lower limb exoskeleton system for children. In Proceedings of the 2019 5th International Conference on Signal Processing, Computing and Control (ISPCC), Solan, India, 10–12 October 2019; IEEE: New York, NY, USA, 2019; pp. 102–107. [Google Scholar]
- Wang, F.; Shi, P.; Li, S.; Zhao, S.; Liu, W. Trajectory control of lower limb exoskeleton robot with variable forgetting factor. In Proceedings of the 2016 12th World Congress on Intelligent Control and Automation (WCICA), Guilin, China, 12–15 June 2016; IEEE: New York, NY, USA, 2016; pp. 1502–1507. [Google Scholar]
- Castro, D.L.; Zhong, C.H.; Braghin, F.; Liao, W.H. Lower limb exoskeleton control via linear quadratic regulator and disturbance observer. In Proceedings of the 2018 IEEE International Conference on Robotics and Biomimetics (ROBIO), Kuala Lumpur, Malaysia, 12–15 December 2018; IEEE: New York, NY, USA, 2018; pp. 1743–1748. [Google Scholar]
- Wang, Y.; Wang, H.; Tian, Y. Adaptive interaction torque-based AAN control for lower limb rehabilitation exoskeleton. ISA Trans. 2021, 128, 184–197. [Google Scholar]
- Maggioni, S.; Reinert, N.; Lünenburger, L.; Melendez-Calderon, A. An adaptive and hybrid end-point/joint impedance controller for lower limb exoskeletons. Front. Robot. AI 2018, 5, 104. [Google Scholar]
- Shi, D.; Zhang, W.; Zhang, W.; Ding, X. Force field control for the three-dimensional gait adaptation using a lower limb rehabilitation robot. In Advances in Mechanism and Machine Science: Proceedings of the 15th IFToMM World Congress on Mechanism and Machine Science; Springer: Berlin/Heidelberg, Germany, 2019; pp. 1919–1928. [Google Scholar]
- Asl, H.J.; Narikiyo, T. An assistive control strategy for rehabilitation robots using velocity field and force field. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; IEEE: New York, NY, USA, 2019; pp. 790–795. [Google Scholar]
- Hidayah, R.; Bishop, L.; Jin, X.; Chamarthy, S.; Stein, J.; Agrawal, S.K. Gait adaptation using a cable-driven active leg exoskeleton (C-ALEX) with post-stroke participants. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1984–1993. [Google Scholar] [CrossRef]
- Martinez, A.; Lawson, B.; Goldfarb, M. A controller for guiding leg movement during overground walking with a lower limb exoskeleton. IEEE Trans. Robot. 2017, 34, 183–193. [Google Scholar]
- Xia, L.; Feng, Y.; Chen, F.; Wu, X. A bio-signal enhanced adaptive impedance controller for lower limb exoskeleton. 2020 IEEE International Conference on Robotics and Automation (ICRA), Paris, France, 31 May–31 August 2020; IEEE: New York, NY, USA, 2020; pp. 4739–4744. [Google Scholar]
- Vinoj, P.; Jacob, S.; Menon, V.G.; Rajesh, S.; Khosravi, M.R. Brain-controlled adaptive lower limb exoskeleton for rehabilitation of post-stroke paralyzed. IEEE Access 2019, 7, 132628–132648. [Google Scholar] [CrossRef]
- Gordleeva, S.Y.; Lobov, S.A.; Grigorev, N.A.; Savosenkov, A.O.; Shamshin, M.O.; Lukoyanov, M.V.; Khoruzhko, M.A.; Kazantsev, V.B. Real-time EEG–EMG human–machine interface-based control system for a lower-limb exoskeleton. IEEE Access 2020, 8, 84070–84081. [Google Scholar]
- Wei, Q.; Li, Z.; Zhao, K.; Kang, Y.; Su, C.Y. Synergy-based control of assistive lower-limb exoskeletons by skill transfer. IEEE/ASME Trans. Mechatronics 2019, 25, 705–715. [Google Scholar]
- Xu, F.; Qiu, J.; Yuan, W.; Cheng, H. A Novel Balance Control Strategy Based on Enhanced Stability Pyramid Index and Dynamic Movement Primitives for a Lower Limb Human-Exoskeleton System. Front. Neurorobotics 2021, 15, 751642. [Google Scholar] [CrossRef]
- Ma, Y.; Wu, X.; Yang, S.X.; Dang, C.; Liu, D.X.; Wang, C.; Wang, C.; Chen, C. Online gait planning of lower-limb exoskeleton robot for paraplegic rehabilitation considering weight transfer process. IEEE Trans. Autom. Sci. Eng. 2020, 18, 414–425. [Google Scholar] [CrossRef]
- Banala, S.K.; Agrawal, S.K.; Scholz, J.P. Active Leg Exoskeleton (ALEX) for gait rehabilitation of motor-impaired patients. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; IEEE: New York, NY, USA, 2007; pp. 401–407. [Google Scholar]
- Agarwal, P.; Deshpande, A.D. Impedance and force-field control of the index finger module of a hand exoskeleton for rehabilitation. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR), Singapore, 11–14 August 2015; IEEE: New York, NY, USA, 2015; pp. 85–90. [Google Scholar]
- Chen, L.; Wang, C.; Song, X.; Wang, J.; Zhang, T.; Li, X. Dynamic trajectory adjustment of lower limb exoskeleton in swing phase based on impedance control strategy. Proc. Inst. Mech. Eng. Part J. Syst. Control. Eng. 2020, 234, 1120–1132. [Google Scholar] [CrossRef]
- Gui, K.; Liu, H.; Zhang, D. A generalized framework to achieve coordinated admittance control for multi-joint lower limb robotic exoskeleton. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July2017; IEEE: New York, NY, USA, 2017; pp. 228–233. [Google Scholar]
- Chen, C.F.; Du, Z.J.; He, L.; Shi, Y.J.; Wang, J.Q.; Xu, G.Q.; Zhang, Y.; Wu, D.M.; Dong, W. Development and hybrid control of an electrically actuated lower limb exoskeleton for motion assistance. IEEE Access 2019, 7, 169107–169122. [Google Scholar] [CrossRef]
- Ott, C.; Mukherjee, R.; Nakamura, Y. A hybrid system framework for unified impedance and admittance control. J. Intell. Robot. Syst. 2015, 78, 359–375. [Google Scholar] [CrossRef]
- Fleerkotte, B.M.; Koopman, B.; Buurke, J.H.; van Asseldonk, E.H.; van der Kooij, H.; Rietman, J.S. The effect of impedance-controlled robotic gait training on walking ability and quality in individuals with chronic incomplete spinal cord injury: An explorative study. J. Neuroeng. Rehabil. 2014, 11, 26. [Google Scholar] [CrossRef]
- Paredes, V.; Hereid, A. Dynamic Locomotion of a Lower-Limb Exoskeleton Through Virtual Constraints Based ZMP Regulation. In Dynamic Systems and Control Conference; American Society of Mechanical Engineers: New York, NY, USA, 2020; Volume 84270, p. V001T14A001. [Google Scholar]
- Harib, O.; Hereid, A.; Agrawal, A.; Gurriet, T.; Finet, S.; Boeris, G.; Duburcq, A.; Mungai, M.E.; Masselin, M.; Ames, A.D.; et al. Feedback control of an exoskeleton for paraplegics: Toward robustly stable, hands-free dynamic walking. IEEE Control. Syst. Mag. 2018, 38, 61–87. [Google Scholar] [CrossRef]
- Gurriet, T.; Finet, S.; Boeris, G.; Duburcq, A.; Hereid, A.; Harib, O.; Masselin, M.; Grizzle, J.; Ames, A.D. Towards restoring locomotion for paraplegics: Realizing dynamically stable walking on exoskeletons. In Proceedings of the 2018 IEEE International Conference on Robotics and Automation (ICRA), Brisbane, QLD, Australia, 21–25 May 2018; IEEE: New York, NY, USA, 2018; pp. 2804–2811. [Google Scholar]
- Agrawal, A.; Harib, O.; Hereid, A.; Finet, S.; Masselin, M.; Praly, L.; Ames, A.D.; Sreenath, K.; Grizzle, J.W. First steps towards translating HZD control of bipedal robots to decentralized control of exoskeletons. IEEE Access 2017, 5, 9919–9934. [Google Scholar] [CrossRef]
- Karacan, K.; Meyer, J.T.; Bozma, H.I.; Gassert, R.; Samur, E. An environment recognition and parameterization system for shared-control of a powered lower-limb exoskeleton. In Proceedings of the 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), New York, NY, USA, 29 November–1 December 2020; IEEE: New York, NY, USA, 2020; pp. 623–628. [Google Scholar]
- Bao, W.; Villarreal, D.; Chiao, J.C. Vision-based autonomous walking in a lower-limb powered exoskeleton. In Proceedings of the 2020 IEEE 20th International Conference on Bioinformatics and Bioengineering (BIBE), Cincinnati, OH, USA, 26–28 October 2020; IEEE: New York, NY, USA, 2020; pp. 830–834. [Google Scholar]
- Marchal-Crespo, L.; Reinkensmeyer, D.J. Review of control strategies for robotic movement training after neurologic injury. J. Neuroeng. Rehabil. 2009, 6, 20. [Google Scholar]
- Duschau-Wicke, A.; Caprez, A.; Riener, R. Patient-cooperative control increases active participation of individuals with SCI during robot-aided gait training. J. Neuroeng. Rehabil. 2010, 7, 43. [Google Scholar] [CrossRef] [PubMed]
- Holleran, C.L.; Straube, D.D.; Kinnaird, C.R.; Leddy, A.L.; Hornby, T.G. Feasibility and potential efficacy of high-intensity stepping training in variable contexts in subacute and chronic stroke. Neurorehabilit. Neural Repair 2014, 28, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Hornby, T.G.; Holleran, C.L.; Hennessy, P.W.; Leddy, A.L.; Connolly, M.; Camardo, J.; Woodward, J.; Mahtani, G.; Lovell, L.; Roth, E.J. Variable intensive early walking poststroke (views) a randomized controlled trial. Neurorehabilit. Neural Repair 2016, 30, 440–450. [Google Scholar] [CrossRef]
- Patton, J.L.; Stoykov, M.E.; Kovic, M.; Mussa-Ivaldi, F.A. Evaluation of robotic training forces that either enhance or reduce error in chronic hemiparetic stroke survivors. Exp. Brain Res. 2006, 168, 368–383. [Google Scholar]
- Reisman, D.S.; Wityk, R.; Silver, K.; Bastian, A.J. Locomotor adaptation on a split-belt treadmill can improve walking symmetry post-stroke. Brain 2007, 130, 1861–1872. [Google Scholar] [CrossRef] [PubMed]
- Sigrist, R.; Rauter, G.; Riener, R.; Wolf, P. Augmented visual, auditory, haptic, and multimodal feedback in motor learning: A review. Psychon. Bull. Rev. 2013, 20, 21–53. [Google Scholar] [CrossRef] [PubMed]
- Malone, L.A.; Bastian, A.J. Thinking about walking: Effects of conscious correction versus distraction on locomotor adaptation. J. Neurophysiol. 2010, 103, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Choi, S. Effects of haptic guidance and disturbance on motor learning: Potential advantage of haptic disturbance. In Proceedings of the 2010 IEEE Haptics Symposium, Waltham, MA, USA, 25–26 March 2010; IEEE: New York, NY, USA, 2010; pp. 335–342. [Google Scholar]
- Kao, P.C.; Srivastava, S.; Agrawal, S.K.; Scholz, J.P. Effect of robotic performance-based error-augmentation versus error-reduction training on the gait of healthy individuals. Gait Posture 2013, 37, 113–120. [Google Scholar] [CrossRef]
- Simon, A.M.; Gillespie, R.B.; Ferris, D.P. Symmetry-based resistance as a novel means of lower limb rehabilitation. J. Biomech. 2007, 40, 1286–1292. [Google Scholar] [CrossRef]
- Simon, A.M.; Ferris, D.P. Lower limb force production and bilateral force asymmetries are based on sense of effort. Exp. Brain Res. 2008, 187, 129–138. [Google Scholar] [CrossRef]
- Kilicarslan, A.; Prasad, S.; Grossman, R.G.; Contreras-Vidal, J.L. High accuracy decoding of user intentions using EEG to control a lower-body exoskeleton. In Proceedings of the 2013 35th annual international conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; IEEE: New York, NY, USA, 2013; pp. 5606–5609. [Google Scholar]
- Fleischer, C.; Hommel, G. Calibration of an EMG-Based Body Model with six Muscles to control a Leg Exoskeleton. In Proceedings of the 2007 IEEE International Conference on Robotics and Automation, Rome, Italy, 10–14 April 2007; IEEE: New York, NY, USA, 2007; pp. 2514–2519. [Google Scholar]
- Liu, M.; Zhang, F.; Huang, H.H. An adaptive classification strategy for reliable locomotion mode recognition. Sensors 2017, 17, 2020. [Google Scholar] [CrossRef]
- Huang, H.; Zhang, F.; Hargrove, L.J.; Dou, Z.; Rogers, D.R.; Englehart, K.B. Continuous locomotion-mode identification for prosthetic legs based on neuromuscular–mechanical fusion. IEEE Trans. Biomed. Eng. 2011, 58, 2867–2875. [Google Scholar] [CrossRef]
- Kyeong, S.; Shin, W.; Yang, M.; Heo, U.; Feng, J.r.; Kim, J. Recognition of walking environments and gait period by surface electromyography. Front. Inf. Technol. Electron. Eng. 2019, 20, 342–352. [Google Scholar] [CrossRef]
- Kundu, A.S.; Mazumder, O.; Lenka, P.K.; Bhaumik, S. Hand gesture recognition based omnidirectional wheelchair control using IMU and EMG sensors. J. Intell. Robot. Syst. 2018, 91, 529–541. [Google Scholar] [CrossRef]
- Liu, D.; Chen, W.; Pei, Z.; Wang, J. A brain-controlled lower-limb exoskeleton for human gait training. Rev. Sci. Instruments 2017, 88, 104302. [Google Scholar] [CrossRef]
- Choi, J.; Kim, K.T.; Jeong, J.H.; Kim, L.; Lee, S.J.; Kim, H. Developing a motor imagery-based real-time asynchronous hybrid BCI controller for a lower-limb exoskeleton. Sensors 2020, 20, 7309. [Google Scholar] [CrossRef] [PubMed]
- Schrade, S.O.; Nager, Y.; Wu, A.R.; Gassert, R.; Ijspeert, A. Bio-inspired control of joint torque and knee stiffness in a robotic lower limb exoskeleton using a central pattern generator. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; IEEE: New York, NY, USA, 2017; pp. 1387–1394. [Google Scholar]
- Liu, J.; Zhang, Y.; Wang, J.; Chen, W. Adaptive sliding mode control for a lower-limb exoskeleton rehabilitation robot. In Proceedings of the 2018 13th IEEE Conference on Industrial Electronics and Applications (ICIEA), Wuhan, China, 31 May–2 June 2018; IEEE: New York, NY, USA, 2018; pp. 1481–1486. [Google Scholar]
- Shushtari, M.; Nasiri, R.; Arami, A. Online reference trajectory adaptation: A personalized control strategy for lower limb exoskeletons. IEEE Robot. Autom. Lett. 2021, 7, 128–134. [Google Scholar] [CrossRef]
- Jatsun, S.; Savin, S.; Yatsun, A. Motion control algorithm for a lower limb exoskeleton based on iterative LQR and ZMP method for trajectory generation. In New Trends in Medical and Service Robots: Design, Analysis and Control; Springer: Berlin/Heidelberg, Germany, 2016; pp. 305–317. [Google Scholar]
- Aole, S.; Elamvazuthi, I.; Waghmare, L.; Patre, B.; Meriaudeau, F. Improved active disturbance rejection control for trajectory tracking control of lower limb robotic rehabilitation exoskeleton. Sensors 2020, 20, 3681. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Tian, Y.; Han, S.; Wang, X. ZMP theory-based gait planning and model-free trajectory tracking control of lower limb carrying exoskeleton system. Stud. Inform. Control. 2017, 26, 161–170. [Google Scholar] [CrossRef]
- Sun, W.; Lin, J.W.; Su, S.F.; Wang, N.; Er, M.J. Reduced adaptive fuzzy decoupling control for lower limb exoskeleton. IEEE Trans. Cybern. 2020, 51, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Crespo, R.; Torricelli, D.; Huegel, J.C.; Gordillo, J.L.; Pons, J.L.; Soto, R. An adaptable human-like gait pattern generator derived from a lower limb exoskeleton. Front. Robot. AI 2019, 6, 36. [Google Scholar] [CrossRef]
- Seo, K.; Kim, K.; Park, Y.J.; Cho, J.K.; Lee, J.; Choi, B.; Lim, B.; Lee, Y.; Shim, Y. Adaptive oscillator-based control for active lower-limb exoskeleton and its metabolic impact. In Proceedings of the 2018 IEEE International Conference on Robotics and Automation (ICRA), Brisbane, QLD, Australia, 21–25 May 2018; IEEE: New York, NY, USA, 2018; pp. 6752–6758. [Google Scholar]
- Chung, Y.; Kim, J.H.; Cha, Y.; Hwang, S. Therapeutic effect of functional electrical stimulation-triggered gait training corresponding gait cycle for stroke. Gait Posture 2014, 40, 471–475. [Google Scholar] [CrossRef]
- Nightingale, E.; Raymond, J.; Middleton, J.; Crosbie, J.; Davis, G. Benefits of FES gait in a spinal cord injured population. Spinal Cord 2007, 45, 646–657. [Google Scholar] [CrossRef]
- Granat, M.; Ferguson, A.; Andrews, B.; Delargy, M. The role of functional electrical stimulation in the rehabilitation of patients with incomplete spinal cord injury-observed benefits during gait studies. Spinal Cord 1993, 31, 207–215. [Google Scholar] [CrossRef]
- Krause, P.; Szecsi, J.; Straube, A. Changes in spastic muscle tone increase in patients with spinal cord injury using functional electrical stimulation and passive leg movements. Clin. Rehabil. 2008, 22, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Del-Ama, A.J.; Gil-Agudo, Á.; Pons, J.L.; Moreno, J.C. Hybrid FES-robot cooperative control of ambulatory gait rehabilitation exoskeleton. J. Neuroeng. Rehabil. 2014, 11, 27. [Google Scholar] [CrossRef]
- Ha, K.H.; Quintero, H.A.; Farris, R.J.; Goldfarb, M. Enhancing stance phase propulsion during level walking by combining FES with a powered exoskeleton for persons with paraplegia. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; IEEE: New York, NY, USA, 2012; pp. 344–347. [Google Scholar]
- Stewart, A.; Pretty, C.; Chen, X. A portable assist-as-need upper-extremity hybrid exoskeleton for FES-induced muscle fatigue reduction in stroke rehabilitation. BMC Biomed. Eng. 2019, 1, 30. [Google Scholar] [CrossRef] [PubMed]
- Ha, K.H.; Murray, S.A.; Goldfarb, M. An approach for the cooperative control of FES with a powered exoskeleton during level walking for persons with paraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 24, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Alouane, M.A.; Huo, W.; Rifai, H.; Amirat, Y.; Mohammed, S. Hybrid fes-exoskeleton controller to assist sit-to-stand movement. IFAC-Pap. 2019, 51, 296–301. [Google Scholar] [CrossRef]
- Quintero, H.A.; Farris, R.J.; Ha, K.; Goldfarb, M. Preliminary assessment of the efficacy of supplementing knee extension capability in a lower limb exoskeleton with FES. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; IEEE: New York, NY, USA, 2012; pp. 3360–3363. [Google Scholar]
- Alibeji, N.A.; Molazadeh, V.; Moore-Clingenpeel, F.; Sharma, N. A muscle synergy-inspired control design to coordinate functional electrical stimulation and a powered exoskeleton: Artificial generation of synergies to reduce input dimensionality. IEEE Control. Syst. Mag. 2018, 38, 35–60. [Google Scholar] [CrossRef]
- Shin, D.; Lee, S.; Hwang, S. Locomotion Mode Recognition Algorithm Based on Gaussian Mixture Model Using IMU Sensors. Sensors 2021, 21, 2785. [Google Scholar] [CrossRef]
- Lou, Y.; Wang, R.; Mai, J.; Wang, N.; Wang, Q. IMU-Based Gait Phase Recognition for Stroke Survivors. Robotica 2019, 37, 2195–2208. [Google Scholar] [CrossRef]
- Ding, S.; Ouyang, X.; Liu, T.; Li, Z.; Yang, H. Gait event detection of a lower extremity exoskeleton robot by an intelligent IMU. IEEE Sensors J. 2018, 18, 9728–9735. [Google Scholar] [CrossRef]
- Sánchez Manchola, M.D.; Bernal, M.J.P.; Munera, M.; Cifuentes, C.A. Gait phase detection for lower-limb exoskeletons using foot motion data from a single inertial measurement unit in hemiparetic individuals. Sensors 2019, 19, 2988. [Google Scholar] [CrossRef]
- Li, M.; Deng, J.; Zha, F.; Qiu, S.; Wang, X.; Chen, F. Towards online estimation of human joint muscular torque with a lower limb exoskeleton robot. Appl. Sci. 2018, 8, 1610. [Google Scholar] [CrossRef]
- Hsiao, T.; Yip, K.; Chiu, Y.J. Estimation of Ground Reaction Forces Based on Knee Joint Acceleration of Lower-Limb Exoskeletons. In Proceedings of the 2020 International Automatic Control Conference (CACS), Hsinchu, Taiwan, 4–7 November 2020; IEEE: New York, NY, USA, 2020; pp. 1–6. [Google Scholar]
- Kazerooni, H.; Racine, J.L.; Huang, L.; Steger, R. On the control of the berkeley lower extremity exoskeleton (BLEEX). In Proceedings of the 2005 IEEE International Conference on Robotics and Automation, Barcelona, Spain, 18–22 April 2005; IEEE: New York, NY, USA, 2005; pp. 4353–4360. [Google Scholar]
- Şahin, Y.; Botsalı, F.M.; Kalyoncu, M.; Tinkir, M.; Önen, Ü.; Yılmaz, N.; Baykan, Ö.K.; Çakan, A. Force feedback control of lower extremity exoskeleton assisting of load carrying human. Appl. Mech. Mater. 2014, 598, 546–550. [Google Scholar]
- He, Y.; Eguren, D.; Azorín, J.M.; Grossman, R.G.; Luu, T.P.; Contreras-Vidal, J.L. Brain–machine interfaces for controlling lower-limb powered robotic systems. J. Neural Eng. 2018, 15, 021004. [Google Scholar] [CrossRef] [PubMed]
- Al-Quraishi, M.S.; Elamvazuthi, I.; Daud, S.A.; Parasuraman, S.; Borboni, A. EEG-based control for upper and lower limb exoskeletons and prostheses: A systematic review. Sensors 2018, 18, 3342. [Google Scholar] [CrossRef]
- Donati, A.R.; Shokur, S.; Morya, E.; Campos, D.S.; Moioli, R.C.; Gitti, C.M.; Augusto, P.B.; Tripodi, S.; Pires, C.G.; Pereira, G.A.; et al. Long-term training with a brain-machine interface-based gait protocol induces partial neurological recovery in paraplegic patients. Sci. Rep. 2016, 6, 30383. [Google Scholar] [CrossRef]
- Lee, K.; Liu, D.; Perroud, L.; Chavarriaga, R.; Millán, J.d.R. A brain-controlled exoskeleton with cascaded event-related desynchronization classifiers. Robot. Auton. Syst. 2017, 90, 15–23. [Google Scholar] [CrossRef]
- López-Larraz, E.; Trincado-Alonso, F.; Rajasekaran, V.; Pérez-Nombela, S.; Del-Ama, A.J.; Aranda, J.; Minguez, J.; Gil-Agudo, A.; Montesano, L. Control of an ambulatory exoskeleton with a brain–machine interface for spinal cord injury gait rehabilitation. Front. Neurosci. 2016, 10, 359. [Google Scholar] [CrossRef]
- Formaggio, E.; Storti, S.F.; Boscolo Galazzo, I.; Gandolfi, M.; Geroin, C.; Smania, N.; Spezia, L.; Waldner, A.; Fiaschi, A.; Manganotti, P. Modulation of event-related desynchronization in robot-assisted hand performance: Brain oscillatory changes in active, passive and imagined movements. J. Neuroeng. Rehabil. 2013, 10, 24. [Google Scholar] [CrossRef]
- Kwak, N.S.; Müller, K.R.; Lee, S.W. A lower limb exoskeleton control system based on steady state visual evoked potentials. J. Neural Eng. 2015, 12, 056009. [Google Scholar] [CrossRef]
- Zhang, Y.; Prasad, S.; Kilicarslan, A.; Contreras-Vidal, J.L. Multiple kernel based region importance learning for neural classification of gait states from EEG signals. Front. Neurosci. 2017, 11, 170. [Google Scholar] [CrossRef]
- Selinger, J.C.; Donelan, J.M. Myoelectric control for adaptable biomechanical energy harvesting. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 24, 364–373. [Google Scholar] [CrossRef]
- Kiguchi, K.; Hayashi, Y. An EMG-based control for an upper-limb power-assist exoskeleton robot. IEEE Trans. Syst. Man Cybern. Part B (Cybern.) 2012, 42, 1064–1071. [Google Scholar] [CrossRef]
- Rosen, J.; Brand, M.; Fuchs, M.B.; Arcan, M. A myosignal-based powered exoskeleton system. IEEE Trans. Syst. Man-Cybern.-Part A Syst. Humans 2001, 31, 210–222. [Google Scholar] [CrossRef]
- Lloyd, D.G.; Besier, T.F. An EMG-driven musculoskeletal model to estimate muscle forces and knee joint moments in vivo. J. Biomech. 2003, 36, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Veronica, J.; Parasuraman, S.; Khan, M.A.; DSingh, K.J. Emg-torque correction on human upper extremity using evolutionary computation. In Proceedings of the IOP Conference Series: Materials Science and Engineering, Bali, Indonesia, 19–20 March 2016; IOP Publishing: Bristol, UK, 2016; Volume 149, p. 012152. [Google Scholar]
- Gui, K.; Tan, U.X.; Liu, H.; Zhang, D. Electromyography-driven progressive assist-as-needed control for lower limb exoskeleton. IEEE Trans. Med. Robot. Bionics 2020, 2, 50–58. [Google Scholar] [CrossRef]
- Chen, B.; Ma, H.; Qin, L.Y.; Guan, X.; Chan, K.M.; Law, S.W.; Qin, L.; Liao, W.H. Design of a lower extremity exoskeleton for motion assistance in paralyzed individuals. In Proceedings of the 2015 IEEE International Conference on Robotics and Biomimetics (ROBIO), Zhuhai, China, 6–9 December 2015; IEEE: New York, NY, USA, 2015; pp. 144–149. [Google Scholar]
- Lancini, M.; Serpelloni, M.; Pasinetti, S.; Guanziroli, E. Healthcare sensor system exploiting instrumented crutches for force measurement during assisted gait of exoskeleton users. IEEE Sens. J. 2016, 16, 8228–8237. [Google Scholar] [CrossRef]
- Yang, W.; Zhang, J.; Zhang, S.; Yang, C. Lower Limb Exoskeleton Gait Planning Based on Crutch and Human-Machine Foot Combined Center of Pressure. Sensors 2020, 20, 7216. [Google Scholar] [CrossRef]









| Perspective, Criteria | GAR | BAM | DEM | LOM | SEC |
|---|---|---|---|---|---|
| Stability | ✓ | ✓ | |||
| Efficiency | ✓ | ||||
| Kinematics | ✓ | ✓ | ✓ | ||
| Dynamics | ✓ | ✓ | ✓ | ✓ | |
| Physical interaction | ✓ | ✓ | ✓ | ||
| Cognitive interaction | ✓ | ✓ | |||
| Safety | ✓ | ✓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karami, H.; Maludrottu, S.; Vassallo, C.; Laffranchi, M.; De Michieli, L. Review and Analysis of Platform-Related Performance of Rehabilitation Lower Limb Exoskeletons. Actuators 2023, 12, 406. https://doi.org/10.3390/act12110406
Karami H, Maludrottu S, Vassallo C, Laffranchi M, De Michieli L. Review and Analysis of Platform-Related Performance of Rehabilitation Lower Limb Exoskeletons. Actuators. 2023; 12(11):406. https://doi.org/10.3390/act12110406
Chicago/Turabian StyleKarami, Hossein, Stefano Maludrottu, Christian Vassallo, Matteo Laffranchi, and Lorenzo De Michieli. 2023. "Review and Analysis of Platform-Related Performance of Rehabilitation Lower Limb Exoskeletons" Actuators 12, no. 11: 406. https://doi.org/10.3390/act12110406
APA StyleKarami, H., Maludrottu, S., Vassallo, C., Laffranchi, M., & De Michieli, L. (2023). Review and Analysis of Platform-Related Performance of Rehabilitation Lower Limb Exoskeletons. Actuators, 12(11), 406. https://doi.org/10.3390/act12110406