
Three-Dimensional Imaging and Histopathological Features of Third Metacarpal/Tarsal Parasagittal Groove and Proximal Phalanx Sagittal Groove Fissures in Thoroughbred Horses
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Handling of Cadaver Limbs for Image Acquisition
- (1)
- MR images were acquired using a low-field (0.27 T) open magnet MRI system within 8 h of cadaver limb collection. After MR imaging, the limb was frozen at −20 °C for 8 h in a frame to standardise the imaging position between MRI and CT [29]. CBCT and FBCT images were then acquired from the frozen limb.
- (2)
- The cadaver limb was frozen at −20 °C for at least 8 h in the frame immediately after collection to standardise the imaging position between MRI and CT. CBCT and FBCT images were acquired from the frozen limb. After CT imaging, the frozen limb was then defrosted in the frame for at least 8 h for MR imaging.
2.2.2. Standing Low-Field MRI
- (1)
- MRI-1: Sequences selected for optimal image quality but longer acquisition time: T1-weighted (W) 3D high resolution (HR), T2*W 3D, T2W fast spin echo (FSE), short tau inversion recovery (STIR) FSE, proton density (SE) spin echo (SE), and T1W SE sequences;
- (2)
- MRI-2: Sequences selected for a shorter acquisition time: T1W gradient echo (GRE) FAST, T2*W GRE FAST, T2W fast spin echo (FSE) FAST, and STIR FSE FAST sequences, to simulate a combination more often used clinically.
- (1)
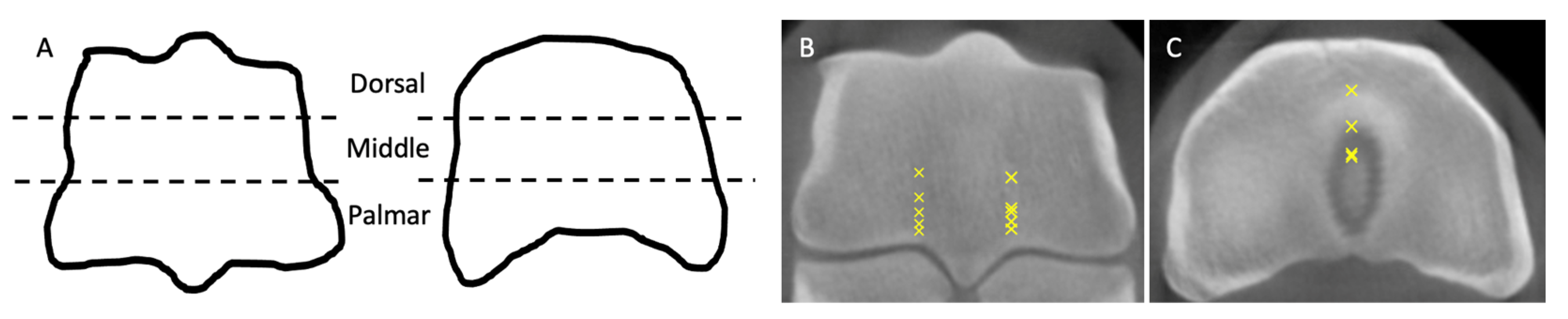
- Sagittal: aligned parallel to the longitudinal axis of the third metacarpus/tarsus and the proximal phalanx and perpendicular to the articular surface;
- (2)
- Dorsal: aligned parallel to the dorsal aspects of the third metacarpus/tarsus and the proximal phalanx;
- (3)
- Transverse: aligned perpendicular, 30° clockwise, and 30° anti-clockwise to the longitudinal axis of the third metacarpus/tarsus and proximal phalanx.
2.2.3. Standing Cone-Beam CT (CBCT)
2.2.4. Fan-Beam CT (FBCT)
2.2.5. Image Analysis
2.2.6. Macroscopic Examination
2.2.7. Histological Preparation
2.2.8. Histological Examination
2.3. Data Analysis
3. Results
3.1. Identification of Fissures between Imaging Modalities (Supplemtary Table S1)
3.2. Features of Fissures on CT Images
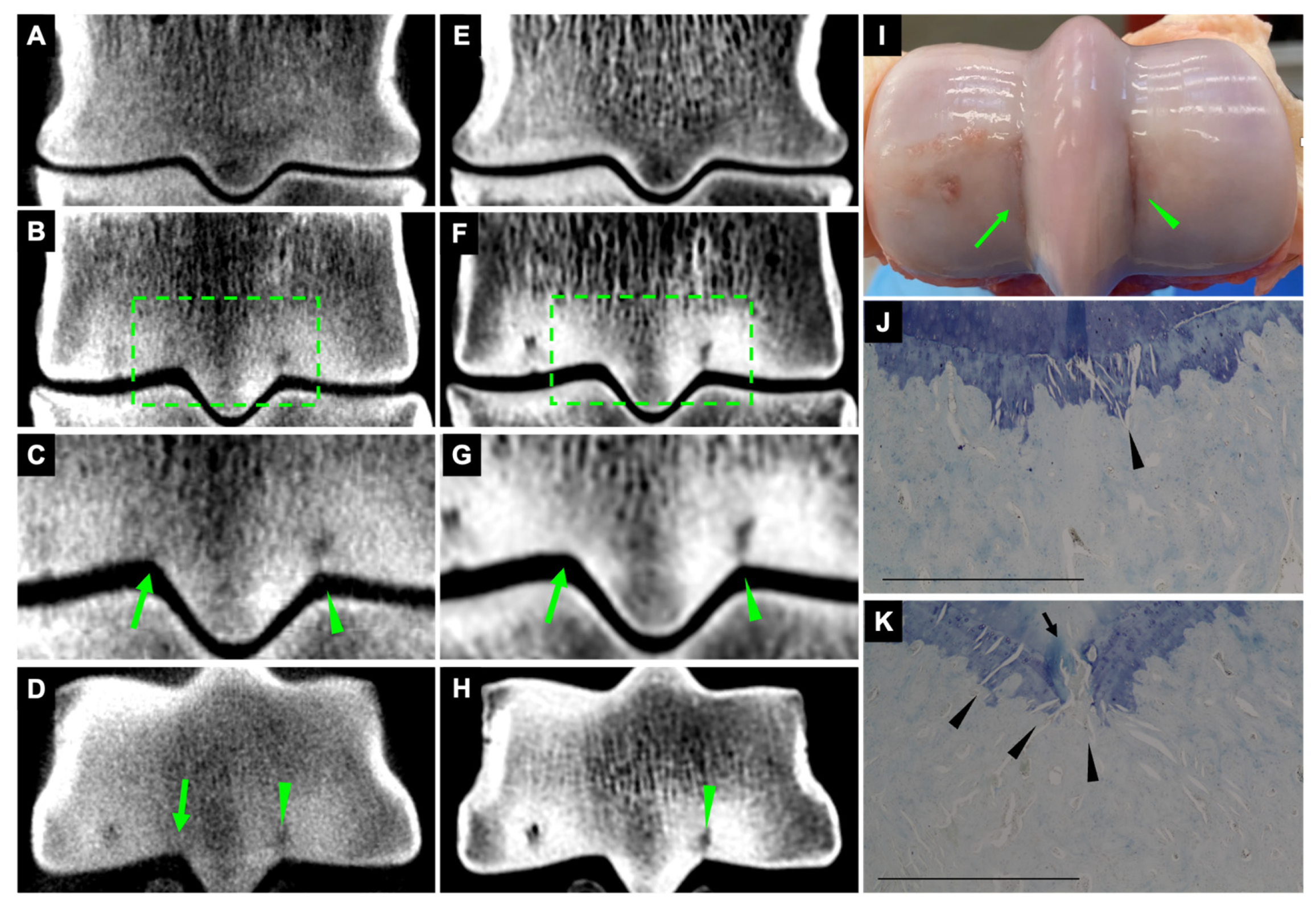
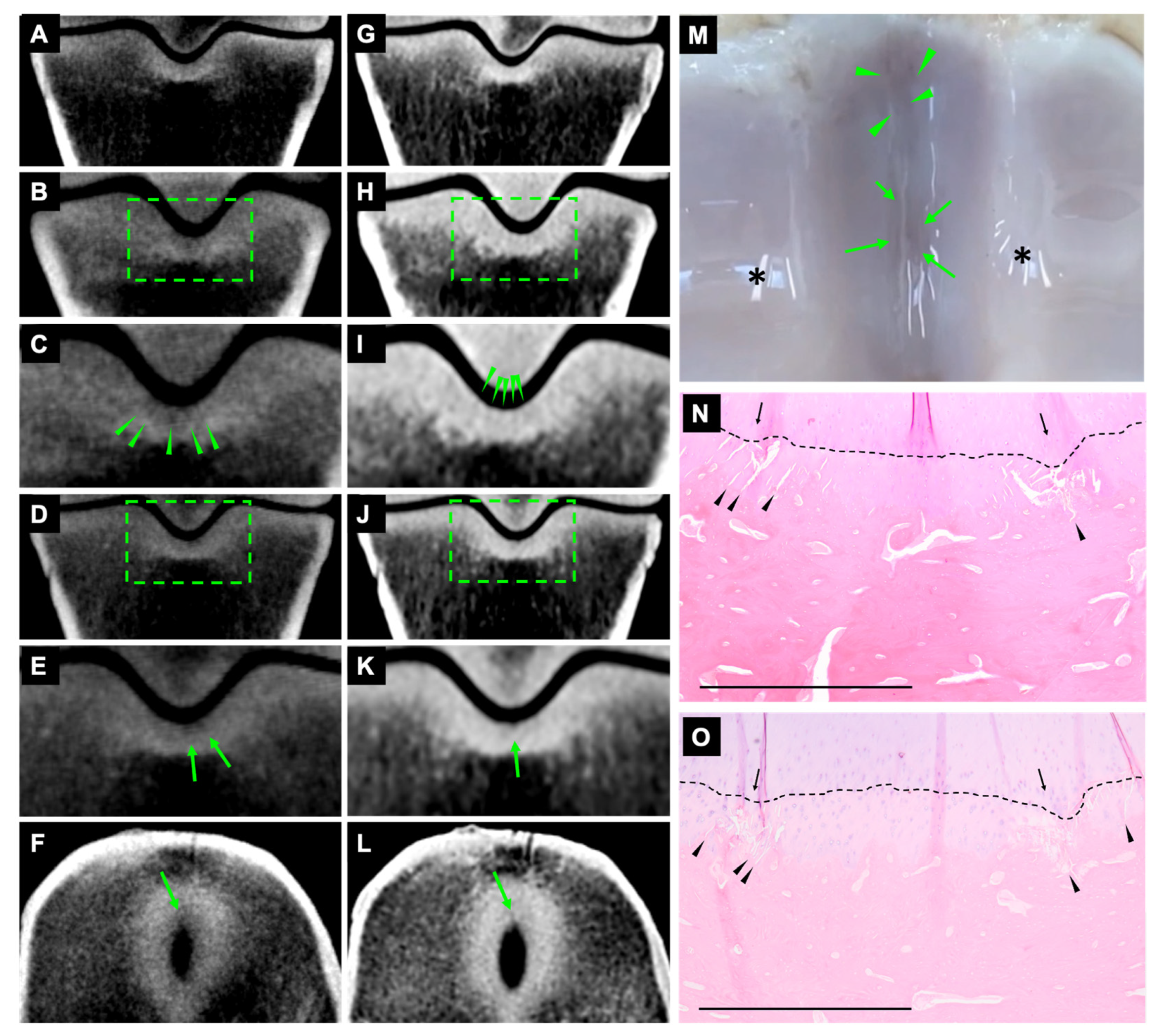
3.2.1. Hypoattenuating Linear Defects
3.2.2. Striated Hypoattenuating Lines on CBCT and FBCT
3.2.3. Subchondral Outline Irregularity on CBCT and FBCT
3.2.4. Striated Hypoattenuating Lines on CBCT and Subchondral Outline Irregularity on FBCT
3.3. Length of Fissures on CT Images
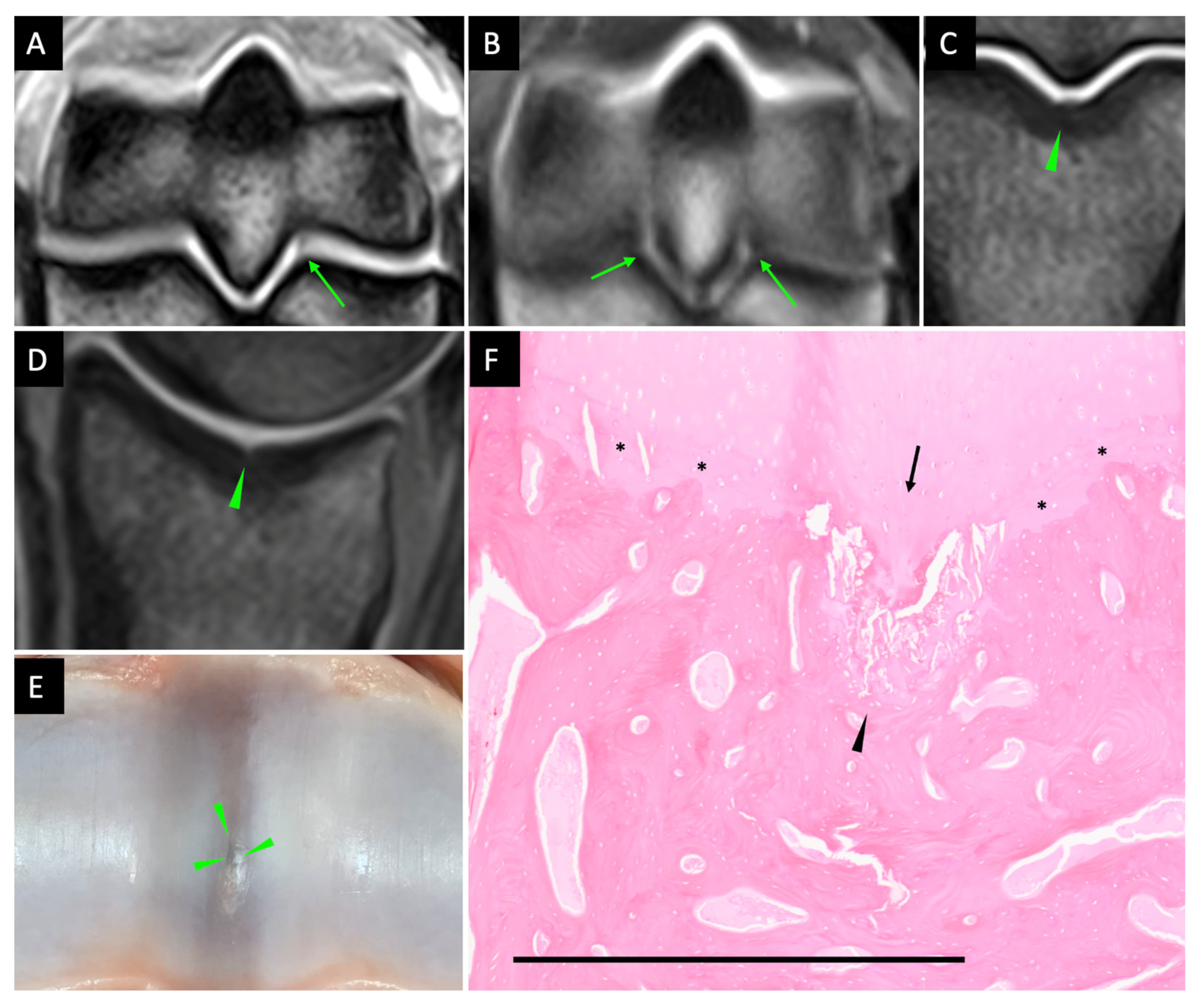
3.4. Features of Fissures on MR Images
3.5. Macroscopic Examination
3.6. Histopathology Associated with Fissures (Supplemtary Table S2)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parkin, T.; French, N.; Riggs, C.; Morgan, K.; Clegg, P.; Proudman, C.; Singer, E.; Webbon, P. Risk of fatal distal limb fractures among thoroughbreds involved in the five types of racing in the United Kingdom. Vet. Rec. 2004, 154, 493–497. [Google Scholar] [CrossRef]
- Parkin, T.D. Epidemiology of racetrack injuries in racehorses. Vet. Clin. N. Am. Equine Pract. 2008, 24, 1–19. [Google Scholar] [CrossRef]
- Riggs, C.; Whitehouse, G.; Boyde, A. Pathology of the distal condyles of the third metacarpal and third metatarsal bones of the horse. Equine Vet. J. 1999, 31, 140–148. [Google Scholar] [CrossRef]
- Muir, P.; McCarthy, J.; Radtke, C.; Markel, M.; Santschi, E.M.; Scollay, M.; Kalscheur, V. Role of endochondral ossification of articular cartilage and functional adaptation of the subchondral plate in the development of fatigue microcracking of joints. Bone 2006, 38, 342–349. [Google Scholar] [CrossRef]
- Muir, P.; Peterson, A.; Sample, S.; Scollay, M.; Markel, M.; Kalscheur, V. Exercise-induced metacarpophalangeal joint adaptation in the Thoroughbred racehorse. J. Anat. 2008, 213, 706–717. [Google Scholar] [CrossRef]
- Lacourt, M.; Gao, C.; Li, A.; Girard, C.; Beauchamp, G.; Henderson, J.; Laverty, S. Relationship between cartilage and subchondral bone lesions in repetitive impact trauma-induced equine osteoarthritis. Osteoarthr. Cartil. 2012, 20, 572–583. [Google Scholar] [CrossRef]
- Parkin, T.; Clegg, P.; French, N.; Proudman, C.; Riggs, C.; Singer, E.; Webbon, P.; Morgan, K. Catastrophic fracture of the lateral condyle of the third metacarpus/metatarsus in UK racehorses–fracture descriptions and pre-existing pathology. Vet. J. 2006, 171, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.W.; Santschi, E.M.; Zekas, L.J.; Scollay-Ward, M.C.; Markel, M.D.; Radtke, C.L.; Sample, S.J.; Keuler, N.S.; Muir, P. Comparison of radiography and computed tomography to evaluate metacarpo/metatarsophalangeal joint pathology of paired limbs of thoroughbred racehorses with severe condylar fracture. Vet. Surg. 2006, 35, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Wright, I. Are there radiologically identifiable prodromal changes in T horoughbred racehorses with parasagittal fractures of the proximal phalanx? Equine Vet. J. 2014, 46, 88–91. [Google Scholar] [CrossRef]
- Ramzan, P.; Powell, S. Clinical and imaging features of suspected prodromal fracture of the proximal phalanx in three Thoroughbred racehorses. Equine Vet. J. 2010, 42, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Powell, S. Low-field standing magnetic resonance imaging findings of the metacarpo/metatarsophalangeal joint of racing Thoroughbreds with lameness localised to the region: A retrospective study of 131 horses. Equine Vet. J. 2012, 44, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Tranquille, C.; Parkin, T.; Murray, R. Magnetic resonance imaging-detected adaptation and pathology in the distal condyles of the third metacarpus, associated with lateral condylar fracture in Thoroughbred racehorses. Equine Vet. J. 2012, 44, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Tranquille, C.; Murray, R.; Parkin, T. Can we use subchondral bone thickness on high-field magnetic resonance images to identify Thoroughbred racehorses at risk of catastrophic lateral condylar fracture? Equine Vet. J. 2017, 49, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Dubois, M.-S.; Morello, S.; Rayment, K.; Markel, M.D.; Vanderby Jr, R.; Kalscheur, V.L.; Hao, Z.; McCabe, R.P.; Marquis, P.; Muir, P. Computed tomographic imaging of subchondral fatigue cracks in the distal end of the third metacarpal bone in the thoroughbred racehorse can predict crack micromotion in an ex-vivo model. PLoS ONE 2014, 9, e101230. [Google Scholar] [CrossRef]
- Crijns, C.; Martens, A.; Bergman, H.J.; van der Veen, H.; Duchateau, L.; van Bree, H.; Gielen, I. Intramodality and intermodality agreement in radiography and computed tomography of equine distal limb fractures. Equine Vet. J. 2014, 46, 92–96. [Google Scholar] [CrossRef]
- Brünisholz, H.P.; Hagen, R.; Fürst, A.E.; Kuemmerle, J.M. Radiographic and computed tomographic configuration of incomplete proximal fractures of the proximal phalanx in horses not used for racing. Vet. Surg. 2015, 44, 809–815. [Google Scholar] [CrossRef]
- Olive, J.; D’Anjou, M.A.; Alexander, K.; Laverty, S.; Theoret, C. Comparison of magnetic resonance imaging, computed tomography, and radiography for assessment of noncartilaginous changes in equine metacarpophalangeal osteoarthritis. Vet. Radiol. Ultrasound 2010, 51, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Dyson, S.; Nagy, A.; Murray, R. Clinical and diagnostic imaging findings in horses with subchondral bone trauma of the sagittal groove of the proximal phalanx. Vet. Radiol. Ultrasound 2011, 52, 596–604. [Google Scholar] [CrossRef]
- Johnston, G.C.; Ahern, B.J.; Palmieri, C.; Young, A.C. Imaging and gross pathological appearance of changes in the parasagittal grooves of Thoroughbred racehorses. Animals 2021, 11, 3366. [Google Scholar] [CrossRef]
- Cianci, J.M.; Wulster, K.B.; Richardson, D.W.; Stefanovski, D.; Ortved, K.F. Computed tomographic assessment of fracture characteristics and subchondral bone injury in Thoroughbred racehorses with lateral condylar fractures and their relationship to outcome. Vet. Surg. 2022, 51, 426–437. [Google Scholar] [CrossRef]
- Zubrod, C.J.; Schneider, R.K.; Tucker, R.L.; Gavin, P.R.; Ragle, C.A.; Farnsworth, K.D. Use of magnetic resonance imaging for identifying subchondral bone damage in horses: 11 cases (1999–2003). J. Am. Vet. Med. Assoc. 2004, 224, 411–418. [Google Scholar] [CrossRef]
- Curtiss, A.L.; Ortved, K.F.; Dallap-Schaer, B.; Gouzeev, S.; Stefanovski, D.; Richardson, D.W.; Wulster, K.B. Validation of standing cone beam computed tomography for diagnosing subchondral fetlock pathology in the Thoroughbred racehorse. Equine Vet. J. 2021, 53, 510–523. [Google Scholar] [CrossRef] [PubMed]
- Mageed, M. Standing computed tomography of the equine limb using a multi-slice helical scanner: Technique and feasibility study. Equine Vet. Educ. 2022, 34, 77–83. [Google Scholar] [CrossRef]
- Brounts, S.H.; Lund, J.R.; Whitton, R.C.; Ergun, D.L.; Muir, P. Use of a novel helical fan beam imaging system for computed tomography of the distal limb in sedated standing horses: 167 cases (2019–2020). J. Am. Vet. Med. Assoc. 2022, 260, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Mathee, N.; Robert, M.; Higgerty, S.M.; Fosgate, G.T.; Rogers, A.L.; d’Ablon, X.; Carstens, A. Computed tomographic evaluation of the distal limb in the standing sedated horse: Technique, imaging diagnoses, feasibility, and artifacts. Vet. Radiol. Ultrasound 2023, 64, 243–252. [Google Scholar] [CrossRef]
- McIlwraith, C.; Frisbie, D.; Kawcak, C.; Fuller, C.; Hurtig, M.; Cruz, A. The OARSI histopathology initiative–recommendations for histological assessments of osteoarthritis in the horse. Osteoarthr. Cartil. 2010, 18, S93–S105. [Google Scholar] [CrossRef]
- Engiles, J.B.; Stewart, H.; Janes, J.; Kennedy, L.A. A diagnostic pathologist’s guide to carpal disease in racehorses. J. Vet. Diagn. Investig. 2017, 29, 414–430. [Google Scholar] [CrossRef]
- Pinilla, M.; Tranquille, C.; Blunden, A.; Chang, Y.; Parkin, T.; Murray, R. Histological features of the distal third metacarpal bone in thoroughbred racehorses, with and without lateral condylar fractures. J. Comp. Pathol. 2017, 157, 1–10. [Google Scholar] [CrossRef]
- Lin, S.T.; Peter, V.G.; Schiavo, S.; Pokora, R.; Patrick, H.; Bolas, N.; Foote, A.K.; Sargan, D.R.; Murray, R.C. Identification of Heterotopic Mineralization and Adjacent Pathology in the Equine Fetlock Region by Low-Field Magnetic Resonance Imaging, Cone-Beam and Fan-Beam Computed Tomography. J. Equine Vet. Sci. 2023, 126, 104252. [Google Scholar] [CrossRef]
- Lin, S.T.; Bolas, N.M.; Sargan, D.R.; Restif, O.; Peter, V.G.; Pokora, R.; Patrick, H.; Foote, A.K.; Murray, R.C. Comparison of cone-beam and fan-beam computed tomography and low-field magnetic resonance imaging for detection of proximal phalanx dorsoproximal osteochondral defects. Equine Vet. J. 2023. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Travlos, G.S. Histopathology of bone marrow. Toxicol. Pathol. 2006, 34, 566–598. [Google Scholar] [CrossRef] [PubMed]
- Miracle, A.; Mukherji, S. Conebeam CT of the head and neck, part 1: Physical principles. Am. J. Neuroradiol. 2009, 30, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Honda, E.; Tetsumura, A.; Kurabayashi, T. A comparative study for spatial resolution and subjective image characteristics of a multi-slice CT and a cone-beam CT for dental use. Eur. J. Radiol. 2011, 77, 397–402. [Google Scholar] [CrossRef]
- Scarfe, W.C.; Farman, A.G. What is cone-beam CT and how does it work? Dent. Clin. N. Am. 2008, 52, 707–730. [Google Scholar] [CrossRef]
- Ballrick, J.W.; Palomo, J.M.; Ruch, E.; Amberman, B.D.; Hans, M.G. Image distortion and spatial resolution of a commercially available cone-beam computed tomography machine. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 573–582. [Google Scholar] [CrossRef]
- Goldman, L.W. Principles of CT: Radiation dose and image quality. J. Nucl. Med. Technol. 2007, 35, 213–225. [Google Scholar] [CrossRef]
- Brüllmann, D.; Schulze, R. Spatial resolution in CBCT machines for dental/maxillofacial applications—What do we know today? Dentomaxillofac. Radiol. 2015, 44, 20140204. [Google Scholar] [CrossRef]
- Bolas, N. Basic MRI principles. In Equine MRI; John Wiley & Sons: New York, NY, USA, 2010; pp. 1–37. [Google Scholar]
- Murray, R.C. Equine MRI; John Wiley & Sons: New York, NY, USA, 2010. [Google Scholar]
- Seref-Ferlengez, Z.; Kennedy, O.D.; Schaffler, M.B. Bone microdamage, remodeling and bone fragility: How much damage is too much damage? BoneKey Rep. 2015, 4, 644. [Google Scholar] [CrossRef]
- Augat, P.; Schorlemmer, S. The role of cortical bone and its microstructure in bone strength. Age Ageing 2006, 35, ii27–ii31. [Google Scholar] [CrossRef]
- Donell, S. Subchondral bone remodelling in osteoarthritis. EFORT Open Rev. 2019, 4, 221. [Google Scholar] [CrossRef] [PubMed]
- Herman, B.C.; Cardoso, L.; Majeska, R.J.; Jepsen, K.J.; Schaffler, M.B. Activation of bone remodeling after fatigue: Differential response to linear microcracks and diffuse damage. Bone 2010, 47, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.M.; Hurtig, M.B. Multiple pathways to osteoarthritis and articular fractures: Is subchondral bone the culprit? Vet. Clin. N. Am. Equine Pract. 2008, 24, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Whitton, R.; Ayodele, B.; Hitchens, P.; Mackie, E. Subchondral bone microdamage accumulation in distal metacarpus of Thoroughbred racehorses. Equine Vet. J. 2018, 50, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Wu, X.; Trevisan Franca De Lima, L.; Stehbens, S.; Punyadeera, C.; Webb, R.; Hamilton, B.; Ayyapann, V.; McLauchlan, C.; Crawford, R. The deterioration of calcified cartilage integrity reflects the severity of osteoarthritis—A structural, molecular, and biochemical analysis. FASEB J. 2022, 36, e22142. [Google Scholar] [CrossRef] [PubMed]
- Murray, R.; Zhu, C.; Goodship, A.; Lakhani, K.; Agrawal, C.; Athanasiou, K. Exercise affects the mechanical properties and histological appearance of equine articular cartilage. J. Orthop. Res. 1999, 17, 725–731. [Google Scholar] [CrossRef]
- Lotz, M.K.; Otsuki, S.; Grogan, S.P.; Sah, R.; Terkeltaub, R.; D’Lima, D. Cartilage cell clusters. Arthritis Rheum. 2010, 62, 2206. [Google Scholar] [CrossRef]
- Firth, E.; Doube, M.; Boyde, A. Changes in mineralised tissue at the site of origin of condylar fracture are present before athletic training in Thoroughbred horses. N. Z. Vet. J. 2009, 57, 278–283. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Locations | Both CT | Type (i) | Type (ii) | Type (iii) | Type (iv) |
|---|---|---|---|---|---|
| Medial parasagittal groove—palmar/plantar | 24 | 12 | 8 | 3 | 1 |
| Medial parasagittal groove—middle | 0 | 0 | 0 | 0 | 0 |
| Medial parasagittal groove—dorsal | 0 | 0 | 0 | 0 | 0 |
| Lateral parasagittal groove—palmar/plantar | 21 | 6 | 10 | 3 | 2 |
| Lateral parasagittal groove—middle | 0 | 0 | 0 | 0 | 0 |
| Lateral parasagittal groove—dorsal | 0 | 0 | 0 | 0 | 0 |
| Sagittal groove—palmar/plantar | 6 | 1 | 1 | 2 | 2 |
| Sagittal groove—middle | 24 | 1 | 11 | 4 | 8 |
| Sagittal groove—dorsal | 17 | 1 | 4 | 7 | 5 |
| Total counts | 92 | 21 | 34 | 19 | 18 |
| Locations | MRI | A | B | C | D | E | F | G | H | I | J |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Medial parasagittal groove—palmar/plantar | 25 | 14 | 11 | 8 | 6 | 14 | 17 | 9 | 6 | 10 | 1 |
| Medial parasagittal groove—middle | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Medial parasagittal groove—dorsal | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 |
| Lateral parasagittal groove—palmar/plantar | 21 | 7 | 4 | 5 | 3 | 13 | 12 | 7 | 1 | 7 | 1 |
| Lateral parasagittal groove—middle | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Lateral parasagittal groove—dorsal | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Sagittal groove—palmar/plantar | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Sagittal groove—middle | 3 | 3 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 1 | 0 |
| Sagittal groove—dorsal | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total counts | 50 | 25 | 17 | 15 | 9 | 30 | 31 | 18 | 7 | 19 | 2 |
| Items | p Value |
|---|---|
| Hyaline cartilage | |
| Reduced staining for glycosaminoglycans in cartilage | 0.03 * |
| Cartilage surface irregularity | 0.15 |
| Cartilage fibrillation | 0.73 |
| Cartilage thickness variation | 0.03 * |
| Irregular chondrocyte distribution | <0.001 ** |
| Chondrocyte loss/necrosis | 0.01 * |
| Chondrocyte clustering | <0.001 ** |
| Calcified cartilage | |
| Tidemark incongruence | <0.001 ** |
| Calcified cartilage cleft | 0.03 * |
| Calcified cartilage depth variation | <0.001 ** |
| Vascular invasion | <0.001 ** |
| Island of hyaline cartilage in subchondral bone plate | 0.03 † |
| Subchondral/trabecular bone | |
| Sclerosis of subchondral bone plate and adjacent cancellous bone | <0.001 ** |
| Subchondral bone collapse | <0.001 ** |
| Replacement of cancellous bone with compact bone | <0.001 ** |
| Trabecular thickening with reduced marrow spaces | <0.001 ** |
| Replacement with osteon/lamellar bone | <0.001 ** |
| Microcracks in cancellous bone | <0.001 ** |
| Replacement with woven bone | <0.001 ** |
| Howship’s lacunae with/without osteoclast | 0.04 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.-T.; Foote, A.K.; Bolas, N.M.; Peter, V.G.; Pokora, R.; Patrick, H.; Sargan, D.R.; Murray, R.C. Three-Dimensional Imaging and Histopathological Features of Third Metacarpal/Tarsal Parasagittal Groove and Proximal Phalanx Sagittal Groove Fissures in Thoroughbred Horses. Animals 2023, 13, 2912. https://doi.org/10.3390/ani13182912
Lin S-T, Foote AK, Bolas NM, Peter VG, Pokora R, Patrick H, Sargan DR, Murray RC. Three-Dimensional Imaging and Histopathological Features of Third Metacarpal/Tarsal Parasagittal Groove and Proximal Phalanx Sagittal Groove Fissures in Thoroughbred Horses. Animals. 2023; 13(18):2912. https://doi.org/10.3390/ani13182912
Chicago/Turabian StyleLin, Szu-Ting, Alastair K. Foote, Nicholas M. Bolas, Vanessa G. Peter, Rachel Pokora, Hayley Patrick, David R. Sargan, and Rachel C. Murray. 2023. "Three-Dimensional Imaging and Histopathological Features of Third Metacarpal/Tarsal Parasagittal Groove and Proximal Phalanx Sagittal Groove Fissures in Thoroughbred Horses" Animals 13, no. 18: 2912. https://doi.org/10.3390/ani13182912
APA StyleLin, S.-T., Foote, A. K., Bolas, N. M., Peter, V. G., Pokora, R., Patrick, H., Sargan, D. R., & Murray, R. C. (2023). Three-Dimensional Imaging and Histopathological Features of Third Metacarpal/Tarsal Parasagittal Groove and Proximal Phalanx Sagittal Groove Fissures in Thoroughbred Horses. Animals, 13(18), 2912. https://doi.org/10.3390/ani13182912