

Accuracy of Instrument Portal Placement Using a Custom-Made 3D-Printed Aiming Device versus Free Hand Technique in Canine Elbow Arthroscopy
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
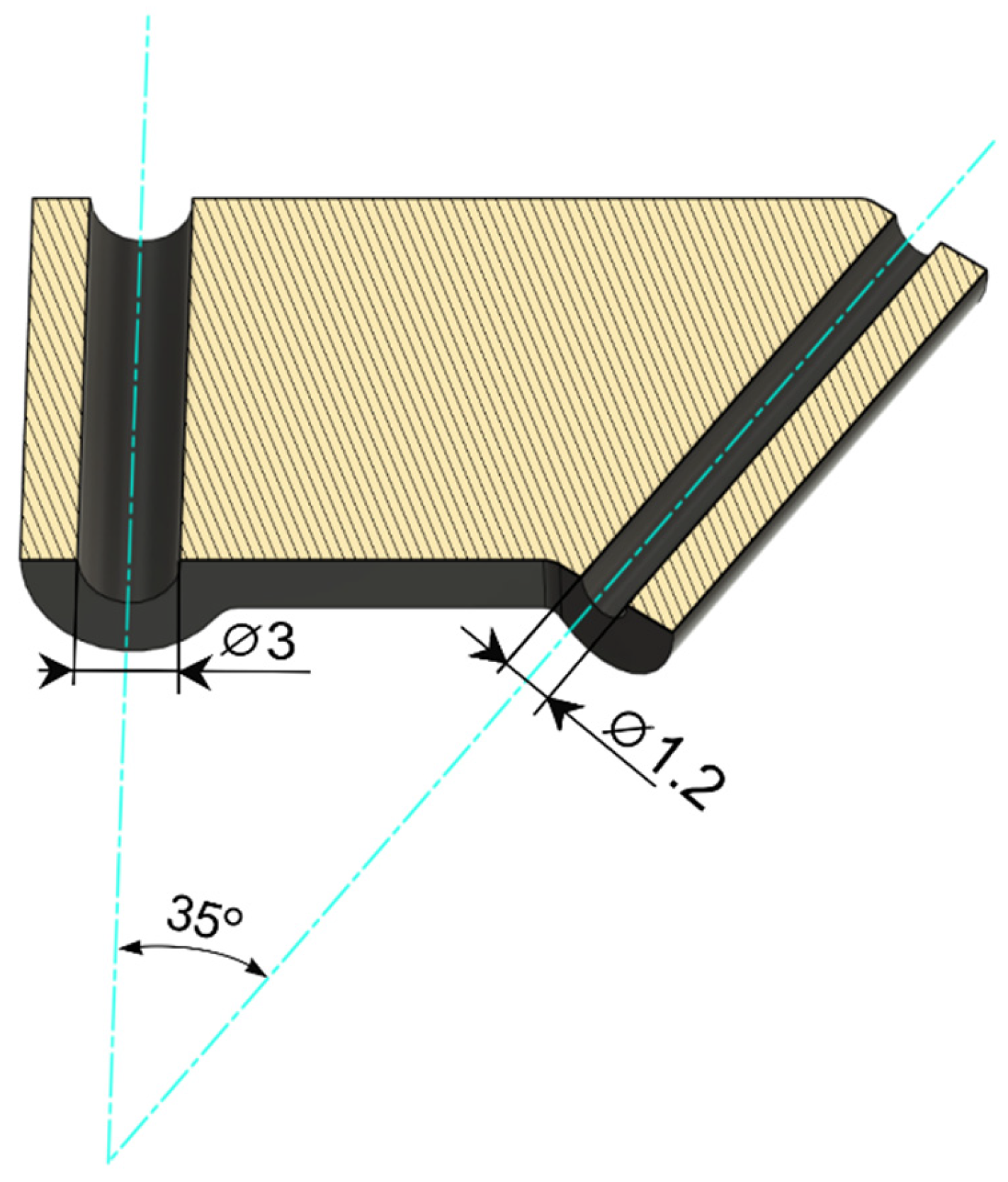
2.1. 3D Design and Printing
- -
- Converting the CAD (computer aided design) files into 3D surface models consisting of triangle meshes to create a STL (stereolithography) file.
- -
- Processing the model with software to reduce noise and artefacts, and converting the geometry file to a machine code file type recognized by the 3D printer.
2.2. Cadaver Studies
2.3. Statistical Analysis
3. Results
3.1. 3D Design and Printing
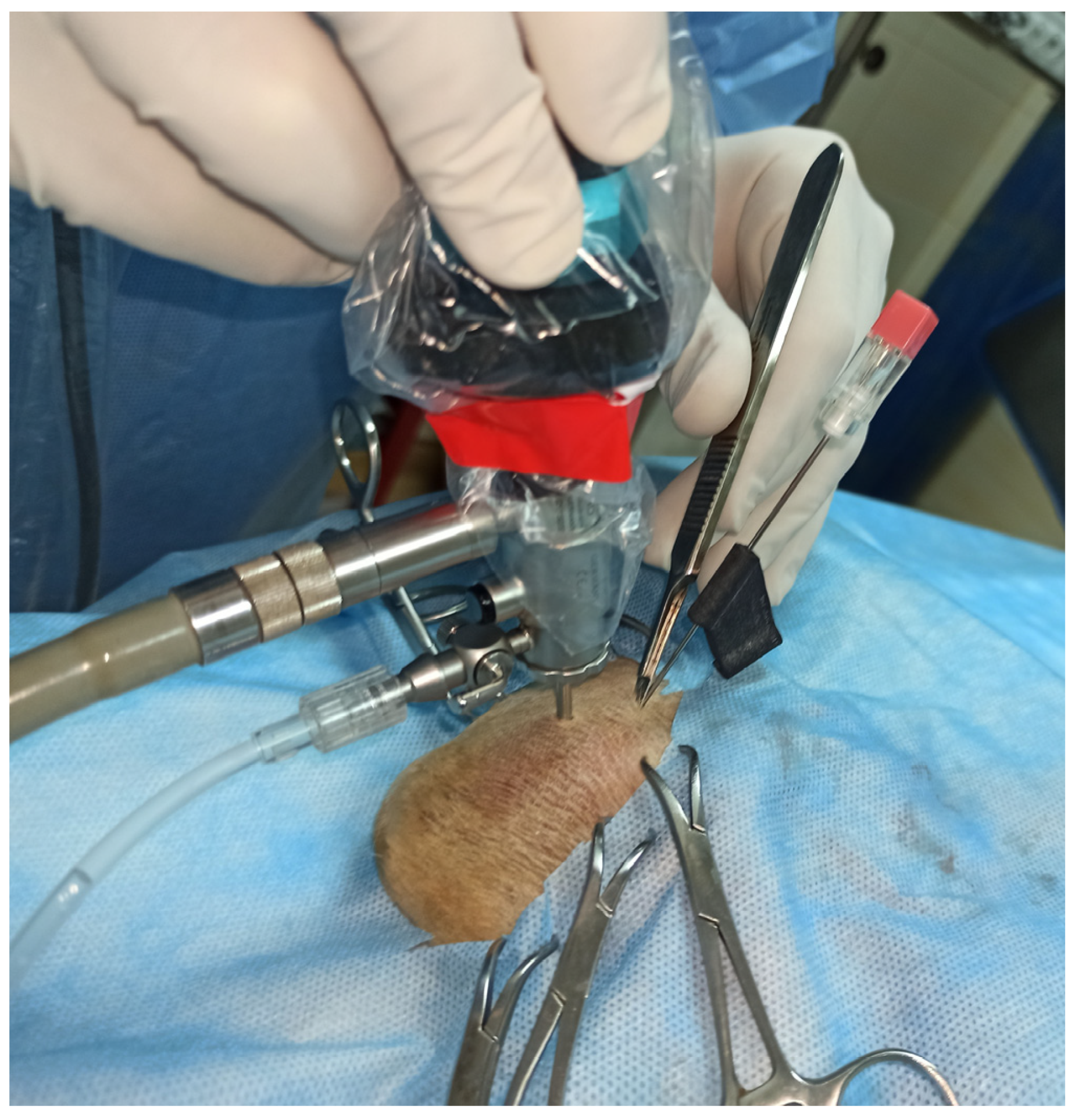
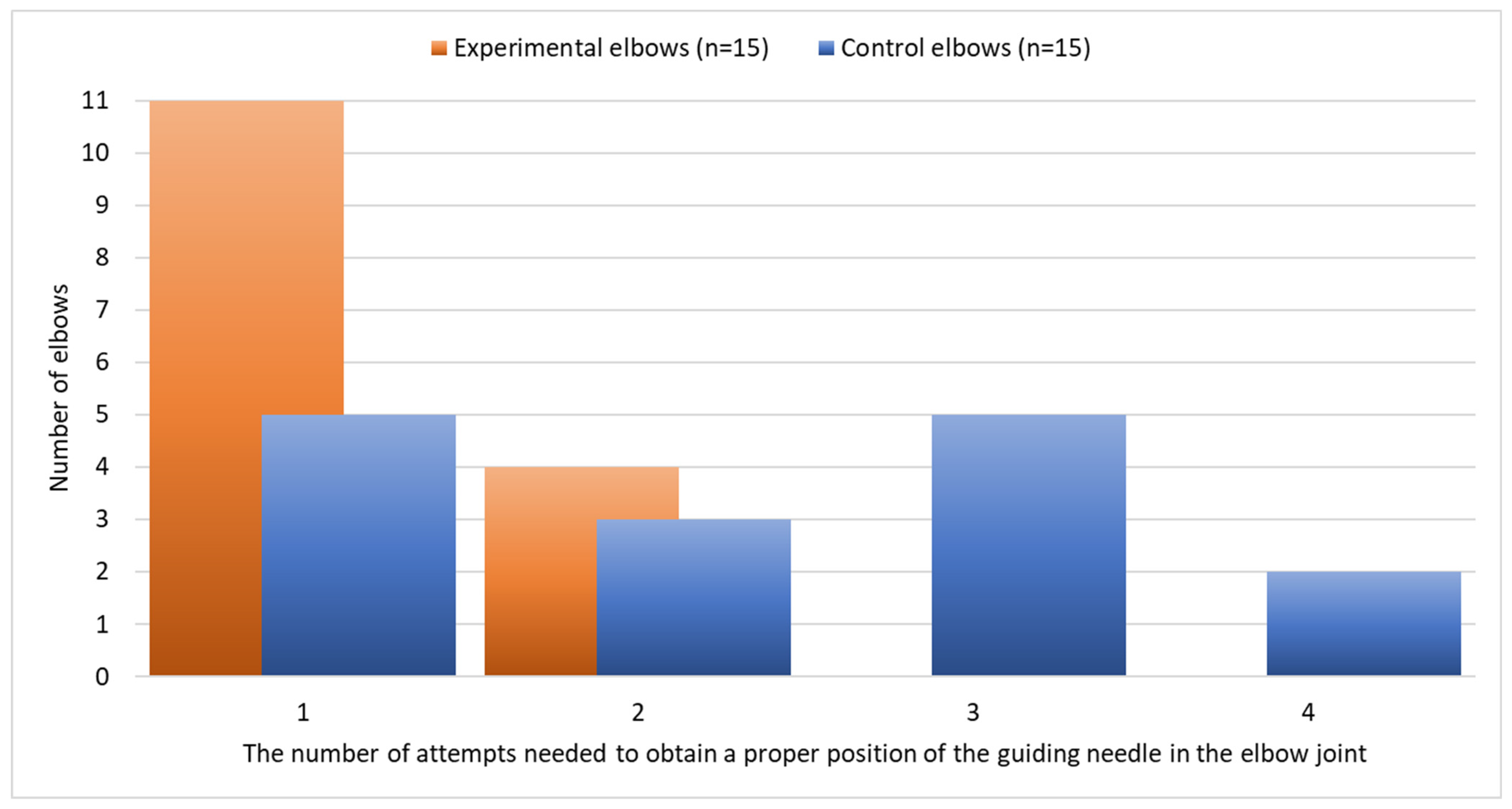
3.2. Cadaver Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Ryssen, B.; Van Bree, H.; Philip, V. Arthroscopy of the shoulder joint in the dog. J. Am. Anim. Hosp. Assoc. 1993, 29, 101–105. [Google Scholar]
- Lehman, M.; Lehman, K. Modification of the triangulation technique for arthroscopy of the canine shoulder joint using a new target device. Vet. Comp. Orthop. Traumatol. 2004, 17, 1–8. [Google Scholar] [CrossRef]
- McCarthy, T.C. Patient preparation, positioning, and operating room setup. In Veterinary Arthroscopy for the Small Animal Practitioner; John Wiley & Sons: Hoboken, NJ, USA, 2021; p. 24. [Google Scholar]
- Frede, T.; Stock, C.; Renner, C.; Budair, Z.; Abdel-Salam, Y.; Rassweiler, J. Geometry of laparoscopic suturing and knotting techniques. J. Endourol. 1999, 13, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Beale, B.S.; Hulse, D.A.; Schulz, K.S.; Whitney, W.O. Arthroscopically assisted surgery of the elbow joint. In Small Animal Arthroscopy; Saunders: Philadelphia, PA, USA, 2003; pp. 51–79. [Google Scholar]
- Abbound, W.A. Novel guide device for temporomandibular arthroscopy. Int. J. Oral Maxillofac. Surg. 2020, 49, 1217–1219. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Breinan, H.A.; Hsu, H.P.; Spector, M. Healing of defects in canine articular cartilage: Distribution of nonvascular alpha-smooth muscle actin-containing cells. Wound Repair Regen. 2000, 8, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Riener, S.; Lehman, K.; Lorinson, D.; Skalicky, M. The cranial instrument port in arthroscopy of the canine shoulder joint. A new method using a target device. Vet. Comp. Orthop. Traumatol. 2009, 22, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-R.; Adam, G.O.; Kim, S.-J. Application of patient-specific instrumentation in a dog model with antebrachial growth deformity using a 3D phantom bone model. Vet. Sci. 2022, 9, 157. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.A.; Granger, L.A.; Aulakh, K.S.; Gines, J.A. Accuracy of a drilling with a custom 3D printed guide or free-hand technique in canine experimental sacroiliac luxations. Vet. Surg. 2022, 51, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Roh, Y.; Jeong, J.; Jeon, Y.; Kim, D.; Jeong, S.; Lee, H. Pelvic endoprosthesis after hemipelvectomy using a 3D-printed osteotomy guide for infiltrative osteoma in a cat. Vet. Sci. 2022, 9, 237. [Google Scholar] [CrossRef] [PubMed]
- Frymus, J.; Trębacz, P.; Kurkowska, A.; Pawlik, M.; Barteczko, A.; Barański, M.; Galanty, M. Three-Dimensional models of liver vessels for navigation during laparotomic attenuation of intrahepatic portosystemic shunt in dogs. Animals 2023, 13, 2004. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Cadaver Characteristics | Elbow | Number of Attempts Needed to Place the Guiding Needle Properly | |||||
|---|---|---|---|---|---|---|---|---|
| Breed | Sex | Age (Years) | Body Weight (kg) | Left | Right | Custom-Made Arthroscopic Aiming Device (Experimental Elbow) | Free Hand (Control Elbow) | |
| 1 | Crossbreed | male | 5 | 31 | 1 | 1 * | 1 | 1 |
| 2 | Boerboel | male | 6 | 57 | 1 * | 2 | 1 | 2 |
| 3 | Newfoundland | male | 2 | 45 | 1 * | 4 | 1 | 4 |
| 4 | Labrador retriever | male | 2 | 29 | 3 | 1 * | 1 | 3 |
| 5 | Crossbreed | male | 2 | 19 | 1 | 1 * | 1 | 1 |
| 6 | German Shepherd | male | 3 | 35 | 2 * | 1 | 2 | 1 |
| 7 | Chow-chow | female | 1 | 17 | 1 * | 3 | 1 | 3 |
| 8 | Crossbreed | female | 6 | 35 | 1 | 1 * | 1 | 1 |
| 9 | Golden retriever | female | 4 | 32 | 2 | 1 * | 1 | 2 |
| 10 | Crossbreed | male | 3 | 25 | 3 | 2 * | 2 | 3 |
| 11 | Labrador retriever | male | 6 | 35 | 2 * | 4 | 2 | 4 |
| 12 | Staffordshire Bull Terrier | male | 2 | 17 | 1 * | 1 | 1 | 1 |
| 13 | Crossbreed | female | 5 | 20 | 1 * | 2 | 1 | 2 |
| 14 | Labrador retriever | female | 4 | 30 | 2 * | 3 | 2 | 3 |
| 15 | Staffordshire Bull Terrier | female | 6 | 27 | 3 | 1 * | 1 | 3 |
| Descriptive statistics | ||||||||
| Median | 4 | 30 | 1 | 1 | 1 | 2 | ||
| Range | 1 | 17 | 1–3 | 1–4 | 1–2 | 1–4 | ||
| p-value | 6 | 57 | 0.625 | 0.009 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trębacz, P.; Frymus, J.; Barteczko, A.; Pawlik, M.; Kurkowska, A.; Czopowicz, M. Accuracy of Instrument Portal Placement Using a Custom-Made 3D-Printed Aiming Device versus Free Hand Technique in Canine Elbow Arthroscopy. Animals 2023, 13, 3592. https://doi.org/10.3390/ani13233592
Trębacz P, Frymus J, Barteczko A, Pawlik M, Kurkowska A, Czopowicz M. Accuracy of Instrument Portal Placement Using a Custom-Made 3D-Printed Aiming Device versus Free Hand Technique in Canine Elbow Arthroscopy. Animals. 2023; 13(23):3592. https://doi.org/10.3390/ani13233592
Chicago/Turabian StyleTrębacz, Piotr, Jan Frymus, Anna Barteczko, Mateusz Pawlik, Aleksandra Kurkowska, and Michał Czopowicz. 2023. "Accuracy of Instrument Portal Placement Using a Custom-Made 3D-Printed Aiming Device versus Free Hand Technique in Canine Elbow Arthroscopy" Animals 13, no. 23: 3592. https://doi.org/10.3390/ani13233592
APA StyleTrębacz, P., Frymus, J., Barteczko, A., Pawlik, M., Kurkowska, A., & Czopowicz, M. (2023). Accuracy of Instrument Portal Placement Using a Custom-Made 3D-Printed Aiming Device versus Free Hand Technique in Canine Elbow Arthroscopy. Animals, 13(23), 3592. https://doi.org/10.3390/ani13233592