

Outcomes of a Short-Duration, Large-Scale Canine Rabies Vaccination Campaign in Central Cambodia

 , , , , , and
, , , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Campaign Dates and Location
2.2. The 2023 Campaign Project Approval
2.3. Pre-Campaign Community Awareness
2.4. Campaign Coordination
2.5. Vaccination Protocol
2.6. Post-Vaccination Survey
2.7. Data Analysis
3. Results
3.1. Campaign Summary
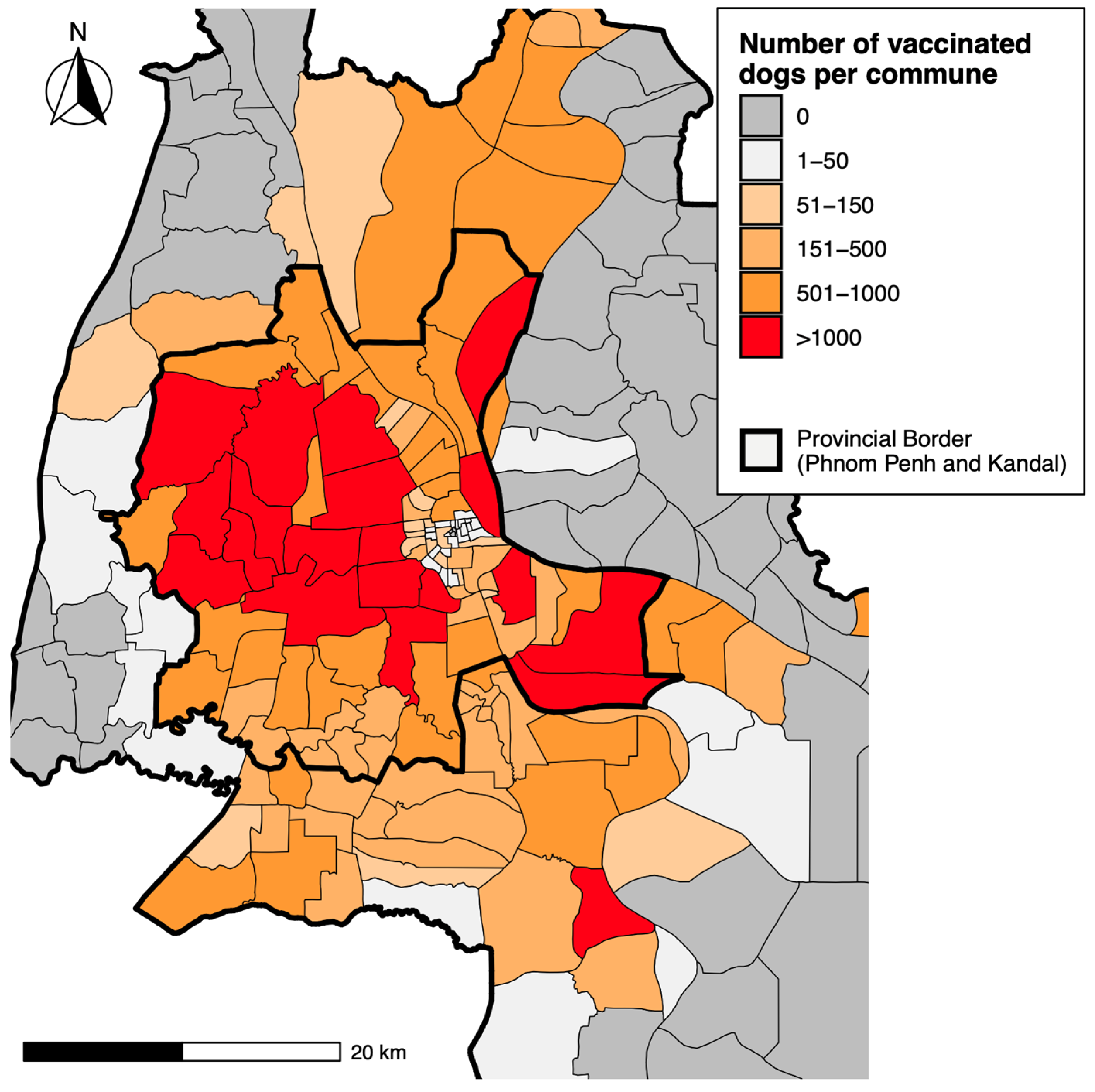
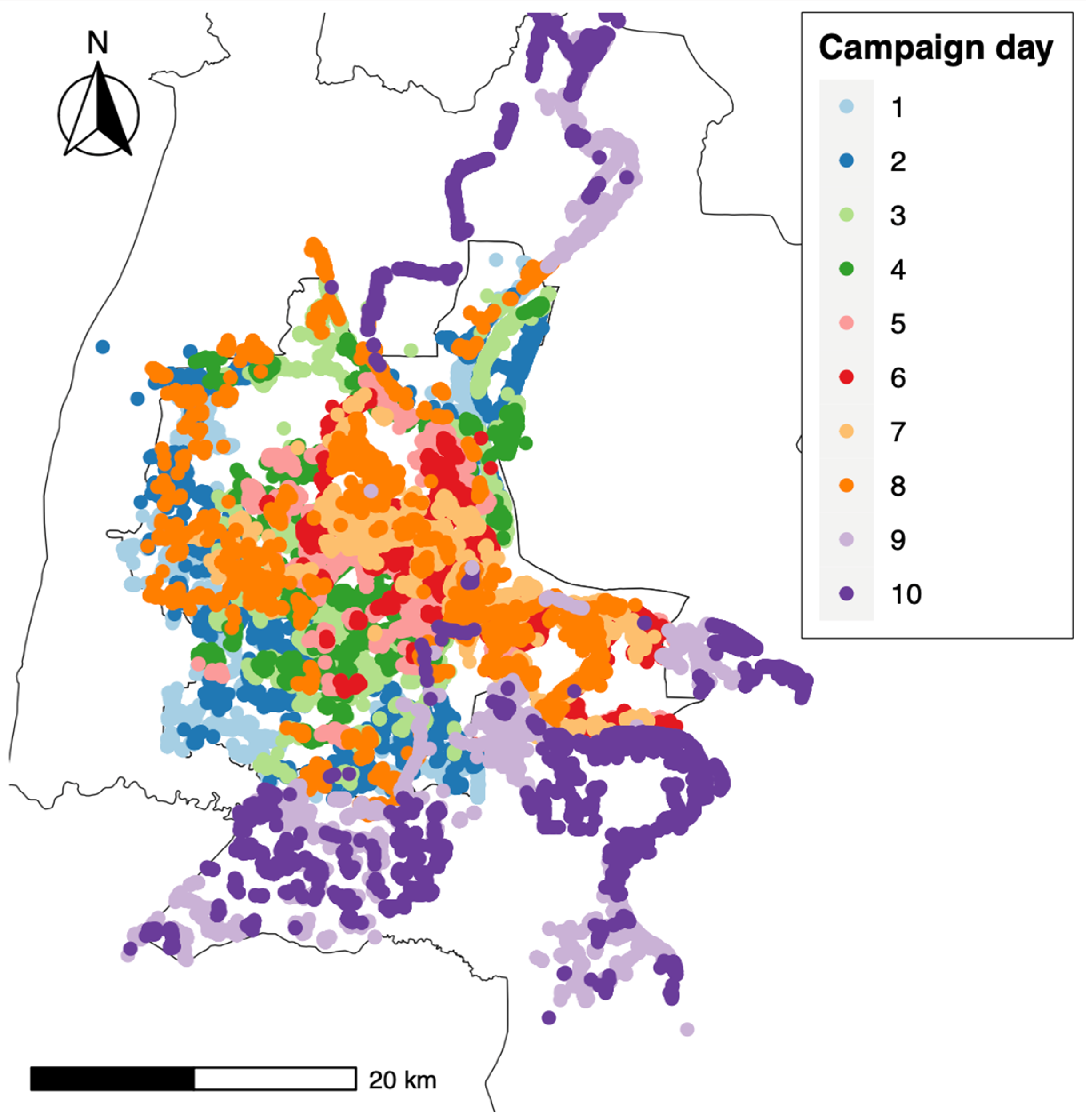
3.2. Campaign Progress
3.3. Encountered and Vaccinated Dog Demography
3.4. Reasons for Not Vaccinating Encountered Dogs
3.5. The Outcome of the Pre-Campaign Sensitization
3.6. Post-Vaccination Survey Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hampson, K.; Coudeville, L.; Lembo, T.; Sambo, M.; Kieffer, A.; Attlan, M.; Barrat, J.; Blanton, J.D.; Briggs, D.J.; Cleaveland, S.; et al. Estimating the global burden of endemic canine rabies. PLoS Neglect. Trop. Dis. 2015, 9, e0003709. [Google Scholar] [CrossRef]
- World Health Organization (WHO); Food and Agriculture Organization of the United Nations (FAO); World Organisation for Animal Health (OIE). United Against Rabies Collaboration: First Annual Progress Report. 2019. Available online: https://www.woah.org/app/uploads/2021/03/zeroby30annualreportfinal.pdf (accessed on 1 October 2023).
- Cleaveland, S.; Thumbi, S.; Sambo, M.; Lugelo, A.; Lushasi, K.; Hampson, K.; Lankester, F. Proof of concept of mass dog vaccination for thecontrol and elimination of canine rabies. Rev. Sci. Technol. 2018, 37, 559–568. [Google Scholar] [CrossRef]
- Kawaya, E.K.; Marcotty, T.; Mfumu-Kazadi, L.M.; Marcotty, D.; Van Gucht, S.; Kirschvink, N. Evaluation of dog vaccination schemes against rabies in Kinshasa, Democratic Republic of the Congo. Prev. Veter. Med. 2022, 198, 105531. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Expert Consultation on Rabies: Third Report; World Health Organization (WHO): Geneva, Switzerland, 2018; Volume 1012, ISBN 9789241210218. [Google Scholar]
- Zinsstag, J.; Lechenne, M.; Laager, M.; Mindekem, R.; Naïssengar, S.; Oussiguéré, A.; Bidjeh, K.; Rives, G.; Tessier, J.; Madjaninan, S.; et al. Vaccination of dogs in an African city interrupts rabies transmission and reduces human exposure. Sci. Transl. Med. 2017, 9, eaaf6984. [Google Scholar] [CrossRef]
- Freire De Carvalho, M.; Vigilato, M.A.N.; Pompei, J.A.; Rocha, F.; Vokaty, A.; Molina-Flores, B.; Cosivi, O.; Del Rio Vilas, V. Rabies in the Americas: 1998–2014. PLoS Negl. Trop. Dis. 2018, 12, e0006271. [Google Scholar] [CrossRef] [PubMed]
- Vigilato, M.A.N.; Clavijo, A.; Knobl, T.; Silva, H.M.T.; Cosivi, O.; Schneider, M.C.; Leanes, L.F.; Belotto, A.J.; Espinal, M.A. Progress towards eliminating canine rabies: Policies and perspectives from Latin America and the Caribbean. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2013, 368, 20120143. [Google Scholar] [CrossRef]
- Gibson, A.D.; Yale, G.; Corfmat, J.; Appupillai, M.; Gigante, C.M.; Lopes, M.; Betodkar, U.; Costa, N.C.; Fernandes, K.A.; Mathapati, P. Elimination of Human Rabies in Goa, India through an Integrated One Health Approach. Nat. Commun. 2022, 13, 2788. [Google Scholar] [CrossRef]
- Gibson, A.D.; Handel, I.G.; Shervell, K.; Roux, T.; Mayer, D.; Muyila, S.; Maruwo, G.B.; Nkhulungo, E.M.S.; Foster, R.A.; Chikungwa, P.; et al. The Vaccination of 35,000 Dogs in 20 Working Days Using Combined Static Point and Door-to-Door Methods in Blantyre, Malawi. PLoS Neglected Trop. Dis. 2016, 10, e0004824. [Google Scholar] [CrossRef]
- Sánchez-Soriano, C.; Gibson, A.D.; Gamble, L.; Bailey, J.L.B.; Mayer, D.; Lohr, F.; Chikungwa, P.; Chulu, J.; Handel, I.G.; Bronsvoort, B.M.D.; et al. Implementation of a mass canine rabies vaccination campaign in both rural and urban regions in southern Malawi. PLoS Neglected Trop. Dis. 2020, 14, e0008004. [Google Scholar] [CrossRef]
- Léchenne, M.; Oussiguere, A.; Naissengar, K.; Mindekem, R.; Mosimann, L.; Rives, G.; Hattendorf, J.; Moto, D.D.; Alfaroukh, I.O.; Zinsstag, J. Operational performance and analysis of two rabies vaccination campaigns in N’Djamena, Chad. Vaccine 2016, 34, 571–577. [Google Scholar] [CrossRef]
- Wallace, R.M.; Undurraga, E.A.; Gibson, A.; Boone, J.; Pieracci, E.G.; Gamble, L.; Blanton, J.D. Estimating the effectiveness of vaccine programs in dog populations. Epidemiol. Infect. 2019, 147, e247. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Neyra, R.; Toledo, A.M.; Arevalo-Nieto, C.; MacDonald, H.; De la Puente-León, M.; Naquira-Velarde, C.; Paz-Soldan, V.A.; Buttenheim, A.M.; Levy, M.Z. Socio-spatial heterogeneity in participation in mass dog rabies vaccination campaigns, Arequipa, Peru. PLoS Neglected Trop. Dis. 2019, 13, e0007600. [Google Scholar] [CrossRef] [PubMed]
- Mazeri, S.; Gibson, A.D.; Meunier, N.; Bronsvoort, B.M.; Handel, I.G.; Mellanby, R.J.; Gamble, L. Barriers of attendance to dog rabies static point vaccination clinics in Blantyre, Malawi. PLoS Neglected Trop. Dis. 2018, 12, e0006159. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.D.; Ohal, P.; Shervell, K.; Handel, I.G.; Bronsvoort, B.M.; Mellanby, R.J.; Gamble, L. Vaccinate-assess-move method of mass canine rabies vaccination utilising mobile technology data collection in Ranchi, India. BMC Infect. Dis. 2015, 15, 589. [Google Scholar] [CrossRef]
- Chanachai, K.; Wongphruksasoong, V.; Vos, A.; Leelahapongsathon, K.; Tangwangvivat, R.; Sagarasaeranee, O.; Lekcharoen, P.; Trinuson, P.; Kasemsuwan, S. Feasibility and Effectiveness Studies with Oral Vaccination of Free-Roaming Dogs against Rabies in Thailand. Viruses 2021, 13, 571. [Google Scholar] [CrossRef]
- Gibson, A.D.; Yale, G.; Vos, A.; Corfmat, J.; Airikkala-Otter, I.; King, A.; Wallace, R.M.; Gamble, L.; Handel, I.G.; Mellanby, R.J.; et al. Oral bait handout as a method to access roaming dogs for rabies vaccination in Goa, India: A proof of principle study. Vaccine X 2019, 1, 100015. [Google Scholar] [CrossRef] [PubMed]
- Wallace, R.M.; Cliquet, F.; Fehlner-Gardiner, C.; Fooks, A.R.; Sabeta, C.T.; Setién, A.A.; Tu, C.; Vuta, V.; Yakobson, B.; Yang, D.-K. Role of Oral Rabies Vaccines in the Elimination of Dog-Mediated Human Rabies Deaths. Emerg. Infect. Dis. 2020, 26, e201266. [Google Scholar] [CrossRef]
- Yale, G.; Lopes, M.; Isloor, S.; Head, J.R.; Mazeri, S.; Gamble, L.; Dukpa, K.; Gongal, G.; Gibson, A.D. Review of Oral Rabies Vaccination of Dogs and Its Application in India. Viruses 2022, 14, 155. [Google Scholar] [CrossRef]
- Freuling, C.M.; Busch, F.; Vos, A.; Ortmann, S.; Lohr, F.; Hedimbi, N.; Peter, J.; Nelson, H.A.; Shoombe, K.; Shilongo, A. Oral Rabies Vaccination of Dogs—Experiences from a Field Trial in Namibia. PLoS Negl. Trop. Dis. 2022, 16, e0010422. [Google Scholar] [CrossRef]
- Ly, S.; Buchy, P.; Heng, N.Y.; Ong, S.; Chhor, N.; Bourhy, H.; Vong, S. Rabies Situation in Cambodia. PLoS Negl. Trop. Dis. 2009, 3, e511. [Google Scholar] [CrossRef]
- Layan, M.; Dacheux, L.; Lemey, P.; Brunker, K.; Ma, L.; Troupin, C.; Dussart, P.; Chevalier, V.; Wood, J.L.N.; Ly, S. Uncovering the Endemic Circulation of Rabies in Cambodia. Mol. Ecol. 2023, 32, 5140–5155. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health; Ministry of Agriculture, Forestry and Fisheries; Ministry of Education, Youth and Sports; World Organisation for Animal Health (WOAH). The National Strategic Plan to Eliminate Rabies in Cambodia 2023–2030; (Forthcoming); WOAH: Paris, France, 2024. [Google Scholar]
- National Institute of Statistics. General Population Census of the Kingdom of Cambodia 2019, National Report on Final Census Results. 2019. Available online: https://www.nis.gov.kh/nis/Census2019/Provisional%20Population%20Census%202019_English_FINAL.pdf (accessed on 7 October 2023).
- Yen, Y.; Zhao, P.; Sohail, M.T. The Morphology and Circuity of Walkable, Bikeable, and Drivable Street Networks in Phnom Penh, Cambodia. Environ. Plan. B Urban Anal. City Sci. 2021, 48, 169–185. [Google Scholar] [CrossRef]
- Gibson, A.D.; Mazeri, S.; Lohr, F.; Mayer, D.; Burdon Bailey, J.L.; Wallace, R.M.; Handel, I.G.; Shervell, K.; de Bronsvoort, B.M.C.; Mellanby, R.J. One Million Dog Vaccinations Recorded on mHealth Innovation Used to Direct Teams in Numerous Rabies Control Campaigns. PLoS ONE 2018, 13, e0200942. [Google Scholar] [CrossRef] [PubMed]
- Monroe, B.; Ludder, F.; Dilius, P.; Crowdis, K.; Lohr, F.; Cleaton, J.; Gamble, L.; Blanton, J.; Etheart, M.; Pieracci, E.G. Every Dog Has Its Data: Evaluation of a Technology-Aided Canine Rabies Vaccination Campaign to Implement a Microplanning Approach. Front. Public Health 2021, 9, 757668. [Google Scholar] [CrossRef]
- Chevalier, V.; Davun, H.; Sorn, S.; Ly, P.; Pov, V.; Ly, S. Large Scale Dog Population Demography, Dog Management and Bite Risk Factors Analysis: A Crucial Step towards Rabies Control in Cambodia. PLoS ONE 2021, 16, e0254192. [Google Scholar] [CrossRef]
- Tarantola, A.; Blanchi, S.; Cappelle, J.; Ly, S.; Chan, M.; In, S.; Peng, Y.; Hing, C.; Taing, C.N.; Ly, S. Rabies Postexposure Prophylaxis Noncompletion After Dog Bites: Estimating the Unseen to Meet the Needs of the Underserved. Am. J. Epidemiol. 2018, 187, 306–315. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Putra, A.A.G.; Hampson, K.; Girardi, J.; Hiby, E.; Knobel, D.; Mardiana, W. Response to a Rabies Epidemic, Bali, Indonesia, 2008–2011. Emerg. Infect. Dis. 2013, 19, 648–651. [Google Scholar] [CrossRef]
- Wera, E.; Velthuis, A.G.J.; Geong, M.; Hogeveen, H. Costs of Rabies Control: An Economic Calculation Method Applied to Flores Island. PLoS ONE 2013, 8, e83654. [Google Scholar] [CrossRef]
- Gibson, A.D.; Wallace, R.M.; Rahman, A.; Bharti, O.K.; Isloor, S.; Lohr, F.; Gamble, L.; Mellanby, R.J.; King, A.; Day, M.J. Reviewing Solutions of Scale for Canine Rabies Elimination in India. Trop. Med. Infect. Dis. 2020, 5, 47. [Google Scholar] [CrossRef]
- LeRoux, K.; Stewart, D.; Perrett, K.D.; Nel, L.H.; Kessels, J.A.; Abela-Ridder, B. Rabies Control in KwaZulu-Natal, South Africa. Bull. World Health Org. 2018, 96, 360–365. [Google Scholar] [CrossRef]
- Walugembe, D.R.; Sibbald, S.; Le Ber, M.J.; Kothari, A. Sustainability of Public Health Interventions: Where Are the Gaps? Health Res. Policy Syst. 2019, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- De la Puente-León, M.; Levy, M.Z.; Toledo, A.M.; Recuenco, S.; Shinnick, J.; Castillo-Neyra, R. Spatial Inequality Hides the Burden of Dog Bites and the Risk of Dog-Mediated Human Rabies. Am. J. Trop. Med. Hyg. 2020, 103, 1247–1257. [Google Scholar] [CrossRef] [PubMed]
- Muthiani, Y.; Traoré, A.; Mauti, S.; Zinsstag, J.; Hattendorf, J. Low Coverage of Central Point Vaccination against Dog Rabies in Bamako, Mali. Prev. Vet. Med. 2015, 120, 203–209. [Google Scholar] [CrossRef]
- MacPhillamy, I.; Young, J.; Siek, S.; Bun, C.; Suon, S.; Toribio, J.-A.; Windsor, P.; Bush, R. Improving Village Animal Health Worker Participation in National Disease Surveillance Systems: A Case Study from Cambodia. Transbound. Emerg. Dis. 2020, 67, 967–978. [Google Scholar] [CrossRef]
- Sieng, S.; Patrick, I.W.; Windsor, P.A.; Walkden-Brown, S.W.; Kerr, J.; Sen, S.; Sar, C.; Smith, R.G.B.; Kong, R. Contributions of Village Animal Health Workers to Foot-and-Mouth Disease Control in Cambodia. Transbound. Emerg. Dis. 2022, 69, e406–e422. [Google Scholar] [CrossRef]
- Duamor, C.T.; Hampson, K.; Lankester, F.; Lugelo, A.; Mpolya, E.; Kreppel, K.; Cleaveland, S.; Wyke, S. Development, Feasibility and Potential Effectiveness of Community-Based Continuous Mass Dog Vaccination Delivery Strategies: Lessons for Optimization and Replication. PLoS Neglected Trop. Dis. 2022, 16, e0010318. [Google Scholar] [CrossRef]
- Lim, P.C.; Lembo, T.; Hampson, K.; Changalucha, J.; Sambo, M.; Ghosal, S. Tackling Barriers to Collective Action for Effective Vaccination Campaigns: Rabies in Rural Africa as an Example. Human. Soc. Sci. Commun. 2022, 9, 364. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.J.; Burdon Bailey, J.L.; Lohr, F.E.; Opira, W.; Migadde, M.; Gibson, A.D.; Handel, I.G.; de Bronsvoort, B.M.C.; Mellanby, R.J.; Gamble, L. Implementation of High Coverage Mass Rabies Vaccination in Rural Uganda Using Predominantly Static Point Methodology. Vet. J. 2019, 249, 60–66. [Google Scholar] [CrossRef]
- Kongkaew, W.; Coleman, P.; Pfeiffer, D.U.; Antarasena, C.; Thiptara, A. Vaccination Coverage and Epidemiological Parameters of the Owned-Dog Population in Thungsong District, Thailand. Prev. Vet. Med. 2004, 65, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Morters, M.K.; McKinley, T.J.; Restif, O.; Conlan, A.J.K.; Cleaveland, S.; Hampson, K.; Whay, H.R.; Damriyasa, I.M.; Wood, J.L.N. The Demography of Free-Roaming Dog Populations and Applications to Disease and Population Control. J. Appl. Ecol. 2014, 51, 1096–1106. [Google Scholar] [CrossRef]
- Nasiry, Z.; Mazlan, M.; Noordin, M.M.; Mohd Lila, M.A. Evaluation of Dynamics, Demography and Estimation of Free-Roaming Dog Population in Herat City, Afghanistan. Animals 2023, 13, 1126. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, H.K.; Robertson, I.D.; O’Dea, M.; Vanak, A.T. Demographic Characteristics of Free-Roaming Dogs (FRD) in Rural and Urban India Following a Photographic Sight-Resight Survey. Sci. Rep. 2019, 9, 16562. [Google Scholar] [CrossRef] [PubMed]
- Widyastuti, M.D.W.; Bardosh, K.L.; Sunandar, C.B.; Basri, C.; Basuno, E.; Jatikusumah, A.; Arief, R.A.; Putra, A.A.G.; Rukmantara, A.; Estoepangestie, A.T.S. On Dogs, People, and a Rabies Epidemic: Results from a Sociocultural Study in Bali, Indonesia. Infect. Dis. Poverty 2015, 4, 30. [Google Scholar] [CrossRef]
- Downes, M.J.; Dean, R.S.; Stavisky, J.H.; Adams, V.J.; Grindlay, D.J.; Brennan, M.L. Methods Used to Estimate the Size of the Owned Cat and Dog Population: A Systematic Review. BMC Vet. Res. 2013, 9, 121. [Google Scholar] [CrossRef]
- Lunney, M.; Fèvre, S.J.S.; Stiles, E.; Ly, S.; San, S.; Vong, S. Knowledge, Attitudes and Practices of Rabies Prevention and Dog Bite Injuries in Urban and Peri-Urban Provinces in Cambodia, 2009. Int. Health 2012, 4, 4–9. [Google Scholar] [CrossRef] [PubMed]
- World Bank Group Urban. Development in Phnom Penh. 2017. Available online: https://hdl.handle.net/10986/28958 (accessed on 13 October 2023). [CrossRef]
- Carvelli, A.; Scaramozzino, P.; Iacoponi, F.; Condoleo, R.; Marta, U.D. Size, Demography, Ownership Profiles, and Identification Rate of the Owned Dog Population in Central Italy. PLoS ONE 2020, 15, e0240551. [Google Scholar] [CrossRef]
- Thanapongtharm, W.; Kasemsuwan, S.; Wongphruksasoong, V.; Boonyo, K.; Pinyopummintr, T.; Wiratsudakul, A.; Gilbert, M.; Leelahapongsathon, K. Spatial Distribution and Population Estimation of Dogs in Thailand: Implications for Rabies Prevention and Control. Front. Vet. Sci. 2021, 8, 790701. [Google Scholar] [CrossRef]
- Hudson, E.G.; Brookes, V.J.; Ward, M.P.; Dürr, S. Using roaming behaviours of dogs to estimate contact rates: The predicted effect on rabies spread. Epidemiol. Infect. 2019, 147, e135. [Google Scholar] [CrossRef]
- Warembourg, C.; Fournié, G.; Abakar, M.F.; Alvarez, D.; Berger-González, M.; Odoch, T.; Wera, E.; Alobo, G.; Carvallo, E.T.L.; Bal, V.D.; et al. Predictors of free-roaming domestic dogs’ contact network centrality and their relevance for rabies control. Sci. Rep. 2021, 11, 12898. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Reasons for Non-Vaccination | # Among Dogs Older Than 3 Month Old (%) (n = 75,596) | # Among Puppies under 3 Months Old (%) (n = 13,690) | # Among Dogs (%) (n = 89,285) |
|---|---|---|---|
| Dog could not be held | 5243 (6.9) | 160 (1.2) | 5403 (6.1) |
| Owner was not present | 3365 (4.5) | 150 (1.1) | 3515 (3.9) |
| Refused by the owner due to recent vaccination | 2367 (3.1) | 111 (0.8) | 2478 (2.8) |
| Refused by the owner as the owner had no time to engage | 382 (0.5) | 14 (0.1) | 396 (0.4) |
| Refused by the owner due to a lack of trust in vaccination teams | 805 (1.1) | 75 (0.5) | 880 (1) |
| Refused by the owner due to a lack of awareness | 382 (0.5) | 16 (0.1) | 398 (0.4) |
| Other reasons | 1002 (1.3) | 158 (1.2) | 1160 (1.3) |
| Total | 13,546 (17.9) | 684 (5) | 14,230 (15.9) |
| Types of Sensitization | Total |
|---|---|
| Saw/heard the campaign advertisement | 12,686 (61.7) |
| Visited by village chief | 2818 (13.7) |
| Heard from family or friends | 2645 (12.9) |
| Heard the local announcement vehicle | 2607 (12.7) |
| Met Education Officers | 2473 (12.0) |
| Saw campaign materials | 2430 (11.8) |
| 1548 (6.8) | |
| Telegram | 310 (1.5) |
| Radio | 377 (1.6) |
| Did not see/hear the campaign advertisement | 7867 (38.3) |
| Districts | Number of Dogs Surveyed | Number of Surveyed Dogs That Were Vaccinated | Vaccination Coverage in % (95% CI) |
|---|---|---|---|
| Central districts | 99 | 67 | 67.7 (57.5–76.7) |
| Chbar Ampov | 555 | 364 | 65.6 (61.5–69.5) |
| Chraoy Chongvar | 459 | 325 | 70.8 (66.4–74.9) |
| Dangkao | 849 | 725 | 85.4 (82.8–87.7) |
| Kamboul | 984 | 518 | 52.6 (49.5–55.8) |
| Mean Chey | 173 | 101 | 58.4 (50.7–65.8) |
| Praek Pnov | 235 | 188 | 80 (74.3–84.9) |
| Pur SenChey | 928 | 597 | 64.3 (61.2–67.4) |
| Russey Keo | 123 | 104 | 84.6 (76.9–90.4) |
| Saensokh | 379 | 295 | 77.8 (73.3–81.9) |
| District average | 70.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tazawa, K.; Lewis, A.N.; Lohr, F.; Gibson, A.D.; Mayr, M.; Tep, B.; Heng, M.; Mazeri, S.; Phimpraphai, W.; Gamble, L. Outcomes of a Short-Duration, Large-Scale Canine Rabies Vaccination Campaign in Central Cambodia. Animals 2024, 14, 2654. https://doi.org/10.3390/ani14182654
Tazawa K, Lewis AN, Lohr F, Gibson AD, Mayr M, Tep B, Heng M, Mazeri S, Phimpraphai W, Gamble L. Outcomes of a Short-Duration, Large-Scale Canine Rabies Vaccination Campaign in Central Cambodia. Animals. 2024; 14(18):2654. https://doi.org/10.3390/ani14182654
Chicago/Turabian StyleTazawa, Keiichiro, Amy N. Lewis, Frederic Lohr, Andrew D. Gibson, Martina Mayr, Bengthay Tep, Morany Heng, Stella Mazeri, Waraphon Phimpraphai, and Luke Gamble. 2024. "Outcomes of a Short-Duration, Large-Scale Canine Rabies Vaccination Campaign in Central Cambodia" Animals 14, no. 18: 2654. https://doi.org/10.3390/ani14182654
APA StyleTazawa, K., Lewis, A. N., Lohr, F., Gibson, A. D., Mayr, M., Tep, B., Heng, M., Mazeri, S., Phimpraphai, W., & Gamble, L. (2024). Outcomes of a Short-Duration, Large-Scale Canine Rabies Vaccination Campaign in Central Cambodia. Animals, 14(18), 2654. https://doi.org/10.3390/ani14182654