
Evaluation of the Effects of an Undenatured Collagen Type-2-Based Nutraceutical (ARTHROSHINE® HA²) on Recovery Time after TPLO in Dogs: A Prospective, Randomized Study with Objective Gait Analysis as the Primary Outcome Measure
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
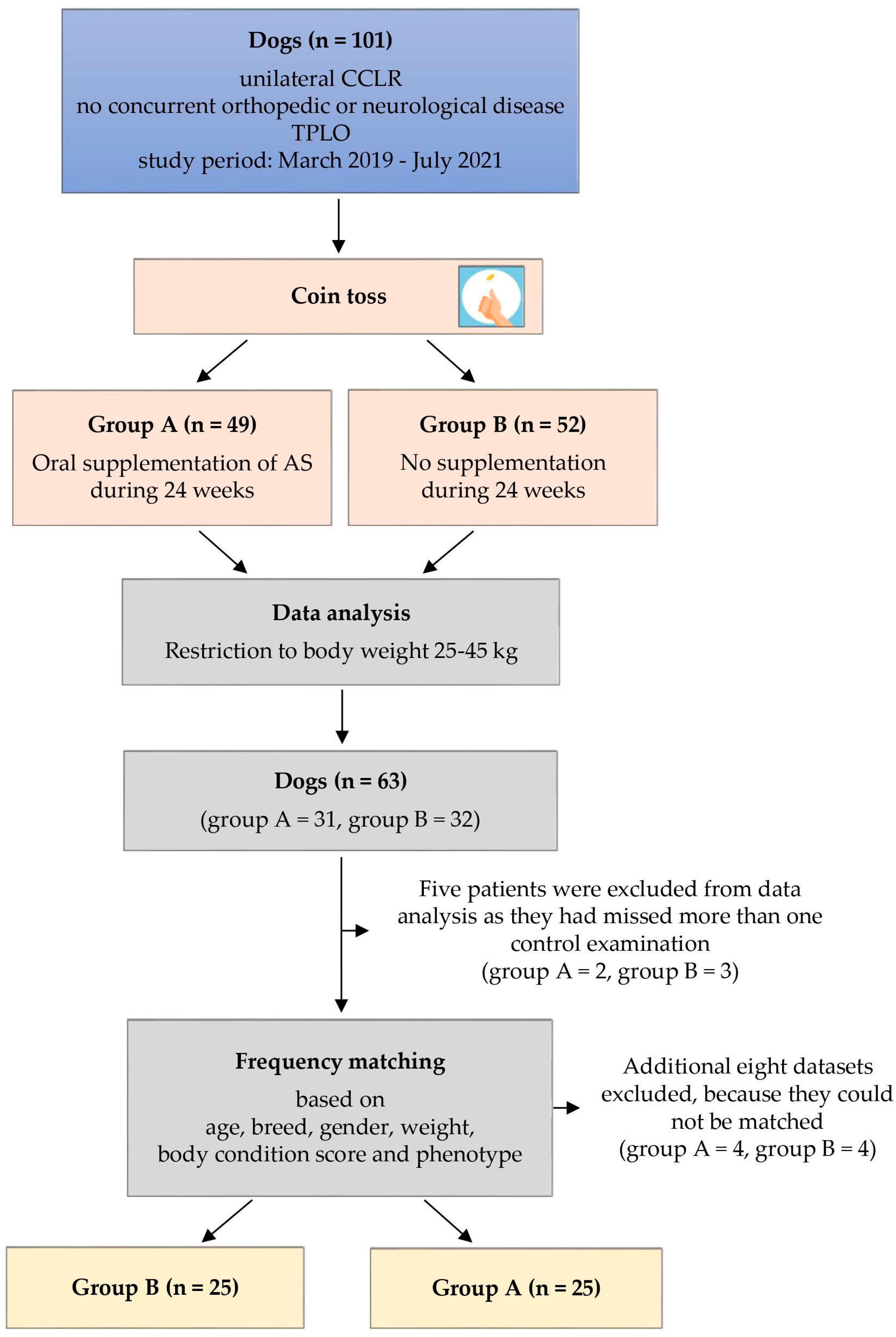
2.1. Study Design
2.2. Surgery and Rehabilitation
2.3. Computerized Gait Analysis
2.4. Data Analysis
3. Results
3.1. Comparability of Study Groups
3.2. Acceptance of Nutraceutical Supplementation
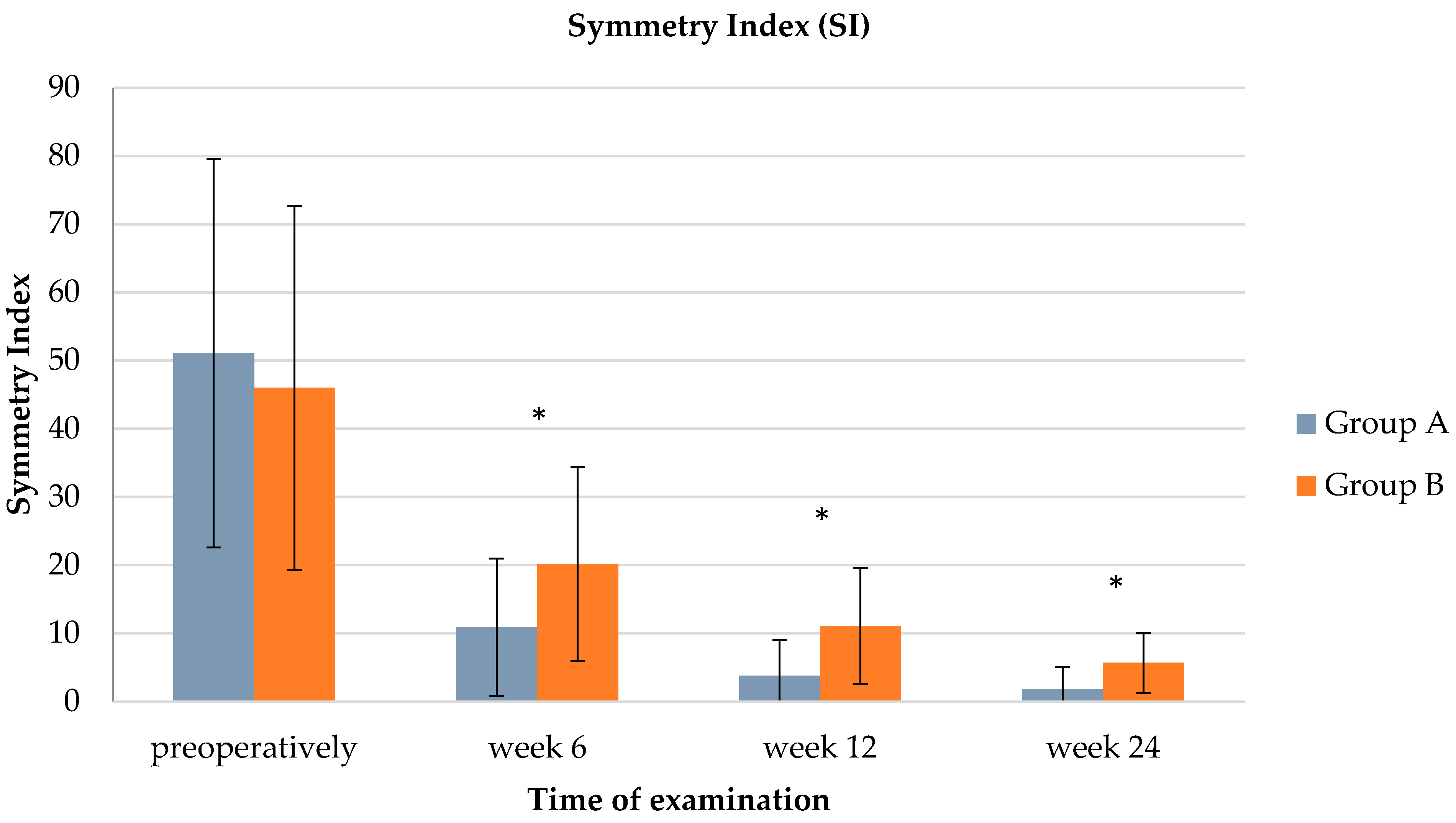
3.3. Gait Analysis
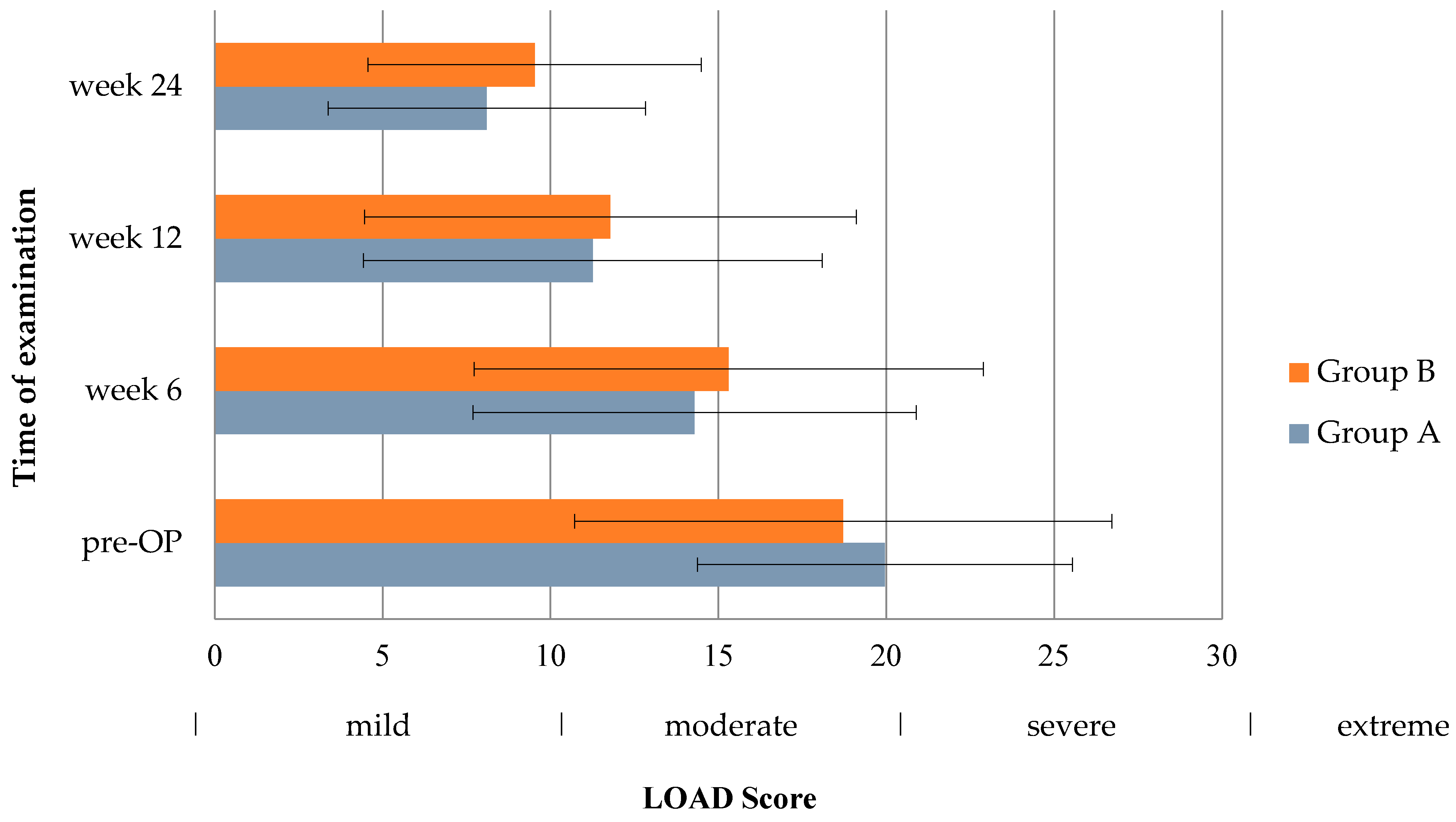
3.4. LOAD Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Comerford, E.J.; Smith, K.; Hayashi, K. Update on the aetiopathogenesis of canine cranial cruciate ligament disease. Vet. Comp. Orthop. Traumatol. 2011, 24, 91–98. [Google Scholar] [PubMed]
- Moore, E.V.; Weeren, R.; Paek, M. Extended long-term radiographic and functional comparison of tibial plateau leveling osteotomy vs tibial tuberosity advancement for cranial cruciate ligament rupture in the dog. Vet. Surg. 2020, 49, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Berger, B.; Knebel, J.; Steigmeier-Raith, S.; Reese, S.; Meyer-Lindenberg, A. Long-term outcome after surgical treatment of cranial cruciate ligament rupture in small breed dogs. Comparison of tibial plateau leveling osteotomy and extra-articular stifle stabilization. Tierarztl. Prax. Ausg. K Kleintiere Heimtiere 2015, 43, 373–380. [Google Scholar] [PubMed]
- von Pfeil, D.J.F.; Kowaleski, M.P.; Glassman, M.; Dejardin, L.M. Results of a survey of Veterinary Orthopedic Society members on the preferred method for treating cranial cruciate ligament rupture in dogs weighing more than 15 kilograms (33 pounds). J. Am. Vet. Med. Assoc. 2018, 253, 586–597. [Google Scholar] [PubMed]
- Krotscheck, U.; Nelson, S.A.; Todhunter, R.J.; Stone, M.; Zhang, Z. Long Term Functional Outcome of Tibial Tuberosity Advancement vs. Tibial Plateau Leveling Osteotomy and Extracapsular Repair in a Heterogeneous Population of Dogs. Vet. Surg. 2016, 45, 261–268. [Google Scholar] [CrossRef]
- Böddeker, J.; Drüen, S.; Meyer-Lindenberg, A.; Fehr, M.; Nolte, I.; Wefstaedt, P. Computer-assisted gait analysis of the dog: Comparison of two surgical techniques for the ruptured cranial cruciate ligament. Vet. Comp. Orthop. Traumatol. 2012, 25, 11–21. [Google Scholar] [PubMed]
- Nelson, S.A.; Krotscheck, U.; Rawlinson, J.; Todhunter, R.J.; Zhang, Z.; Mohammed, H. Long-term functional outcome of tibial plateau leveling osteotomy versus extracapsular repair in a heterogeneous population of dogs. Vet. Surg. 2013, 42, 38–50. [Google Scholar] [CrossRef]
- Monk, M.L.; Preston, C.A.; McGowan, C.M. Effects of early intensive postoperative physiotherapy on limb function after tibial plateau leveling osteotomy in dogs with deficiency of the cranial cruciate ligament. Am. J. Vet. Res. 2006, 67, 529–536. [Google Scholar] [CrossRef]
- Luna, S.P.L.; Basílio, A.C.; Steagall, P.V.M.; Machado, L.P.; Moutinho, F.Q.; Takahira, R.K.; Brandão, C.V.S. Evaluation of adverse effects of long-term oral administration of carprofen, etodolac, flunixin meglumine, ketoprofen, and meloxicam in dogs. Am. J. Vet. Res. 2007, 68, 258–264. [Google Scholar] [CrossRef]
- Pollmeier, M.; Toulemonde, C.; Fleishman, C.; Hanson, P.D. Clinical evaluation of firocoxib and carprofen for the treatment of dogs with osteoarthritis. Vet. Rec. 2006, 159, 547–551. [Google Scholar]
- Joubert, K.E. The effects of firocoxib (Previcox) in geriatric dogs over a period of 90 days. J. S Afr. Vet. Assoc. 2009, 80, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Lascelles, B.D.X.; Blikslager, A.T.; Fox, S.M.; Reece, D. Gastrointestinal tract perforation in dogs treated with a selective cyclooxygenase-2 inhibitor: 29 cases (2002–2003). J. Am. Vet. Med. Assoc. 2005, 227, 1112–1117. [Google Scholar]
- Reed, S. Nonsteroidal anti-inflammatory drug-induced duodenal ulceration and perforation in a mature rottweiler. Can. Vet. J. 2002, 43, 971–972. [Google Scholar] [PubMed]
- Duerr, F.M.; Carr, A.P.; Bebchuk, T.N.; Pople, N.C. Challenging diagnosis--icterus associated with a single perforating duodenal ulcer after long-term nonsteroidal antiinflammatory drug administration in a dog. Can. Vet. J. 2004, 45, 507–510. [Google Scholar]
- Gupta, R.C.; Canerdy, T.D.; Lindley, J.; Konemann, M.; Minniear, J.; Carroll, B.A.; Hendrick, C.; Goad, J.T.; Rohde, K.; Doss, R.; et al. Comparative therapeutic efficacy and safety of type-II collagen (UC-II), glucosamine and chondroitin in arthritic dogs: Pain evaluation by ground force plate. J. Anim. Physiol. Anim. Nutr. 2012, 96, 770–777. [Google Scholar] [CrossRef] [PubMed]
- D’Altilio, M.; Peal, A.; Alvey, M.; Simms, C.; Curtsinger, A.; Gupta, R.C.; Canerdy, T.D.; Goad, J.T.; Bagchi, M.; Bagchi, D. Therapeutic Efficacy and Safety of Undenatured Type II Collagen Singly or in Combination with Glucosamine and Chondroitin in Arthritic Dogs. Toxicol. Mech. Methods. 2007, 17, 189–196. [Google Scholar] [PubMed]
- Deparle, L.A.; Gupta, R.C.; Canerdy, T.D.; Goad, J.T.; D’Altilio, M.; Bagchi, M.; Bagchi, D. Efficacy and safety of glycosylated undenatured type-II collagen (UC-II) in therapy of arthritic dogs. J. Vet. Pharmacol. Ther. 2005, 28, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Crowley, D.C.; Lau, F.C.; Sharma, P.; Evans, M.; Guthrie, N.; Bagchi, M.; Bagchi, D.; Dey, D.K.; Raychaudhuri, S.P. Safety and efficacy of undenatured type II collagen in the treatment of osteoarthritis of the knee: A clinical trial. Int. J. Med. Sci. 2009, 6, 312–321. [Google Scholar]
- Lugo, J.P.; Saiyed, Z.M.; Lane, N.E. Efficacy and tolerability of an undenatured type II collagen supplement in modulating knee osteoarthritis symptoms: A multicenter randomized, double-blind, placebo-controlled study. Nutr. J. 2016, 15, 14. [Google Scholar] [CrossRef]
- Varney, J.L.; Fowler, J.W.; Coon, C.N. Undenatured type II collagen mitigates inflammation and cartilage degeneration in healthy Labrador Retrievers during an exercise regimen. Transl. Anim. Sci. 2021, 5, txab084. [Google Scholar]
- Bagi, C.; Berryman, E.; Teo, S.; Lane, N. Oral administration of undenatured native chicken type II collagen (UC-II) diminished deterioration of articular cartilage in a rat model of osteoarthritis (OA). Osteoarthr. Cartil. 2017, 25, 2080–2090. [Google Scholar] [CrossRef] [PubMed]
- Bagchi, D.; Misner, B.; Bagchi, M.; Kothari, S.C.; Downs, B.W.; Fafard, R.D.; Preuss, H.G. Effects of orally administered undenatured type II collagen against arthritic inflammatory diseases: A mechanistic exploration. Int. J. Clin. Pharmacol. Res. 2002, 22, 101–110. [Google Scholar] [PubMed]
- Nagler-Anderson, C.; A Bober, L.; E Robinson, M.; Siskind, G.W.; Thorbecke, G.J. Suppression of type II collagen-induced arthritis by intragastric administration of soluble type II collagen. Proc. Natl. Acad. Sci. USA 1986, 83, 7443–7446. [Google Scholar] [CrossRef] [PubMed]
- Trentham, D.E.; Dynesius-Trentham, R.A.; Orav, E.J.; Combitchi, D.; Lorenzo, C.; Sewell, K.L.; Hafler, D.A.; Weiner, H.L. Effects of oral administration of type II collagen on rheumatoid arthritis. Science 1993, 261, 1727–1730. [Google Scholar] [PubMed]
- Asnagli, H.; Martire, D.; Belmonte, N.; Quentin, J.; Bastian, H.; Boucard-Jourdin, M.; Fall, P.B.; Mausset-Bonnefont, A.-L.; Mantello-Moreau, A.; Rouquier, S.; et al. Type 1 regulatory T cells specific for collagen type II as an efficient cell-based therapy in arthritis. Arthritis Res. Ther. 2014, 16, R115. [Google Scholar] [CrossRef]
- Tiku, M.L.; Shah, R.; Allison, G.T. Evidence linking chondrocyte lipid peroxidation to cartilage matrix protein degradation. Possible role in cartilage aging and the pathogenesis of osteoarthritis. J. Biol. Chem. 2000, 275, 20069–20076. [Google Scholar] [PubMed]
- Beer, P.; Bockstahler, B.; Schnabl-Feichter, E. Tibial plateau leveling osteotomy and tibial tuberosity advancement—A systematic review. Tierarztl. Prax. Ausg. K Kleintiere Heimtiere 2018, 46, 223–235. [Google Scholar] [CrossRef]
- Walton, M.B.; Cowderoy, E.; Lascelles, D.; Innes, J.F. Evaluation of construct and criterion validity for the ‘Liverpool Osteoarthritis in Dogs’ (LOAD) clinical metrology instrument and comparison to two other instruments. PLoS ONE 2013, 8, e58125. [Google Scholar]
- Knebel, J.; Eberle, D.; Steigmeier-Raith, S.; Reese, S.; Meyer-Lindenberg, A. Outcome after Tibial Plateau Levelling Osteotomy and Modified Maquet Procedure in Dogs with Cranial Cruciate Ligament Rupture. Vet. Comp. Orthop. Traumatol. 2020, 33, 189–197. [Google Scholar]
- Warzee, C.C.; Dejardin, L.M.; Arnoczky, S.P.; Perry, R.L. Effect of tibial plateau leveling on cranial and caudal tibial thrusts in canine cranial cruciate-deficient stifles: An in vitro experimental study. Vet. Surg. 2001, 30, 278–286. [Google Scholar] [CrossRef]
- Budsberg, S.C.; Jevens, D.J.; Brown, J.; Foutz, T.L.; E DeCamp, C.; Reece, L. Evaluation of limb symmetry indices, using ground reaction forces in healthy dogs. Am. J. Vet. Res. 1993, 54, 1569–1574. [Google Scholar]
- Fanchon, L.; Grandjean, D. Accuracy of asymmetry indices of ground reaction forces for diagnosis of hind limb lameness in dogs. Am. J. Vet. Res. 2007, 68, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.O.; Herzog, W.; Nigg, B.M. Use of force platform variables to quantify the effects of chiropractic manipulation on gait symmetry. J. Manipulative Physiol. Ther. 1987, 10, 172–176. [Google Scholar] [PubMed]
- Pietsch, S.; Steigmeier-Raith, S.; Reese, S.; Meyer-Lindenberg, A. Reliability of kinetic measurements of healthy dogs examined while walking on a treadmill. Am. J. Vet. Res. 2020, 81, 804–809. [Google Scholar] [PubMed]
- Imhof, J.; Kaestner, S.; Montavon, P.M.; Voss, K. Force plate gait analysis at the walk and trot in dogs with low-grade hindlimb lameness. Vet. Comp. Orthop. Traumatol. 2007, 20, 299–304. [Google Scholar]
- Stegen, B.; Berger, B.; Assies, M.; Doherr, M.; Rohwedder, T.; Böttcher, P. Type 2 undenatured collagen—Effects in convalescence and osteoarthritis progression after TPLO in dogs: A prospective, blinded and randomized study. Vet. Surg. 2024, in press. [Google Scholar]
- Hercock, C.A.; Pinchbeck, G.; Giejda, A.; Clegg, P.D.; Innes, J.F. Validation of a client-based clinical metrology instrument for the evaluation of canine elbow osteoarthritis. J. Small Anim. Pract. 2009, 50, 266–271. [Google Scholar]
- Lubis, A.M.T.; Siagian, C.; Wonggokusuma, E.; Marsetyo, A.F.; Setyohadi, B. Comparison of Glucosamine-Chondroitin Sulfate with and without Methylsulfonylmethane in Grade I-II Knee Osteoarthritis: A Double Blind Randomized Controlled Trial. Acta Med. Indones 2017, 49, 105–111. [Google Scholar]
- Withee, E.D.; Tippens, K.M.; Dehen, R.; Tibbitts, D.; Hanes, D.; Zwickey, H. Effects of Methylsulfonylmethane (MSM) on exercise-induced oxidative stress, muscle damage, and pain following a half-marathon: A double-blind, randomized, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2017, 14, 24. [Google Scholar]
- Kim, L.; Axelrod, L.; Howard, P.; Buratovich, N.; Waters, R. Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain of the knee: A pilot clinical trial. Osteoarthr. Cartil. 2006, 14, 286–294. [Google Scholar] [CrossRef]
- Marañón, G.; Muñoz-Escassi, B.; Manley, W.; García, C.; Cayado, P.; de la Muela, M.S.; Olábarri, B.; León, R.; Vara, E. The effect of methyl sulphonyl methane supplementation on biomarkers of oxidative stress in sport horses following jumping exercise. Acta Vet. Scand 2008, 50, 45. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, T.; Seino, S.; Sato, T.; Matsuoka, R.; Masuda, Y.; Fukui, N. Oral administration of polymer hyaluronic acid alleviates symptoms of knee osteoarthritis: A double-blind, placebo-controlled study over a 12-month period. Sci. World J. 2012, 2012, 167928. [Google Scholar] [CrossRef] [PubMed]
- Ricci, M.; Micheloni, G.M.; Berti, M.; Perusi, F.; Sambugaro, E.; Vecchini, E.; Magnan, B. Clinical comparison of oral administration and viscosupplementation of hyaluronic acid (HA) in early knee osteoarthritis. Musculoskelet. Surg. 2017, 101, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.; Awad, M.E.; Hamrick, M.W.; Hunter, M.; Fulzele, S. Recent advances in hyaluronic acid based therapy for osteoarthritis. Clin. Transl. Med. 2018, 7, 6. [Google Scholar] [CrossRef]
- Peal, A.; D’Altilio, M.; Simms, C.; Alvey, M.; Gupta, R.C.; Goad, J.T.; Canerdy, T.D.; Bagchi, M.; Bagchi, D. Therapeutic efficacy and safety of undenatured type-II collagen (UC-II) alone or in combination with (-)-hydroxycitric acid and chromemate in arthritic dogs. J. Vet. Pharmacol. Ther. 2007, 30, 275–278. [Google Scholar]
- Stabile, M.; Lacitignola, L.; Samarelli, R.; Fiorentino, M.; Crovace, A.; Staffieri, F. Evaluation of clinical efficacy of undenatured type II collagen supplementation compared to cimicoxib and their association in dogs affected by natural occurring osteoarthritis. Res. Vet. Sci. 2022, 151, 27–35. [Google Scholar] [CrossRef]
- McMillan, F.D. The placebo effect in animals. J. Am. Vet. Med. Assoc. 1999, 215, 992–999. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group A (n = 25) | Group B (n = 25) | p-Value | |
|---|---|---|---|
| Age (years) | 5.52 ± 2.62 | 6.12 ± 2.83 | 0.44 |
| Weight (kg) | 35.24 ± 6.16 | 32.9 ± 6.5 | 0.21 |
| Sex | 1.0 | ||
| Male | 9 | 9 | |
| Female | 16 | 16 | |
| Body condition score (1–9) | 5 ± 0.58 | 5 ± 0.54 | 0.8 |
| Subtotal meniscectomy | 8 | 10 | 0.57 |
| Cruciate tear type | 0.69 | ||
| Partial | 4 | 3 | |
| Complete | 21 | 22 | |
| CCL side | 1.0 | ||
| Left | 15 | 15 | |
| Right | 10 | 10 |
| Time | ||||
|---|---|---|---|---|
| Pre-OP (n = 49) | Week 6 (n = 48) | Week 12 (n = 47) | Week 24 (n = 41) | |
| Group A | 29.0 ± 9.2 | 40.2 ± 5.0 | 42.5 ± 5.1 | 44.2 ± 4.1 |
| Group B | 30.2 ± 7.9 | 36.8 ± 4.4 | 39.5 ± 4.1 | 41.4 ± 3.9 |
| p-value | 0.6264 | 0.0143 | 0.0275 | 0.0346 |
| Time | ||||
|---|---|---|---|---|
| Pre-OP (n = 49) | Week 6 (n = 48) | Week 12 (n = 47) | Week 24 (n = 41) | |
| Group A | 22.4 ± 13.6 | 4.5 ± 4.1 | 2.0 ± 2.8 | 0.8 ± 1.4 |
| Group B | 18.3 ± 10 | 8.3 ± 5.6 | 4.5 ± 3.6 | 3.1 ± 2.8 |
| p-value | 0.2297 | 0.01 | 0.0114 | 0.0008 |
| Time | ||||
|---|---|---|---|---|
| Pre-OP (n = 49) | Week 6 (n = 48) | Week 12 (n = 47) | Week 24 (n = 41) | |
| Group A | 51.1 ± 28.5 | 10.9 ± 10.1 | 3.8 ± 5.3 | 1.8 ± 3.3 |
| Group B | 46.0 ± 26.7 | 20.2 ± 14.2 | 11.1 ± 8.5 | 5.7 ± 4.4 |
| p-value | 0.5194 | 0.0119 | 0.001 | 0.0026 |
| Time | ||||
|---|---|---|---|---|
| Pre-OP (n = 49) | Week 6 (n = 48) | Week 12 (n = 47) | Week 24 (n = 41) | |
| Group A | 0 | 41.7 | 80.0 | 95.8 |
| Group B | 0 | 20.8 | 48.0 | 52.9 |
| p-value | - | 0.1222 | 0.0241 | 0.0012 |
| Time | ||||
|---|---|---|---|---|
| Pre-OP (n = 49) | Week 6 (n = 48) | Week 12 (n = 47) | Week 24 (n = 41) | |
| Group A | 0 | 41.7 | 87.0 | 95.8 |
| Group B | 0 | 20.8 | 41.7 | 82.4 |
| p-value | - | 0.1222 | 0.0014 | 0.1594 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assies, M.; Berger, B.; Stegen, B.; Rohwedder, T.; Doherr, M.; Böttcher, P. Evaluation of the Effects of an Undenatured Collagen Type-2-Based Nutraceutical (ARTHROSHINE® HA²) on Recovery Time after TPLO in Dogs: A Prospective, Randomized Study with Objective Gait Analysis as the Primary Outcome Measure. Animals 2024, 14, 298. https://doi.org/10.3390/ani14020298
Assies M, Berger B, Stegen B, Rohwedder T, Doherr M, Böttcher P. Evaluation of the Effects of an Undenatured Collagen Type-2-Based Nutraceutical (ARTHROSHINE® HA²) on Recovery Time after TPLO in Dogs: A Prospective, Randomized Study with Objective Gait Analysis as the Primary Outcome Measure. Animals. 2024; 14(2):298. https://doi.org/10.3390/ani14020298
Chicago/Turabian StyleAssies, Maria, Björn Berger, Bente Stegen, Thomas Rohwedder, Marcus Doherr, and Peter Böttcher. 2024. "Evaluation of the Effects of an Undenatured Collagen Type-2-Based Nutraceutical (ARTHROSHINE® HA²) on Recovery Time after TPLO in Dogs: A Prospective, Randomized Study with Objective Gait Analysis as the Primary Outcome Measure" Animals 14, no. 2: 298. https://doi.org/10.3390/ani14020298
APA StyleAssies, M., Berger, B., Stegen, B., Rohwedder, T., Doherr, M., & Böttcher, P. (2024). Evaluation of the Effects of an Undenatured Collagen Type-2-Based Nutraceutical (ARTHROSHINE® HA²) on Recovery Time after TPLO in Dogs: A Prospective, Randomized Study with Objective Gait Analysis as the Primary Outcome Measure. Animals, 14(2), 298. https://doi.org/10.3390/ani14020298