



Stereoselective Pharmacokinetics of Ketamine Administered at a Low Dose in Awake Dogs
 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animal Ethics
2.2. Animals and Data Collection
2.3. Plasma Level Analysis
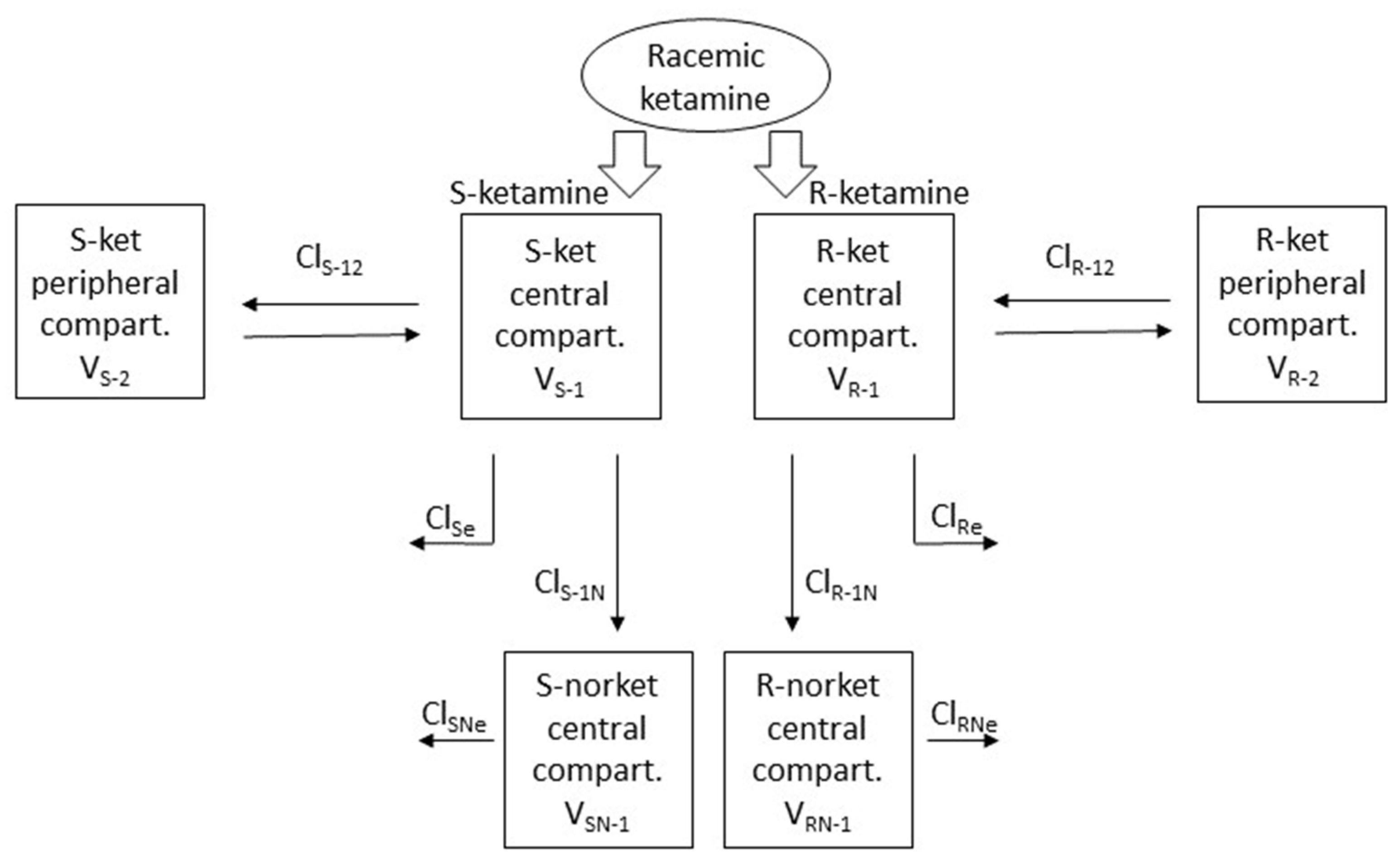
2.4. Pharmacokinetic Modelling
2.5. Prediction
2.6. Behavioural and Antinociceptive Data
2.7. Statistical Analysis
3. Results
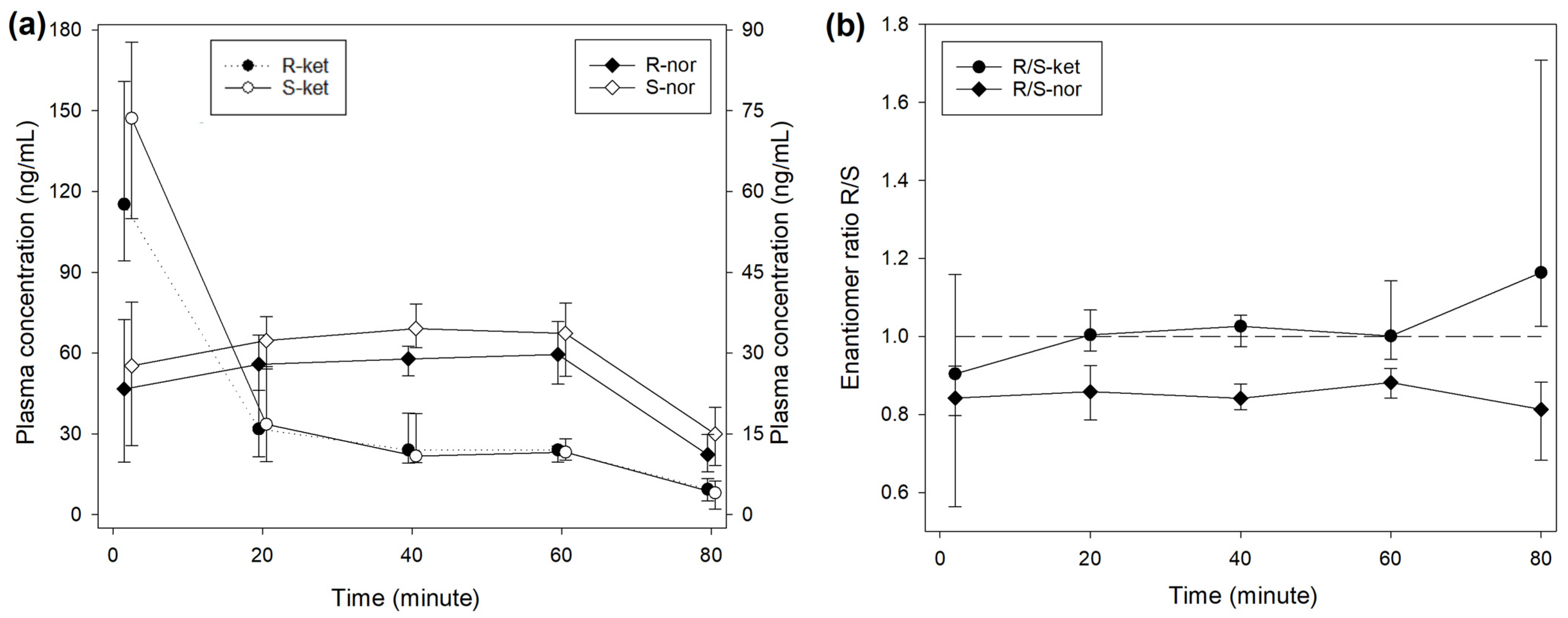
3.1. Plasma Concentrations
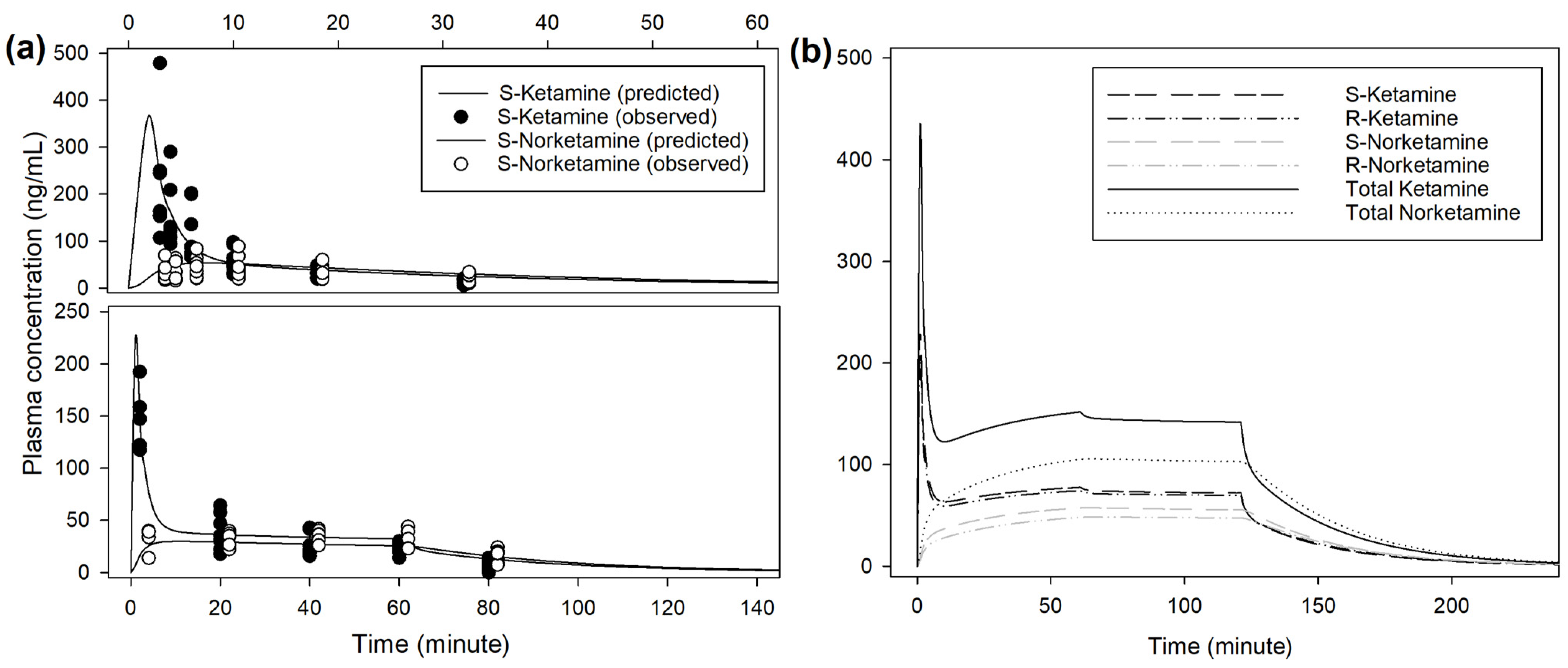
3.2. Pharmacokinetic Analysis and Prediction
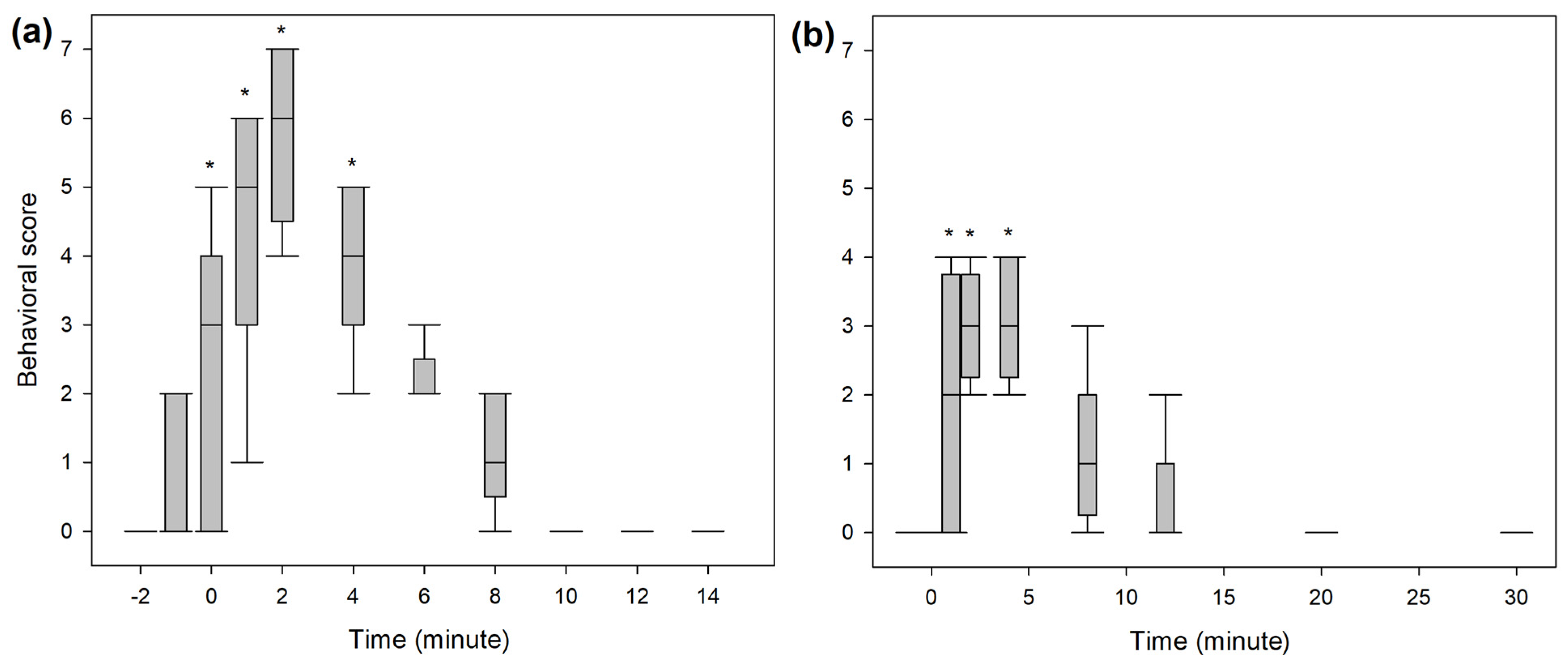
3.3. Behavioural Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wright, M. Pharmacologic effects of ketamine and its use in veterinary medicine. J. Am. Vet. Med. Assoc. 1982, 180, 1462–1471. [Google Scholar] [PubMed]
- Domino, E.F. Taming the ketamine tiger. 1965. Anesthesiology 2010, 113, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Filibeck, U.; Castellano, C. Strain dependent effects of ketamine on locomotor activity and antinociception in mice. Pharmacol. Biochem. Behav. 1980, 13, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Sadove, M.S.; Shulman, M.; Hatano, S.; Fevold, N. Analgesic effects of ketamine administered in subdissociative doses. Anesth. Analg. 1971, 50, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Anis, N.A.; Berry, S.C.; Burton, N.R.; Lodge, D. The dissociative anaesthetics, ketamine and phencyclidine, selectively reduce excitation of central mammalian neurones by N-methyl-aspartate. Br. J. Pharmacol. 1983, 79, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.F.; Dahl, J.B.; Moore, R.A.; Kalso, E. Peri-operative ketamine for acute post-operative pain: A quantitative and qualitative systematic review (Cochrane review). Acta Anaesthesiol. Scand. 2005, 49, 1405–1428. [Google Scholar] [CrossRef] [PubMed]
- McNicol, E.D.; Schumann, R.; Haroutounian, S. A systematic review and meta-analysis of ketamine for the prevention of persistent post-surgical pain. Acta Anaesthesiol. Scand. 2014, 58, 1199–1213. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.E.; Walton, J.A.; Hellyer, P.W.; Gaynor, J.S.; Mama, K.R. Use of low doses of ketamine administered by constant rate infusion as an adjunct for postoperative analgesia in dogs. J. Am. Vet. Med. Assoc. 2002, 221, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Bergadano, A.; Andersen, O.K.; Arendt-Nielsen, L.; Theurillat, R.; Thormann, W.; Spadavecchia, C. Plasma levels of a low-dose constant-rate-infusion of ketamine and its effect on single and repeated nociceptive stimuli in conscious dogs. Vet. J. 2009, 182, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Slingsby, L.S.; Waterman-Pearson, A.E. The post-operative analgesic effects of ketamine after canine ovariohysterectomy--a comparison between pre- or post-operative administration. Res. Vet. Sci. 2000, 69, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Sarrau, S.; Jourdan, J.; Dupuis-Soyris, F.; Verwaerde, P. Effects of postoperative ketamine infusion on pain control and feeding behaviour in bitches undergoing mastectomy. J. Small Anim. Pract. 2007, 48, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Bednarski, R.M. Dogs and Cats. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2015; pp. 819–826. [Google Scholar]
- Gaynor, J.S.; Muir, W.W. Handbook of Veterinary Pain Management, 3rd ed.; Elsevier: St. Louis, MO, USA, 2015; p. 620. [Google Scholar] [CrossRef]
- Kerr, C. Pain management I: Systemic analgesics. In BSAVA Manual of Canine and Feline Anaesthesia and Analgesia; Duke-Novakovski, T., De Vries, M., Seymour, C., Eds.; BSAVA: Gloucester, UK, 2016; pp. 124–142. [Google Scholar] [CrossRef]
- Clements, J.A.; Nimmo, W.S.; Grant, I.S. Bioavailability, pharmacokinetics, and analgesic activity of ketamine in humans. J. Pharm. Sci. 1982, 71, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Domino, E.F.; Zsigmond, E.K.; Domino, L.E.; Domino, K.E.; Kothary, S.P.; Domino, S.E. Plasma levels of ketamine and two of its metabolites in surgical patients using a gas chromatographic mass fragmentographic assay. Anesth. Analg. 1982, 61, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Richebe, P.; Rivat, C.; Rivalan, B.; Maurette, P.; Simonnet, G. Low doses ketamine: Antihyperalgesic drug, non-analgesic. Ann. Fr. Anesth. Reanim. 2005, 24, 1349–1359. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.; Wise, R.G.; Painter, D.J.; Longe, S.E.; Tracey, I. An investigation to dissociate the analgesic and anesthetic properties of ketamine using functional magnetic resonance imaging. Anesthesiology 2004, 100, 292–301. [Google Scholar] [CrossRef]
- Mion, G. Ketamine stakes in 2018: Right doses, good choices. Eur. J. Anaesthesiol. 2019, 36, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Mion, G.; Villevieille, T. Ketamine pharmacology: An update (pharmacodynamics and molecular aspects, recent findings). CNS Neurosci. Ther. 2013, 19, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Kaka, U.; Saifullah, B.; Abubakar, A.A.; Goh, Y.M.; Fakurazi, S.; Kaka, A.; Behan, A.A.; Ebrahimi, M.; Chen, H.C. Serum concentration of ketamine and antinociceptive effects of ketamine and ketamine-lidocaine infusions in conscious dogs. BMC Vet. Res. 2016, 12, 198. [Google Scholar] [CrossRef] [PubMed]
- Kaka, J.S.; Hayton, W.L. Pharmacokinetics of ketamine and two metabolites in the dog. J. Pharmacokinet. Biopharm. 1980, 8, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Schwieger, I.M.; Szlam, F.; Hug, C.C., Jr. The pharmacokinetics and pharmacodynamics of ketamine in dogs anesthetized with enflurane. J. Pharmacokinet. Biopharm. 1991, 19, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Henthorn, T.K.; Krejcie, T.C.; Niemann, C.U.; Enders-Klein, C.; Shanks, C.A.; Avram, M.J. Ketamine distribution described by a recirculatory pharmacokinetic model is not stereoselective. Anesthesiology 1999, 91, 1733–1743. [Google Scholar] [CrossRef]
- Roncada, P.; Zaghini, A.; Riciputi, C.; Romagnoli, N.; Spadari, A. Kinetics of ketamine plasma and urine metabolite levels following intravenous administration in the dog. Vet. Res. Commun. 2003, 27 (Suppl. 1), 433–436. [Google Scholar] [CrossRef]
- Pypendop, B.H.; Ilkiw, J.E. Pharmacokinetics of ketamine and its metabolite, norketamine, after intravenous administration of a bolus of ketamine to isoflurane-anesthetized dogs. Am. J. Vet. Res. 2005, 66, 2034–2038. [Google Scholar] [CrossRef]
- Sandbaumhuter, F.A.; Theurillat, R.; Bektas, R.N.; Kutter, A.P.N.; Bettschart-Wolfensberger, R.; Thormann, W. Pharmacokinetics of ketamine and three metabolites in Beagle dogs under sevoflurane vs. medetomidine comedication assessed by enantioselective capillary electrophoresis. J. Chromatogr. A 2016, 1467, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, N.; Bektas, R.N.; Kutter, A.P.; Barbarossa, A.; Roncada, P.; Hartnack, S.; Bettschart-Wolfensberger, R. Pharmacokinetics of ketamine and norketamine enantiomers after racemic or S-ketamine IV bolus administration in dogs during sevoflurane anaesthesia. Res. Vet. Sci. 2017, 112, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Berke, K.; KuKanich, B.; Orchard, R.; Rankin, D.; Joo, H. Clinical and pharmacokinetic interactions between oral fluconazole and intravenous ketamine and midazolam in dogs. Vet. Anaesth. Analg. 2019, 46, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, N.; Bektas, R.N.; Kutter, A.P.N.; Barbarossa, A.; Roncada, P.; Hartnack, S.; Bettschart-Wolfensberger, R. Pharmacokinetics of S-ketamine and R-ketamine and their active metabolites after racemic ketamine or S-ketamine intravenous administration in dogs sedated with medetomidine. Vet. Anaesth. Analg. 2020, 47, 168–176. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Petersen-Felix, S.; Fischer, M.; Bak, P.; Bjerring, P.; Zbinden, A.M. The effect of N-methyl-D-aspartate antagonist (ketamine) on single and repeated nociceptive stimuli: A placebo-controlled experimental human study. Anesth. Analg. 1995, 81, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Theurillat, R.; Knobloch, M.; Schmitz, A.; Lassahn, P.G.; Mevissen, M.; Thormann, W. Enantioselective analysis of ketamine and its metabolites in equine plasma and urine by CE with multiple isomer sulfated beta-CD. Electrophoresis 2007, 28, 2748–2757. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, A.; Thormann, W.; Moessner, L.; Theurillat, R.; Helmja, K.; Mevissen, M. Enantioselective CE analysis of hepatic ketamine metabolism in different species in vitro. Electrophoresis 2010, 31, 1506–1516. [Google Scholar] [CrossRef]
- Levionnois, O.L.; Mevissen, M.; Thormann, W.; Spadavecchia, C. Assessing the efficiency of a pharmacokinetic-based algorithm for target-controlled infusion of ketamine in ponies. Res. Vet. Sci. 2010, 88, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Goksuluk, D.; Korkmaz, S.; Zararsiz, G.; Karaağaoğlu, A.E. EasyROC: An Interactive Web-tool for ROC Curve Analysis Using R Language Environment. R J. 2016, 8, 213–230. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Capponi, L.; Schmitz, A.; Thormann, W.; Theurillat, R.; Mevissen, M. In vitro evaluation of differences in phase 1 metabolism of ketamine and other analgesics among humans, horses, and dogs. Am. J. Vet. Res. 2009, 70, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, A.; Portier, C.J.; Thormann, W.; Theurillat, R.; Mevissen, M. Stereoselective biotransformation of ketamine in equine liver and lung microsomes. J. Vet. Pharmacol. Ther. 2008, 31, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Larenza, M.P.; Peterbauer, C.; Landoni, M.F.; Levionnois, O.L.; Schatzmann, U.; Spadavecchia, C.; Thormann, W. Stereoselective pharmacokinetics of ketamine and norketamine after constant rate infusion of a subanesthetic dose of racemic ketamine or S-ketamine in Shetland ponies. Am. J. Vet. Res. 2009, 70, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, F.; Terrier, J.; Favre, S.; Gosselin, P.; Fontana, P.; Daali, Y.; Lenoir, C.; Samer, C.F.; Rollason, V.; Reny, J.L.; et al. Population pharmacokinetics of apixaban in a real-life hospitalized population from the OptimAT study. CPT Pharmacomet. Syst. Pharmacol. 2023, 12, 1541–1552. [Google Scholar] [CrossRef] [PubMed]
- Lixoft. Inter Occasion Variability. Monolix Documentation Version 2023. Available online: https://monolix.lixoft.com/statistical-model/individual-model/iov-2/ (accessed on 15 September 2023).
- Bailey, J.M. Context-sensitive half-times: What are they and how valuable are they in anaesthesiology? Clin. Pharmacokinet. 2002, 41, 793–799. [Google Scholar] [CrossRef]
- Grant, I.S.; Nimmo, W.S.; Clements, J.A. Pharmacokinetics and analgesic effects of i.m. and oral ketamine. Br. J. Anaesth. 1981, 53, 805–810. [Google Scholar] [CrossRef]
- Shimoyama, M.; Shimoyama, N.; Gorman, A.L.; Elliott, K.J.; Inturrisi, C.E. Oral ketamine is antinociceptive in the rat formalin test: Role of the metabolite, norketamine. Pain. 1999, 81, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Holtman, J.R., Jr.; Crooks, P.A.; Johnson-Hardy, J.K.; Hojomat, M.; Kleven, M.; Wala, E.P. Effects of norketamine enantiomers in rodent models of persistent pain. Pharmacol. Biochem. Behav. 2008, 90, 676–685. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Kobayashi, S.; Nakao, K.; Dong, C.; Han, M.; Qu, Y.; Ren, Q.; Zhang, J.C.; Ma, M.; Toki, H.; et al. AMPA Receptor Activation-Independent Antidepressant Actions of Ketamine Metabolite (S)-Norketamine. Biol. Psychiatry 2018, 84, 591–600. [Google Scholar] [CrossRef]
- Leung, A.; Wallace, M.S.; Ridgeway, B.; Yaksh, T. Concentration-effect relationship of intravenous alfentanil and ketamine on peripheral neurosensory thresholds, allodynia and hyperalgesia of neuropathic pain. Pain 2001, 91, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.H. Injectable anesthetics. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2015; pp. 283–287. [Google Scholar]
- Short, B.; Dong, V.; Galvez, V.; Vulovic, V.; Martin, D.; Bayes, A.J.; Zarate, C.A.; Murrough, J.W.; McLoughlin, D.M.; Riva-Posse, P.; et al. Development of the Ketamine Side Effect Tool (KSET). J. Affect. Disord. 2020, 266, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Highland, J.N.; Farmer, C.A.; Zanos, P.; Lovett, J.; Zarate, C.A., Jr.; Moaddel, R.; Gould, T.D. Sex-dependent metabolism of ketamine and (2R,6R)-hydroxynorketamine in mice and humans. J. Psychopharmacol. 2022, 36, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Saland, S.K.; Kabbaj, M. Sex Differences in the Pharmacokinetics of Low-dose Ketamine in Plasma and Brain of Male and Female Rats. J. Pharmacol. Exp. Ther. 2018, 367, 393–404. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S-Ket | R-Ket | |||||
|---|---|---|---|---|---|---|
| Fixed Effect | Covariate | Random Effect (γ IOV) | Fixed Effect | Covariate | Random Effect (γ IOV) | |
| VS/R-1 (L kg−1) | 1.05 | 1.52 | ||||
| VS/R-2 (L kg−1) | 2.82 | 4.14 | ||||
| ClS/R-12 (L kg−1 min−1) | 0.18 | 0.88 | 0.16 | 0.92 | ||
| ClS/R-e (L kg−1 min−1) | 0.42 | −0.13·BW | 0.4 | 0.11 | 0.46 | |
| ClS/R-1N (L kg−1 min−1) | 0.062 | 0.36 | 0.016 | +0.11·BW | 0.25 | |
| ClS/R-Ne (L kg−1 min−1) | 0.079 | 0.091 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pargätzi, G.; Bergadano, A.; Spadavecchia, C.; Theurillat, R.; Thormann, W.; Levionnois, O.L. Stereoselective Pharmacokinetics of Ketamine Administered at a Low Dose in Awake Dogs. Animals 2024, 14, 1012. https://doi.org/10.3390/ani14071012
Pargätzi G, Bergadano A, Spadavecchia C, Theurillat R, Thormann W, Levionnois OL. Stereoselective Pharmacokinetics of Ketamine Administered at a Low Dose in Awake Dogs. Animals. 2024; 14(7):1012. https://doi.org/10.3390/ani14071012
Chicago/Turabian StylePargätzi, Gwenda, Alessandra Bergadano, Claudia Spadavecchia, Regula Theurillat, Wolfgang Thormann, and Olivier L. Levionnois. 2024. "Stereoselective Pharmacokinetics of Ketamine Administered at a Low Dose in Awake Dogs" Animals 14, no. 7: 1012. https://doi.org/10.3390/ani14071012
APA StylePargätzi, G., Bergadano, A., Spadavecchia, C., Theurillat, R., Thormann, W., & Levionnois, O. L. (2024). Stereoselective Pharmacokinetics of Ketamine Administered at a Low Dose in Awake Dogs. Animals, 14(7), 1012. https://doi.org/10.3390/ani14071012