
Feline Facial Spindle Cell Tumors in 29 Cats: Histomorphological and Immunohistochemical Characterization
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Sampling and HE-Findings
2.2. Immunohistochemistry
2.3. PCR for Bovine Papillomavirus 14 (BPV14)
2.4. Follow-Up
3. Results
3.1. Clinical Findings
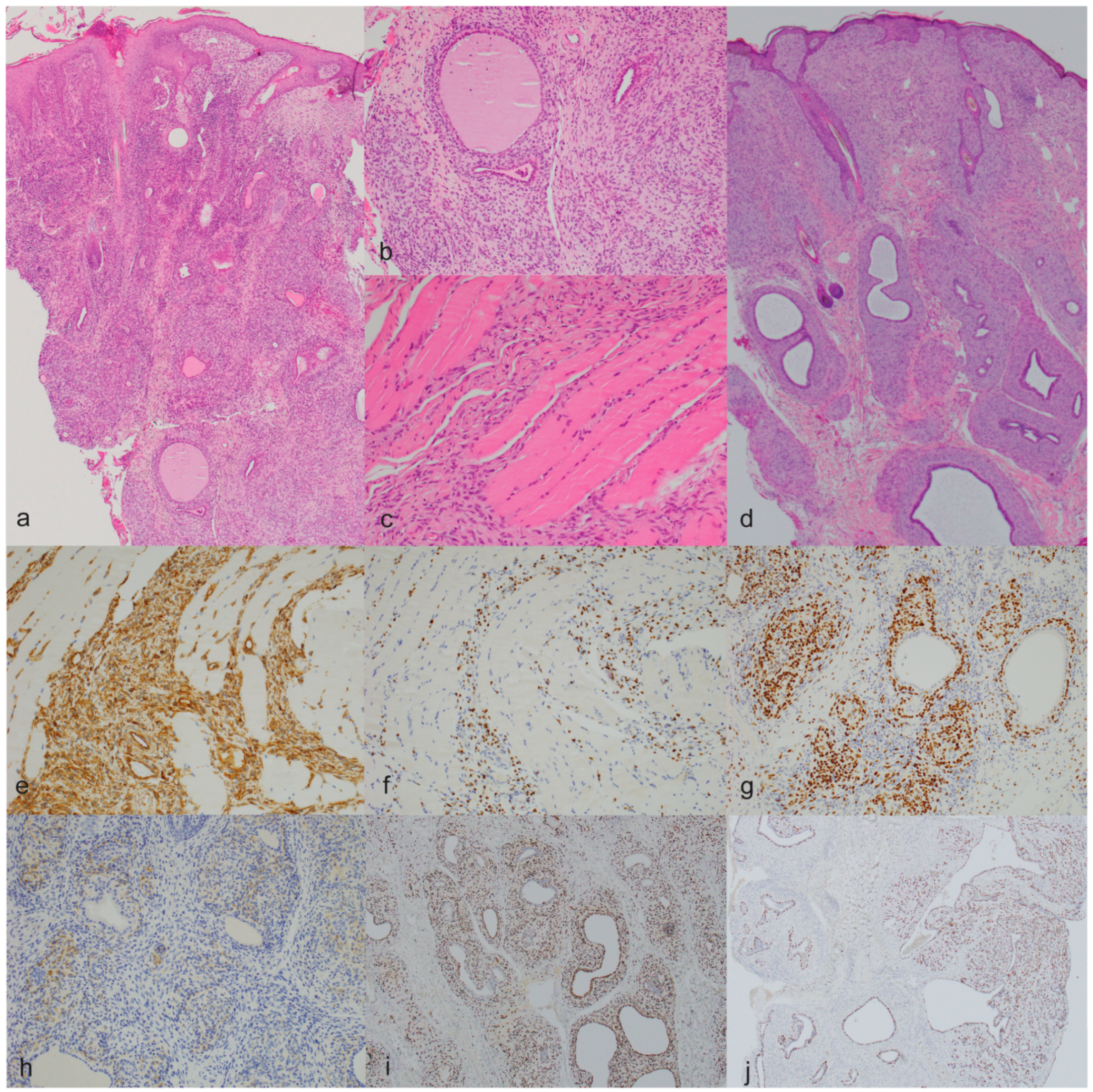
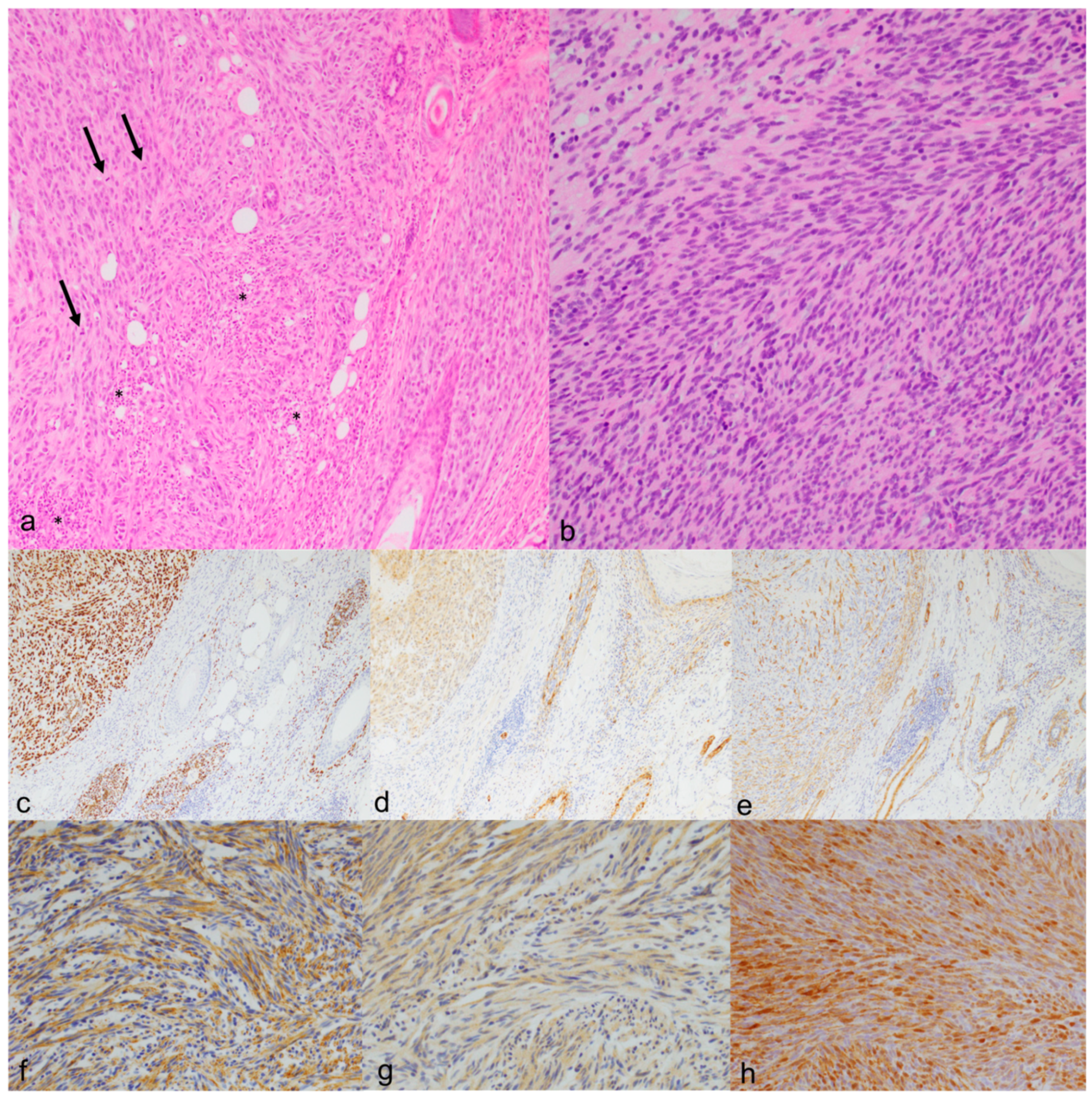
3.2. Pathological Findings
3.3. PCR for Bovine Papillomavirus 14 (BPV14)
3.4. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dennis, M.M.; McSporran, K.D.; Bacon, N.J.; Schulman, F.Y.; Foster, R.A.; Powers, B.E. Prognostic factors for cutaneous and subcutaneous soft tissue sarcomas in dogs. Vet. Pathol. 2011, 48, 73–84. [Google Scholar] [CrossRef]
- Dobromylskyj, M. Feline Soft Tissue Sarcomas: A Review of the Classification and Histological Grading, with Comparison to Human and Canine. Animals 2022, 12, 2736. [Google Scholar] [CrossRef]
- Mauldin, G.N. Soft tissue sarcomas. Radiat. Oncol. 1997, 27, 139–148. [Google Scholar] [CrossRef]
- Avallone, G.; Stefanello, D.; Ferrari, R.; Roccabianca, P. The controversial histologic classification of canine subcutaneous whorling tumours: The path to perivascular wall tumours. Vet. Comp. Oncol. 2020, 18, 3–8. [Google Scholar] [CrossRef]
- Hendrick, M.J. Mesenchymal Tumors of the Skin and Soft Tissues. In Tumors of Domestic Animals; Meuten, D.J., Ed.; Wiley Blackwell: Ames, IA, USA, 2017; pp. 142–175. [Google Scholar]
- Trojani, M.; Contesso, G.; Coindre, J.M.; Rouesse, J.; Bui, N.B.; De Mascarel, A.; Goussot, J.F.; David, M.; Bonichon, F.; Lagarde, C. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int. J. Cancer 1984, 33, 37–42. [Google Scholar] [CrossRef]
- Munday, J.S.; Sharp, C.R.; Beatty, J.A. Novel viruses: Update on the significance of papillomavirus infections in cats. J. Feline Med. Surg. 2019, 21, 409–418. [Google Scholar] [CrossRef]
- Wood, C.J.; Selmic, L.E.; Schlag, A.N.; Bacmeister, C.; Séguin, B.; Culp, W.T.; Ayres, S.A.; Sumner, J.P.; Byer, B.; Mayer, U.K.; et al. Biological behaviour and clinical outcome in 42 cats with sarcoids (cutaneous fibropapillomas). Vet. Comp. Oncol. 2020, 18, 699–705. [Google Scholar] [CrossRef]
- Munday, J.S.; Thomson, N.A. Papillomaviruses in domestic cats. Viruses 2021, 13, 1664. [Google Scholar] [CrossRef]
- Roccabianca, P.; Schulman, F.Y.; Avallone, G.; Foster, R.A.; Scruggs, J.L.; Dittmer, K.; Kiupel, M. Surgical Pathology of Tumors of Domestic Animals, Vol 3: Tumors of Soft Tissue; International Histologic Classification of Tumors of Soft Tissues of Domestic Animals; Kiupel, M., Ed.; Davis-Thompson Foundation: Washington DC, USA, 2020. [Google Scholar]
- Dobromylskyj, M.J.; Richards, V.; Smith, K.C. Prognostic factors and proposed grading system for cutaneous and subcutaneous soft tissue sarcomas in cats, based on a retrospective study. J. Feline Med. Surg. 2021, 23, 168–174. [Google Scholar] [CrossRef]
- Munday, J.S.; Knight, C.G.; Howe, L. The same papillomavirus is present in feline sarcoids from North America and New Zealand but not in any non-sarcoid feline samples. J. Vet. Diagn. Invest. 2010, 22, 97–100. [Google Scholar] [CrossRef]
- Kiefer, C.; Tobler, K.; Ramsauer, A.S.; Biegel, U.; Kuehn, N.; Ruetten, M. Feline sarcoid in a 1-year-old domestic short-haired cat caused by bovine papillomavirus type 14 in Switzerland. Schweiz. Arch. Tierheilkd. 2017, 159, 487–491. [Google Scholar] [CrossRef]
- Schulman, F.Y.; Krafft, A.E.; Janczewski, T. Feline Cutaneous Fibropapillomas: Clinicopathologic Findings and Association with Papillomavirus Infection. Vet. Pathol. 2001, 38, 291–296. [Google Scholar] [CrossRef]
- Munday, J.S.; Kiupel, M. Papillomavirus-associated cutaneous neoplasia in mammals. Vet. Pathol. 2010, 47, 254–264. [Google Scholar] [CrossRef]
- Teifke, J.P.; Kidney, B.A.; Löhr, C.V.; Yager, J.A. Detection of papillomavirus-DNA in mesenchymal tumour cells and not in the hyperplastic epithelium of feline sarcoids. Vet. Dermatol. 2003, 14, 47–56. [Google Scholar] [CrossRef]
- Mandara, M.T.; Fabriani, E.; Pavone, S.; Pumarola, M. Feline cutaneous nerve sheath tumours: Histological features and immunohistochemical evaluations. Res. Vet. Sci. 2013, 95, 548–555. [Google Scholar] [CrossRef]
- Cronin, J.C.; Loftus, S.K.; Baxter, L.L.; Swatkoski, S.; Gucek, M.; Pavan, W.J. Identification and functional analysis of SOX10 phosphorylation sites in melanoma. PLoS ONE 2018, 13, e0190834. [Google Scholar] [CrossRef]
- Nonaka, D.; Chiriboga, L.; Rubin, B.P. Sox10: A Pan-Schwannian and Melanocytic Marker. Am. J. Surg. Pathol. 2008, 32, 1291–1298. [Google Scholar] [CrossRef]
- Porcellato, I.; Orlandi, M.; Lo Giudice, A.; Sforna, M.; Mechelli, L.; Brachelente, C. Canine melanocytes: Immunohistochemical expression of melanocytic markers in different somatic areas. Vet. Dermatol. 2023, 34, 284–297. [Google Scholar] [CrossRef]
- Ramos-Vara, J.A.; Borst, L.K. Immunohistochemistry: Fundamentals and Applications in Oncology. In Tumors of Domestic Animals; Meuten, D.J., Ed.; Wiley Blackwell: Ames, IA, USA, 2017; pp. 44–87. [Google Scholar]
- Tsoi, M.F.; Thaiwong, T.; Smedley, R.C.; Noland, E.; Kiupel, M. Quantitative Expression of TYR, CD34, and CALD1 Discriminates Between Canine Oral Malignant Melanomas and Soft Tissue Sarcomas. Front. Vet. Sci. 2021, 8, 701457. [Google Scholar] [CrossRef]
- Huajun, J.; Wei, Q.; Yuxuan, W.; Jingjing, Y. Intraosseous schwannoma of the proximal humerus with pathologic fracture. Eur. J. Med. Res. 2021, 26, 72. [Google Scholar] [CrossRef]
- Higgins, R.J.; Bollen, A.W.; Dickinson, P.J.; Siso-Llonch, S. Tumors of the Nervous System. In Tumors of Domestic Animals; Meuten, D.J., Ed.; Wiley Blackwell: Ames, IA, USA, 2017; pp. 834–891. [Google Scholar]
- Stilwell, J.M.; Rissi, D.R. Pathology and immunohistochemistry of a malignant nerve sheath tumor in a pig: Case report and brief review of the literature. J. Vet. Diagn. Investig. 2019, 31, 122–127. [Google Scholar] [CrossRef]
- Chen, V.S.; Bollen, A.W.; Marco-Salazar, P.; Higgins, R.J.; Sisó, S. Case Report: Neuroblastoma-Like Schwannoma in a Domestic Short-Haired Cat. Front. Vet. Sci. 2022, 9, 905302. [Google Scholar] [CrossRef]
- Hasegawa, D.; Aoshima, K.; Sasaoka, K.; Kobayashi, A.; Takiguchi, M.; Kimura, T. Malignant oligoastrocytoma in the spinal cord of a cat. J. Vet. Med. Sci. 2022, 84, 1277–1282. [Google Scholar] [CrossRef]
- Reck, A.; Kessler, M. Melanocytic tumours of the nasal planum in cats: 10 cases (2004–2019). J. Small Anim. Pract. 2021, 62, 131–136. [Google Scholar] [CrossRef]
- Sabattini, S.; Renzi, A.; Albanese, F.; Fantinati, M.; Rigillo, A.; Abramo, F.; Tornago, R.; Tortorella, G.; Massaro, M.; Pagano, T.B.; et al. Evaluation of Ki-67 expression in feline non-ocular melanocytic tumours. BMC Vet. Res. 2018, 14, 309. [Google Scholar] [CrossRef]
- Van Raamsdonk, C.D.; Deo, M. Links between Schwann cells and melanocytes in development and disease. Pigment Cell Melanoma Res. 2013, 26, 634–645. [Google Scholar] [CrossRef]
- Chamel, G.; Abadie, J.; Albaric, O.; Labrut, S.; Ponce, F.; Ibisch, C. Non-ocular melanomas in cats: A retrospective study of 30 cases. J. Feline Med. Surg. 2017, 19, 351–357. [Google Scholar] [CrossRef]
- Ramos-Vara, J.A.; Miller, M.A.; Johnson, G.C.; Turnquist, S.E.; Kreeger, J.M.; Watson, G.L. BRIEF COMMUNICATIONS and CASE REPORTS Melan A and S100 Protein Immunohistochemistry in Feline Melanomas: 48 Cases. Vet. Pathol. 2002, 39, 127–132. [Google Scholar] [CrossRef]
- Smith, S.H.; Goldschmidt, M.H.; Mcmanus, P.M. A Comparative Review of Melanocytic Neoplasms. Vet. Pathol. 2002, 39, 651–678. [Google Scholar] [CrossRef]
- Day, M.J.; Lucke, V.M. Melanocvtic neoplasiii-in the cat. J. Small Anim. Pract. 1995, 36, 207–213. [Google Scholar] [CrossRef]
- Luna, L.D.; Higginbotham, M.L.; Henry, C.J.; Turnquist, S.E.; Moore, A.S.; Graham, J.C. Feline non-ocular melanoma: A retrospective study of 23 cases (1991-1999). J. Feline Med. Surg. 2000, 2, 173–181. [Google Scholar] [CrossRef]
- van der Linde-Sipman, J.S.; de Wit, M.M.; van Garderen, E.; Molenbeek, R.F.; van der Velde-Zimmermann, D.; de Weger, R.A. Cutaneous malignant melanomas in 57 cats: Identification of (amelanotic) signet-ring and balloon cell types and verification of their origin by immunohistochemistry, electron microscopy, and in situ hybridization. Vet. Pathol. 1997, 34, 31–38. [Google Scholar] [CrossRef]
- Buza, E.L.; Menzies, R.A.; Goldschmidt, M.H.; Durham, A.C. Malignant peripheral nerve sheath tumor in a cat with nodal and pulmonary metastases. J. Vet. Diagn. Investig. 2012, 24, 781–784. [Google Scholar] [CrossRef]
- Evans, P.M.; Lynch, G.L.; Dubielzig, R.R. Anterior uveal spindle cell tumor in a cat. Vet. Ophthalmol. 2010, 13, 387–390. [Google Scholar] [CrossRef]
- Schulman, F.Y.; Johnson, T.O.; Facemire, P.R.; Fanburg-Smith, J.C. Feline peripheral nerve sheath tumors: Histologic, immunohistochemical, and clinicopathologic correlation (59 tumors in 53 cats). Vet. Pathol. 2009, 46, 1166–1180. [Google Scholar] [CrossRef]
- Tremblay, N.; Lanevschi, A.; Doré, M.; Lanthier, I.; Desnoyers, M. Of all the nerve! A subcutaneous forelimb mass on a cat. Vet. Clin. Pathol. 2005, 34, 417–420. [Google Scholar] [CrossRef]
- Jo, V.Y.; Fletcher, C.D.M. p63 immunohistochemical staining is limited in soft tissue tumors. Am. J. Clin. Pathol. 2011, 136, 762–766. [Google Scholar] [CrossRef]
- Guisado, F.R.; Castro, P.L. Piloleiomyosarcoma in cats: Histological and immunohistochemical features. Vet. Pathol. 2022, 59, 57–62. [Google Scholar] [CrossRef]
- Carneiro, C.S.; de Queiroz, G.F.; Pinto, A.C.B.C.F.; Dagli, M.L.Z.; Matera, J.M. Feline injection site sarcoma: Immunohistochemical characteristics. J. Feline Med. Surg. 2019, 21, 314–321. [Google Scholar] [CrossRef]
- Ge, L.L.; Xing, M.Y.; Zhang, H.B.; Wang, Z.C. Neurofibroma Development in Neurofibromatosis Type 1: Insights from Cellular Origin and Schwann Cell Lineage Development. Cancers 2022, 14, 4513. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Antibody | Species | Clone | Source (1) | Antibody Dilution | Pretreatment Method (2) |
|---|---|---|---|---|---|
| Vimentin | Mouse | V9 | Dako | 1:1000 | H2(10)95 |
| Sox10 | Mouse | EP268 | Cell Marque | 1:400 | H2(40)95 |
| S100 | Mouse | EP32 | Cell Marque | 1:800 | H2(40)95 |
| GFAP | Mouse | 6F2 | Dako | 1:50 | H1(20) |
| NSE | Mouse | MRQ-55 | Cell Marque | 1:100 | H2(20)95 |
| Periaxin | Rabbit | Polyclonal | Sigma-Aldrich | 1:200 | Pressure cooker, 20 min, 98 °C, Ph9 |
| SMA | Mouse | 1A4 | Cell Marque | 1:500 | H2(20)95 |
| p63 | Mouse | 4A4 | Bio SB | 1:800 | H2(40)95 |
| MelanA | Mouse | A103 | Leica Novocastra | 1:100 | H2(20)95 |
| PNL2 | Mouse | PNL2 | Cell Marque | 1:100 | H2(20)95 |
| Case | Breed | Sex | Age | Tumors | Location | Clinical Features of the Tumor | Dead/Alive | Cause of Death |
|---|---|---|---|---|---|---|---|---|
| 1 | DSH | mc | 14 y | Poorly demarcated lesions | Right medial canthus, nasal bridge, nasal planum, right and left nares | Erosion, ulceration and crusts | Dead | Euthanasia (cardiomyopathy) |
| 2 | Maine Coon | fc | 3 y | 1 | Nasal planum and upper lip | Erythema and erosion evolving into mass | Dead | Euthanasia (tumor) |
| 3 | Mixed breed | mc | 12 y | 2 | Right nares/left upper lip | Ulceration and crusts evolving into mass (both) | Dead | Euthanasia (tumor) |
| 4 | Maine Coon | mc | 10 y | 1 | Lower lip | Mass | Dead | Euthanasia (tumor) |
| 5 | Canadian Sphynx | mc | 10 y | 1 | Nasal planum and nasal bridge | Mass | Dead | Unknown |
| 6 | DSH | mc | 12 y | 1 | Upper lip | Mass | Dead | Euthanasia (tumor) |
| 7 | ESH | fnc | Unknown | 1 | Forehead left | Mass | Unknown | n/a |
| 8 | DSH | mc | 13 y | 1 | Upper lip | Mass | Unknown | n/a |
| 9 | ESH | fc | 15 y | 1 | Nasal bridge | Mass | Dead | Euthanasia (tumor) |
| 10 | ESH | mc | 14 y | 2 | Left cheek/right cheek | Mass | Dead | Euthanasia (tumor) |
| 11 | DSH | mc | 14 y | 1 | Upper lip | Mass | Dead | Unknown |
| 12 | DSH | mnc | 9 y | 3 | Left medial canthus extending in upper and inferior eyelids/left upper lip/left cheek | Plaque/Mass/Mass | Dead | Unknown |
| 13 | ESH | fc | 15 y | 1 | Lip | Mass | Unknown | n/a |
| 14 | ESH | fc | 4.5 y | 1 | Nasal bridge | Mass | Unknown | n/a |
| 15 | ESH | mnc | Unknown | 1 | Lip | Mass | Unknown | n/a |
| 16 | DSH | mnc | 12 y | 1 | Lip | Mass | Unknown | n/a |
| 17 | BSH | mc | 6y | 1 | Nasal bridge | Mass | Unknown | n/a |
| 18 | ESH | fnc | 15y | 1 | Lip | Mass | Unknown | n/a |
| 19 | ESH | fc | 16 y | 1 | Lip | Mass | Unknown | n/a |
| 20 | Maine Coon | mc | 16 y | 2 | Right nare/right upper lip | Erythematous plaque with evolution into mass of the lip tumor | Dead | Euthanasia (tumor) |
| 21 | ESH | Unknown | 1 y | 1 | Left nares | Mass | Alive | n/a |
| 22 | ESH | mc | 9 y | 1 | Forehead | Mass | Dead | Euthanasia (tumor) |
| 23 | ESH | mc | 2 y | 1 | Upper lip | Mass | Alive | n/a |
| 24 | ESH | mnc | 6 m | 1 | Nasal planum | Mass | Dead | Unknown |
| 25 | ESH | mc | 12 y | 1 | Nose | Mass | Dead | Euthanasia (abdominal lymphoma) |
| 26 | BSH | fc | 9 m | 1 | Left upper lip | Mass | Alive | n/a |
| 27 | ESH | mc | 1 y | 1 | Lip | Mass | Unknown | n/a |
| 28 | ESH | fc | Unknown | 1 | Lip | Mass | Unknown | n/a |
| 29 | ESH | mnc | 2.5 y | 1 | Lip | Mass | Unknown | n/a |
| Case | Tumor | Histopathological Diagnosis (HE-Based) | Histo Grade a | Whorling b | BPV 14 | Vim. | Sox10 | S100 | GFAP | NSE | Periaxin | MelanA | PNL2 | SMA | p63 | Final Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cat 1 | 1 | STS | 1 | Yes | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| Cat 2 | 2 | STS | 2 | NI | Neg. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| Cat 3 | 3 | STS | 1 | Yes | I | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| 4 | STS | 1 | Yes | I | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST | |
| Cat 4 | 5 | Feline sarcoid | 2 | No | I | Pos. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| Cat 5 | 6 | STS vs. AM | 3 | No | Neg. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Pos. | Neg. | PNST |
| Cat 6 | 7 | STS | 1 | Yes | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Pos. | PNST |
| Cat 7 | 8 | Feline sarcoid | 1 | Yes | Neg. | Pos. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| Cat 8 | 9 | STS | 1 | NI | Neg. | Pos. | Pos. | Pos. | Neg. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| Cat 9 | 10 | STS | 2 | NI | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Pos. | PNST |
| Cat 10 | 11 | STS | 1 | Yes | Neg. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | Pos. | Neg. | PNST |
| 12 | STS | 1 | No | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | NA | Neg. | Neg. | Neg. | Neg. | PNST | |
| Cat 11 | 13 | Feline sarcoid | 2 | Yes | Neg. | Pos. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Pos. | Pos. | PNST |
| Cat 12 | 14 | Feline sarcoid | 1 | No | Neg. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| 15 | Feline sarcoid | 1 | No | Neg. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST | |
| 16 | Feline sarcoid | 1 | Yes | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Pos. | Neg. | PNST | |
| Cat 13 | 17 | STS vs. AM | 3 | Yes | Neg. | Pos. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Pos. | Neg. | PNST |
| Cat 14 | 18 | STS | 1 | No | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| Cat 15 | 19 | STS | 1 | NI | Neg. | Pos. | Pos. | Pos. | Pos. | Pos. | Pos. | Neg. | NA | Neg. | Neg. | PNST |
| Cat 16 | 20 | STS | 1 | NI | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| Cat 17 | 21 | STS | 1 | No | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Pos. | Neg. | PNST |
| Cat 18 | 22 | STS | 2 | No | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | NA | Neg. | Neg. | PNST |
| Cat 19 | 23 | STS | 1 | No | Neg. | Pos. | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | NA | Neg. | Neg. | PNST |
| Cat 20 | 24 | STS | 1 | Yes | Neg. | Pos. | Pos. | Pos. | Pos. | Neg. | NA | Neg. | Neg. | Neg. | Neg. | PNST |
| 25 | STS | 1 | Yes | Neg. | Pos. | Pos. | Pos. | Neg. | Neg. | NA | Neg. | Neg. | Neg. | Neg. | PNST | |
| Cat 21 | 26 | Feline sarcoid | 1 | No | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | NA | Neg. | NA | Neg. | Neg. | Feline sarcoid |
| Cat 22 | 27 | STS | 1 | No | Neg. | Pos. | Neg. | Neg. | Neg. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | PNST |
| Cat 23 | 28 | Feline sarcoid | 1 | NI | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | NA | Neg. | Neg. | Feline sarcoid |
| Cat 24 | 29 | Feline sarcoid | 1 | NI | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | NA | Neg. | Neg. | Feline sarcoid |
| Cat 25 | 30 | STS | 1 | NI | Neg. | Pos. | Neg. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Pos. | Neg. | PNST |
| Cat 26 | 31 | Feline sarcoid | 1 | No | Neg. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | NA | Neg. | Neg. | Feline-sarcoid like |
| Cat 27 | 32 | Feline sarcoid | 1 | No | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | NA | Neg. | Neg. | Feline sarcoid |
| Cat 28 | 33 | STS | 1 | NI | Neg. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | Pos. | Neg. | Leiomyosarcoma |
| Cat 29 | 34 | Feline sarcoid | 1 | No | Pos. | Pos. | Neg. | Neg. | Neg. | Neg. | Neg. | Neg. | NA | Neg. | Neg. | Feline sarcoid |
| Total | 5/31 | 34/34 | 25/34 | 25/34 | 15/34 | 7/34 | 1/30 | 0/34 | 0/25 | 8/34 | 3/34 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soto, S.; Blatter, S.; Hobi, S.; Steck, M.; Lechmann, J.; Rüfenacht, S.; Kühn, N.; Ruetten, M.; Ignatenko, N.; Krudewig, C. Feline Facial Spindle Cell Tumors in 29 Cats: Histomorphological and Immunohistochemical Characterization. Animals 2024, 14, 1103. https://doi.org/10.3390/ani14071103
Soto S, Blatter S, Hobi S, Steck M, Lechmann J, Rüfenacht S, Kühn N, Ruetten M, Ignatenko N, Krudewig C. Feline Facial Spindle Cell Tumors in 29 Cats: Histomorphological and Immunohistochemical Characterization. Animals. 2024; 14(7):1103. https://doi.org/10.3390/ani14071103
Chicago/Turabian StyleSoto, Sara, Sohvi Blatter, Stefan Hobi, Marco Steck, Julia Lechmann, Silvia Rüfenacht, Nicolas Kühn, Maja Ruetten, Nataliia Ignatenko, and Christiane Krudewig. 2024. "Feline Facial Spindle Cell Tumors in 29 Cats: Histomorphological and Immunohistochemical Characterization" Animals 14, no. 7: 1103. https://doi.org/10.3390/ani14071103
APA StyleSoto, S., Blatter, S., Hobi, S., Steck, M., Lechmann, J., Rüfenacht, S., Kühn, N., Ruetten, M., Ignatenko, N., & Krudewig, C. (2024). Feline Facial Spindle Cell Tumors in 29 Cats: Histomorphological and Immunohistochemical Characterization. Animals, 14(7), 1103. https://doi.org/10.3390/ani14071103