Experiences in the Decision-Making Regarding the Place of Care of the Elderly: A Systematic Review



Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Sampling
2.3. Inclusion/Exclusion Criteria
2.4. Data Collection Process
2.5. Data Abstraction
2.6. Synthesis
2.7. Quality Appraisal
3. Results
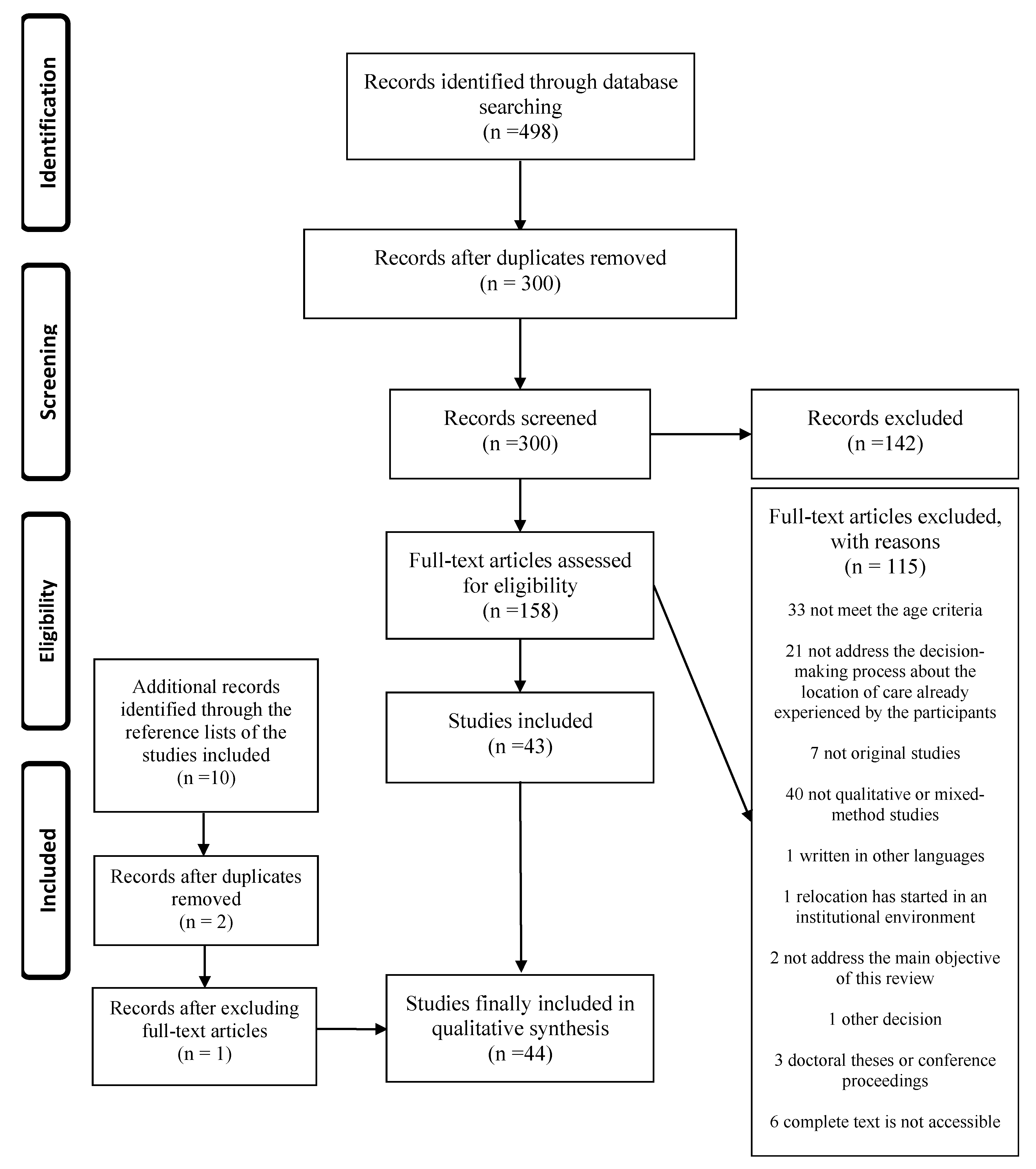
3.1. Search Results
3.2. Synthesis Results
3.3. Experiences
- -
- The elderly
- -
- Family members
- -
- Professionals
- -
- Other relevant participants
3.4. Differences between Groups
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Population Prospects 2019: Highlights. 2019. Available online: https://population.un.org/wpp/Publications/Files/WPP2019_Highlights.pdf (accessed on 5 May 2020).
- Organización Mundial de la Salud. Informe Mundial sobre el envejecimiento y la salud. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/186466/9789240694873_spa.pdf;jsessionid=54558A8AD04FB1D596ED8222A0EF33D3?sequence=1 (accessed on 5 May 2020).
- The Future Supply of Long-Term Care Workers In Relation to the Aging Baby Boom Generation: Report To Congress. 2003. Available online: https://aspe.hhs.gov/system/files/pdf/72961/ltcwork.pdf (accessed on 5 May 2020).
- Kogan, A.C.; Wilber, K.; Mosqueda, L. Person-Centered Care for Older Adults with Chronic Conditions and Functional Impairment: A Systematic Literature Review. J. Am. Geriatr. Soc. 2016, 64, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- United Nations Humans Rigths Office of the High Commissioner. United Nations Principles for Older Persons. 1991. Available online: https://www.ohchr.org/EN/ProfessionalInterest/Pages/OlderPersons.aspx (accessed on 5 May 2020).
- Schumacher, K.L.; Meleis, A.l. Theoretical development of transitions: Transitions: A central concept in nursing. In Transitions Theory: Middle-range and Situation-specific Theories in Nursing Research and Practice; Meleis, A., Ed.; Springer Publishing Company: New York, NY, USA, 2009; pp. 38–51. [Google Scholar]
- Hays, J.C. Living arrangements and health status in later life: A review of recent literature. Public Health Nurs. 2002, 19, 136–151. [Google Scholar] [CrossRef] [PubMed]
- Oswald, F.; Rowles, G.D. Beyond the relocation trauma in old age: New trends in elders’ residential decisions. In New Dynamics in Old Age: Individual, Environmental and Societal Perspectives; Wahl, H.-W., Tesch-Römer, C., Hoff, A., Eds.; Routledge: New York, NY, USA, 2017; pp. 127–152. [Google Scholar]
- Bandyopadhyay, D.; Pammi, V.S.C.; Srinivasan, N. Chapter 3—Role of affect in decision making. In Progress in Brain Research; Pammi, V.S.C., Srinivasan, N., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; Volume 202, pp. 37–53. [Google Scholar] [CrossRef]
- King, L.; Harrington, A.; Linedale, E.; Tanner, E. A mixed methods thematic review: Health-related decision-making by the older person. J. Clin. Nurs. 2018, 27, e1327–e1343. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Gemes, G.; Serrano-del-Rosal, R.; Rich-Ruiz, M. Decision-making on the location of care of the elderly: Protocol for a systematic review of qualitative studies. BMJ Open 2018, 8, e022411. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Gemes, G.; Rich-Ruiz, M.; Serrano-del-Rosal, R. Systematic review of qualitative studies on participants in the decision-making process about the location of care of the elderly. BMJ Open 2020, 10, e036551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrano-Gemes, G.; Rich-Ruiz, M.; Serrano-del-Rosal, R. Reasons for the Place of Care of the Elders: A Systematic Review. Healthcare 2020, 8, 436. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Glaser, B.G. The Constant Comparative Method of Qualitative Analysis. Soc. Probl. 1965, 12, 436–445. [Google Scholar] [CrossRef]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine Publishing Company: New York, NY, USA, 1967. [Google Scholar]
- Lockwood, C.; Porritt, K.; Munn, Z.; Rittenmeyer, L.; Salmond, S.; Bjerrum, M.; Loveday, H.; Carrier, J.; Stannard, D. Chapter 2: Systematic reviews of qualitative evidence. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Cano Arana, A.; González Gil, T.; Cabello López, J. CASPe. Plantilla para ayudarte a entender un estudio cualitativo. In CASPe. Guías CASPe de Lectura Crítica de la Literatura Médica; CASPe: Alicante, Spain, 2010; Cuaderno III; pp. 3–8. Available online: http://www.redcaspe.org/system/tdf/materiales/plantilla_cualitativa.pdf?file=1&type=node&id=147&force= (accessed on 5 May 2020).
- Butler, A.; Hall, H.; Copnell, B. A Guide to Writing a Qualitative Systematic Review Protocol to Enhance Evidence-Based Practice in Nursing and Health Care. Worldviews Evid. Based Nurs. 2016, 13, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Woods, M.; Bonas, S.; Booth, A.; Jones, D.R.; Miller, T.; Sutton, A.J.; Shaw, R.L.; Smith, J.A.; Young, B. How can systematic reviews incorporate qualitative research? A critical perspective. Qual. Res. 2006, 6, 27–44. [Google Scholar] [CrossRef]
- Ayalon, L. Intergenerational perspectives on autonomy following a transition to a continuing care retirement community. Res. Aging 2016, 38, 127–149. [Google Scholar] [CrossRef] [PubMed]
- Bekhet, A.K.; Zauszniewski, J.A.; Nakhla, W.E. Reasons for relocation to retirement communities: A qualitative study. West. J. Nurs. Res. 2009, 31, 462–479. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Rosenberg, M.W.; Wang, W.; Yang, L.; Li, H. Access to residential care in Beijing, China: Making the decision to relocate to a residential care facility. Ageing Soc. 2012, 32, 1277–1299. [Google Scholar] [CrossRef]
- Ducharme, F.; Couture, M.; Lamontagne, J. Decision-making process of family caregivers regarding placement of a cognitively impaired elderly relative. Home Health Care Serv. Q. 2012, 31, 197–218. [Google Scholar] [CrossRef]
- Gabrielsson-Jarhult, F.; Nilsen, P. On the threshold: Older people’s concerns about needs after discharge from hospital. Scand. J. Caring Sci. 2016, 30, 135–144. [Google Scholar] [CrossRef] [Green Version]
- Gottlieb, A.S.; Stoeckel, K.J.; Caro, F.G. Residential adjustment of elders: Learning from experiences with parents and peers. J. Hous. Elder. 2009, 23, 149–165. [Google Scholar] [CrossRef]
- Groger, L. Decision as process: A conceptual model of Black elders’ nursing home placement. J. Aging Stud. 1994, 8, 77–94. [Google Scholar] [CrossRef]
- Groger, L.; Kinney, J. CCRC here we come! Reasons for moving to continuing care retirement community. J. Hous. Elder. 2006, 20, 79–101. [Google Scholar] [CrossRef]
- Hartwigsen, G. Older widows and the transference of home. Int. J. Aging Hum. Dev. 1987, 25, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Heppenstall, C.P.; Keeling, S.; Hanger, H.C.; Wilkinson, T.J. Perceived factors which shape decision-making around the time of residential care admission in older adults: A qualitative study. Australas. J. Ageing 2014, 33, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Iwasiw, C.; Goldenberg, D.; MacMaster, E.; McCutcheon, S.; Bol, N. Residents’ perspectives of their first 2 weeks in a long-term care facility. J. Clin. Nurs. 1996, 5, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, C.L. Care arrangement choices for older widows: Decision participants’ perspectives. J. Women Aging 2003, 15, 127–143. [Google Scholar] [CrossRef]
- Kemp, C.L. Negotiating transitions in later life: Married couples in assisted living. J. Appl. Gerontol. 2008, 27, 231–251. [Google Scholar] [CrossRef]
- Laditka, S.B. «It Can’t Happen Soon Enough.» The Role of Readiness in Residential Moves by Older Parents. Gerontologist 2017, 57, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Lynch, J.S. The cycle of relocation: One family’s experience with elder care. Top. Adv. Pract. Nurs. eJ. 2006, 6, 1–8. Available online: https://www.medscape.com/viewarticle/549625 (accessed on 5 May 2020).
- McKenna, D.; Staniforth, B. Older people moving to residential care in Aotearoa New Zealand: Considerations for social work at practice and policy levels. Aotearoa N. Z. Soc. Work 2017, 29, 28–40. [Google Scholar] [CrossRef] [Green Version]
- Nord, C. Free choice in residential care for older people—A philosophical reflection. J. Aging Stud. 2016, 37, 59–68. [Google Scholar] [CrossRef]
- Peace, S.; Holland, C.; Kellaher, L. «Option recognition» in later life: Variations in ageing in place. Ageing Soc. 2011, 31, 734–757. [Google Scholar] [CrossRef]
- Saunders, J.C.; Heliker, D. Lessons learned from 5 women as they transition into assisted living. Geriatr. Nurs. 2008, 29, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Söderberg, M.; Ståhl, A.; Melin Emilsson, U. Independence as a stigmatizing value for older people considering relocation to a residential home. Eur. J. Soc. Work 2013, 16, 391–406. [Google Scholar] [CrossRef] [Green Version]
- Vasara, P. Not ageing in place: Negotiating meanings of residency in age-related housing. J. Aging Stud. 2015, 35, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.; McNamara, B. Relocating to retirement living: An occupational perspective on successful transitions. Aust. Occup. Ther. J. 2013, 60, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.M.; Vihos, J.; Hewitt, J.A.; Barnes, N.; Peterson, K.; Magnus, R. Examining waiting placement in hospital: Utilization and the lived experience. Glob. J. Health Sci. 2013, 6, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Brown, J.W.; Mefford, L.C.; de La Roche, A.; McLain, A.M.; Haun, M.W.; Persell, D.J. Elders’ decisions to enter assisted living facilities: A grounded theory study. J. Hous. Elder. 2008, 22, 86–103. [Google Scholar] [CrossRef]
- Couture, M.; Ducharme, F.; Lamontagne, J. The Role of Health care Professionals in the Decision-Making Process of Family Caregivers Regarding Placement of a Cognitively Impaired Elderly Relative. Home Health Care Manag. Pract. 2012, 24, 283–291. [Google Scholar] [CrossRef]
- Ewen, H.H.; Chahal, J. Influence of Late Life Stressors on the Decisions of Older Women to Relocate into Congregate Senior Housing. J. Hous. Elder. 2013, 27, 392–408. [Google Scholar] [CrossRef] [Green Version]
- Jorgensen, D.; Arksey, H.; Parsons, M.; Senior, H.; Thomas, D. Why do older people in New Zealand enter residential care rather than choosing to remain at home, and who makes that decision? Ageing Int. 2009, 34, 15–32. [Google Scholar] [CrossRef]
- Koenig, T.L.; Lee, J.H.; Macmillan, K.R.; Fields, N.L.; Spano, R. Older adult and family member perspectives of the decision-making process involved in moving to assisted living. Qual. Soc. Work 2014, 13, 335–350. [Google Scholar] [CrossRef]
- Löfqvist, C.; Granbom, M.; Himmelsbach, I.; Iwarsson, S.; Oswald, F.; Haak, M. Voices on relocation and aging in place in very old age—A complex and ambivalent matter. Gerontologist 2013, 53, 919–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Söderberg, M.; Ståhl, A.; Melin Emilsson, U. Family members’ strategies when their elderly relatives consider relocation to a residential home—Adapting, representing and avoiding. J. Aging Stud. 2012, 26, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Tyvimaa, T.; Kemp, C.L. Finnish Seniors’ Move to a Senior House: Examining the Push and Pull Factors. J. Hous. Elder. 2011, 25, 50–71. [Google Scholar] [CrossRef]
- Vassallo, T. Systemic therapy and aged respite care: A neglected area. Aust. N. Z. J. Fam. Ther. 1995, 16, 73–80. [Google Scholar] [CrossRef]
- Caron, C.D.; Ducharme, F.; Griffith, J. Deciding on institutionalization for a relative with dementia: The most difficult decision for caregivers. Can. J. Aging Rev. Can. Vieil. 2006, 25, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Dellasega, C.; Mastrian, K. The process and consequences of institutionalizing an elder. West. J. Nurs. Res. 1995, 17, 123–136. [Google Scholar] [CrossRef]
- Dellasega, C.; Nolan, M. Admission to care: Facilitating role transition amongst family carers. J. Clin. Nurs. 1997, 6, 443–451. [Google Scholar] [CrossRef]
- Fjelltun, A.-M.S.; Henriksen, N.; Norberg, A.; Gilje, F.; Normann, H.K. Carers’ and nurses’ appraisals of needs of nursing home placement for frail older in Norway. J. Clin. Nurs. 2009, 18, 3079–3088. [Google Scholar] [CrossRef]
- Kao, H.F.; Stuifbergen, A.K. Family experiences related to the decision to institutionalize an elderly member in Taiwan: An exploratory study. Soc. Sci. Med. 1999, 49, 1115–1123. [Google Scholar] [CrossRef]
- Koplow, S.M.; Gallo, A.M.; Knafl, K.A.; Vincent, C.; Paun, O.; Gruss, V. Family Caregivers Define and Manage the Nursing Home Placement Process. J. Fam. Nurs. 2015, 21, 469–493. [Google Scholar] [CrossRef]
- Mamier, I.; Winslow, B.W. Divergent views of placement decision-making: A qualitative case study. Issues Ment. Health Nurs. 2014, 35, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Butcher, H.K.; Maas, M.L. A thematic analysis of Korean family caregivers’ experiences in making the decision to place a family member with dementia in a long-term care facility. Res. Nurs. Health 2004, 27, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, B.L. Family members’ experiences with the nursing home placement of an older adult. Appl. Nurs. Res. 1997, 10, 57–63. [Google Scholar] [CrossRef]
- Chang, Y.-P.; Schneider, J.K. Decision-making process of nursing home placement among Chinese family caregivers. Perspect. Psychiatr. Care 2010, 46, 108–118. [Google Scholar] [CrossRef]
- Légaré, F.; Stacey, D.; Brière, N.; Robitaille, H.; Lord, M.-C.; Desroches, S.; Drolet, R. An interprofessional approach to shared decision making: An exploratory case study with family caregivers of one IP home care team. Bmc Geriatr. 2014, 14, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamiya, N.; Chen, L.-M.; Sugisawa, H. Caregivers’ decisions on placement of family members in long-term care facilities in Japan: Analysis of caregiver interviews. Soc. Behav. Pers. 2009, 37, 393–410. [Google Scholar] [CrossRef]
- Lee, D.T.F.; Woo, J.; Mackenzie, A.E. A review of older people’s experiences with residential care placement. J. Adv. Nurs. 2002, 37, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Fjordside, S.; Morville, A. Factors influencing older people’s experiences of participation in autonomous decisions concerning their daily care in their own homes: A review of the literature. Int. J. Older People Nurs. 2016, 11, 284–297. [Google Scholar] [CrossRef]
- Rossen, E.K.; Knafl, K.A. Women’s Well-Being After Relocation to Independent Living Communities. West. J. Nurs. Res. 2007, 29, 183–199. [Google Scholar] [CrossRef]
- Maust, D.T.; Blass, D.M.; Black, B.S.; Rabins, P.V. Treatment decisions regarding hospitalization and surgery for nursing home residents with advanced dementia: The CareAD Study. Int. Psychogeriatr. 2008, 20, 406–418. [Google Scholar] [CrossRef]
- Jacobson, J.; Gomersall, J.S.; Campbell, J.; Hughes, M. Carers’ experiences when the person for whom they have been caring enters a residential aged care facility permanently: A systematic review. JBI Database System Rev. Implement. Rep. 2015, 13, 241–317. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. [Data last updated: 10/01/2021, 10:14am CET]. Available online: https://covid19.who.int/ (accessed on 11 January 2021).
- CDC Centers for Disease Control and Prevention. Your Health: Older Adults. [Data last updated: 13/12/2020]. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html#:~:text=The%20risk%20for%20severe%20illness,older%20adults%20at%20highest%20risk.&text=need%20to%20know-,Risk%20for%20severe%20illness%20with%20COVID%2D19%20increases%20with%20age,increase%20risk%20for%20severe%20illness (accessed on 11 January 2021).


{kind=link}
| Population: Type of Experience | Experience | Situations to Which This Experience Refers |
|---|---|---|
| Elders: positive experiences [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45] | Crave for the location [24,25,30,31,33,36,39,45] | They were ready for it [24,25,30,31,33,36,39] Q1 [36] |
| After having participated in the decision together with their family [45] Q2 [45] | ||
| Previous experiences [25,27,28,29,30,31] | Due to experiences in relation to the care and/or relocation of a known relative [27,28,29,30,31] Q3 [30] | |
| Previous personal relocation experiences (of the elderly person himself/herself) [25] | ||
| Feeling support [32,33,35,38,39] | From other people [32,35,38,39]: -Practical and emotional support from family and/or friends [32,35,38] -Professional support [32,38,39] | |
| For themselves [33,38]: -Their way of thinking [33] -Their way of being [38] -Their faith [38] |
| Population: Type of Experience | Experience | Situations to Which This Experience Refers |
|---|---|---|
| Elders: negative experiences [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54] | Fear [24,27,28,30,32,34,39,42,49,51,52,53,54] | At the mere mention of the possibility of relocation [52] |
| To their future [28] | ||
| Of being a burden to their family [30] Q4 [30] | ||
| Of having to rely on support or use places of care that they thought they could not afford [27] Q5 [27] | ||
| Of the loss of autonomy/to dependence [42,51] Q6 [42] | ||
| For their safety and other matters [34,39,49,54]: With special attention to falls [39,49] | ||
| Of isolation/loneliness [32,53] Q7 [32] | ||
| Concern [23,25,27,31,34,39,40,41,42,48,51] | For their future [27,31] | |
| For the home itself [27,34] | ||
| For relocation [39,41] | ||
| For the new place of care [51] | ||
| For the organization/costs [23,27,40,42] | ||
| For their family [27,48] | ||
| For losing autonomy/for dependence [25,27,40] | ||
| With regards to their safety [34,39] | ||
| Difficulty, in relation to several aspects. [24,25,27,30,35,39,40,43,44,54] | To the relocation [24,30,39,54] Q8 [24] | |
| To their home [24,30,43,44] Q9 [24] | ||
| To the organization and costs [27,40] | ||
| To the little time within which the decision was made [35] | ||
| Not knowing what to choose [25,27] | ||
| To the stigmas associated with age [43] | ||
| Being a problematic decision [27,43] |
| Population: Type of Experience | Experience | Situations to Which This Experience Refers |
|---|---|---|
| Family: positive experiences [23,25,26,32,34,35,36,37,40,47,52,54,55,56,57,58,59,60,61,62,63] | The support of the professionals [26,37,47,52,55] | In the care [37,55] |
| With positive interactions and/or feelings between family and professionals [37,47,52,55] | ||
| Taking care of family dynamics, improving communication between family members [47] | ||
| Regarding the operation of the system [37,47] | ||
| In the decision itself [26,37,47,55] Q10 [47] | ||
| Informal network support [26,55,56,61,62] | In the care experience [55] Q11 [55] | |
| Helping to confirm if the current environment meets the needs of the elderly person [26] | ||
| In the search for help and solutions [61] | ||
| Being supported in their decision by other relatives [62] | ||
| Validating the decisions made recognizing the appropriateness of the decision [56] Q12 [56] | ||
| Relief [37,57,58,62] | By keeping the elderly person at home by activating external help [37] | |
| For having a nursing home placement offer [58] | ||
| For family support for the decision [62] | ||
| For the admission decision [57] |
| Population: Type of Experience | Experience | Situations to Which This Experience Refers |
|---|---|---|
| Family: negative experiences [23,24,25,26,27,30,32,34,35,36,37,38,39,47,49,50,52,54,55,56,57,58,59,60,61,62,63,64,65,66] | Concern [23,24,25,26,30,35,36,38,39,47,49,50,55,57,58,59,60,61,62,63,64,65,66] | About the decision of their elderly people to relocate [25] |
| About the relocation process [38] | ||
| About the elder [24,26,30,36,39,47,50,55,58,60,62,63,65] | ||
| About the carer’s situation [26,49,58,62,66] | ||
| About the family [62,64] | ||
| About others who face the location situation [63] Q13 [63] | ||
| About the different costs [23,35,57,58,61,62,63,64,65] Q14 [35] | ||
| About the opinions of others [62,64] Q15 [62] | ||
| About the new location of the elderly person [57,58,60,63,64] | ||
| About other people (outside the family) caring for the elder [49,59] Q16 [49] | ||
| Difficulty [24,26,37,47,49,52,55,56,57,59,60,61,62,63,64,65,66] | Regarding the care [24,26,49,56,59,60,61,62,66] | |
| Because the older person does not see the need for relocation [55] Q17 [55] | ||
| Because the carers do not understand what was happening [57] | ||
| In accepting the need for location [56,57] Q18 [56] | ||
| Due to lack of time in the decision-making process [56,63] | ||
| With the fact that it is a difficult decision [37,47,64,65] | ||
| In the decision making itself [57,64] | ||
| In deciding for the elderly person and/or feeling responsible for the elderly person [26,52] | ||
| In incorporating the values of the elderly in the decision making [65] | ||
| In balancing the needs of those involved [62] | ||
| Because of family dynamics [47,62,63,64] | ||
| In navigating through the health system (if collaboration with professionals is not optimal) [47] | ||
| Due to lack of information and financial concerns [57] | ||
| In related matters: how to sell/get rid of the elderly person’s house, or due to transportation [57] | ||
| In finding the right place [63] | ||
| In the placement process itself [57,60,63] | ||
| Conflict [32,34,50,54,57,59,60,61,62,63,64,65,66] | Due to the safety and independence of the elderly [34,60] Q19 [60] | |
| Within the family [50,57,62,63,64,65] Q20 [50] | ||
| With the marriage vows [61] | ||
| With the care [54] | ||
| With the expectations of society [66] | ||
| Between the needs of the elderly and their own needs [34,59,65,66] Q21 [66] | ||
| With other responsibilities [32,59,62] |
| Population: Type of Experience | Experience | Situations to Which This Experience Refers |
|---|---|---|
| Elders: unique positive experience | Happiness [30,37,39,40] | Because of how the location process was developed [39] |
| When talking about having exchanged space for security reasons [40] | ||
| For being able to take their pet to the new place of care [37] | ||
| Family: unique negative experience | Duty/Responsibility [34,58,59,60,61,62,63] | To keep the elderly person at home while possible [58] |
| Feel care/attention as a duty or responsibility [34,59,60,61,62] Q22 [59] | ||
| Feeling of responsibility for the elderly [63] | ||
| Exhaustion/feeling drained [26,32,37,47,54,55,57,58,59,61,62,64] | For reasons related to the care of the elderly [26,32,37,47,54,55,57,58,59,61,62,64] Q23 [55], Q24 [47], Q25 [26], Q26 [61]: -Making them feel unable to continue caring due to the harmful effects of care on their own health, family life, or employment [57]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrano-Gemes, G.; Serrano-del-Rosal, R.; Rich-Ruiz, M. Experiences in the Decision-Making Regarding the Place of Care of the Elderly: A Systematic Review. Behav. Sci. 2021, 11, 14. https://doi.org/10.3390/bs11020014
Serrano-Gemes G, Serrano-del-Rosal R, Rich-Ruiz M. Experiences in the Decision-Making Regarding the Place of Care of the Elderly: A Systematic Review. Behavioral Sciences. 2021; 11(2):14. https://doi.org/10.3390/bs11020014
Chicago/Turabian StyleSerrano-Gemes, Gema, Rafael Serrano-del-Rosal, and Manuel Rich-Ruiz. 2021. "Experiences in the Decision-Making Regarding the Place of Care of the Elderly: A Systematic Review" Behavioral Sciences 11, no. 2: 14. https://doi.org/10.3390/bs11020014
APA StyleSerrano-Gemes, G., Serrano-del-Rosal, R., & Rich-Ruiz, M. (2021). Experiences in the Decision-Making Regarding the Place of Care of the Elderly: A Systematic Review. Behavioral Sciences, 11(2), 14. https://doi.org/10.3390/bs11020014