
The Impact of Wildfires on Mental Health: A Scoping Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
- Reviews and subjective reports without any new objective primary data were excluded from this review.
- Studies focusing primarily on firefighters, emergency responders, or burn victims were excluded.
- Studies were excluded if the exposure was non-wildfire based or the primary outcome was not related to mental health.
- Studies with a primary outcome of schizophrenia and psychosis were excluded due to the limited number of total studies available.
2.3. Data Extraction
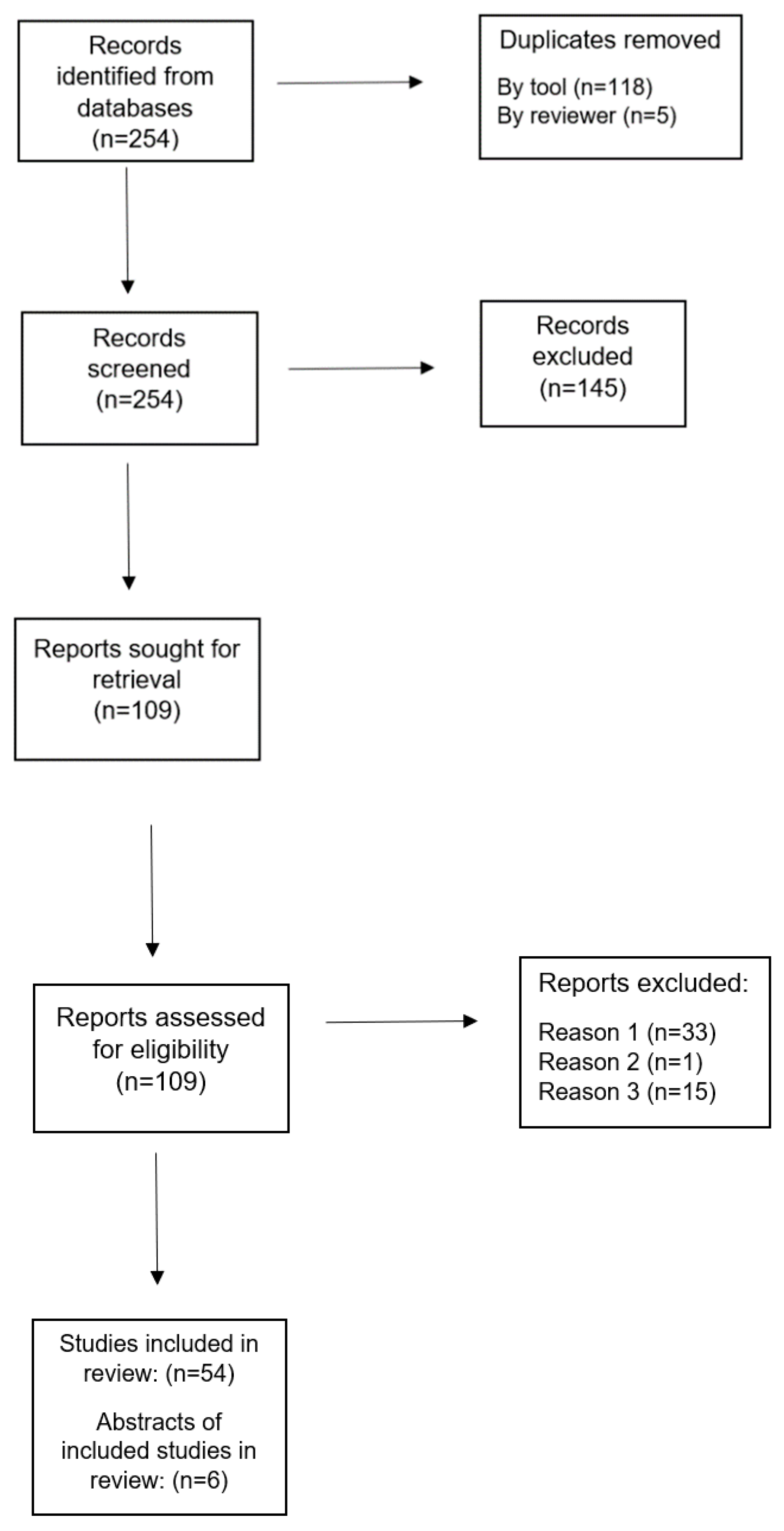
3. Results
Outcome of Literature Search
4. Discussion
4.1. Post-Traumatic Stress Disorder
4.2. Depression
4.3. Anxiety
4.4. Substance Use
4.5. Resilience
4.6. Environmentally Related Distress
4.7. Future Research
4.8. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krawisz, B. Health Effects of Climate Destabilization: Understanding the Problem. WMJ Off. Publ. State Med. Soc. Wis. 2020, 119, 132–138. [Google Scholar]
- The Combustion Process. Available online: http://www.auburn.edu/academic/forestry_wildlife/fire/combustion.htm (accessed on 7 March 2021).
- Xu, R.; Yu, P.; Abramson, M.J.; Johnston, F.H.; Samet, J.M.; Bell, M.L.; Haines, A.; Ebi, K.L.; Li, S.; Guo, Y. Wildfires, Global Climate Change, and Human Health. N. Engl. J. Med. 2020, 383, 2173–2181. [Google Scholar] [CrossRef]
- Wildfires. Available online: https://www.who.int/westernpacific/health-topics/wildfires (accessed on 4 March 2021).
- Nelson, R. US Wildfires and Mental Illness Stress Health Systems. Lancet 2020, 396, 1546–1547. [Google Scholar] [CrossRef]
- B.J. Stocks Wildfire Investigations Ltd. Evaluating Past, Current and Future Forest Fire Load Trends in Canada. 2013. Available online: https://www.ccfm.org/wp-content/uploads/2013/08/2-Fire-Load-Trends.pdf (accessed on 3 January 2021).
- Zhang, Y.; Beggs, P.J.; McGushin, A.; Bambrick, H.; Trueck, S.; Hanigan, I.C.; Morgan, G.G.; Berry, H.L.; Linnenluecke, M.K.; Johnston, F.H.; et al. The 2020 Special Report of the MJA-Lancet Countdown on Health and Climate Change: Lessons Learnt from Australia’s “Black Summer”. Med. J. Aust. 2020, 213, 490–492.e10. [Google Scholar] [CrossRef] [PubMed]
- A Cohesive Strategy is Needed to Address Catastrophic Wildfire Threats. Available online: https://www.govinfo.gov/content/pkg/CHRG-106hhrg59491/html/CHRG-106hhrg59491.htm (accessed on 4 March 2021).
- Johns, C. Wildfires, Greenhouse Gas Emissions and Climate Change; Future Directions International: Nedlands, Australia, 2020. [Google Scholar]
- Doerr, S.H.; Santín, C. Global Trends in Wildfire and Its Impacts: Perceptions versus Realities in a Changing World. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20150345. [Google Scholar] [CrossRef] [PubMed]
- Weilnhammer, V.; Schmid, J.; Mittermeier, I.; Schreiber, F.; Jiang, L.; Pastuhovic, V.; Herr, C.; Heinze, S. Extreme Weather Events in Europe and Their Health Consequences—A Systematic Review. Int. J. Hyg. Environ. Health 2021, 233, 113688. [Google Scholar] [CrossRef]
- Hrabok, M.; Delorme, A.; Agyapong, V.I.O. Threats to Mental Health and Well-Being Associated with Climate Change. J. Anxiety Disord. 2020, 76, 102295. [Google Scholar] [CrossRef] [PubMed]
- Clayer, J.R.; Bookless-Pratz, C.; Harris, R.I. Some Health Consequences of a Natural Disaster. Med. J. Aust. 1985, 143, 182–184. [Google Scholar] [CrossRef]
- Cherry, N.; Haynes, W. Effects of the Fort McMurray Wildfires on the Health of Evacuated Workers: Follow-up of 2 Cohorts. CMAJ Open 2017, 5, E638–E645. [Google Scholar] [CrossRef] [Green Version]
- Howard, C.; Rose, C.; Dodd, W.; Kohle, K.; Scott, C.; Scott, P.; Cunsolo, A.; Orbinski, J. SOS! Summer of Smoke: A Retrospective Cohort Study Examining the Cardiorespiratory Impacts of a Severe and Prolonged Wildfire Season in Canada’s High Subarctic. BMJ Open 2021, 11, e037029. [Google Scholar] [CrossRef]
- Jones, R.T.; Ribbe, D.P.; Cunningham, P.B.; Weddle, J.D.; Langley, A.K. Psychological Impact of Fire Disaster on Children and Their Parents. Behav. Modif. 2002, 26, 163–186. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.R.G.; Agyapong, V.; Greenshaw, A.J.; Cribben, I.; Brett-MacLean, P.; Drolet, J.; McDonald-Harker, C.; Omeje, J.; Mankowsi, M.; Noble, S.; et al. Significant PTSD and Other Mental Health Effects Present 18 Months After the Fort Mcmurray Wildfire: Findings From 3070 Grades 7–12 Students. Front. Psychiatry 2019, 10, 623. [Google Scholar] [CrossRef] [Green Version]
- McFarlane, A.C.; Policansky, S.K.; Irwin, C. A Longitudinal Study of the Psychological Morbidity in Children Due to a Natural Disaster. Psychol. Med. 1987, 17, 727–738. [Google Scholar] [CrossRef]
- McDermott, B.M.C.; Palmer, L.J. Post-Disaster Service Provision Following Proactive Identification of Children with Emotional Distress and Depression. Aust. N. Z. J. Psychiatry 1999, 33, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, K.R.; Feldt, B.A.; Zane, D.F.; Haywood, T.; Jones, R.W.; Horney, J.A. Longitudinal Community Assessment for Public Health Emergency Response to Wildfire, Bastrop County, Texas. Health Secur. 2016, 14, 93–104. [Google Scholar] [CrossRef]
- NIMH. U.S. Leading Categories of Diseases/Disorders. Available online: https://www.nimh.nih.gov/health/statistics/disability/us-leading-categories-of-diseases-disorders.shtml (accessed on 4 March 2021).
- Bryant, R.A.; Gibbs, L.; Colin Gallagher, H.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; Ireton, G.; Richardson, J.; et al. The Dynamic Course of Psychological Outcomes Following the Victorian Black Saturday Bushfires. Aust. N. Z. J. Psychiatry 2020, 55, 666–677. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, A.C.; Van Hooff, M. Impact of Childhood Exposure to a Natural Disaster on Adult Mental Health: 20-Year Longitudinal Follow-up Study. Br. J. Psychiatry 2009, 195, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Comtesse, H.; Ertl, V.; Hengst, S.M.C.; Rosner, R.; Smid, G.E. Ecological Grief as a Response to Environmental Change: A Mental Health Risk or Functional Response? Int. J. Environ. Res. Public Health 2021, 18, 734. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, L.A.; Wong, M. Global Climate Change and Mental Health. Curr. Opin. Psychol. 2020, 32, 12–16. [Google Scholar] [CrossRef]
- Bryant, R.A.; Waters, E.; Gibbs, L.; Gallagher, H.C.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; Snowdon, E.; et al. Psychological Outcomes Following the Victorian Black Saturday Bushfires. Aust. N. Z. J. Psychiatry 2014, 48, 634–643. [Google Scholar] [CrossRef] [Green Version]
- Adamis, D.; Papanikolaou, V.; Mellon, R.C.; Prodromitis, G.; Tyrovola, K.; Kyriopoulos, J. P-1035—Long-Term Psychological Effects of a Wildfire Disaster in Greece. Eur. Psychiatry 2012, 27, 1. [Google Scholar] [CrossRef]
- Adamis, D.; Papanikolaou, V.; Kyriopoulos, J. P-581—Quality of Life after a Wildfire Disaster in a Rural Area of Greece. Eur. Psychiatry 2012, 27, 1. [Google Scholar] [CrossRef]
- Adamis, D.; Papanikolaou, V.; Mellon, R.C.; Prodromitis, G. The Impact of Wildfires on Mental Health of Residents in a Rural Area of Greece. A Case Control Population Based Study. Eur. Psychiatry 2011, 26, 1188. [Google Scholar] [CrossRef]
- Afifi, W.A.; Felix, E.D.; Afifi, T.D. The Impact of Uncertainty and Communal Coping on Mental Health Following Natural Disasters. Anxiety Stress Coping 2012, 25, 329–347. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Hrabok, M.; Juhas, M.; Omeje, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Moosavi, S.; Brown, M.; et al. Prevalence Rates and Predictors of Generalized Anxiety Disorder Symptoms in Residents of Fort McMurray Six Months After a Wildfire. Front. Psychiatry 2018, 9, 345. [Google Scholar] [CrossRef] [Green Version]
- Agyapong, V.I.O.; Ritchie, A.; Brown, M.R.G.; Noble, S.; Mankowsi, M.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Moosavi, S.; et al. Long-Term Mental Health Effects of a Devastating Wildfire Are Amplified by Socio-Demographic and Clinical Antecedents in Elementary and High School Staff. Front. Psychiatry 2020, 11, 448. [Google Scholar] [CrossRef]
- Oral Communications. Eur. Psychiatry 2018, 48, S72–S140. [CrossRef]
- Agyapong, V.I.O.; Juhas, M.; Omege, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Brown, M.; Chue, P.; Li, X.-M.; et al. Prevalence Rates and Correlates of Likely Post-Traumatic Stress Disorder in Residents of Fort McMurray 6 Months After a Wildfire. Int. J. Ment. Health Addict. 2019, 19. [Google Scholar] [CrossRef]
- Belleville, G.; Lebel, J.; Ouellet, M.-C.; Békés, V.; Morin, C.M.; Bergeron, N.; Campbell, T.; Ghosh, S.; Bouchard, S.; Guay, S.; et al. Resilient—An Online Multidimensional Treatment to Promote Resilience and Better Sleep: A Randomized Controlled Trial. Sleep Med. 2019, 64, S214–S215. [Google Scholar] [CrossRef]
- Belleville, G.; Ouellet, M.-C.; Morin, C.M. Post-Traumatic Stress among Evacuees from the 2016 Fort McMurray Wildfires: Exploration of Psychological and Sleep Symptoms Three Months after the Evacuation. Int. J. Environ. Res. Public Health 2019, 16, 1604. [Google Scholar] [CrossRef] [Green Version]
- Binet, É.; Ouellet, M.-C.; Lebel, J.; Békés, V.; Morin, C.M.; Bergeron, N.; Campbell, T.; Ghosh, S.; Bouchard, S.; Guay, S.; et al. A Portrait of Mental Health Services Utilization and Perceived Barriers to Care in Men and Women Evacuated During the 2016 Fort McMurray Wildfires. Adm. Policy Ment. Health Ment. Health Serv. Res. 2021, 1–13. [Google Scholar] [CrossRef]
- Block, K.; Molyneaux, R.; Gibbs, L.; Alkemade, N.; Baker, E.; MacDougall, C.; Ireton, G.; Forbes, D. The Role of the Natural Environment in Disaster Recovery: “We Live Here Because We Love the Bush”. Health Place 2019, 57, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, M.R.G.; Agyapong, V.; Greenshaw, A.J.; Cribben, I.; Brett-MacLean, P.; Drolet, J.; McDonald-Harker, C.; Omeje, J.; Mankowsi, M.; Noble, S.; et al. After the Fort McMurray Wildfire There Are Significant Increases in Mental Health Symptoms in Grade 7–12 Students Compared to Controls. BMC Psychiatry 2019, 19, 18. [Google Scholar] [CrossRef] [Green Version]
- Bryant, R.A.; Creamer, M.; O’Donnell, M.; Forbes, D.; Felmingham, K.L.; Silove, D.; Malhi, G.; van Hoof, M.; McFarlane, A.C.; Nickerson, A. Separation from Parents during Childhood Trauma Predicts Adult Attachment Security and Post-Traumatic Stress Disorder. Psychol. Med. 2017, 47, 2028–2035. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Gallagher, H.C.; Gibbs, L.; Pattison, P.; MacDougall, C.; Harms, L.; Block, K.; Baker, E.; Sinnott, V.; Ireton, G.; et al. Mental Health and Social Networks After Disaster. Am. J. Psychiatry 2017, 174, 277–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryant, R.A.; Gibbs, L.; Gallagher, H.C.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; Sinnott, V.; Ireton, G.; et al. Longitudinal Study of Changing Psychological Outcomes Following the Victorian Black Saturday Bushfires. Aust. N. Z. J. Psychiatry 2018, 52, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Byrne, M.K.; Lerias, D.; Sullivan, N.L. Predicting Vicarious Traumatization in Those Indirectly Exposed to Bushfires. Stress Health 2006, 22, 167–177. [Google Scholar] [CrossRef]
- Caamano-Isorna, F.; Figueiras, A.; Sastre, I.; Montes-Martínez, A.; Taracido, M.; Piñeiro-Lamas, M. Respiratory and Mental Health Effects of Wildfires: An Ecological Study in Galician Municipalities (North-West Spain). Environ. Health 2011, 10, 48. [Google Scholar] [CrossRef] [Green Version]
- Camilleri, P.; Healy, C.; Macdonald, E.; Nicholls, S.; Sykes, J.; Winkworth, G.; Woodward, M. Recovery from Bushfires: The Experience of the 2003 Canberra Bushfires Three Years After. Australas. J. Paramed. 2010, 8. [Google Scholar] [CrossRef] [Green Version]
- Cowlishaw, S.; Metcalf, O.; Varker, T.; Stone, C.; Molyneaux, R.; Gibbs, L.; Block, K.; Harms, L.; MacDougall, C.; Gallagher, H.C.; et al. Anger Dimensions and Mental Health Following a Disaster: Distribution and Implications After a Major Bushfire. J. Trauma. Stress 2021, 34, 46–55. [Google Scholar] [CrossRef]
- Felix, E.; Afifi, T.; Kia-Keating, M.; Brown, L.; Afifi, W.; Reyes, G. Family Functioning and Posttraumatic Growth among Parents and Youth Following Wildfire Disasters. Am. J. Orthopsychiatry 2015, 85, 191–200. [Google Scholar] [CrossRef]
- Forbes, D.; Alkemade, N.; Waters, E.; Gibbs, L.; Gallagher, C.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; et al. The Role of Anger and Ongoing Stressors in Mental Health Following a Natural Disaster. Aust. N. Z. J. Psychiatry 2015, 49, 706–713. [Google Scholar] [CrossRef]
- Gallagher, H.C.; Block, K.; Gibbs, L.; Forbes, D.; Lusher, D.; Molyneaux, R.; Richardson, J.; Pattison, P.; MacDougall, C.; Bryant, R.A. The Effect of Group Involvement on Post-Disaster Mental Health: A Longitudinal Multilevel Analysis. Soc. Sci. Med. 2019, 220, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, H.C.; Lusher, D.; Gibbs, L.; Pattison, P.; Forbes, D.; Block, K.; Harms, L.; MacDougall, C.; Kellett, C.; Ireton, G.; et al. Dyadic Effects of Attachment on Mental Health: Couples in a Postdisaster Context. J. Fam. Psychol. 2017, 31, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, H.C.; Richardson, J.; Forbes, D.; Harms, L.; Gibbs, L.; Alkemade, N.; MacDougall, C.; Waters, E.; Block, K.; Lusher, D.; et al. Mental Health Following Separation in a Disaster: The Role of Attachment: Disaster-Related Separation and Attachment. J. Trauma. Stress 2016, 29, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Hashoul-Andary, R.; Assayag-Nitzan, Y.; Yuval, K.; Aderka, I.M.; Litz, B.; Bernstein, A. A Longitudinal Study of Emotional Distress Intolerance and Psychopathology Following Exposure to a Potentially Traumatic Event in a Community Sample. Cogn. Ther. Res. 2016, 40, 1–13. [Google Scholar] [CrossRef]
- Hertz-Picciotto, I. 43.3 Mental Health in Children and Adolescents Exposed to the 2017 and/or 2018 Wildfires in Northern California. J. Am. Acad. Child. Adolesc. Psychiatry 2020, 59, S66. [Google Scholar] [CrossRef]
- Hooper, J.; Magor-Blatch, L.; Bhullar, N. Life after Bushfire: Post-Traumatic Stress, Coping, Post-Traumatic Growth. Australas. J. Paramed. 2018, 15. [Google Scholar] [CrossRef] [Green Version]
- Ho, R.C.; Zhang, M.W.; Ho, C.S.; Pan, F.; Lu, Y.; Sharma, V.K. Impact of 2013 South Asian Haze Crisis: Study of Physical and Psychological Symptoms and Perceived Dangerousness of Pollution Level. BMC Psychiatry 2014, 14, 81. [Google Scholar] [CrossRef] [Green Version]
- Jones, R.T.; Ribbe, D.P.; Cunningham, P. Psychosocial Correlates of Fire Disaster among Children and Adolescents. J. Trauma. Stress 1994, 7, 117–122. [Google Scholar] [CrossRef]
- Marshall, G.N.; Schell, T.L.; Elliott, M.N.; Rayburn, N.R.; Jaycox, L.H. Psychiatric Disorders Among Adults Seeking Emergency Disaster Assistance After a Wildland-Urban Interface Fire. Psychiatr. Serv. 2007, 58, 509–514. [Google Scholar] [CrossRef]
- McDermott, B.M.; Lee, E.M.; Judd, M.; Gibbon, P. Posttraumatic Stress Disorder and General Psychopathology in Children and Adolescents Following a Wildfire Disaster. Can. J. Psychiatry 2005, 50, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Mcdermott, B.M.; Palmer, L.J. Postdisaster Emotional Distress, Depression and Event-Related Variables: Findings Across Child and Adolescent Developmental Stages. Aust. N. Z. J. Psychiatry 2002, 36, 754–761. [Google Scholar] [CrossRef]
- McFarlane, A.C.; Clayer, J.R.; Bookless, C.L. Psychiatric Morbidity Following a Natural Disaster: An Australian Bushfire. Soc. Psychiatry Psychiatr. Epidemiol. 1997, 32, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Mellon, R.C.; Papanikolau, V.; Prodromitis, G. Locus of Control and Psychopathology in Relation to Levels of Trauma and Loss: Self-Reports of Peloponnesian Wildfire Survivors: Locus of Control and Psychopathology in Relation to Levels of Trauma and Loss. J. Trauma. Stress 2009, 22, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Molyneaux, R.; Gibbs, L.; Bryant, R.A.; Humphreys, C.; Hegarty, K.; Kellett, C.; Gallagher, H.C.; Block, K.; Harms, L.; Richardson, J.F.; et al. Interpersonal Violence and Mental Health Outcomes Following Disaster. BJPsych Open 2020, 6, e1. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Copes, R.; Fisk, R.; Joy, R.; Chan, K.; Brauer, M. Population Health Effects of Air Quality Changes Due to Forest Fires in British Columbia in 2003: Estimates from Physician-Visit Billing Data. Can. J. Public Health 2006, 97, 105–108. [Google Scholar] [CrossRef]
- Moosavi, S.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Chue, P.; Greenshaw, A.J.; Silverstone, P.H.; Li, X.-M.; Agyapong, V.I.O. Mental Health Effects in Primary Care Patients 18 Months After a Major Wildfire in Fort McMurray: Risk Increased by Social Demographic Issues, Clinical Antecedents, and Degree of Fire Exposure. Front. Psychiatry 2019, 10, 683. [Google Scholar] [CrossRef]
- Papadatou, D.; Giannopoulou, I.; Bitsakou, P.; Bellali, T.; Talias, M.A.; Tselepi, K. Adolescents’ Reactions after a Wildfire Disaster in Greece. J. Trauma. Stress 2012, 25, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, V.; Adamis, D.; Mellon, R.C.; Prodromitis, G. Psychological Distress Following Wildfires Disaster in a Rural Part of Greece: A Case-Control Population-Based Study. Int. J. Emerg. Ment. Health 2011, 13, 11–26. [Google Scholar]
- Papanikolaou, V.; Leon, G.R.; Kyriopoulos, J.; Levett, J.; Pallis, E. Surveying the Ashes: Experience from the 2007 Peloponnese Wildfires Six Months after the Disaster. Prehosp. Disaster Med. 2011, 26, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Parslow, R.A.; Jorm, A.F. Tobacco Use after Experiencing a Major Natural Disaster: Analysis of a Longitudinal Study of 2063 Young Adults. Addiction 2006, 101, 1044–1050. [Google Scholar] [CrossRef]
- Parslow, R.A.; Jorm, A.F.; Christensen, H. Associations of Pre-Trauma Attributes and Trauma Exposure with Screening Positive for PTSD: Analysis of a Community-Based Study of 2085 Young Adults. Psychol. Med. 2006, 36, 387–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psarros, C.; Theleritis, C.; Economou, M.; Tzavara, C.; Kioulos, K.T.; Mantonakis, L.; Soldatos, C.R.; Bergiannaki, J.-D. Insomnia and PTSD One Month after Wildfires: Evidence for an Independent Role of the “Fear of Imminent Death”. Int. J. Psychiatry Clin. Pract. 2017, 21, 137–141. [Google Scholar] [CrossRef]
- Ritchie, A.; Sautner, B.; Omege, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Moosavi, S.; Greenshaw, A.; Chue, P.; et al. Long-Term Mental Health Effects of a Devastating Wildfire Are Amplified by Sociodemographic and Clinical Antecedents in College Students. Disaster Med. Public Health Prep. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Scher, C.D.; Ellwanger, J. Fire-Related Cognitions Moderate the Impact of Risk Factors on Adjustment Following Wildfire Disaster. J. Anxiety Disord. 2009, 23, 891–896. [Google Scholar] [CrossRef]
- Silveira, S.; Kornbluh, M.; Withers, M.C.; Grennan, G.; Ramanathan, V.; Mishra, J. Chronic Mental Health Sequelae of Climate Change Extremes: A Case Study of the Deadliest Californian Wildfire. Int. J. Environ. Res. Public Health 2021, 18, 1487. [Google Scholar] [CrossRef]
- Tally, S.; Levack, A.; Sarkin, A.J.; Gilmer, T.; Groessl, E.J. The Impact of the San Diego Wildfires on a General Mental Health Population Residing in Evacuation Areas. Adm. Policy Ment. Health Ment. Health Serv. Res. 2013, 40, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Verstraeten, B.S.E.; Elgbeili, G.; Hyde, A.; King, S.; Olson, D.M. Maternal Mental Health after a Wildfire: Effects of Social Support in the Fort McMurray Wood Buffalo Study. Can. J. Psychiatry 2020, 070674372097085. [Google Scholar] [CrossRef]
- Yelland, C.; Robinson, P.; Lock, C.; La Greca, A.M.; Kokegei, B.; Ridgway, V.; Lai, B. Bushfire Impact on Youth. J. Trauma. Stress 2010. [Google Scholar] [CrossRef]
- Zeller, M.; Yuval, K.; Nitzan-Assayag, Y.; Bernstein, A. Self-Compassion in Recovery Following Potentially Traumatic Stress: Longitudinal Study of At-Risk Youth. J. Abnorm. Child Psychol. 2015, 43, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.T.; Ribbe, D.P.; Cunningham, P.; Weddle, J.D. Psychosocial Correlates of a Wildfire Disaster: Post Disaster Adult Reactions. Fire Technol. 2003, 39, 103–117. [Google Scholar] [CrossRef]
- McFarlane, A.C. Posttraumatic Phenomena in a Longitudinal Study of Children Following a Natural Disaster. J. Am. Acad. Child Adolesc. Psychiatry 1987, 26, 764–769. [Google Scholar] [CrossRef]
- The Lancet Australia on Fire. Lancet 2020, 395, 165. [CrossRef] [Green Version]
- Reid, C.E.; Brauer, M.; Johnston, F.H.; Jerrett, M.; Balmes, J.R.; Elliott, C.T. Critical Review of Health Impacts of Wildfire Smoke Exposure. Environ. Health Perspect. 2016, 124, 1334–1343. [Google Scholar] [CrossRef] [Green Version]
- Cianconi, P.; Betrò, S.; Janiri, L. The Impact of Climate Change on Mental Health: A Systematic Descriptive Review. Front. Psychiatry 2020, 11, 74. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.R.; Adams, Z.W.; Menon, S.V.; Youngstrom, E.A.; Bunnell, B.E.; Acierno, R.; Ruggiero, K.J.; Danielson, C.K. How Should We Screen for Depression Following a Natural Disaster? An ROC Approach to Post-Disaster Screening in Adolescents and Adults. J. Affect. Disord. 2016, 202, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Eisenman, D.; McCaffrey, S.; Donatello, I.; Marshal, G. An Ecosystems and Vulnerable Populations Perspective on Solastalgia and Psychological Distress After a Wildfire. EcoHealth 2015, 12, 602–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clayton, S. Climate Anxiety: Psychological Responses to Climate Change. J. Anxiety Disord. 2020, 74, 102263. [Google Scholar] [CrossRef]
- Barlow, D.H.; Durand, V.M.; Hofmann, S.G. Abnormal Psychology: An Integrative Approach, 8th ed.; Cengage Learning: Boston, MA, USA, 2017. [Google Scholar]
- Ross, S.; Peselow, E. Co-Occurring Psychotic and Addictive Disorders: Neurobiology and Diagnosis. Clin. Neuropharmacol. 2012, 35, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Kelly, T.M.; Daley, D.C. Integrated Treatment of Substance Use and Psychiatric Disorders. Soc. Work Public Health 2013, 28, 388–406. [Google Scholar] [CrossRef]
- Shantna, K.; Chaudhury, S.; Verma, A.; Singh, A. Comorbid Psychiatric Disorders in Substance Dependence Patients: A Control Study. Ind. Psychiatry J. 2009, 18, 84. [Google Scholar] [CrossRef]
- Comorbidity of Substance Use and Mental Health Disorders in Europe (Perspectives on Drugs). Available online: https://www.emcdda.europa.eu/publications/pods/comorbidity-substance-use-mental-health (accessed on 5 March 2021).
- Friedberg, A.; Malefakis, D. Resilience, Trauma, and Coping. Psychodyn. Psychiatry 2018, 46, 81–113. [Google Scholar] [CrossRef] [Green Version]
- Windle, G. What Is Resilience? A Review and Concept Analysis. Rev. Clin. Gerontol. 2011, 21, 152–169. [Google Scholar] [CrossRef]
- Cunsolo, A.; Ellis, N.R. Ecological Grief as a Mental Health Response to Climate Change-Related Loss. Nat. Clim. Chang. 2018, 8, 275–281. [Google Scholar] [CrossRef]
- Dodd, W.; Scott, P.; Howard, C.; Scott, C.; Rose, C.; Cunsolo, A.; Orbinski, J. Lived Experience of a Record Wildfire Season in the Northwest Territories, Canada. Can. J. Public Health 2018, 109, 327–337. [Google Scholar] [CrossRef]
- Clayton, S.; Karazsia, B.T. Development and Validation of a Measure of Climate Change Anxiety. J. Environ. Psychol. 2020, 69, 101434. [Google Scholar] [CrossRef]
- Usher, K.; Durkin, J.; Bhullar, N. Eco-anxiety: How Thinking about Climate Change-related Environmental Decline Is Affecting Our Mental Health. Int. J. Ment. Health Nurs. 2019, 28, 1233–1234. [Google Scholar] [CrossRef] [PubMed]
- Parker, C.L.; Wellbery, C.E.; Mueller, M. The Changing Climate: Managing Health Impacts. Am. Fam. Physician 2019, 100, 618–626. [Google Scholar]
- Husk, K.; Lovell, R.; Cooper, C.; Stahl-Timmins, W.; Garside, R. Participation in Environmental Enhancement and Conservation Activities for Health and Well-Being in Adults: A Review of Quantitative and Qualitative Evidence. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- McFarlane, A.C.; Van Hooff, M. Learning for the Future: The Challenge of Disaster Research. Aust. N. Z. J. Psychiatry 2014, 48, 600–602. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O.; Hrabok, M.; Shalaby, R.; Vuong, W.; Noble, J.M.; Gusnowski, A.; Mrklas, K.; Li, D.; Urichuck, L.; Snaterse, M.; et al. Text4Hope: Receiving Daily Supportive Text Messages for 3 Months During the COVID-19 Pandemic Reduces Stress, Anxiety, and Depression. Disaster Med. Public Health Prep. 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O. Coronavirus Disease 2019 Pandemic: Health System and Community Response to a Text Message (Text4Hope) Program Supporting Mental Health in Alberta. Disaster Med. Public Health Prep. 2020, 14, e5–e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agyapong, V.I.O.; Hrabok, M.; Vuong, W.; Gusnowski, A.; Shalaby, R.; Mrklas, K.; Li, D.; Urichuk, L.; Snaterse, M.; Surood, S.; et al. Closing the Psychological Treatment Gap During the COVID-19 Pandemic with a Supportive Text Messaging Program: Protocol for Implementation and Evaluation. JMIR Res. Protoc. 2020, 9, e19292. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Shalaby, R.; Hrabok, M.; Vuong, W.; Noble, J.M.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; et al. Mental Health Outreach via Supportive Text Messages during the COVID-19 Pandemic: Improved Mental Health and Reduced Suicidal Ideation after Six Weeks in Subscribers of Text4Hope Compared to a Control Population. Int. J. Environ. Res. Public Health 2021, 18, 2157. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O.; Hrabok, M.; Vuong, W.; Shalaby, R.; Noble, J.M.; Gusnowski, A.; Mrklas, K.J.; Li, D.; Urichuk, L.; Snaterse, M.; et al. Changes in Stress, Anxiety, and Depression Levels of Subscribers to a Daily Supportive Text Message Program (Text4Hope) During the COVID-19 Pandemic: Cross-Sectional Survey Study. JMIR Ment. Health 2020, 7, e22423. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O.; Mrklas, K.; Suen, V.Y.M.; Rose, M.S.; Jahn, M.; Gladue, I.; Kozak, J.; Leslie, M.; Dursun, S.; Ohinmaa, A.; et al. Supportive Text Messages to Reduce Mood Symptoms and Problem Drinking in Patients with Primary Depression or Alcohol Use Disorder: Protocol for an Implementation Research Study. JMIR Res. Protoc. 2015, 4, e55. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; McLoughlin, D.M.; Farren, C.K. Six-Months Outcomes of a Randomised Trial of Supportive Text Messaging for Depression and Comorbid Alcohol Use Disorder. J. Affect. Disord. 2013, 151, 100–104. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Ahern, S.; McLoughlin, D.M.; Farren, C.K. Supportive Text Messaging for Depression and Comorbid Alcohol Use Disorder: Single-Blind Randomised Trial. J. Affect. Disord. 2012, 141, 168–176. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Mrklas, K.; Juhás, M.; Omeje, J.; Ohinmaa, A.; Dursun, S.M.; Greenshaw, A.J. Cross-Sectional Survey Evaluating Text4Mood: Mobile Health Program to Reduce Psychological Treatment Gap in Mental Healthcare in Alberta through Daily Supportive Text Messages. BMC Psychiatry 2016, 16, 378. [Google Scholar] [CrossRef] [Green Version]
- Agyapong, V.I.O.; Milnes, J.; McLoughlin, D.M.; Farren, C.K. Perception of Patients with Alcohol Use Disorder and Comorbid Depression about the Usefulness of Supportive Text Messages. Technol. Health Care 2013, 21, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Shalaby, R.; Vuong, W.; Hrabok, M.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; Cao, B.; Li, X.-M.; et al. Gender Differences in Satisfaction with a Text Messaging Program (Text4Hope) and Anticipated Receptivity to Technology-Based Health Support During the COVID-19 Pandemic: Cross-Sectional Survey Study. JMIR MHealth UHealth 2021, 9, e24184. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | N = 63 |
|---|---|
| Country of origin of study | |
| Australia | 26 |
| Canada | 14 |
| United States | 11 |
| Greece | 8 |
| Israel | 2 |
| Singapore | 1 |
| Spain | 1 |
| Type of study | |
| Cross-sectional | 42 |
| Cohort | 20 |
| Randomized Controlled Trial | 1 |
| Outcomes studied | |
| Post-Traumatic Stress Disorder (PTSD) | 11 |
| Generalized Anxiety Disorder (GAD) | 1 |
| Major Depressive Disorder (MDD) | 1 |
| Combination of PTSD and/or MDD and/or GAD | 30 |
| Various other Combinations of Mental Health Outcomes/Measures | 20 |
| Number of studies including common outcome measures | |
| PHQ-9: Patient Health Questionnaire-9 | 18 |
| PCL-5: PTSD Checklist for Diagnostic Statistical Manual V | 17 |
| AUDIT or AUDIT-C: Alcohol Use Disorder Identification Test (Consumption) | 10 |
| IES: Impact of Events Scale +/− Revised | 10 |
| SCL-90-R: Symptom Checklist 90-Revised Instrument | 6 |
| K6/10: Kessler Psychological Distress Scale | 6 |
| GAD-7: Generalized Anxiety Disorder-7 | 5 |
| DUDIT: Drug Use Disorder Identification Test | 4 |
| HADS: Hospital Anxiety and Depression Scale | 3 |
| References (Include Author and Citation #) | Country of Study | Study Aims | Study Design | Diagnoses/Outcome Measures | Main Findings |
|---|---|---|---|---|---|
| Adamis et al. [27] Abstract 2012 | Greece | To assess after a wildfire how psychopathology may evolve longitudinally, 3 years after. | Comparative Cross-sectional Study | The measured variable was psychological distress, using the SCL-90-R. | Psychological distress was significantly lower 3 years post-wildfire compared to 6 months post, but victims of the disaster continued to have higher scores on the SCL-90-R. |
| Adamis et al. [28] Abstract 2012 | Greece | To assess quality of life of adults living in a rural area impacted by a wildfire, 3 years prior. | Cross-sectional Study | The measured variables were quality of life, as assessed on the WHOQOL-BREF. | Multivariable analysis indicated that victims had a statistically significant poorer quality of life, with respect to the environmental health domain. |
| Adamis et al. [29] Abstract 2011 | Greece | To examine risk factors and psychiatric outcomes. | Comparative Cross-sectional Study | The measured variable was psychological distress, using the SCL-90-R. | Victims of the wildfire had significantly higher scores for symptoms, had a greater number of symptoms (PST), and were more distressed by them (GSI). |
| Afifi et al. [30] 2012 | United States | To analyze the impact of uncertainty secondary to experiencing natural disasters on mental health, and to investigate the role of communal coping | Cross-sectional Study | Measures included the MHI-5, rating personal feelings of uncertainty, and a measure for communal coping. | Residents who were evacuated experienced greater uncertainty regarding their home. In those evacuated, communal coping had a moderating role for uncertainty. |
| Agyapong et al. [31] 2018 | Canada | To examine the prevalence rate and risk factors for GAD 6 months after a wildfire. | Cross-Sectional Study | Outcome measures included the GAD-7, the AUDIT, the DUDIT, and the Fagerstrom Test for Nicotine Dependence. | The one month prevalence rate for GAD was 19.8%, and between 7 and 14% had scores indicative of a substance use disorder. |
| Agyapong et al. [32] 2020 | Canada | To evaluate prevalence rates for likely PTSD, MDD, and GAD 18 months after a wildfire. | Cross-sectional Study | Outcome measures included the PHQ-9, GAD-7, PCL-5, the AUDIT, and the DUDIT. | The 1 month prevalence rates for likely MDD, GAD, and PTSD were 18.3, 15.7, and 10.2%, respectively. While, 11.2% of participants reported symptoms of high-risk drinking and/or problematic drug use. |
| Agyapong et al. [33] Oral Communications- Abstract 2018 | Canada | To evaluate the prevalence rate and risk factors for MDD 6 months after a wildfire. | Cross-Sectional Study | The PHQ-9 was used to evaluate for MDD. | The one month prevalence rate for likely MDD was 14.8% (10.4% for males, and 17.1% for females). |
| Agyapong et al. [34] 2019 | Canada | To evaluate the prevalence rate and risk factors for PTSD 6 months after a wildfire. | Cross-sectional Study | Outcome measures included part 3 of the PCL-5, AUDIT, DUDIT, and Fagerstrom test for nicotine dependence. | 12.8% of respondents (14.9% of females and 8.7% of males) met criteria for PTSD. Those with PTSD reported increased drug use. |
| Belleville et al. [35] Abstract 2019 | Canada | To study a tool for supporting resilience and improving sleep after a wildfire. | Randomized Controlled Trial | Measures for symptoms of post-traumatic stress, depression, and insomnia. | Analyses revealed a significant improvement in post-traumatic stress, depression, and insomnia symptoms in the treatment group. |
| Belleville et al. [36] 2019 | Canada | To evaluate psychological symptoms 3 months after a wildfire. | Cross-Sectional Study | Outcome measures included the PCL-5, the PHQ-9, Insomnia Severity Index, PSQI-A, PTCI, and WCQ. | Approximately 60% of participants had post-traumatic stress, 33.1% MDD, 27.0% for anxiety disorders other than panic, 17.4% for panic disorder, and 17.1% for alcohol abuse disorder. |
| Binet et al. [37] 2021 | Canada | To determine if mental health service utilization post-wildfire differed by gender. | Cross-sectional Study | Outcome measures included the Perceived Need for Care Questionnaire, PCL-5, PHQ-9, and the Insomnia Severity Index. | From survey measures, 50.2% had a probable diagnosis of PTSD, 58.5% a probable diagnosis of MDD, and 57.4% a probable diagnosis of insomnia. Female gender was a statistically significant predictor of receiving mental health services. |
| Block et al. [38] 2019 | Australia | To evaluate how the natural environment can be part of personal recovery after a wildfire. | Cross-Sectional Study | Outcome measures included self report of environmental attachment, the K6, the PCL, the PHQ-9, the CD-RISC, and the short-form for post-traumatic growth inventory. | Those with a weak attachment to the environment had higher scores of psychological distress, fire-related PTSD, and MDD symptoms, and lower levels of resiliency. |
| Brown et al. [17] 2019 | Canada | To investigate how youth mental health is impacted 18 months after a wildfire. | Cross-Sectional Study | Outcome measures included the CPSS, PQH-A, the HADS, the CRAFFT, Tobacco Use Questionnaire, the RSE, the Kidscreen Questionnaire, and the Child and Youth Resilience Measure. | A total of 37% of the students met criteria for probable PTSD, 31% for probable depression, and 27% for probable anxiety. Students classified as high resilience had lower scores on all the mental health disorder screens and higher self-esteem and quality of life scores. |
| Brown et al. [39] 2019 | Canada | To assess the impact of a wildfire disaster on adolescent mental health. | Comparative Cross-Sectional Study | Outcome measures included the PHQ-A, the HADS, the CRAFFT Questionnaire, the Tobacco Use Questionnaire, the RSE, the Kidscreen Questionnaire, and the CPSS. | In the wildfire exposure group, adolescents had higher depression and anxiety scores and rates of probable depression. While, 37% of the students met criteria for probable PTSD. |
| Bryant et al. [22] 2020 | Australia | To examine the long-term psychological outcomes 10 years after a wildfire. | Cohort Study | Outcome measures included the PCL-5, PHQ-9, K6, and the AUDIT-C. | In the high-impact group, the rate of probable PTSD was 16.8% and MDE was 9.8%. The likelihood of developing any disorder was higher in the heavy drinking category than those who did not meet criteria, 29.2% versus 17.3%. |
| Bryant et al. [26] 2014 | Australia | To investigate the prevalence and predictors of psychological outcomes 3–4 years after a wildfire. | Cohort Study | Outcome measures included the abbreviated version of PCL-5, PHQ-9, K6 scale, and an abbreviated AUDIT. | Among the high impact group, 15.6% had probable wildfire related PTSD, 12.9% had probable MDD, and 24.7% had rates of heavy drinking. |
| Bryant et al. [40] 2017 | Australia | To examine how separation from an attachment figure as a child during a trauma can influence long-term attachment styles and future psychopathology. | Comparative Cohort Study | Outcome measures included parental presence during the wildfire, Experiences in Close Relationships scale, and the PCL-5. | Children exposed to bushfires and children separated from their parents during that time had higher scores on the avoidant attachment scale as adults. An avoidant attachment style was positively associated with PTSD symptoms. |
| Bryant et al. [41] 2017 | Australia | To examine how social connections between survivors of a disaster are linked to mental health outcomes. | Cohort Study | Outcome measures included social support questions, the PCL-5, and the PHQ-9. | Analyses found that identifying social support was associated with less depression, and being nominated by others as a support was associated with less PTSD. |
| Bryant et al. [42] 2018 | Australia | To examine the changing prevalence and predictors of psychological outcomes in communities 5 years post-wildfire. | Cohort Study | Outcome measures included the abbreviated PCL-5, PHQ-9, the K6, and the AUDIT-C. | In the high-impact group, the rate of probable fire-related PTSD was 10.9%, general PTSD was 18.7%, MDE was 10.9%, and heavy alcohol use was 23.2%. |
| Byrne et al. [43] 2006 | Australia | To determine the prevalence and risk factors for vicarious traumatization post-wildfire. | Cross-Sectional Study | Outcomes included IES, Vicarious Traumatization Questionnaire, and Coping Strategies Indicator. | Demographic factors were not found to be significant risk factors for vicarious traumatization. |
| Caamano-Isorna et al. [44] 2011 | Spain | To analyze the impact of a wildfire on respiratory systems and mental health. | Cohort Study | Outcome of interest was the drug dispensing rates for anxiolytics/hypnotics and drugs for obstructive airway disease 12 months before and after the wildfires. | Male non-pensioners saw a relative increase of 12.2% and male pensioners of 15.88% in the defined daily doses for anxiolytics and hypnotics. |
| Camilleri et al. [45] 2010 | Australia | To evaluate the impact of a wildfire on current health and wellbeing. | Cross-Sectional Study | Outcome measures included K10 and a survey on perceived wellbeing | A total of 39% reported their lives were more difficult after the bushfire. While, 19.5% were found to have high to very high rates of psychological distress. |
| Cherry and Haynes [14] 2017 | Canada | To examine how a wildfire impacted mental and physical health. | Cohort Study | Outcome measures included the HADS. | It was reported that 16.7% of those evacuated had scores indicative of moderate to severe anxiety or depression |
| Clayer et al. [13] 1985 | Australia | To evaluate immediate and long-term health effects 12 months after a wildfire. | Comparative Cross-Sectional Study | The outcome was evaluated on the GHQ. | Rates of alcoholism and drug problems approximately tripled pre-bushfire to post. Mental illness increased from 0.79% pre-bushfire to 3.01% post-bushfire. |
| Cowlishaw et al. [46] 2021 | Australia | To examine rates of significant anger problems following a bushfire and how this relates to mental health. | Cross-Sectional Study | Outcome measures included the DAR-5, PCL-4, PHQ-9, and the K6. | Among those with anger problems, 58.6% had probable PTSD, 43.2% had probable depression, and 34.5% had K6 scores indicative of severe mental illness. |
| Felix et al. [47] 2015 | United States | To study post-traumatic growth and coping mechanisms in parents and youth following a wildfire. | Cross-Sectional Study | Outcome measures included a scale to assess fire-related stress, the PTGI-SF, the MHI-5, the PFS, and the CERQ-Short Form. | Use of positive reappraisal coping techniques was associated with greater post-traumatic growth in youth and approached significance in parents. |
| Forbes et al. [48] 2015 | Australia | To examine how anger and patient factors can impact mental health outcomes following a wildfire. | Cross-Sectional Study | Outcome measures included the PCL-5, the PHQ-9, the AUDIT, and the AAQ. | Analyses showed significant indirect effects for anger and stressful life events on mental health outcomes. |
| Gallagher et al. [49] 2019 | Australia | To examine how voluntary group involvement can impact post-disaster mental health. | Cohort Study | Outcome measures included group involvement, the PCL-C, and the PHQ-9. | Curvilinear relationship between group involvement and PTSD at both times of follow-up but no significant relationship with depression. |
| Gallagher et al. [50] 2017 | Australia | To examine how attachment styles influence depression and PTSD following a wildfire. | Cross-Sectional Study | Heterosexual couples were surveyed regarding their PTSD and depression symptoms and attachment styles. | Male partners with avoidant attachment styles were associated with depression and PTSD symptoms in both partners. Female partners with avoidant attachment styles were associated with more PTSD and depression symptoms in themselves. |
| Gallagher et al. [51] 2016 | Australia | To evaluate if separation from family peri-wildfire disaster modifies the relationship between attachment style and mental health outcomes. | Cross-Sectional Study | Outcome measures included separation status, the ECR, the PHQ-9, and the PCL-5. | Separation from loved ones during the fire was associated with higher PTSD symptoms but not depression symptoms. There was an association between attachment anxiety and depression. |
| Hashoul-Andary et al. [52] 2016 | Israel | To study the relationship between anxiety sensitivity, distress tolerance, and psychopathology post-trauma. | Cohort Study | Outcome measures included the ASI, DTS, PDS, the IDAS, and the Panic Attack Questionnaire-short form. | The 1-month levels of emotional avoidance and distress predicted the emotional distress intolerance and degree of distress at 3 months. The level of emotional distress intolerance at 3 months strongly predicted the degree of distress post-trauma at 6 months. |
| Hertz-Picciotto, I [53] Abstract 2020 | United States | To study children and adolescents’ mental health 6 months post-wildfire. | Cross-Sectional Study | Outcome measures included changes in depressive mood, anxiety, and sleep symptoms. | A total of 21.7% of children and 28.7% of adolescents had changes in 3 or more behaviours or symptoms. |
| Ho et al. [55] 2014 | Singapore | To study the acute physical and psychological symptoms during seasonal haze. | Cross-Sectional Study | Outcome measures included personal views on what is considered to be a dangerous PSI value, physical symptoms, and the IES-R. | Respondents who perceived lower PSI values as dangerous were more likely to be experiencing more physical symptoms or have higher IES-R scores. |
| Hooper et al. [54] 2018 | Australia | To study how post-traumatic symptoms, coping strategies, and post-traumatic growth are related. | Cross-Sectional Study | Outcome measures included the IES-R, the Brief COPE Inventory, and the PTGI. | Greater post-traumatic symptoms and post-traumatic growth were associated with the utilization of avoidant, problem-focused, and emotion-focused coping strategies. |
| Jones et al. [16] 2002 | United States | To study psychosocial functioning and short-term mental health consequences in children 6 weeks after a wildfire. | Cross-Sectional Study | Outcome measures were obtained from the DICA-R. Self-report measures included the IES, the STAI-C, and the FQ-C. Parents received the PTSD component of the DIS and the IES. | There was an average of 5 PTSD symptoms reported by children in the high loss (HL) group, and 4.2 in the low loss (LL) group. Participants of the HL group had an average score of 39.9 on the IES, and 23.4 in the LL group. There was no significant association between symptoms among parent and child pairs. |
| Jones et al. [56] 1994 | United States | To examine short-term consequences of a wildfire on mental health in children and adolescents. | Comparative Cross-Sectional Study | Outcome measures were obtained from the DICA-R, the IES, and the FQ-C. | Victims met an average of 2.8 out of 5 PTSD criteria and control participants met an average of 1.6 criteria. |
| Jones et al. [78] 2003 | United States | To examine the rates of PTSD, depression, and anxiety post-wildfire. | Comparative Cohort Study | The initial follow-up outcome measures included the PTSD module DIS, the IES, the BDI, FQ-A, and the STAI. The second follow-up outcome measures included the DIS, the IES, and the FQ-A. | At the first point of follow-up, the victim group had significantly higher scores for PTSD and depression. At the second point of follow-up, the victim group had a significant decline in total score and intrusive psychological symptoms on the IES. |
| Kirsch et al. [20] 2016 | United States | To study longitudinal disaster recovery following a wildfire. | Cohort Study | Outcome measures were obtained from CASPER assessments designed for the study, and the mental health questions were based on the CDC BRFSS. | At initial point of follow-up, 54.8% of adults reported someone in the household experiencing depressed mood or hopelessness and sleeping problems. At the second point of follow-up, property damage resulted in a 19.3% greater likelihood of depression and/or hopelessness. |
| Marshall et al. [57] 2007 | United States | To evaluate the prevalence of PTSD and MDD among individuals who had sought disaster relief from a wildfire 3 months prior. | Cross-Sectional Study | Outcome measures included the PCL-5 and the PHQ-9. | A total of 24% had probable PTSD and 33% had probable MDD. |
| Mcdermott and Palmer [19] 1999 | Australia | To identify students experiencing significant emotional distress and depression after a wildfire and provide interventions. | Cross-Sectional Study | Outcome measures included the IES, the RMA, and the BDS. | A reported 12% of students were experiencing moderate-severe emotional distress symptoms, 4.7% had symptoms of depressive illness, and 14.1% had symptoms of high-trait anxiety. |
| McDermott et al. [58] 2005 | Australia | To identify children and adolescents who require mental health support and interventions after experiencing a wildfire. | Cross-Sectional Study | Outcome measures included the PTSD-RI and the SDQ. | A reported 12.1% had moderate PTSD, and 9.0% had severe–very severe PTSD. There were significantly higher scores in the primary grades (4–6), then junior or senior grades (7–12). |
| Mcdermott and Palmer [59] 2002 | Australia | To study depression and emotional distress in children and adolescents post-wildfire and association with developmental stage. | Cross-Sectional Study | Outcome measures included the IES, the RMA, and the BDS. | Multivariate analyses suggested that the IES score, the RMA score, grade at school, and experiencing evacuation significantly predicted the BDS index. BDS scores were lowest in middle grades. Adjusted emotional distress scores were lowest in the lower and high grades. |
| McFarlane et al. [18] 1987 | Australia | To perform a longitudinal assessment of children, examining the evolution of psychological morbidity after a wildfire. | Comparative Cohort Study | Outcome measures obtained via parent and teacher administered Rutter Questionnaires. | From teacher questionnaires, the caseness rate at 2, 8, and 26 months was 1.8%, 6.5%, and 12%, respectively. There were variable results in comparison to the control group. |
| McFarlane and Van Hooff [23] 2009 | Australia | To examine the rate of PTSD and other psychological disorders in adults who had experienced a wildfire during childhood. | Comparative Cohort Study | Outcome measures included the CDI, the AUDIT, and the IES-R. | A total of 36.7% of the bush-fire exposed participants and 31.7% of the controls met criteria for DSM-IV disorder in their lifetime. When DSM diagnoses were analyzed, the only one more significantly prevalent in the exposed group was lifetime history of specific phobia. |
| McFarlane et al. [60] 1997 | Australia | To examine the prevalence of mental health problems following a bushfire. | Comparative Cohort Study | Outcome measures included the 28 item GHQ. The second part of the study involved a subset of victims. Outcome measures included the GHQ and the DIS. | From the first follow-up, the mean GHQ score was 5.6, and 42% met criteria as possible psychiatric cases. At the second point of follow-up, 23% of the surveyed victims met criteria for psychiatric caseness. |
| McFarlane [79] 1987 | Australia | To examine post-traumatic symptoms and pathology in children following a wildfire. | Cohort Study | Outcome measures were obtained from Rutter Parent and Teacher Questionnaires. | The post-traumatic phenomena did not decrease in children from 8 to 26 months post-bushfire. There was significant correlation between the 2 month teacher symptom score and the 26 month scores. There was no 1:1 relationship between post-traumatic phenomena and psychological disorder. |
| Mellon et al. [61] 2009 | Greece | To assess the relationship between an external locus of control and levels of psychopathology. | Comparative Cross-Sectional Study | Outcome measures were the Brown Locus of Control scale and the SCL-90-R. | Participants who resided in the wildfire impacted area had a higher external locus of control views and higher global levels of psychopathology (GSI). There was a statistically significant correlation between levels of external locus of control and psychopathology in those with greater trauma. |
| Molyneaux et al. [62] 2020 | Australia | To study rates of interpersonal violence amongst communities impacted by a wildfire and the relationship with mental health. | Cross-Sectional Study | Outcome measures included participant experience of violence, the PCL-5, the PHQ-9, and the AUDIT-C. | There were more reports of experiencing violence in high-impact regions versus medium and low, 7.4% versus 0–1%. Experiencing violence predicted increased symptoms of depression and PTSD symptoms among women but not men. |
| Moore et al. [63] 2006 | Canada | To examine if increases in particulate matter (PM2.5 and PM10) created by wildfires were linked to changes in physician visits. | Cohort Study | Outcome measures included PM2.5, PM10 levels and physician billing for visits related to respiratory cardiovascular and mental health disorders. | There was no significant difference in weekly rates for physician visits for respiratory or cardiovascular diseases or mental health disorders during the time of worsening air quality |
| Moosavi et al. [64] 2019 | Canada | To assess the prevalence rates of likely PTSD, MDD, and GAD in patients of an after-hours family medicine clinic 18 months post-wildfire. | Cross-Sectional Study | Outcome measures included the PCL-5, the PHQ-9, and the GAD-7. | The rate for likely PTSD, MDD, and GAD was 13.6%, 24.8%, and 18.0%, respectively. |
| Papadatou et al. [65] 2012 | Greece | To examine rates and risk factors for PTSD and depression in adolescents who had experienced a wildfire 6 months prior. | Cross-Sectional Study | Outcome measures included the WEQ, CRIES-13, the DSRS, and the Kidcope-Adolescent Version. | Depression and PTSD symptom scores differed between boys and girls. While, 29.4% of adolescents reported symptoms above the cutoff score for PTSD, and 20% for depression. |
| Papanikolaou et al. [66] 2011 | Greece | To examine the psychological distress and morbidity following a wildfire. | Comparative Cross-Sectional Study | Outcome measures included the SCL-90-R. | The victim group had significantly higher symptom scores in somatization, depression, anxiety, hostility, phobic anxiety, obsession, and paranoia. There was a 43.6% case rate in the victim group, and 29.8% in the control group. |
| Papanikolaou et al. [67] 2011 | Greece | To examine the psychological status and personal perceptions of a population impacted by a wildfire. | Comparative Cross-Sectional Study | Outcome measures included the SCL-90-R. | The fire exposure group had significantly higher scores on 7 out of 9 of the primary scales in the SCL-90-R, and on the Global Severity Index and Positive Symptom Total. |
| Parslow and Jorm [68] 2006 | Australia | To determine the extent that tobacco use is impacted by a traumatic experience and symptoms of PTSD. | Cohort Study | Participants answered questions about wildfire experience, tobacco use, and completed the TSQ. | A reported 5% of participants screened positive for PTSD. In the regression analysis, increased levels of smoking were associated with a higher number of fire-related experiences but not PTSD symptoms. |
| Parslow et al. [69] 2006 | Australia | To study risk factors for PTSD following a wildfire. | Cohort Study | Initial outcome measures included the GADS and the short form of the Eysenck Personality Questionnaire. At the second point of follow-up, participants also completed the TSQ. | A total of 5% of participants after the wildfire met criteria for PTSD. Overall, 6 variables were strongly associated with PTSD symptoms, female gender, fewer years of education, prior history of depression or anxiety, evacuation, injury or death of a loved one from the fire, and the degree of peritraumatic emotions. |
| Psarros et al. [70] 2017 | Greece | To examine the relationship between insomnia and PTSD one month after a wildfire. | Cross-Sectional Study | Outcome measures included the SCL-90-R and the Athens Insomnia Scale. | A reported 46.7% met criteria for PTSD. Insomnia rates were higher in those with PTSD, at 79.1% versus 49% of those without. |
| Ritchie et al. [71] 2020 | Canada | To study the prevalence of PTSD, GAD, and MDD in college students 18 months after experiencing a wildfire. | Cross-Sectional Study | Outcome measures included the PHQ-9, GAD-7, the PCL-5, the AUDIT, and the DUDIT. | The one month prevalence rate for likely MDD, GAD, and PTSD was 23.4%, 18.7%, and 11.0%, respectively. It was found that 15.5%, 13.5%, and 4.4% of participants screened positive for high risk drinking, problematic drug use, and moderate to high nicotine dependence. |
| Scher and Ellwanger [72] 2009 | United States | To examine potential risk and protective factors for post-disaster adjustment and pathology. | Cohort Study | Two time-points of follow-up. Outcome measures included the FIQ, PTCI, BAI, BDI-II, and the PILL. | At the first point of follow-up, analyses found that female gender and negative fire-related cognitions were associated with increased anxiety symptoms. Increased negative fire-relation cognitions were associated with increased depression symptoms. |
| Silveira et al. [73] 2021 | United States | To study mental health consequences and associated risk factors after a wildfire. | Comparative Cross-Sectional Study | Outcomes were assessed using the PCL-5, the PHQ-9, and the GAD-7. | PCL-5 scores were significantly higher for those directly exposed. PHQ-9 and GAD-7 scores were higher in those directly or indirectly exposed vs. not exposed. |
| Tally et al. [74] 2013 | United States | To assess the impact of a wildfire on patients who utilized the public mental healthcare system. | Cross-Sectional Study | A regularly scheduled survey post-wildfire contained additional questions on the impact of the wildfires, evacuation status, and need for additional services. | A reported 18.1% of evacuees sought additional mental health services, compared to 8% of individuals who did not evacuate the area despite living in an evacuation zone, and 2.1% of those who lived in non-evacuation areas. Analyses revealed that the act of evacuation was significant for all 8 fire impact questions. |
| Verstraeten et al. [75] 2020 | Canada | To assess the development of PTSD-like symptoms in perinatal women following exposure to a wildfire and protective factors. | Cross-Sectional Study | Outcome measures included the IES-R, the PDI, the PDEQ, the short-form SSQ, and the CD-RISC. | A total of 26% qualified for probable PTSD. Both peritraumatic distress and dissociative experience scores were positively associated with post-traumatic symptoms. Analyses found only social support satisfaction had a moderating effect on the relationship between peritraumatic distress (when it was not significantly high) and post-traumatic symptom scores. |
| Yelland et al. [76] 2010 | Australia | To examine if wildfire disaster exposure variables or child demographics are associated with the severity of PTSD symptoms in youth. | Cross-Sectional Study | Outcome measures included the PTSD-RI-R and bushfire impact/experience questionnaire. | Average PTSD symptom score was 18.41; 17% had symptoms in the moderate range and 10% in the severe–very severe range. In analysis, relevant risk factors were perceived threat to life, ongoing loss or disruption in life, and younger age. |
| Zeller et al. [77] 2015 | Israel | To explore the relationship between self-compassion and trauma-related psychopathology. | Cohort Study | Outcome measures included the SCS, the IDAS, the MAAS, and the Carmel Trauma Questionnaire. | Self-compassion did not have an impact on overall wellbeing post-wildfire. Higher levels of self-compassion were associated with lower levels of depression at all 3 time-points and anxiety at 3 and 6 months. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
To, P.; Eboreime, E.; Agyapong, V.I.O. The Impact of Wildfires on Mental Health: A Scoping Review. Behav. Sci. 2021, 11, 126. https://doi.org/10.3390/bs11090126
To P, Eboreime E, Agyapong VIO. The Impact of Wildfires on Mental Health: A Scoping Review. Behavioral Sciences. 2021; 11(9):126. https://doi.org/10.3390/bs11090126
Chicago/Turabian StyleTo, Patricia, Ejemai Eboreime, and Vincent I. O. Agyapong. 2021. "The Impact of Wildfires on Mental Health: A Scoping Review" Behavioral Sciences 11, no. 9: 126. https://doi.org/10.3390/bs11090126
APA StyleTo, P., Eboreime, E., & Agyapong, V. I. O. (2021). The Impact of Wildfires on Mental Health: A Scoping Review. Behavioral Sciences, 11(9), 126. https://doi.org/10.3390/bs11090126