Impact of Burnout on Daily Activities from an Occupational Therapy Perspective: A Serial Mediation Model with the IDA Scale

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sampling and Procedure
2.2. Measurements
2.3. Data Analysis
3. Results
3.1. Validation of the IDA Scale
3.2. Validity and Relationship with Other Variables
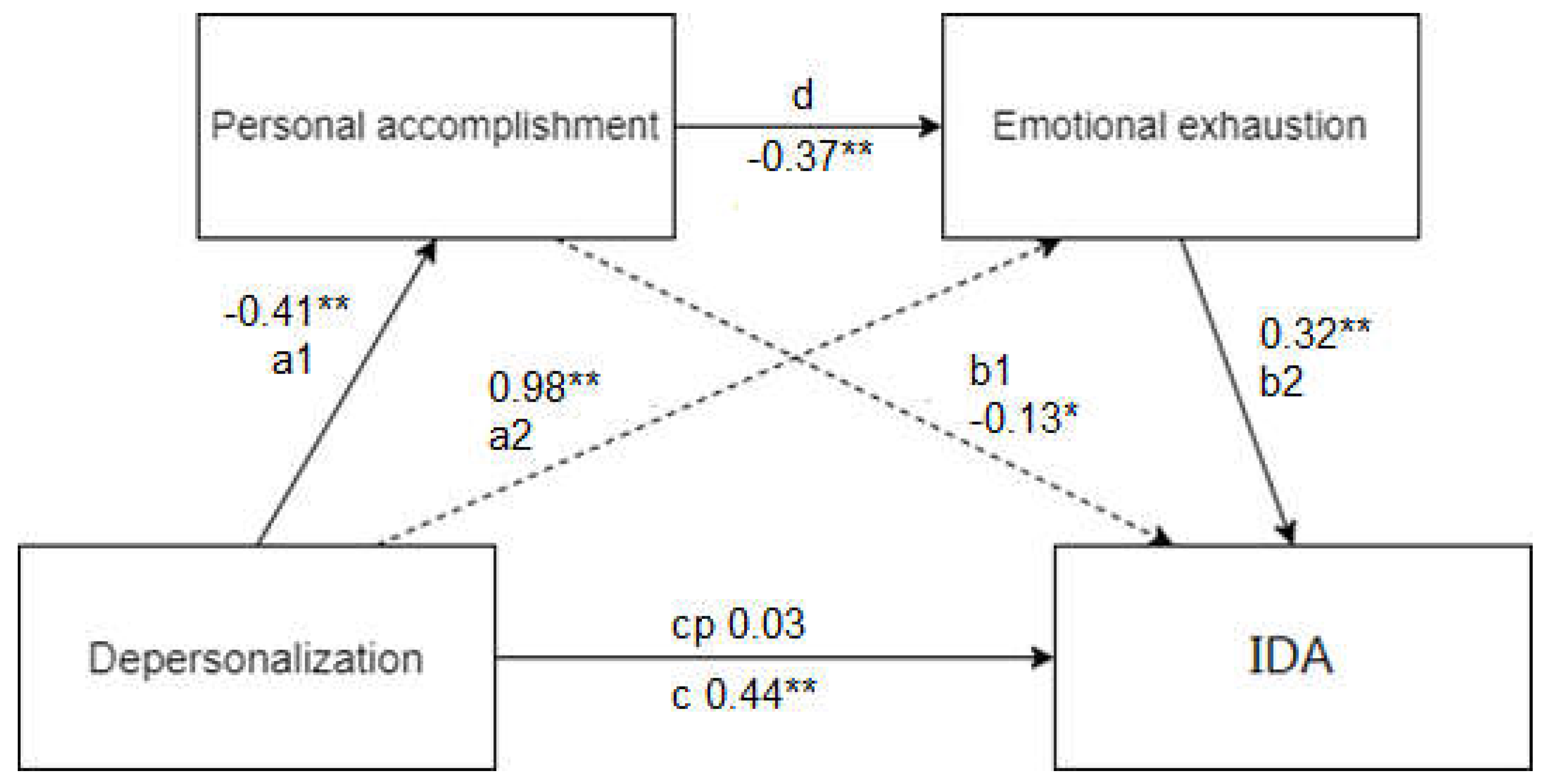
3.3. Serial Mediation Model Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Num | Statement |
|---|---|
| 1 | I feel that I have neglected my personal hygiene and cleanliness. |
| 2 | I have stopped cooking often, I resort to fast food or pre-cooked food or I think I have neglected my diet. |
| 3 | I take very little care of my appearance. I don’t care about the clothes I wear. |
| 4 | I have neglected the cleanliness and tidiness of my home. |
| 5 | My sexual desire has decreased considerably. |
| 6 | I have stopped enjoying taking care of others (family members, small children, friends, etc.). |
| 7 | I no longer enjoy looking after my pet or find it unthinkable to have one. |
| 8 | I rest poorly or have trouble falling asleep. |
| 9 | I feel that my work performance has declined. |
| 10 | I enjoy the leisure and free time activities that interested me much less than before. |
| 11 | I have stopped meeting friends or family, or I find it difficult to socialise as I used to. |
Appendix B
| Num | Statement | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|
| 1 | I feel that I have neglected my personal hygiene and cleanliness. | |||||
| 2 | I have stopped cooking often, I resort to fast food or pre-cooked food, or I think I have neglected my diet. | |||||
| 3 | I take very little care of my appearance. I don’t care about the clothes I wear. | |||||
| 4 | I have neglected the cleanliness and tidiness of my home. | |||||
| 5 | My sexual desire has decreased considerably. | |||||
| 6 | I have stopped enjoying taking care of others (family members, small children, friends, etc.). | |||||
| 9 | I feel that my work performance has declined. | |||||
| 10 | I enjoy the leisure and free time activities that interested me much less than before. | |||||
| 11 | I have stopped meeting friends or family, or I find it difficult to socialise as I used to. |
References
- Perlman, B.; Hartman, E.A. Burnout: Summary and Future Research. Hum. Relat. 1982, 35, 283–305. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S. Burnout in Health Professions: A Social Psychological Analysis. In Social Psychology of Health and Illness; Lawrence Erlbaum Associates: London, UK, 1982. [Google Scholar]
- Maslach, C. Burnout in Health Professionals. In Cambridge Handbook of Psychology, Health and Medicine; Cambridge University Press: Cambridge, UK, 2007; pp. 427–430. [Google Scholar]
- Golembiewski, R.T.; Munzenrider, R.F.; Stevenson, J.G. Phases of Burnout: Developments in Concepts and Applications; Praeger: Westport, CT, USA, 1986. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Demerouti, E.; Bakker, A.B.; Peeters, M.C.W.; Breevaart, K. New Directions in Burnout Research. Eur. J. Work. Organ. Psychol. 2021, 30, 686–691. [Google Scholar] [CrossRef]
- International Labour Organisation C161—Occupational Health Services Convention; International Labour Organisation: Geneva, Switzerland, 1985.
- Ndongo, J.M.; Lélé, C.B.; Manga, L.O.; Ngalagou, P.M.; Ayina, C.A.; Tanga, M.L.; Guessogo, W.; Barth, N.; Bongue, B.; Mandengue, S.; et al. Epidemiology of Burnout Syndrome in Four Occupational Sectors in Cameroon-Impact of the Practice of Physical Activities and Sport. AIMS Public Health 2020, 7, 319–335. [Google Scholar] [CrossRef] [PubMed]
- Longas, J.; Chamarro, A.; Riera, J.; Cladellas, R. La Incidencia Del Contexto Interno Docente En La Aparición Del Síndrome Del Quemado Por El Trabajo En Profesionales de La Enseñanza. Rev. Psicol. Trab. Organ. 2012, 28, 107–118. [Google Scholar] [CrossRef]
- Moukarzel, A.; Michelet, P.; Durand, A.-C.; Sebbane, M.; Bourgeois, S.; Markarian, T.; Bompard, C.; Gentile, S. Burnout Syndrome among Emergency Department Staff: Prevalence and Associated Factors. BioMed Res. Int. 2019, 2019, e6462472. [Google Scholar] [CrossRef]
- European Risk Observatory New and Emerging Risks in Occupational Safety and Health; European Agency for Safety and Health at Work: Bruxelles, Belgium, 2009.
- Gil-Monte, P. Desgaste Psíquico En El Trabajo: El Síndrome de Quemarse.; Síntesis: Madrid, Spain, 1997; ISBN 978-84-7738-472-4. [Google Scholar]
- Blanca-Gutiérrez, J.J.; Arias-Herrera, A.; Blanca-Gutiérrez, J.J.; Arias-Herrera, A. Síndrome de burnout en personal de enfermería: Asociación con estresores del entorno hospitalario, Andalucía, España. Enfermería Univ. 2018, 15, 30–44. [Google Scholar] [CrossRef]
- Muñoz, A.I.; Velásquez, M.S. Síndrome de quemarse por el trabajo en profesionales de enfermería, Bogotá, Colombia. Rev. Fac. Nac. Salud Pública 2016, 34, 202–211. [Google Scholar] [CrossRef]
- Blank, A.; Hayward, M. The Role of Work in Recovery. Br. J. Occup. Ther. 2009, 72, 324–326. [Google Scholar] [CrossRef]
- Liu, Q.; Wilson, L.H. Adding a Vocational Focus to Asian Mental Health Services in New Zealand: Occupational Therapy Opportunities. N. Zealand J. Occup. Ther. 2009, 56, 40–45. [Google Scholar] [CrossRef]
- Machingura, T.; Lloyd, C. Mental Health Occupational Therapy and Supported Employment. Ir. J. Occup. Ther. 2017, 45, 52–57. [Google Scholar] [CrossRef]
- World Health Organization The World Health Report: 2006: Working Together for Health; World Health Organization: Geneva, Switzerland, 2006.
- World Federation of Occupational Therapists About Occupational Therapy. Available online: https://wfot.org/about/about-occupational-therapy (accessed on 26 October 2022).
- Occupational Therapy Practice Framework: Domain and Process—Fourth Edition. Am. J. Occup. Ther. 2020, 74 (Suppl. S2), 7412410010p1–7412410010p87. [CrossRef] [PubMed]
- Martínez Pizarro, S. Síndrome Del Cuidador Quemado. Rev. Clínica Med. Fam. 2020, 13, 97–100. [Google Scholar]
- Hattori, A.; Ouchi, A.; Shibuya, K.; Sato, K.; Nakahara, K.-I.; Nishinaga, M.; Kameda, N.; Tuchimochi, H.; Fukayama, M.; Matsusita, S.; et al. Effect of the Level of Basic Activities of Daily Living on Home Caregiver Burnout. Nippon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2000, 37, 799–804. [Google Scholar] [CrossRef][Green Version]
- Maslach, C.; Jackson, S.E.; Michael, P.L.; Wilmar, B.S.; Richard, L. Schwab Maslach Burnout Inventory; Mind Garden: Menlo Park, CA, USA, 1986. [Google Scholar]
- Gil-Monte, P.R. El Síndrome de Burnout: Un Modelo Multicausal de Antecedentes y Consecuentes en Profesionales de Enfermería; Universidad de La Laguna: Santa Cruz de Tenerife, Spain, 1994; Available online: http://purl.org/dc/dcmitype/Text (accessed on 30 August 2022).
- IBM Corp. IBM SPSS Statistics for Windows; IBM Corp.: New York, NY, USA, 2017. [Google Scholar]
- JASP Team . JASP (Version 0.16.3)[Computer software]. 2022. Available online: https://jasp-stats.org/ (accessed on 15 July 2022).
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022.
- Montoya, A.K.; Hayes, A.F. Two-Condition within-Participant Statistical Mediation Analysis: A Path-Analytic Framework. Psychol Methods 2017, 22, 6–27. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Press: New York, NY, USA, 2008. [Google Scholar]
- Ferrando, P.J.; Lorenzo-Seva, U.; Hernández-Dorado, A.; Muñiz, J. Decalogue for the Factor Analysis of Test Items. Psicothema 2022, 34, 7–17. [Google Scholar] [CrossRef]
- Kahn, J.H. Factor Analysis in Counseling Psychology Research, Training, and Practice: Principles, Advances, and Applications. Couns. Psychol. 2006, 34, 684–718. [Google Scholar] [CrossRef]
- Timmerman, M.E.; Lorenzo-Seva, U. Dimensionality Assessment of Ordered Polytomous Items with Parallel Analysis. Psychol Methods 2011, 16, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Hancock, G.R.; An, J. A Closed-Form Alternative for Estimating ω Reliability under Unidimensionality. Meas. Interdiscip. Res. Perspect. 2020, 18, 1–14. [Google Scholar] [CrossRef]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Jensen, C.L.; Bibbo, J.; Rodriguez, K.E.; O’Haire, M.E. The Effects of Facility Dogs on Burnout, Job-Related Well-Being, and Mental Health in Paediatric Hospital Professionals. J. Clin. Nurs. 2021, 30, 1429–1441. [Google Scholar] [CrossRef]
- Lass-Hennemann, J.; Schäfer, S.K.; Sopp, M.R.; Michael, T. The Relationship between Dog Ownership, Psychopathological Symptoms and Health-Benefitting Factors in Occupations at Risk for Traumatization. Int. J. Environ. Res. Public Health 2020, 17, 2562. [Google Scholar] [CrossRef]
- McNicholas, J.; Gilbey, A.; Rennie, A.; Ahmedzai, S.; Dono, J.-A.; Ormerod, E. Pet Ownership and Human Health: A Brief Review of Evidence and Issues. BMJ 2005, 331, 1252–1254. [Google Scholar] [CrossRef] [PubMed]
- Wolkow, A.P.; Barger, L.K.; O’Brien, C.S.; Sullivan, J.P.; Qadri, S.; Lockley, S.W.; Czeisler, C.A.; Rajaratnam, S.M.W. Associations between Sleep Disturbances, Mental Health Outcomes and Burnout in Firefighters, and the Mediating Role of Sleep during Overnight Work: A Cross-Sectional Study. J. Sleep Res. 2019, 28, e12869. [Google Scholar] [CrossRef]
- Cheng, W.-J.; Cheng, Y. Night Shift and Rotating Shift in Association with Sleep Problems, Burnout and Minor Mental Disorder in Male and Female Employees. Occup. Environ. Med. 2017, 74, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Jarral, O.A.; Baig, K.; Shetty, K.; Athanasiou, T. Sleep Deprivation Leads to Burnout and Cardiothoracic Surgeons Have to Deal with Its Consequences. Int. J. Cardiol. 2015, 179, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Melamed, S.; Shirom, A.; Toker, S.; Berliner, S.; Shapira, I. Burnout and Risk of Cardiovascular Disease: Evidence, Possible Causal Paths, and Promising Research Directions. Psychol. Bull. 2006, 132, 327–353. [Google Scholar] [CrossRef] [PubMed]
- Stewart, N.H.; Arora, V.M. The Impact of Sleep and Circadian Disorders on Physician Burnout. Chest 2019, 156, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Aceves, G.A.; López, M.Á.C.; Moreno, S.; Jiménez, F.F.S.; Campos, J.D.J.S. Síndrome de Burnout. Arch. Neurocienc. 2006, 11, 305–309. [Google Scholar]
- Castillo, A.A.; Benavente, C.S.; Arnold, A.J.; Cruz, M.C. Presencia de síndrome de burnout en Hospital El Pino y su relación con variables epidemiológicas. Rev. Anacem 2012, 6, 9–13. [Google Scholar]
- Romani, M.; Ashkar, K. Burnout among Physicians. Libyan J. Med. 2014, 9, 23556. [Google Scholar] [CrossRef]
- Savio, S.A. El síndrome del burn out: Un proceso de estrés laboral crónico. Hologramática 2008, 8, 121–138. [Google Scholar]
- Taris, T.W.; Le Blanc, P.M.; Schaufeli, W.B.; Schreurs, P.J.G. Are There Causal Relationships between the Dimensions of the Maslach Burnout Inventory? A Review and Two Longitudinal Tests. Work Stress 2005, 19, 238–255. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Buunk, B.P. Burnout: An Overview of 25 Years of Research and Theorizing. In The Handbook of Work and Health Psychology; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2002; pp. 383–425. ISBN 978-0-470-01340-3. [Google Scholar]

| Variable | N (%) | Variable | N (%) | ||
|---|---|---|---|---|---|
| Sex | Women | 115 (76.7) | Employment sector | Health and social care | 79 (52.7) |
| Men | 34 (22.7) | Education | 18 (12.0) | ||
| Age (years) | 20–25 | 43 (28.7) | Hospitality and trade | 17 (11.3) | |
| 26–30 | 27 (18.0) | Leisure, events, culture | 11 (7.3) | ||
| 31–35 | 12 (8.0) | Public admin. | 3 (2.0) | ||
| 36–40 | 8 (5.3) | CIT and telecommunications | 2 (1.3) | ||
| 41–45 | 10 (6.7) | Mining, construction, maintenance and automotive | 8 (5.3) | ||
| 46–50 | 13 (8.7) | ||||
| 51–55 | 20 (13.3) | Housewife | 1 (0.7) | ||
| 56 or more | 14 (9.3) | Research | 2 (1.3) | ||
| Length of service | 1 year or less | 41 (27.3) | |||
| 1–5 years | 47 (31.3) | ||||
| 6–10 years | 17 (11.3) | ||||
| 11–15 years | 9 (6.0) | ||||
| 16 years and over | 33 (22.0) | ||||
| Item | Factor Loadings | Reliability if Items 8 and 9 are Dropped | Item–Rest Correlation | |
|---|---|---|---|---|
| McDonald’s ω | Cronbach’s α | |||
| 1 | 0.772 | 0.859 | 0.860 | 0.548 |
| 2 | 0.732 | 0.860 | 0.857 | 0.576 |
| 3 | 0.782 | 0.851 | 0.850 | 0.652 |
| 4 | 0.716 | 0.857 | 0.856 | 0.587 |
| 5 | 0.712 | 0.861 | 0.858 | 0.559 |
| 6 | 0.745 | 0.856 | 0.855 | 0.604 |
| 7 | 0.772 | 0.857 | 0.855 | 0.592 |
| 10 | 0.789 | 0.847 | 0.847 | 0.683 |
| 11 | 0.732 | 0.854 | 0.852 | 0.624 |
| Model | Χ² | df | Goodness-of-Fit Criteria Values |
|---|---|---|---|
| Baseline model | 474,819 | 36 | |
| Factor model | 30,290 | 27 | |
| Index | Value | ||
| Comparative Fit Index (CFI) | 0.993 | ≥0.95 | |
| Tucker–Lewis Index (TLI) | 0.990 | >0.95 | |
| Root mean square error of approximation (RMSEA) | 0.042 | ≤0.10 | |
| Standardised root mean square residual (SRMR) | 0.099 | ≤0.08 | |
| Goodness-of-fit index (GFI) | 0.987 | ≥0.95 |
| MBI EE | MBI DP | MBI PA | IDA | |
|---|---|---|---|---|
| MBI EE | 1 | |||
| MBI DP | 0.333 ** | 1 | ||
| MBI PA | −0.315 ** | −0.215 ** | 1 | |
| IDA | 0.440 ** | 0.242 ** | −0.276 ** | 1 |
| Indirect Effect | Boot SE | p | Bootstrapping 95% CI | ||
|---|---|---|---|---|---|
| Total Indirect Effects | 0.411 | 0.081 | 0.000 | [0.270; 0.589] | |
| Ind effect M1: Despersonalisation → Personal Accomplishment → IDA | a1b1 | 0.052 | 0.034 | 0.12 | [0.005; 0.141] |
| Ind Effect M2: Despersonalisation → Emotional Exhaustion → IDA | a2b2 | 0.312 | 0.069 | 0.000 | [0.005; 0.141] |
| Ind Effect M1-M2: Despersonalisation → Personal Accomplishment → Emotional Exhaustion → IDA | a1db2 | 0.047 | 0.022 | 0.03 | [0.015; 0.105] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Santiago, A.; Márquez-Álvarez, L.-J.; Llosa, J.A.; Jiménez Arberas, E. Impact of Burnout on Daily Activities from an Occupational Therapy Perspective: A Serial Mediation Model with the IDA Scale. Behav. Sci. 2022, 12, 426. https://doi.org/10.3390/bs12110426
Pérez-Santiago A, Márquez-Álvarez L-J, Llosa JA, Jiménez Arberas E. Impact of Burnout on Daily Activities from an Occupational Therapy Perspective: A Serial Mediation Model with the IDA Scale. Behavioral Sciences. 2022; 12(11):426. https://doi.org/10.3390/bs12110426
Chicago/Turabian StylePérez-Santiago, Alicia, Luis-Javier Márquez-Álvarez, José Antonio Llosa, and Estíbaliz Jiménez Arberas. 2022. "Impact of Burnout on Daily Activities from an Occupational Therapy Perspective: A Serial Mediation Model with the IDA Scale" Behavioral Sciences 12, no. 11: 426. https://doi.org/10.3390/bs12110426
APA StylePérez-Santiago, A., Márquez-Álvarez, L.-J., Llosa, J. A., & Jiménez Arberas, E. (2022). Impact of Burnout on Daily Activities from an Occupational Therapy Perspective: A Serial Mediation Model with the IDA Scale. Behavioral Sciences, 12(11), 426. https://doi.org/10.3390/bs12110426