Abstract
The increase in the demands for surveillance of chronic diseases, long-term care, and self-health management has allowed mobile smart health wearable devices to become products with greater business potential in past years. Wearable devices being able to be worn for long periods are the most suitable for 24-h weatherproof monitoring. Nevertheless, most technological products are not developed specifically for older adults. Older adults might be apprehensive and fearful about the use of technological equipment and might appear “technologically anxious”, so it was wondered whether older adults could smoothly operate and comfortably use smart wearable device products, and how “technological anxiety” would affect their behavior and attitude towards using these devices. The variables of “technology readiness”, “technological interactivity”, “perceived usefulness”, “perceived ease of use”, “attitude”, and “intention to use” are therefore discussed in this study. Taking “technological anxiety” as the moderating variable to develop the questionnaire scale, the quantitative research with structural equation model is applied to discuss the older adults’ intention to use smart health wearable devices. The questionnaire was distributed to older adults’ community care centers, senior centers, and senior learning centers in Taiwan, and to an older adults’ group above the age of 60 with experience in using smart bracelets. A total of 200 questionnaires were distributed, and 183 were retrieved, with 166 valid copies. The research results reveal that users with higher technology readiness, and older adult users with higher technological interactivity, present a higher perceived ease of use and perceived usefulness. Technological anxiety would affect users’ attitude and further influence the intention to use. The research results could help understand older adults’ needs for using smart health wearable devices.
1. Introduction
Along with the boom and diversification of technological products, new man–machine digital product technology provides different communication, entertainment, and care and is able to interact with the older adults group [1]. Mobile health devices (e.g., smart phones, smart watches) use mobile technology, wireless equipment, and sensors [2,3]. By wearing devices during daily activities, the accurate physiological, psychological, and emotional information as well as environmental status could be acquired through the sensors outputting data and the added self-reported data [4,5]. The behavioral surveillance with individualized feedback could track users’ health conditions, including sleep and psychological/physiological data of calories burned, heart rate, brain activity, and muscle action [6,7]. Such devices used for health-related surveillance present higher precision than traditional sampling frequency and are more suitable for long-period digital preventive measure and self-evaluation of behavior [8,9]. Since Apple promoted Apple Watch, the media started to pay attention to smart wearable devices. In face of the problems of low birth rate and aging society, smart wearable devices with medical technology would play the critical roles of care and accompaniment [10].
With the rapid adoption of smart technologies in people’s daily lives, utilizing smart technologies, such as wearables, service robots, Internet of Things (IoT) applications, and other home devices to satisfy the demand and improve the quality of life of older adults has become more necessary [11]. The boom and diversification of technological products, either software or hardware equipment, result in convenience of people’s life [12]. The design of wearable products is also advanced and has promoted the relationship between people and technological products to be closer. The design of technological products, including battery life, interface display design, man–machine interactivity, and diversified software, enhances people’s quality of life [13]. For older adults, such technological products would result in changes in life, products, or environment. A lot of research therefore has started to discuss the issue related to older adults in an environment with technological products, e.g., a study on older adults’ smart home [14]. Such research provides the smart living environment with digital health surveillance, safety protection, and medical interaction for older adults [8,15]. It reveals the importance and develops the ability of research on older adults and man–machine technological products.
Wearable technology consists of clothing and accessories that incorporate advanced technologies to assist individuals wearing them to perform their daily tasks quickly and efficiently [3]. Such technologies are very fundamental to monitoring the physiological data of older people or individuals with chronic conditions and facilitating timely clinical interventions [1]. Past research also proved the application of smart wearable devices to disease management and prevention, such as diabetes control [16], treatment of depressive disorder [17], hypertension control [18], and assessing function in Alzheimer’s disease [19]. Such preventive measures were verified in clinical research. Burke et al. [20] preceded diet control with PDAs to reduce calorie intake. Schoeppe et al. [21] proved that the use of smart phone applications and a training platform could effectively improve diet as well as physical activity and sedentary prevention behaviors. Kekade et al. [5] surveyed 233 seniors and discovered that more than 60% of older adults were interested in the use of smart wearable devices and expected to use them for improving physical and psychological activities. Tison et al. [22] used a commercially available smartwatch to detect atrial fibrillation. Ray et al. [23] revealed that GPS-based wireless tracking devices, such as Fitbit, Mi band, Oura ring, and Alice PDx, have been preferred and widely used by people with dementias. Ogundaini et al. [24] explored opportunities for integrating mobile health Information and Communication Technologies (ICTs) into the clinical settings of hospitals in South Africa and Nigeria.
Smart wearables are equipped with sensors and transmitters to monitor, collect, display, and transmit data automatically and perpetually [25]. Nevertheless, there are challenges to apply smart wearable technology to smart healthcare, including standard certification, continuous usability, users’ intention to use [26], shortage of cost-effective wearable sensors, heterogeneity of wearable devices connected, and high demand for interoperability, which are the bottlenecks encountered for smart wearable devices in the healthcare market [27]. Most technological products are not developed specifically for older adults [28]. Moschis [29] indicated that elder consumers presented different needs and preferences from the young generation and elder consumers would be less affected by the media and information technology. Adults aged above 50 would pay more attention to convenience, choose products with brands, and be willing to pay more for better product quality or service. Elder consumers seemed to dislike risks but prefer products and service with better safety [30]. Kruse et al. [31] pointed out independence, comprehension, and visibility as the factors in older adults using technological products, while complexity and limited availability as the obstructive factors. Smart wearable devices are helpful for older adults’ health control [1,2,25], but the products have to show obvious advantages for older adults to accept mobile health devices and must conform to the older adults’ goals, expectations, and lifestyles [32]. Shieh et al. [33] studied wearable equipment for monitoring sleep, with a questionnaire survey, to discuss older adults’ opinions about wearable equipment. The results revealed that older adults with distinct backgrounds showed different opinions about wearable equipment.
From previous literature, “technology readiness”, “technology interactivity”, “perceived usefulness”, “perceived ease of use”, “attitude”, and “intention to use” as well as the moderating variable of “technology anxiety” are used in the proposed conceptual model as the antecedents of intention to use health wearable devices for older adults. A questionnaire scale of each variable was developed to analyze older adults’ intentions to use smart health wearable devices. The research results could help the understanding of older adults’ needs for the use of smart health wearable devices as well as understand the physical and mental health management and successful aging of older adults.
2. Literature Review
2.1. Older Adults’ Usage Intention and Technology Anxiety
Healthcare, being an important issue in aging society, is a key factor in older adults’ quality of life [1]. It would have older adults consider obvious advantages of products and would meet the goals, expectations, and lifestyles to have them accept smart health wearable devices [32]. International Society for Gerontechnology (ISG) covers health, housing, mobility, communication, leisure, and work in “gerontechnlogy” [34]. From the viewpoint of technology, it is important to help older adults with declined physical functions to live with health, comfort, safety, and dignity through technologies [35,36]. The most important challenge for industries is not continuously developing new products but trying to have older adults using smart technological products in daily life [27,37]. Kruse et al. [31] discovered in their research that independence, comprehension, and visibility were the factors in enhancing older adults using technological products, while complexity and limited availability were the obstructive factors. However, most technological products were not developed specifically for older adults, and the technology operation required learning and skills. Holzinger et al. [38] compared the use of smart phones between youth and older adults and concluded a high heterogeneity of learning time, performance speed, error rate, and subjective satisfaction between older adults and youth. As a result, in consideration of possible physiological and psychological limits, technological products designed for older adults should be simple and easy to operate [28].
Davis [39] considered that users’ acceptance of information or technology was affected by perceived usefulness and perceived ease of use. A technology acceptance model (TAM) was then constructed to explain and predict the user model under the acceptance of information system. TAM initially discussed interviewees’ acceptance of the use of information system, from users’ cognition. The successive researchers applied the model or the modified model to discuss the acceptance of electronic and digital products or other information systems [2,5,10,13,33,35,40].
Parasuraman [41] proposed the technology readiness index (TRI) to discuss the relevance between personality traits and intention to use technological products, i.e., individual willingness to accept new technologies and the intention to use for work or life, particularly for understanding consumers’ readiness for the use of computers and network. Technology readiness was divided into the four dimensions of optimism, innovativeness, discomfort, and insecurity to represent individual readiness for using technologies. Both optimism and innovativeness were the driving force to use innovative technological products and could be regarded as the positive perception of using technology; discomfort and insecurity, on the other hand, referred to the resistance to the idea of using innovative technological products, as the negative perception of using technologies. Positive driving force and negative resistance might simultaneously exist in an individual and affect users’ technology acceptance and use behavior [42].
Chang et al. [43] considered that factors in users deciding to use smart wearable devices were not defined and were still at the early stage in the market development. They applied TAM to discuss important factors in 342 participants’ smart wearable device use behavior and discovered that users did not expect smart wearable devices to provide telecommunication functions or become fashion items. With wearable equipment for monitoring sleep as the target product, Shieh et al. [33] applied a questionnaire survey to discuss older adults’ opinions about the form of smart wearable devices. The results revealed that older adults with different backgrounds presented distinct opinions about the form of wearable equipment. Taking 233 elders as examples, Kekade et al. [5] discovered that more than 60% of elders were interested in using smart wearable devices in the future and expected to use them for improving physical and psychological activities.
Tsai et al. [44] regarded technology anxiety as apprehension and fear of using technological equipment, i.e., whether older adults could accept and smoothly operate and comfortably use smart wearable device products against negative psychological perception of nervousness, fear, and self-doubt when learning new skills. When older adults find obstacles in using new technological products, the effect of “technology anxiety” on the use behavior and attitude is the research motivation in this study.
2.2. Derivation of Hypotheses
Technology would affect users’ intention to use and evaluation, and user factors would also influence the willingness to adopt and accept new technology. Ajzen and Fishbein [45] mentioned possible external variables to affect users’ behavioral intention, including demographic characteristics, attitudes towards a specific target, and personality traits, where “personality traits” were user factors. The idea was similar to TRI in that users’ personality traits would affect the willingness to accept new technology. Ahmad et al. [46] indicated that individual technology readiness, when using a new technology, contained the basic concept of the new technology and the ambition to use new technology; the higher technology readiness revealed the strong interests in and ability of new technology such that the intention to use would be enhanced. Under strong technology readiness, the concept about new technology would be better. Past research proved the significant effect of technology readiness on perceived usefulness. Chen et al. [26], Ahmad et al. [46], and Widyawan and Santosa [47], with TRI as the external variable of TAM, found out remarkable relations between TRI and perceived usefulness and perceived ease of use in TAM. TRI is also used as the external variable of TAM in this study to discuss the older adults’ intention to use wearable devices. The hypotheses are therefore proposed in this study.
Hypothesis 1 (H1).
Technology readiness shows positive effects on perceived ease of use.
Hypothesis 2 (H2).
Technology readiness reveals positive effects on perceived usefulness.
Older adults being able to use various functions of smart health wearable devices as desired stands for older adults realizing that they do not need to pay extra efforts for using the interactive function of devices, could rapidly and easily use various interactive mechanisms, and simply exchange information with others through such interactive mechanism to increase knowledge and solve problems. Interactivity is the most important characteristic in a smart health wearable device system and shows positive effects on perceived ease of use [48]. Webster and Ho [49] pointed out interactivity as interaction ability between people and systems or feedback acquired from systems. Hsu et al. [50] considered that interactivity contained real-time and helpful information. Smart health wearable devices could provide information like number of steps, calories consumed, running route, heart rate, and blood pressure, which could be easily acquired by older adults, as useful information for self-health management [11]. Accordingly, hypotheses are proposed in this study.
Hypothesis 3 (H3).
Technology interactivity shows positive effects on perceived ease of use.
Hypothesis 4 (H4).
Technology interactivity presents positive effects on perceived usefulness.
Davis [39] proposed a technology acceptance model and pointed out positive effects of perceived ease of use on perceived usefulness. In the technology acceptance model research review, Hung et al. [51] organized and classified journals using the technology acceptance model and discovered that 30 pieces of literature, among 39, showed positive effects of perceived ease of use on perceived usefulness. Hypothesis is then proposed in this study.
Hypothesis 5 (H5).
Perceived ease of use shows positive effects on perceived usefulness.
TAM of Davis et al. [39] and Islam et al. [52] considered that website nature (e.g., perceived usefulness and perceived ease of use) would affect online users’ participation attitude. Pai and Yeh [48] mentioned that individuals with higher perceived usefulness of specific information technology would present positive attitude towards technology. Consequently, hypotheses are proposed in this study.
Hypothesis 6 (H6).
Perceived ease of use reveals positive effects on attitude.
Hypothesis 7 (H7).
Perceived usefulness shows positive effects on attitude.
In the explanation of online consumer behavior, Pavlou and Fygenson [53] revealed the effect of attitude on intention to use. Bruner II and Kumar [54] discovered that users with positive perception of information technology or achieving the engaged behaviors through information technology would show higher possibility to use information technology. Older adults being aware of using smart health wearable devices for self-health management would affect the intention to use. As a result, another hypothesis is proposed in this study.
Hypothesis 8 (H8).
Attitude presents positive effects on intention to use.
From the viewpoint of technology, it is important to help physical-function-declined older adults live with health, comfort, safety, and dignity through technology; however, older adults might discover some obstacles when facing the use of technological products [12,35]. Researchers have found that technological anxiety and resistance to change impact geriatric technology uptake [1]. Technology anxiety refers to apprehension and fear of using technological equipment [44]. Lin [55] indicated that individual emotional reactions of fear and nervousness during the use of or planning to use computers would affect the attitude towards computer products. Jeng et al. [56] defined computer anxiety as individual uncomfortable, scared, nervous, or worrying reactions when learning how to use computers, using computers, or expecting to come into contact with computers. Such reactions might be the negative attitudes towards computers accompanied with physiological and psychological discomfort to further hinder the computer learning or use in the future. As a consequence, the following hypothesis is proposed in this study.
Hypothesis 9 (H9).
Technology anxiety shows moderating effects on attitude and actual intention to use.
3. Research Method
3.1. Research Structure
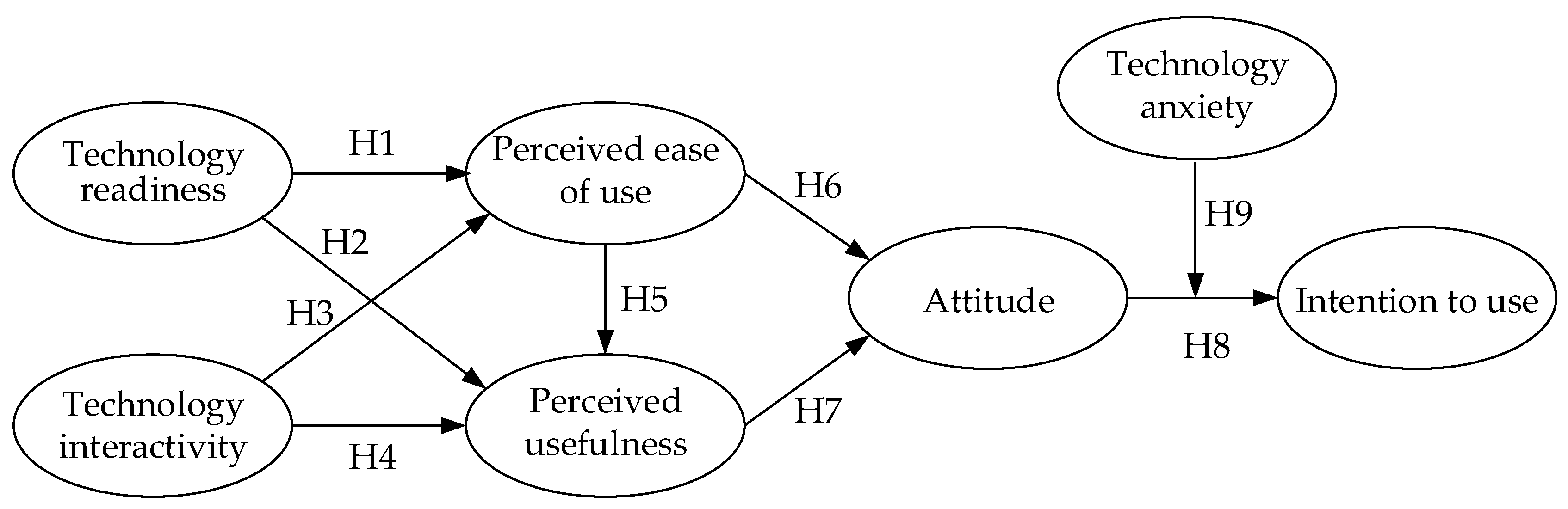
In consideration of the older adults being able to accept, smoothly operate, and comfortably use smart health wearable device products, the effect of “technology anxiety” on use behavior and attitude is studied, when they cannot use such new technological products. Using variables of “technology readiness”, “technology interactivity”, “perceived usefulness”, “perceived ease of use”, “attitude”, and “intention to use” and moderating the variable of “technology anxiety” as well as referring to relevant literature, the hypotheses are established for testing. With a literature review, the research structure is proposed as in Figure 1.
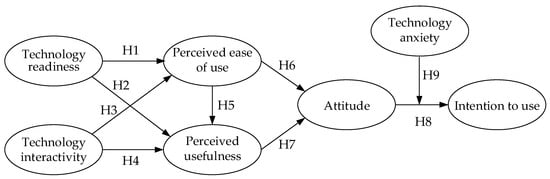
Figure 1.
Concept model of the older adults’ behavioral intention to use smart health wearable devices.
3.2. Questionnaire Design
With the questionnaire survey, two parts are included. According to domestic and international researchers’ research points of view and referring to relevant literature, the item contents are designed, and the questionnaire contents are analyzed, with 7 scales (Table 1). The technology readiness scale aims to understand users’ optimism, innovativeness, discomfort, and insecurity. The technology interactivity scale aims to understand older adults’ use of interactive communication with health devices, including feedback, control, entertainment, and connection. The perceived usefulness scale aims to measure user perception of information provided by smart health wearable devices enhancing living convenience. The perceived ease of use scale aims to understand the degree of users considering smart health wearable devices being easy to operate. The attitude scale is used for measuring users’ perception and evaluation of smart health wearable devices. The intention to use scale measures users’ intention to use health devices. The technology anxiety scale measures older adults’ apprehension and fear about using technological equipment, e.g., anxiety about equipment operation and information exposure. Detailed questionnaire items are shown in Appendix A Table A1.

Table 1.
Operational definitions of variables and sources of reference.
The second part shows demographic variables, covering users’ gender, education, age, marriage, occupation, living situation, average monthly disposable income, experience in using smart phones/tablet for recording or measuring health conditions, experience in using smart health wearable devices, and willingness to use smart health wearable devices. With Likert’s 5-point scale, five options of “extremely agree”, “agree”, “ordinary”, “disagree”, and “extremely disagree” are scored 5, 4, 3, 2, and 1. After the preliminary design of the questionnaire, we sent the questionnaire and procedure to the Research Ethics Committee of National Cheng Kung University, Taiwan, for ethical review. This study was conducted under approval number No.108–184.
3.3. Questionnaire Sample
The questionnaire was distributed to older adults’ community care centers, senior centers, and senior learning centers in Taiwan, and to an older adults’ group above the age of 60 with experience in using smart bracelets. We invited older adults to provide their opinions about smart bracelets first. If the older adults agreed, we provided them smart bracelets. After using the devices and providing opinions, the recruited samples could keep the devices as gifts.
In consideration of older adults’ eyesight and responding ability, the interviewer read out the questions one-to-one to them, who then answered with agree, disagree, extremely disagree, ordinary, or extremely agree, according to their experience. The interviewer then ticked the answer. Some older adults became impatient in the process and quit. A total of 200 copies of questionnaire were distributed, and 183 copies were retrieved, with 166 valid copies.
4. Research Result
4.1. Description of Demographic Variables
The effective questionnaire samples contain responses from 74 males (44.6%) and 92 females (54.4%), where the age group of 60–69 appears the most at 119 (71.6%), followed by 39 people aged 70–79 (23.5%). Eighty people show having the education of university or above (48.2%), followed by 44 with senior high (vocational) school (26.5%). Fifty-seven people are in the service industry (34.3%), followed by 50 people who are retired (30.1%). Seventy people show their monthly disposable income to be 20,000–40,000 NT dollars (42.2%), followed by 44 with 40,001–60,000 NT dollars (26.5%). Up to 102 people live with family members (61.4%), followed by 55 living with a spouse (33.1%). Ninety-nine people have experience in using smart health wearable devices (59.6%). An amount of 123 people show the volunteer willingness to use smart health wearable devices (74.1%). Detailed information is shown in Table 2.
Table 2.
Description of the interview sample.
4.2. Reliability Analysis
Cuieford [64] proposed that the Cronbach’s α reaching above 0.7 was high reliability, between 0.35–0.7 as medium reliability, and lower than 0.35 as low reliability. Nunnally [65] suggested that the Cronbach’s α reaching above 0.7 was acceptable. The Cronbach’s α of dimensions shows technology readiness at 0.76, technology interactivity at 0.91, perceived usefulness at 0.82, perceived ease of use at 0.81, attitude at 0.81, intention to use at 0.86, and technology anxiety at 0.87, higher than 0.7. It reveals certain reliability of the questionnaire (Table 3).
Table 3.
Variable reliability analysis.
Along with an approaching aging society, information technology users are expanded to older adults’ groups who do not frequently use networks to manage their health problems through smart health wearable devices. Aiming at the relations among technology readiness, technology interactivity, perceived usefulness, perceived ease of use, attitude, and intention to use of older adults’ use of smart health wearable devices, the moderating effect of technology anxiety on attitude and intention to use are discussed in this study. In terms of seven variables for this study, older adults show the overall evaluation of 3.932 for technology readiness for a smart health wearable device, revealing that older adults adapt to and are optimistic to use new technologies for mastering their health status, and smart bracelets do not need much time for learning or are not difficult to use. Older adults present the overall evaluation of 4.238 for technology interactivity of smart health wearable devices, explaining that older adults regard the use of smart health wearable devices and being able to rapidly inquire about the desired information is interesting and pleasant. Users show the overall evaluation of 4.289 for perceived usefulness of wearable devices, showing that older adults regard the use of smart health wearable devices as being able to increase the efficiency in health control and effectively improve health to promote the quality of life. The overall evaluation of 3.767 for perceived ease of use reveals that the smart health wearable device interface is easy to operate, and the multiple functions catch older adults’ eyes; however, unsuitable interface design for older adults would be refused, the same results as Choi and DiNitto [66].
The overall evaluation of 4.018 for attitude shows the positive evaluation of users after the use of wearable devices. When older adults consider that the use of technology can acquire useful information of a healthy life and provide entertainment, they will not easily refuse to use new technological information. The overall evaluation of 4.285 for intention to use reveals older adult users’ positive willingness to continuously use smart health wearable devices in the future. Moreover, the overall evaluation of 3.708 for technology anxiety shows that older adult users of smart health wearable devices worry about breaking smart bracelets in the use process and not being able to properly protect personal health information. The safety of technology use is related to personal learning anxiety (e.g., dealing with operation systems, solving problems, and worrying about destroying expensive equipment) [67]. Older adults would reduce the sources of absorbing technological information after retirement and are afraid of coming into contact with information products. In this case, more efforts should be made for the design of smart bracelets/watches and wearable devices; particularly, older adult users’ needs should be emphasized to provide diverse functions and multiple applications to have smart bracelets and watches become smart health wearable devices with high popularity and to integrate into each older adult user’s life, as a part of their life.
4.3. Correlation Analysis
The internal variables of technology readiness, technology interactivity, perceived usefulness, perceived ease of use, and attitude show their significance (p < 0.05). Although there is not a limit to high correlation, a coefficient higher than 0.90 should be particularly paid attention to. Correlation coefficients being higher than 0.80 might demonstrate multicollinearity. The correlations among the seven variables in this study appear in −0.90–0.751, without collinearity, and all variables achieve the significance (p < 0.01), revealing good correlations [68], Table 4.
Table 4.
Correlation analysis among variables.
4.4. Test of Research Hypothesis
There are nine hypotheses in this study. Multiple linear and hierarchical linear regression were used to test the proposed hypotheses. Multiple linear regression and path analysis were used to test H1 to H7 (Table 5). Otherwise, hierarchical linear regression was employed to test H8 and H9 (Table 6).
Table 5.
Research hypothesis test result.
Table 6.
Regression analysis of technology anxiety towards attitude and intention to use.
The research results are concluded as followings. H1: Technology readiness showing positive effects on perceived ease of use is supported (β = 0.385; t = 5.344; p < 0.001). It reveals that users with higher new technology readiness would feel it easier to learn and use technology. H2: Technology readiness presenting positive effects on perceived usefulness is supported (β = 0.545; t = 8.316; p < 0.001). It proves that users with higher new technology readiness can feel the enhancement of quality of life and health through technology. H3: Technology interactivity appearing positive effects on perceived ease of use is also supported (β = 0.511; t = 7.620; p < 0.001), revealing that users with higher new technology interactivity could more rapidly inquire for the desired information through smart health wearable devices.
H4: Technology interactivity presenting positive effects on perceived usefulness is supported (β = 0.751; t = 14.552; p < 0.001), revealing that users with higher new technology interactivity would be interested in the use of smart health wearable devices. H5: Perceived ease of use showing positive effects on perceived usefulness is supported (β = 0.461; t = 6.658; p < 0.001), revealing that users perceiving smart health wearable devices being easy to use would present higher use effectiveness. H6: Perceived ease of use showing positive effects on attitude is also supported (β = 0.579; t = 9.104; p < 0.001), showing that users perceiving smart health wearable devices being easy to use would present higher intention to use.
H7: Perceived usefulness shows positive effects on attitude. The empirical research results prove significantly positive effects of perceived usefulness on attitude (β = 0.600; t = 9.611; p < 0.001), revealing that users regarding the use of wearable devices being able to enhance the performance would demonstrate a higher intention to use.
As for H8 and H9, hierarchical regression was used for hypotheses testing. Hierarchical regression is a way to show if added-in variables can explain a statistically significant amount of variance in dependent variables after accounting for all other variables. It is usually used to test the effects of moderation variables. The hierarchical regression analysis results are presented in Table 5.
H8: Attitude presents positive effects on intention to use. The remarkably positive effects of attitude on behavioral intention are proven in this study (β = 0.647; t = 10.866; p < 0.001), showing that users with higher intention to use would have higher willingness to use. H9 verifies the moderating effect of technology anxiety on attitude and intention to use, with technology anxiety as the moderating variable. The effect of the interaction of attitude and technology anxiety on intention to use is analyzed with hierarchical regression analysis.
Model 1 shows notable correlations between attitude (β = 0.647, p < 0.001) and intention to use. Model 2 adds the moderating variable of technology anxiety which could directly and significantly affect intention to use (β = 0.221, p < 0.001). The interaction between attitude and technology anxiety is further discussed in Model 3. It is discovered that attitude and technology anxiety show remarkable effects on intention to use (β = −0.191, p < 0.001) (Table 5). In this case, technology anxiety presenting moderating effects on the effect of attitude on intention to use is supported. It reveals that users with stronger anxiety would show negative relations with attitude to further affect the intention to use. The empirical results show that the nine hypotheses in the research model are supported (Table 6).
5. Conclusions and Suggestion
Factors in older adults using smart health wearable devices are verified in this study. The first finding is that users with higher technology readiness show higher perceived ease of use and perceived usefulness, i.e., promoting users’ positive attitude to enhance the intention to use. Aiming at users’ technology readiness to segment target groups, optimistic and innovative older adult users could have innovative products promoted to them through various marketing channels. For uncomfortable and insecure users, reinforcing the product demonstration before purchase allows users to rapidly adapt to new products, and the system security of wearable device products should be strengthened. Older adults could easily acquire disease management through mobile software; however, how to define the shared contents or objects would involve personal privacy. Otherwise, the use of technological products would result in negative effects. For example, using video games for exercise might enhance the risk of falls due to limb incoordination or dizziness, worsening eyesight, and fatigue.
The second finding is that older adult users with higher technology interactivity present higher perceived ease of use and perceived usefulness, i.e., promoting users’ positive attitude to further increase the intention to use. For this reason, it is necessary to reinforce the interactivity of smart health wearable devices, perceived ease of use, and perceived usefulness. Technology is strange for most elders such that older adults’ attitudes will be conservative. Nonetheless, after the intervention, the attitude would become positive. When using technologies for acquiring information becomes easy, it reinforces the contact with family members and friends and strengthens the link with society to have older adults be more confident in their self-behavioral ability. The operation interface of wearable devices therefore should be simple and user-friendly, allowing users to perceive the operation or use to be simple. Enterprises and wearable device developers should provide products and services for users’ real needs to enhance users’ dependency on product functions and further affect the intention to use. Accordingly, brand value should be created to reduce users’ technology anxiety. When designing wearable device products, enterprises should reduce the error rate of products. Errors could result in users’ anxiety and negative effects to refuse the use. That is, enterprises and wearable device developers should enhance the interface design and product function of smart bracelets and watches, provide differentiated service, and reinforce marketing and promotion for users’ willingness to continuously use smart bracelets and watches. It should allow consumers finding out product value and reducing technology anxiety to enhance their attitude towards and intention to use wearable devices.
Older adults aged above 60 are the research objects in this study. The research population is people in Taiwan using smart bracelets and watches. Purposive sampling is applied to the survey, which might result in sampling bias. Surveying smart bracelet/watch users such that the research result is inferred to other groups and wearable devices requires further verification. A questionnaire survey is utilized for this study. Being restricted to time and budget, only cross-sectional study data are used for inference and verification. There is not comprehensive research for collecting data to discuss the cause-and-effect relationship among variables. In this case, merely the phenomenon at certain time points is observed, which cannot comprehensively understand the change of users’ attitude and intention to use at different times. The research results are therefore limited to the inference. Successive research is suggested to include qualitative research by an in-depth interview with older adults and different analysis methods to better understand the critical factors in older adult users’ intention to use smart health wearable devices. With the available budget and time, the successive researchers are suggested to survey consumers at different time points and discuss the changes in variables for more effective and reasonable results.
Author Contributions
Conceptualization, supervision, T.-M.Y. Data curation, formal analysis, M.-Y.J. methodology, writing—review and editing, F.-Y.P. All authors have read and agreed to the published version of the manuscript.
Funding
The Ministry of Science and Technology of Taiwan for supporting this research under grant number: MOST 108-2221-E-507-004-MY3.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of National Cheng Kung University, Taiwan (No.108–184).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors would like to express their sincere gratitude to the Editor and the anonymous reviewers for their insightful and constructive comments.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
The list of questionnaire items.
Table A1.
The list of questionnaire items.
| Dimension | Questionnaire Items | |
|---|---|---|
| technology readiness | optimism |
|
| ||
| ||
| innovativeness |
| |
| ||
| ||
| discomfort |
| |
| ||
| ||
| insecurity |
| |
| ||
| ||
| technology interactivity | feedback |
|
| ||
| ||
| control |
| |
| ||
| ||
| ||
| entertainment |
| |
| ||
| ||
| connection |
| |
| ||
| ||
| perceived usefulness |
| |
| ||
| ||
| perceived ease of use |
| |
| ||
| ||
| attitude |
| |
| ||
| ||
| intention to use |
| |
| ||
| ||
| technology anxiety | anxiety about equipment operation |
|
| ||
| ||
| anxiety about information exposure |
| |
| ||
| ||
References
- Larnyo, E.; Dai, B.; Larnyo, A.; Nutakor, J.A.; Ampon-Wireko, S.; Nkrumah, E.N.K.; Appiah, R. Impact of Actual Use Behavior of Healthcare Wearable Devices on Quality of Life: A Cross-Sectional Survey of People with Dementia and Their Caregivers in Ghana. Healthcare 2022, 10, 275. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.J.; Wu, W.Z.; Sun, C. A study on the acceptance of care robots by the elderly via unified theory of acceptance and use of technology. J. Gerontechnol. Serv. Manag. 2017, 5, 109–120. [Google Scholar]
- Guk, K.; Han, G.; Lim, J.; Jeong, K.; Kang, T.; Lim, E.-K.; Jung, J. Evolution of Wearable Devices with Real-Time Disease Monitoring for Personalized Healthcare. Nanomaterials 2019, 9, 813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Nilsen, W.J.; Abernethy, A.; Atienza, A.; Patrick, K.; Pavel, M.; Riley, W.T.; Shar, A.; Spring, B.; Spruijt-Metz, D. Mobile health technology evaluation: The mhealth evidence workshop. Am. J. Prev. Med. 2013, 45, 228–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kekade, S.; Hseieh, C.H.; Islam, M.M.; Atique, S.; Khalfan, M.K.; Li, Y.C.; Abdul, S.S. The usefulness and actual use of wearable devices among the elderly population. Comput. Methods Programs Biomed. 2018, 153, 137–159. [Google Scholar] [CrossRef] [PubMed]
- Spagnolli, A.; Guardigli, E.; Orso, V.; Varotto, A.; Gamberini, L. Measuring user acceptance of wearable symbiotic devices: Validation study across application scenarios. In Symbiotic Interaction; Symbiotic 2015. Lecture Notes in Computer Science; Jacucci, G., Gamberini, L., Freeman, J., Spagnolli, A., Eds.; Springer: Cham, Switzerland, 2014; p. 8820. [Google Scholar]
- Wu, W.; Haick, H. Materials and Wearable Devices for Autonomous Monitoring of Physiological Markers. Adv. Mater. 2018, 30, e1705024. [Google Scholar] [CrossRef] [PubMed]
- Helbostad, J.L.; Vereijken, B.; Becker, C.; Todd, C.; Taraldsen, K.; Pijnappels, M.; Aminian, K.; Mellone, S. Mobile health applications to promote active and healthy ageing. Sensors 2017, 17, 622. [Google Scholar] [CrossRef]
- Kim, J.; Campbell, A.S.; de Ávila, B.E.; Wang, J. Wearable biosensors for healthcare monitoring. Nat. Biotechnol. 2019, 37, 389–406. [Google Scholar] [CrossRef]
- Chuang, H.F. Factors influencing behavioral intention of wearable symbiotic devices–Case study of the mi band. Soochow J. Econ. Bus. 2016, 93, 1–24. [Google Scholar]
- Jeng, M.Y.; Yeh, T.M.; Pai, F.Y. A Performance Evaluation Matrix for Measuring the Life Satisfaction of Older Adults Using eHealth Wearables. Healthcare 2022, 10, 605. [Google Scholar] [CrossRef]
- Wang, Z.H.; Yang, Z.H.; Dong, T. A review of wearable technologies for elderly care that can accurately track indoor position, recognize physical activities and monitor vital signs in real time. Sensors 2017, 17, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Y.M.; Chang, C.C. Users’ psychological perception and perceived readability of wearable devices for elderly people. J. Behav. Inf. Technol. 2016, 35, 225–232. [Google Scholar] [CrossRef]
- Yetisen, A.K.; Martinez-Hurtado, J.L.; Unal, B.; Khademhosseini, A.; Butt, H. Wearables in medicine. Adv. Mater. 2018, 30, 1706910. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.; Afzal, M.; Khan, W.A.; Lee, S. Clinical decision support service for elderly people in smart home environment. In Proceedings of the 12th International Conference on Control, Automation Robotics & Vision, Guangzhou, China, 5–7 December 2012; pp. 678–683. [Google Scholar]
- Holzer, R.; Bloch, W.; Brinkmann, C. Continuous Glucose Monitoring in Healthy Adults—Possible Applications in Health Care, Wellness, and Sports. Sensors 2022, 22, 2030. [Google Scholar] [CrossRef] [PubMed]
- Cormack, F.; McCue, M.; Taptiklis, N.; Skirrow, C.; Glazer, E.; Panagopoulos, E.; van Schaik, T.A.; Fehnert, B.; King, J.; Barnett, J.H. Wearable Technology for High-Frequency Cognitive and Mood Assessment in Major Depressive Disorder: Longitudinal Observational Study. JMIR Ment. Health 2019, 6, e12814. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.W.; Huang, H.K.; Fang, Y.T.; Lin, Y.T.; Li, S.Z.; Chen, B.W.; Lo, Y.C.; Chen, P.C.; Wang, C.F.; Chen, Y.Y. A Data-Driven Model with Feedback Calibration Embedded Blood Pressure Estimator Using Reflective Photoplethysmography. Sensors 2022, 22, 1873. [Google Scholar] [CrossRef]
- Stavropoulos, T.G.; Lazarou, I.; Diaz, A.; Gove, D.; Georges, J.; Manyakov, N.V.; Pich, E.M.; Hinds, C.; Tsolaki, M.; Nikolopoulos, S.; et al. Wearable devices for assessing function in alzheimer’s disease: A european public involvement activity about the features and preferences of patients and caregivers. Front. Aging Neurosci. 2021, 13, 643135. [Google Scholar] [CrossRef]
- Burke, L.E.; Conroy, M.B.; Sereika, S.M.; Elci, O.U.; Styn, M.A.; Acharya, S.D.; Sevick, M.A.; Ewing, L.J.; Glanz, K. The effect of electronic self-monitoring on weight loss and dietary intake: A randomized behavioral weight loss trial. Obesity 2011, 19, 338–344. [Google Scholar] [CrossRef]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef] [Green Version]
- Tison, G.H.; Sanchez, J.M.; Ballinger, B.; Singh, A.; Olgin, J.E.; Pletcher, M.J.; Vittingho, E.; Lee, E.S.; Fan, S.M.; Gladstone, R.A.; et al. Passive detection of atrial fibrillation using a commercially available smartwatch. JAMA Cardiol. 2018, 3, 409–416. [Google Scholar] [CrossRef] [Green Version]
- Ray, P.P.; Dash, D.; De, D. A systematic review and implementation of IOT-based pervasive sensor-enabled tracking system for dementia patients. J. Med. Syst. 2019, 43, 287. [Google Scholar] [CrossRef] [PubMed]
- Ogundaini, O.O.; de la Harpe, R.; McLean, N. Integration of mHealth Information and Communication Technologies into the Clinical Settings of Hospitals in Sub-Saharan Africa: Qualitative Study. Adv. Digit. Health Open Sci. 2021, 9, e26358. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.T. Safety and Efficiency in a New Era of Intelligent Healthcare. Formos. J. Med. 2021, 25, 604–612. [Google Scholar]
- Chen, L.K. Re-evolution of smart medical applications in super-aged society. J. Gerontechnol. Serv. Manag. 2018, 6, 81–87. [Google Scholar]
- Yang, P.; Bi, G.; Qi, J.; Wang, X.; Yang, Y.; Xu, L. Multimodal wearable intelligence for dementia care in healthcare 4.0: A survey. Inf. Syst. Front. 2021, 2021, 1–18. [Google Scholar] [CrossRef]
- Yueh, H.P.; Yang, Y.J.; Chen, Y.J.; Lee, Y.R.; Chou, Y.L.; Lu, T.Y.; Shu, W.C. A usability study of elders use of digital product: Smart pill box system. J. Sci. Technol. Stud. 2010, 44, 35–49. [Google Scholar]
- Moschis, G.P. Marketing to older adults: An updated overview of present knowledge and practice. J. Consum. Mark. 2003, 20, 516–525. [Google Scholar] [CrossRef]
- Bastoni, S.; Wrede, C.; da Silva, M.C.; Sanderman, R.; Gaggioli, A.; Braakman-Jansen, A.; van Gemert-Pijnen, L. Factors Influencing Implementation of eHealth Technologies to Support Informal Dementia Care: Umbrella Review. Adv. Digit. Health Open Sci. 2021, 4, e30841. [Google Scholar]
- Kruse, C.S.; Mileski, M.; Moreno, J. Mobile health solutions for the aging population: A systematic narrative analysis. J. Telemed. Telecare 2016, 23, 439–451. [Google Scholar] [CrossRef]
- Devos, P.; Jou, A.M.; De Waele, G.; Petrovic, M. Design for personallized mobile health applications for enhanced older people participation. Eur. Ger. Med. 2015, 6, 593–597. [Google Scholar] [CrossRef]
- Shieh, M.D.; Hsiao, H.C.; Lin, Y.H.; Lin, J.Y. A study of the elderly people’s perception of wearable device forms. J. Interdiscip. Math. 2017, 20, 789–804. [Google Scholar] [CrossRef]
- International Society of Gerontechnology. 2021. Available online: http://www.gerontechnology.org/ (accessed on 20 November 2021).
- Chen, C.Y. Probing the technology acceptance for older adults: A case study on southern part of Taiwan. J. Kun Shan Univ. 2015, 10, 132–144. [Google Scholar]
- Dai, B.; Larnyo, E.; Tetteh, E.A.; Aboagye, A.K.; Musah, A.-A.I. Factors Affecting Caregivers’ Acceptance of the Use of WearableDevices by Patients with Dementia: An Extension of the Unified Theory of Acceptance and Use of Technology Model. Am. J. Alzheimer Dis. Other Dement. 2020, 35, 1533317519883493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, Y.L. The development and innovation of smart technology in the application of elderly care. Public Gov. Q. 2020, 8, 44–55. [Google Scholar]
- Holzinger, A.; Searle, G.; Nischelwitzer, A. On some aspects of improving mobile applications for the elderly. In Proceedings of the 4th International Conference on Universal Access in Human-Computer Interaction, UAHCI 2007, Beijing, China, 22–27 July 2007. [Google Scholar]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- To, W.M.; Lee, P.K.C.; Lu, J.; Wang, J.; Yang, Y.; Yu, Q. What Motivates Chinese Young Adults to Use mHealth? Healthcare 2019, 7, 156. [Google Scholar] [CrossRef] [Green Version]
- Parasuraman, A. Technology Readiness Index (TRI) a multiple-item scale to measure readiness to embrace new technologies. J. Serv. Res. 2000, 2, 307–320. [Google Scholar] [CrossRef]
- Chen, T.H.; Li, M.T.; Hsiao, J.L. An Investigation of Medical Record Management Professionals Continuance Intentions to Use Electronic Medical Records: Integrating Technology Readiness and Post-Acceptance Model. J. Med. Health Inf. Manag. 2018, 16, 1–19. [Google Scholar]
- Chang, H.S.; Lee, S.C.; Ji, Y.G. Wearable device adoption model with TAM and TTF. Int. J. Mobile Commun. 2016, 14, 518–537. [Google Scholar] [CrossRef]
- Tsai, T.H.; Lin, W.Y.; Chang, Y.S.; Chang, P.C.; Lee, M.L. Technology anxiety and resistance to change behavioral study of a wearable cardiac warming system using an extended TAM for older adults. PLoS ONE 2020, 15, e0227270. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Ahmad, H.; Butt, A.H.; Khan, A.; Shafique, M.N.; Nawaz, Z. Reluctance to acceptance: Factors affecting e-payment adoption in Pakistan (The integration of TRI and TAM). SMART J. Bus. Manag. Stud. 2020, 16, 49–59. [Google Scholar] [CrossRef]
- Widyawan, N.L.; Santosa, P.I. Technology readiness and technology acceptance model in new technology implementation process in low technology SMEs. Int. J. Innov. Manag. Technol. 2017, 8, 113–117. [Google Scholar]
- Pai, F.Y.; Yeh, T.M. The effects of information sharing and interactivity on the intention to use social networking websites. Qual. Quant. 2014, 48, 2191–2207. [Google Scholar] [CrossRef]
- Webster, J.; Ho, H. Audience engagement in multi-media presentations. Data Base Adv. Inf. Syst. 1997, 28, 63–77. [Google Scholar] [CrossRef]
- Hsu, S.H.; Lee, F.L.; Wu, M.C. Designing action games for appealing to buyers. Cyber Psychol. Behav. 2005, 8, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Hung, S.Y.; Liang, T.P.; Chang, C.M. A meta-analysis of empirical research using TAM. J. Inf. Manag. 2005, 12, 211–234. [Google Scholar]
- Islam, H.; Jebarajakirthy, C.; Shankar, A. An experimental based investigation into the effects of website interactivity on customer behavior in on-line purchase context. J. Strateg. Mark. 2021, 29, 117–140. [Google Scholar] [CrossRef]
- Pavlou, P.A.; Fygenson, M. Understanding and predicting electronic commerce adoption: An extension of the theory of planned behavior. MIS Q. 2006, 30, 115–143. [Google Scholar] [CrossRef]
- Bruner II, G.C.; Kumar, A. Explaining consumer acceptance of handheld internet devices. J. Bus. Res. 2005, 58, 553–558. [Google Scholar] [CrossRef]
- Lin, Y.L. The Theoretical Exploration of Computer Phobia. J. Cyber C. Inf. Soc. 2003, 5, 327–358. [Google Scholar]
- Jeng, Y.C.; Lu, S.C.; Chen, C.Y.; Szu, C.C. A study of the relationship between computer anxiety and learning achievements of junior high school students. Chang. Gung J. Hum. Soc. Sci. 2012, 5, 125–158. [Google Scholar]
- Cyr, D.; Head, M.; Ivanov, A. Perceived interactivity leading to e-loyalty: Development of a model for cognitive–affective user responses. Int. J. Hum. Comp. Stud. 2009, 67, 850–869. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Moon, J.; Kim, Y.J.; Mun, Y.Y. Antecedents and consequences of mobile phone usability: Linking simplicity and interactivity to satisfaction, trust, and brand loyalty. Inf. Manag. 2015, 52, 295–304. [Google Scholar] [CrossRef]
- Dholakia, R.; Miao, Z.; Dholakia, N.; Fortin, D. Interactivity and Revisits to Websites: A Theoretical Framework. RITIM Working Paper. 2000. Available online: /http://ritim.cba.uri.edu/wp/S (accessed on 20 November 2021).
- Amoako-Gyampah, K.; Salam, A.F. An extension of the technology acceptance model in an ERP implementation environment. Inf. Manag. 2004, 41, 731–745. [Google Scholar] [CrossRef]
- Ahn, T.; Ryu, S.W.; Han, I. The impact of Web quality and playfulness on user acceptance of online retailing. Inf. Manag. 2007, 44, 263–275. [Google Scholar] [CrossRef]
- Vijayasarathy, L.R. Predicting consumer intentions to use on-line shopping: The case for an augmented technology acceptance model. Inf. Manag. 2004, 41, 747–762. [Google Scholar] [CrossRef]
- Schwaig, K.S.; Segars, A.H.; Grover, V.; Fiedler, K.D. A model of consumers’ perceptions of the invasion of information privacy. Inf. Manag. 2013, 50, 1–12. [Google Scholar] [CrossRef]
- Cuieford, J.P. Fundamental Statistics in Psychology and Education; McGraw-Hill: New York, NY, USA, 1965. [Google Scholar]
- Nunnally, J.C. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Choi, N.G.; Dinette, D.M. The digital divide among low-income homebound older adults: Internet use patterns, eHealth literacy, and attitudes toward computer/Internet use. J. Med. Internet Res. 2013, 15, e93. [Google Scholar] [CrossRef]
- Levine, D.M.; Lipsitz, S.R.; Linder, J.A. Trends in seniors’ use of digital health technology in the United States, 2011–2014. J. Am. Med. Assoc. 2016, 316, 538–540. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5th ed.; Macmillan: New York, NY, USA, 1998. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).