
Enhancing Subjective Wellbeing in Older Individuals with Amnestic Mild Cognitive Impairment: A Randomized Trial of a Positive Psychology Intervention

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction: Background and Objectives
1.1. Positive Psychology: A Paradigm Shift in Understanding Well-Being and Human Flourishing
1.2. The Growing Burden of Dementia and Mild Cognitive Impairment: Implications for Aging Populations and Quality of Life
1.3. Positive Psychology Interventions: Exploring Efficacy and Potential for Enhancing Well-Being in Individuals with Mild Cognitive Impairment
1.4. Aim and Hypotheses of the Current Study
2. Materials and Methods
2.1. Study Design and Participants
2.1.1. Procedure
2.1.2. Blinding
2.1.3. Ethics
2.2. Instruments
2.2.1. PERMA Profiler (PERMA-23)
2.2.2. Positive Psychology Intervention (PPI)
3. Statistical Analysis
3.1. Results
3.1.1. Overall Wellbeing
3.1.2. Positive Emotion and Relationship
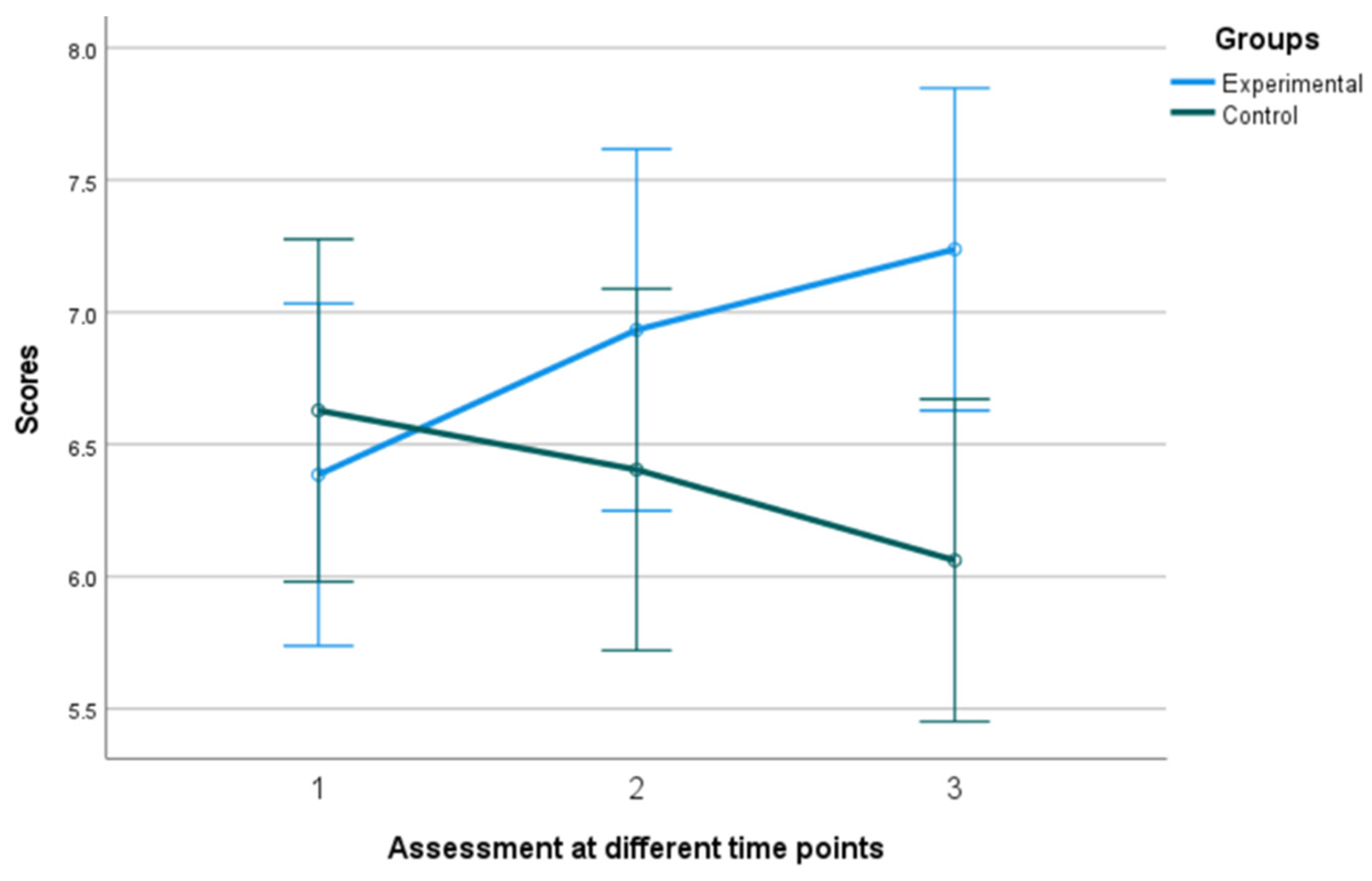
3.1.3. Engagement
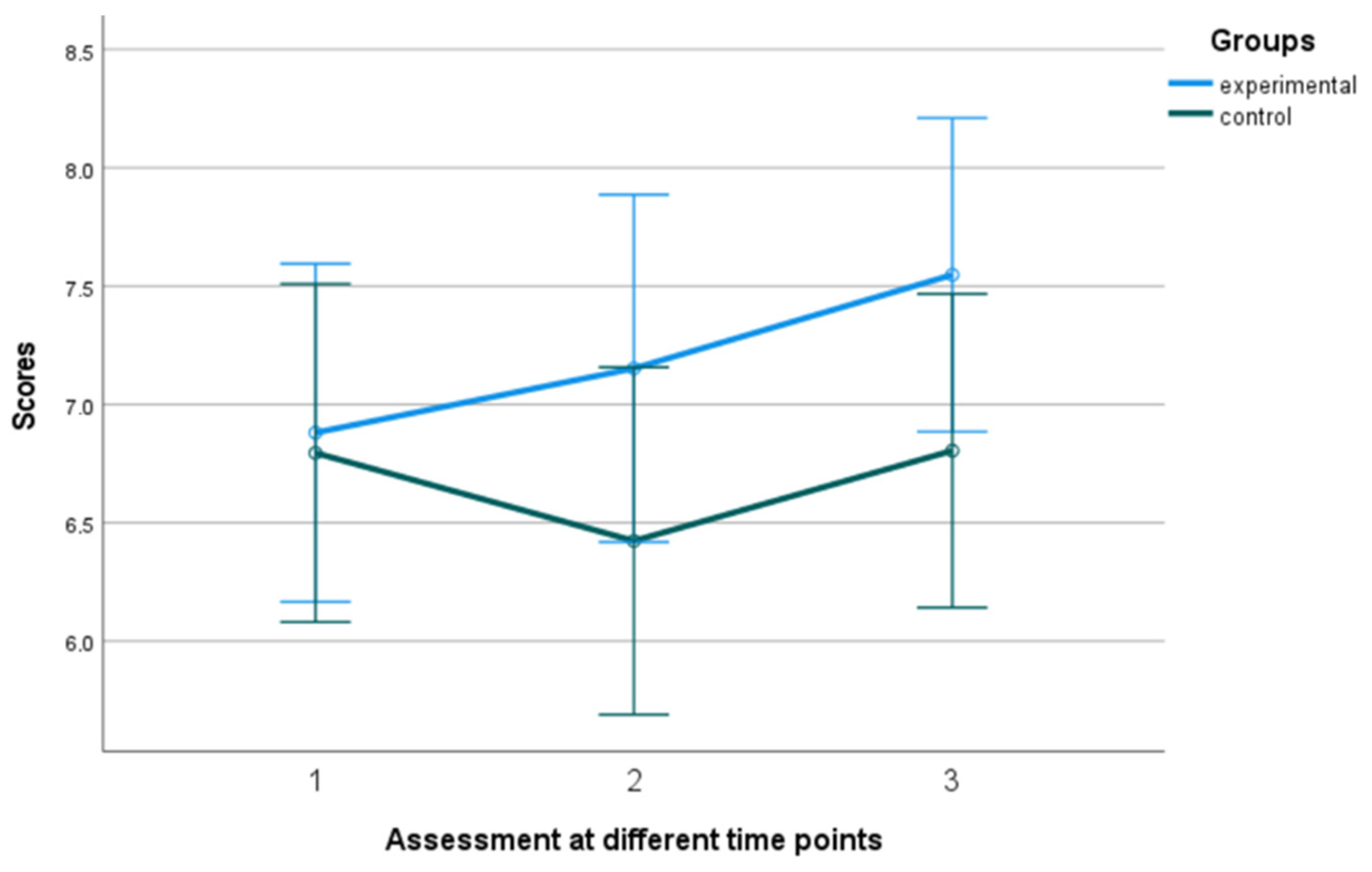
3.1.4. Meaning
3.1.5. Accomplishment
4. Discussion
Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section/Topic | Item No | Checklist Item | Reported on Page No |
|---|---|---|---|
| Title and abstract | |||
| 1a | Identification as a randomized trial in the title | ||
| 1b | Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) | ||
| Introduction | |||
| Background and objectives | 2a | Scientific background and explanation of the rationale | |
| 2b | Specific objectives or hypotheses | ||
| Methods | |||
| Trial design | 3a | Description of trial design (such as parallel, factorial) including allocation ratio | |
| 3b | Important changes to methods after trial commencement (such as eligibility criteria), with reasons | ||
| Participants | 4a | Eligibility criteria for participants | |
| 4b | Settings and locations where the data were collected | ||
| Interventions | 5 | The interventions for each group with sufficient details to allow replication, including how and when they were actually administered | |
| Outcomes | 6a | Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed | |
| 6b | Any changes to trial outcomes after the trial commenced, with reasons | ||
| Sample size | 7a | How sample size was determined | |
| 7b | When applicable, explanation of any interim analyses and stopping guidelines | ||
| Randomisation: | |||
| Sequence generation | 8a | Method used to generate the random allocation sequence | |
| 8b | Type of randomisation; details of any restriction (such as blocking and block size) | ||
| Allocation concealment mechanism | 9 | Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned | |
| Implementation | 10 | Who generated the random allocation sequence, who enrolled participants, and who assigned participants to interventions | |
| Blinding | 11a | If done, who was blinded after assignment to interventions (for example, participants, care providers, those assessing outcomes) and how | |
| 11b | If relevant, description of the similarity of interventions | ||
| Statistical methods | 12a | Statistical methods used to compare groups for primary and secondary outcomes | |
| 12b | Methods for additional analyses, such as subgroup analyses and adjusted analyses | ||
| Results | |||
| Participant flow (a diagram is strongly recommended) | 13a | For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analysed for the primary outcome | |
| 13b | For each group, losses and exclusions after randomization, together with reasons | ||
| Recruitment | 14a | Dates defining the periods of recruitment and follow-up | |
| 14b | Why the trial ended or was stopped | ||
| Baseline data | 15 | A table showing baseline demographic and clinical characteristics for each group | |
| Numbers analysed | 16 | For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups | |
| Outcomes and estimation | 17a | For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval) | |
| 17b | For binary outcomes, presentation of both absolute and relative effect sizes is recommended | ||
| Ancillary analyses | 18 | Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing pre-specified from exploratory | |
| Harms | 19 | All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) | |
| Discussion | |||
| Limitations | 20 | Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses | |
| Generalisability | 21 | Generalisability (external validity, applicability) of the trial findings | |
| Interpretation | 22 | Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence | |
| Other information | |||
| Registration | 23 | Registration number and name of trial registry | |
| Protocol | 24 | Where the full trial protocol can be accessed, if available | |
| Funding | 25 | Sources of funding and other support (such as supply of drugs), role of funders | |
References
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive Psychology: An Introduction; American Psychologist: Washington, DC, USA, 2000; Volume 55, pp. 5–14. [Google Scholar]
- Peterson, C. What Is Positive Psychology, and What Is It not? Psychology Today. 2008. Available online: https://www.psychologytoday.com/us/blog/the-good-life/200805/what-is-positive-psychology-and-what-is-it-not (accessed on 16 May 2023).
- Seligman, M.E.P.; Steen, T.A.; Park, N.; Peterson, C. Positive Psychology Progress: Empirical Validation of Interventions. Am. Psychol. 2005, 60, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Tay, L. A Scientific Review of the Remarkable Benefits of Happiness for Successful and Healthy Living. In Happiness: Transforming the Development Landscape, 1st ed.; The Centre for Bhutan Studies and GNH: Trophy, Bhutan, 2017; pp. 90–117. [Google Scholar]
- OECD. OECD Guidelines on Measuring Subjective Wellbeing; OECD Publishing: Paris, France, 2013. [Google Scholar] [CrossRef]
- Stone, B.M.; Parks, A.C. Cultivating subjective wellbeing through positive psychological interventions. In Handbook of Wellbeing; Diener, E., Oishi, S., Tay, L., Eds.; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- McTiernan, K.; Gullon-Scott, F.; Dudley, R. Do Positive Psychology Interventions Impact on the Subjective Wellbeing and Depression of Clients? A Systematic Methodological Review. J. Contemp. Psychother. 2022, 52, 1–13. [Google Scholar] [CrossRef]
- Böhnke, P.; Kohler, U. Wellbeing and Inequality; No. SP I 2008–201; WZB Discussion Paper: Berlin, Germany, 2008. [Google Scholar]
- D’Acci, L. Measuring Wellbeing and Progress; Social Indicators Research: Turin, Italy, 2011; Volume 104, pp. 47–65. [Google Scholar]
- Efklides, A.; Moraitou, D. (Eds.) A Positive Psychology Perspective on Quality of Life; Springer: Dordrecht, The Netherlands, 2013. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On Happiness and Human Potentials: A Review of Research on Hedonic and Eudaimonic Wellbeing. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef]
- What Is Psychological Wellbeing? Available online: https://www.robertsoncooper.com/blog/what-is-psychological-wellbeing/ (accessed on 15 June 2023).
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- Emmons, R.A.; McCullough, M.E. Counting blessings versus burdens: An experimental investigation of gratitude and subjective wellbeing in daily life. J. Personal. Soc. Psychol. 2003, 84, 377–389. [Google Scholar] [CrossRef]
- Sheldon, K.M.; Lyubomirsky, S. How to increase and sustain positive emotion: The effects of expressing gratitude and visualizing best possible selves. J. Posit. Psychol. 2006, 1, 73–82. [Google Scholar] [CrossRef]
- Pinquart, M.; Forstmeier, S. Effects of reminiscence interventions on psychosocial outcomes: A meta-analysis. Aging Ment. Health 2012, 16, 541–558. [Google Scholar] [CrossRef]
- Pietrowsky, R.; Mikutta, J. Effects of Positive Psychology Interventions in Depressive Patients—A Randomized Control Study. Psychology 2012, 3, 1067–1073. [Google Scholar] [CrossRef]
- Chakhssi, F.; Kraiss, J.T.; Sommers-Spijkerman, M.; Bohlmeijer, E.T. The effect of positive psychology interventions on wellbeing and distress in clinical samples with psychiatric or somatic disorders: A systematic review and meta-analysis. BMC Psychiatry 2018, 18, 211. [Google Scholar] [CrossRef]
- Sin, N.L.; Lyubomirsky, S. Enhancing wellbeing and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. J. Clin. Psychol. 2009, 65, 467–487. [Google Scholar] [CrossRef] [PubMed]
- Weiss, L.A.; Westerhof, G.J.; Bohlmeijer, E.T. Can We Increase Psychological Wellbeing? The Effects of Interventions on Psychological Wellbeing: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2016, 11, e0158092. [Google Scholar] [CrossRef] [PubMed]
- Dementia Statistics Hub. Available online: https://dementiastatistics.org/about-dementia/prevalence-and-incidence/ (accessed on 1 June 2023).
- World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 1 June 2023).
- Petersen, R.C.; Negash, S. Mild Cognitive Impairment: An Overview. CNS Spectr. 2008, 13, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Gates, N.; Valenzuela, M.; Sachdev, P.S.; Singh, F. Psychological wellbeing in individuals with mild cognitive impairment. Clin. Interv. Aging 2014, 9, 779–792. [Google Scholar] [CrossRef]
- dos Santos, S.B.; Rocha, G.P.; Fernandez, L.L.; de Padua, A.C.; Reppold, C.T. Association of Lower Spiritual Wellbeing, Social Support, Self-Esteem, Subjective Wellbeing, Optimism and Hope Scores with Mild Cognitive Impairment and Mild Dementia. Front. Psychol. 2018, 9, 371. [Google Scholar] [CrossRef]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Woodward, M.; Brodaty, H.; McCabe, M.; Masters, C.L.; Naismith, S.L.; Morris, P.; Rowe, C.C.; Walker, P.; Yates, M. Nationally Informed Recommendations on Approaching the Detection, Assessment, and Management of Mild Cognitive Impairment. JAD 2022, 89, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current Concepts in Mild Cognitive Impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.; Cullen, K.; Keeney, C.; Canning, C.; Mooney, O.; Chinseallaigh, E.; O’dowd, A. Effectiveness of positive psychology interventions: A systematic review and meta-analysis. J. Posit. Psychol. 2021, 16, 749–769. [Google Scholar] [CrossRef]
- Cohen, G.D.; Firth, K.M.; Biddle, S.; Lloyd Lewis, M.J.; Simmens, S. The First Therapeutic Game Specifically Designed and Evaluated for Alzheimer’s Disease. Am. J. Alzheimer’s Dis. Other Dement. 2009, 23, 540–551. [Google Scholar] [CrossRef]
- Paller, K.A.; Creery, J.D.; Florczak, S.M.; Weintraub, S.; Mesulam, M.-M.; Reber, P.J.; Kiragu, J.; Rooks, J.; Safron, A.; Morhardt, D.; et al. Benefits of Mindfulness Training for Patients with Progressive Cognitive Decline and Their Caregivers. Am. J. Alzheimer’s Dis. Other Dement. 2015, 30, 257–267. [Google Scholar] [CrossRef]
- Phillips, L.J.; Reid-Arndt, S.A.; Pak, Y. Effects of a Creative Expression Intervention on Emotions, Communication, and Quality of Life in Persons with Dementia. Nurs. Res. 2010, 59, 417–425. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- American Psychiatric Association, DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5TM, 5th ed.; American Psychiatric Publishing, Inc.: Washington, DC, USA, 2013. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Tsolaki, M.; Chantzi, H.; Kazis, A. Mini Mental State Examination (MMSE): A validation study in Greece. Am. J. Alzheimer’s Dis. Other Dementiasr 2000, 15, 342–345. [Google Scholar] [CrossRef]
- Reisberg, B.; Ferris, S.H.; De Leon, M.J.; Crook, T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar] [PubMed]
- Pezirkianidis, C.; Stalikas, A.; Lakioti, A.; Yotsidi, V. Validating a multidimensional measure of wellbeing in Greece: Translation, factor structure, and measurement invariance of the PERMA Profiler. Curr. Psychol. 2021, 40, 3030–3047. [Google Scholar] [CrossRef]
- Bryant, F.B.; Smart, C.M.; King, S.P. Using the Past to Enhance the Present: Boosting Happiness Through Positive Reminiscence. J. Happiness Stud. 2005, 6, 227–260. [Google Scholar] [CrossRef]
- Macfarlane, J. Positive psychology: Kindness and its role within mental health nursing. Br. J. Ment. Health Nurs. 2020, 9, 1–10. [Google Scholar] [CrossRef]
- Gander, F.; Proyer, R.T.; Ruch, W.; Wyss, T. Strength-Based Positive Interventions: Further Evidence for Their Potential in Enhancing Wellbeing and Alleviating Depression. J. Happiness Stud. 2013, 14, 1241–1259. [Google Scholar] [CrossRef]
- IBM Corp, IBM SPSS Statistics for Windows, Version 27.0; IBM Corp: Armonk, NY, USA, 2020.
- Akimbekov, N.S.; Razzaque, M.S. Laughter therapy: A humor-induced hormonal intervention to reduce stress and anxiety. Curr. Res. Physiol. 2021, 4, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Sander, D.; Scherer, K. Oxford Companion to Emotion and the Affective Sciences; Series in Affective Science; OUP Oxford: Oxford, UK, 2009; Available online: https://search-ebscohost-com.ezproxy.leidenuniv.nl/login.aspx?direct=true&db=e000xww&AN=1825774&site=ehost-live (accessed on 16 June 2023).
- Lewis, C.N. Reminiscing and Self-Concept in Old Age. J. Gerontol. 1971, 26, 240–243. [Google Scholar] [CrossRef]
- Hughston, G.A.; Merriam, S.B. Reminiscence: A Nonformal Technique for Improving Cognitive Functioning in the Aged. Int. J. Aging Hum. Dev. 1983, 15, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, M.Y.; DeSteno, D. Gratitude and Prosocial Behavior. Psychol. Sci. 2006, 17, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Warneken, F. How children solve the two challenges of cooperation. Annu. Rev. Psychol. 2018, 69, 205–229. [Google Scholar] [CrossRef] [PubMed]
- Dunn, E.W.; Aknin, L.B.; Norton, M.I. Spending money on others promotes happiness. Science 2008, 319, 1687–1688. [Google Scholar] [CrossRef]
- Mongrain, M.; AnselmoMatthews, T. Do positive psychology exercises work? A replication of Seligman et al. (2005). J. Clin. Psychol. 2012, 68, 382–389. [Google Scholar] [CrossRef]
- Ho, H.C.; Yeung, D.Y.; Kwok, S.Y. Development and evaluation of the positive psychology intervention for older adults. J. Posit. Psychol. 2014, 9, 187–197. [Google Scholar] [CrossRef]
- Skevington, S.; Böhnke, J. How is subjective wellbeing related to quality of life? Do we need two concepts and both measures. Soc. Sci. Med. 2018, 206, 22–30. [Google Scholar] [CrossRef]
- Li, C.; Xia, Y.; Zhang, Y. Relationship between subjective wellbeing and depressive disorders: Novel findings of cohort variations and demographic heterogeneities. Front. Psychol. 2022, 13, 1022643. [Google Scholar] [CrossRef]
- Cohn, M.A.; Fredrickson, B.L. In search of durable positive psychology interventions: Predictors and consequences of long-term positive behavior change. J. Posit. Psychol. 2010, 5, 355–366. [Google Scholar] [CrossRef] [PubMed]












| Variables | Experimental | Control |
|---|---|---|
| M (S.D.) | M (S.D.) | |
| Age (in years) | 71.62(4.3) | 72.71(4.9) |
| Men % (n) | 9.5% (2) | 14.3% (3) |
| Women % (n) | 90.5% (19) | 85.7% (18) |
| Primary education (n) | 14.3% (3) | 9.5% (2) |
| Secondary education (n) | 33.3% (7) | 47.6% (10) |
| Higher education (n) | 52.3% (11) | 42.9% (9) |
| Session | Themes | Purpose | Brief Description |
|---|---|---|---|
| 1 | Gratitude | The first session aimed to introduce the group members and learn about the benefits of gratitude. Cultivate gratitude, increase awareness of positive aspects of life, foster a positive outlook, enhance overall wellbeing, and develop a more optimistic perspective. | Three good things in life: Individuals were encouraged to reflect on and document for one week three positive events or experiences that occurred during their day, along with an explanation of why these events were meaningful or significant to them. |
| 2 | Gratitude | The second session aimed to better understand the concept of gratitude and how it can be put into practice. Increase feelings of appreciation, strengthen relationships, foster a sense of connection and wellbeing, experience an uplift in positive emotions, and develop a greater sense of gratitude towards others. | Gratitude visit: Individuals were encouraged to write a letter expressing gratitude to someone who has positively impacted their lives but has not been properly thanked. After composing the letter, individuals were also encouraged to arrange a meeting with the recipient and read the letter aloud, expressing their gratitude in person. |
| 3 | Positive reminiscence | In session three, the goal was to talk about the benefits of memories and how they can be used in our own favor. Emotional wellbeing, improved self-esteem, increased life satisfaction, and stress reduction are among its great benefits. | The magic box of memories: Individuals were told to each pick, write down, and read out loud one positive memory from their past. Based on what that memory was about, the other members of the subgroup were instructed to share a similar positive memory of their own. Participants were also requested to locate an object or item that serves as a reminder of their chosen positive experience. |
| 4 | Humor | The fourth session introduced the concept of humor and its benefits. Enhance positive emotions and overall wellbeing, reduces stress, increase social connections, foster positive relationships, improve communication, and promote a positive perspective, resilience, and coping skills. | Three funny things: Participants were asked to write down 3 funny things that happened to them during that day or the previous one. They were encouraged to recall the details of these funny experiences, relive the laughter or amusement they brought, and reflect on the positive emotions associated with them. |
| 5 | Kindness | In session number five, the goal was to talk about kindness and mention the benefits of the offer. Promote compassion, empathy, and prosocial behavior, contribute to the wellbeing of others, and experience increased positive emotions, a sense of fulfillment, and a strengthened sense of community. | Random acts of kindness: Participants were encouraged to first brainstorm and then perform for one-week acts of kindness, such as helping someone in need, offering a kind gesture, or performing small acts of generosity, without any expectation of reward or recognition. |
| 6 | Character strengths | In the last session, the subject was to identify and understand the positive qualities/strengths everyone carries and to close the intervention. Increase self-awareness, brings up a positive identity, and promote personal growth and development. | You at your best: Participants were asked to recall and reflect on a specific moment or experience in their life when they felt at their best, accomplished, or in a state of flow. It could be a personal achievement, a fulfilling project, or a time when he overcame a challenge. Then, they were asked to identify the personal strengths or qualities that they showed at that moment. |
| Overall Wellbeing 1 | Overall Wellbeing 2 | Overall Wellbeing 3 | |
|---|---|---|---|
| Mean (S.D.) | Experimental 6.8 (1.3) Control 6.6 (1.3) | Experimental 7.2 (1.3) Control 6.6 (1.3) | Experimental 7.5 (1.0) Control 6.6 (1.3) |
| Positive Emotion 1 | Positive Emotion 2 | Positive Emotion 3 | |
| Mean (S.D.) | Experimental 6.9 (1.6) Control 6.2 (1.9) | Experimental 7.4 (1.2) Control 6.4 (1.6) | Experimental 7.4 (1.2) Control 6.5 (1.3) |
| Relationship 1 | Relationship 2 | Relationship 3 | |
| Mean (S.D.) | Experimental 7.2 (1.9) Control 6.7 (1.9) | Experimental 7.4 (1.8) Control 6.7 (1.5) | Experimental 7.7 (1.7) Control 6.8 (1.6) |
| Engagement 1 | Engagement 2 | Engagement 3 | |
| Mean (S.D.) | Experimental 6.3 (1.6) Control 6.6 (1.2) | Experimental 6.9 (1.7) Control 6.4 (1.2) | Experimental 7.2 (1.3) Control 6.0 (1.4) |
| Meaning 1 | Meaning 2 | Meaning 3 | |
| Mean (S.D.) | Experimental 6.8 (1.7) Control 6.7 (1.4) | Experimental 7.1 (1.7) Control 6.4 (1.5) | Experimental 7.5 (1.3) Control 6.8 (1.6) |
| Accomplishment 1 | Accomplishment 2 | Accomplishment 3 | |
| Mean (S.D.) | Experimental 6.8 (1.5) Control 7.0 (1.2) | Experimental 6.9 (1.6) Control 6.9 (1.5) | Experimental 7.5 (1.0) Control 6.9 (1.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsiflikioti, K.; Moraitou, D.; Pezirkianidis, C.; Papantoniou, G.; Sofologi, M.; Kougioumtzis, G.A.; Tsolaki, M. Enhancing Subjective Wellbeing in Older Individuals with Amnestic Mild Cognitive Impairment: A Randomized Trial of a Positive Psychology Intervention. Behav. Sci. 2023, 13, 838. https://doi.org/10.3390/bs13100838
Tsiflikioti K, Moraitou D, Pezirkianidis C, Papantoniou G, Sofologi M, Kougioumtzis GA, Tsolaki M. Enhancing Subjective Wellbeing in Older Individuals with Amnestic Mild Cognitive Impairment: A Randomized Trial of a Positive Psychology Intervention. Behavioral Sciences. 2023; 13(10):838. https://doi.org/10.3390/bs13100838
Chicago/Turabian StyleTsiflikioti, Konstantina, Despoina Moraitou, Christos Pezirkianidis, Georgia Papantoniou, Maria Sofologi, Georgios A. Kougioumtzis, and Magdalini Tsolaki. 2023. "Enhancing Subjective Wellbeing in Older Individuals with Amnestic Mild Cognitive Impairment: A Randomized Trial of a Positive Psychology Intervention" Behavioral Sciences 13, no. 10: 838. https://doi.org/10.3390/bs13100838
APA StyleTsiflikioti, K., Moraitou, D., Pezirkianidis, C., Papantoniou, G., Sofologi, M., Kougioumtzis, G. A., & Tsolaki, M. (2023). Enhancing Subjective Wellbeing in Older Individuals with Amnestic Mild Cognitive Impairment: A Randomized Trial of a Positive Psychology Intervention. Behavioral Sciences, 13(10), 838. https://doi.org/10.3390/bs13100838