

ACTIVE YOU: Teacher Attributes and Attitudes Predicting Physical Activity Promotion


Abstract
:1. Introduction
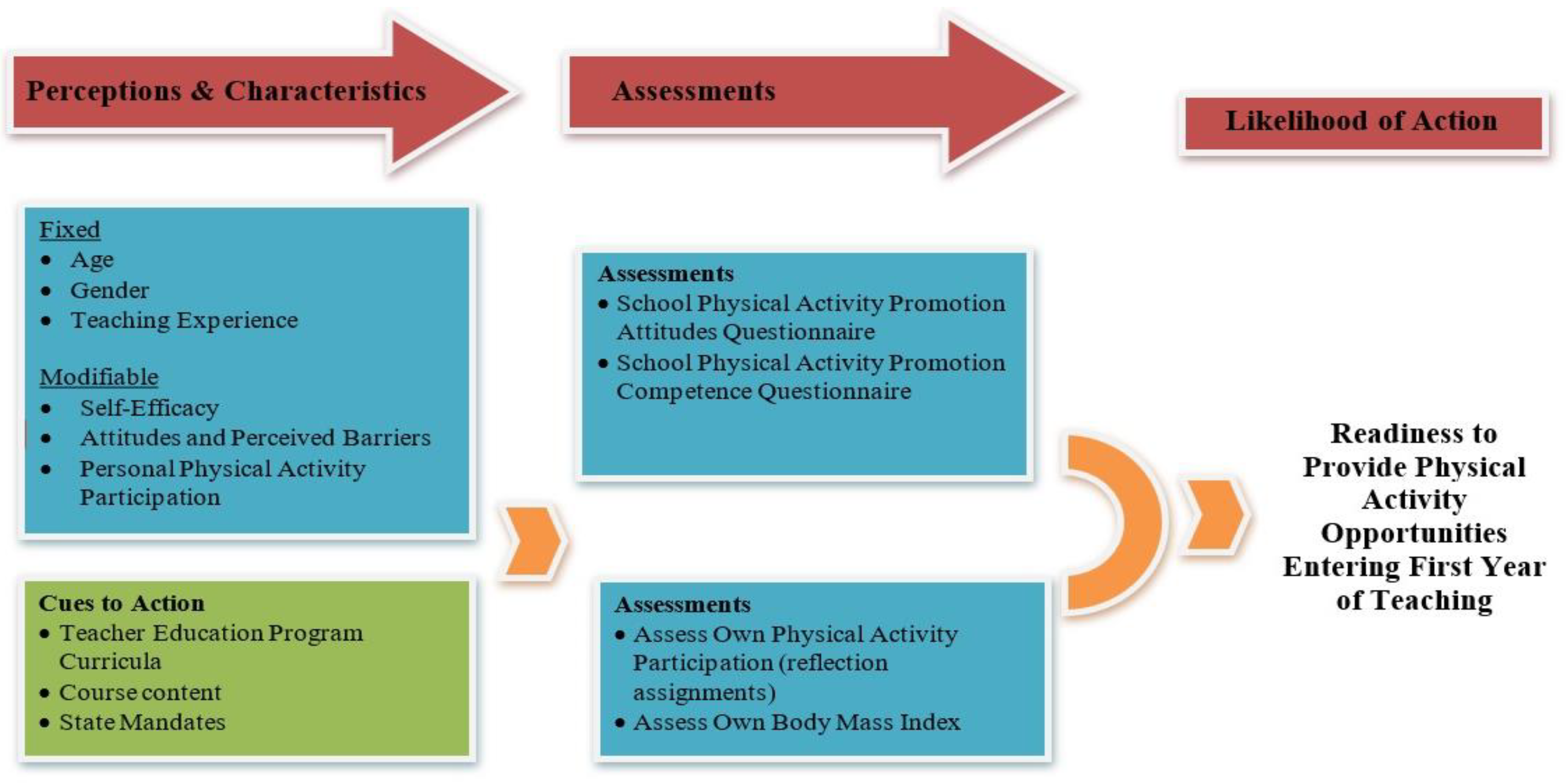
1.1. Theoretical Framework: Health Belief Model
1.2. Teacher Education: Beliefs and Self-Efficacy
1.3. Teachers as Health Promoters in Schools
2. Materials and Methods
2.1. Participants
2.2. Instruments and Measures
2.2.1. Daily Physical Activity Measures of Self
2.2.2. Biographical Questionnaire of Physical Self and Self-Perceptions of Ability
2.2.3. School Physical Activity Promotion Competence (SPAPC)
2.2.4. School Physical Activity Promotion Attitudes (SPAPA)
2.2.5. Power Analysis
2.3. Data Collection Procedures
2.4. Statistical Analysis
3. Results
3.1. Correlation Table Participant Characteristics, BMI, and Physical Activity Level
3.2. Hierarchical Regression Analysis
3.3. Logistical Regression Analysis
4. Discussion
4.1. Teacher Education and Preservice Teachers’ Health
4.2. Teacher Education and Preservice Teachers’ Physical Activity Promotion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical activity, fitness, cognitive function, and academic achievement in children: A systematic review. Med. Sci. Sport. Exerc. 2016, 48, 1197. [Google Scholar] [CrossRef] [Green Version]
- Lubans, D.R.; Leahy, A.A.; Mavilidi, M.F.; Valkenborghs, S.R. Physical Activity, Fitness, and Executive Functions in Youth: Effects, Moderators, and Mechanisms. In Sensitive Periods of Brain Development and Preventive Interventions, 1st ed.; Anderson, S., Ed.; Springer Nature: Cham, Switzerland, 2021; pp. 103–130. [Google Scholar]
- Peterson, J.W.; Loeb, S.; Chamberlain, L.J. The intersection of health and education to address school readiness of all children. Pediatrics 2018, 142, e20181126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, D.E.; Greenberg, M.; Crowley, M. Early social-emotional functioning and public health: The relationship between kindergarten social competence and future wellness. Am. J. Public Health 2015, 105, 2283–2290. [Google Scholar] [CrossRef]
- Webster, C.A.; Zarrett, N.; Cook, B.S.; Egan, C.; Nesbitt, D.; Weaver, R.G. Movement integration in elementary classrooms: Teacher perceptions and implications for program planning. Eval. Program Plan. 2017, 61, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Webster, C.A.; Starrett, A.; Rehling, J.; Chen, B.; Beets, M.W.; Weaver, R.G. Understanding Elementary Classroom Teachers’ Use of Movement Integration Resources. In Frontiers in Education; Frontiers Media SA: Lausanne, Switzerland, 2020; Volume 5, p. 56. [Google Scholar]
- Bartholomew, J.B.; Golaszewski, N.M.; Jowers, E.; Korinek, E.; Roberts, G.; Fall, A.; Vaughn, S. Active learning improves on-task behaviors in 4th grade children. Prev. Med. 2018, 111, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Efstathiou, N.T.; Risvas, G.S.; Theodoraki, E.-M.M.; Galanaki, E.P.; Zampelas, A.D. Health education: Effects on classroom climate and physical activity. Health Educ. J. 2016, 75, 799–810. [Google Scholar] [CrossRef]
- Byrne, J.; Pickett, K.; Rietdijk, W.; Shepherd, J.; Grace, M.; Roderick, P. A longitudinal study to explore the impact of preservice teacher health training on early career teachers’ roles as health promoters. Pedagog. Health Promot. 2016, 2, 170–183. [Google Scholar] [CrossRef]
- Jourdan, D.; Gray, N.J.; Barry, M.M.; Caffe, S.; Cornu, C.; Diagne, F.; El Hage, F.; Farmer, M.Y.; Slade, S.; Marmot, M.; et al. Supporting every school to become a foundation for healthy lives. Lancet Child Adolesc. Health 2021, 5, 295–303. [Google Scholar] [CrossRef]
- Speller, V.; Byrne, J.; Dewhirst, S.; Almond, P.; Mohebati, L.; Norman, M.; Polack, S.; Memon, A.; Grace, M.; Margetts, B.; et al. Developing trainee school teachers’ expertise as health promoters. Health Educ. 2010, 110, 490–507. [Google Scholar] [CrossRef] [Green Version]
- Pulimeno, M.; Piscitelli, P.; Miani, A.; Colao, A.; Colazzo, S. Training Teachers as Health Promoters. JDREAM. J. Interdiscip. REsearch Appl. Med. 2020, 4, 37–46. [Google Scholar]
- Webster, C.; Monsma, E.; Erwin, H. The role of biographical characteristics in preservice classroom teachers’ school physical activity promotion attitudes. J. Teach. Phys. Educ. 2010, 29, 358–377. [Google Scholar] [CrossRef]
- Webster, C. Relationships between personal biography and changes in preservice classroom teachers’ physical activity promotion competence and attitudes. J. Teach. Phys. Educ. 2011, 30, 320–339. [Google Scholar] [CrossRef]
- Shepherd, J.; Pickett, K.; Dewhirst, S.; Byrne, J.; Speller, V.; Grace, M.; Almond, P.; Roderick, P. Initial teacher training to promote health and well-being in schools–A systematic review of effectiveness, barriers and facilitators. Health Educ. J. 2016, 75, 721–735. [Google Scholar] [CrossRef] [Green Version]
- Dugger, R.; Rafferty, A.; Hunt, E.; Beets, M.; Webster, C.; Chen, B.; Rehling, J.; Weaver, R.G. Elementary classroom teachers’ self-reported use of movement integration products and perceived facilitators and barriers related to product use. Children 2020, 7, 143. [Google Scholar] [CrossRef]
- Castelli, D.; Williams, L. Health-related fitness and physical education teachers’ content knowledge. J. Teach. Phys. Educ. 2007, 26, 3–19. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Neumark-Sztainer, D.; Story, M.; Harris, T. Beliefs and attitudes about obesity among teachers and school health care providers working with adolescents. J. Nutr. Educ. 1999, 31, 3–9. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Worth Publishers: New York, NY, USA, 1997. [Google Scholar]
- Randall, L.; Maeda, J.K. Pre-service elementary generalist teachers’ past experiences in elementary physical education and influence of these experiences on current beliefs. Brock Educ. J. 2010, 19, 20–35. [Google Scholar] [CrossRef] [Green Version]
- Morris, D.B.; Usher, E.L.; Chen, J.A. Reconceptualizing the sources of teaching self-efficacy: A critical review of emerging literature. Educ. Psychol. Rev. 2017, 29, 795–833. [Google Scholar] [CrossRef]
- Pan, Y.H. Relationships among teachers’ self-efficacy and students’ motivation, atmosphere, and satisfaction in physical education. J. Teach. Phys. Educ. 2014, 33, 68–92. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Increasing Physical Education and Physical Activity: A Framework for Schools; Centers for Disease Control and Prevention, US Dept of Health and Human Services: Atlanta, GA, USA, 2019. [Google Scholar]
- Orlowski, M.; Lorson, K.; Lyon, A.; Minoughan, S. My classroom physical activity pyramid: A tool for integrating movement into the classroom. J. Phys. Educ. Recreat. Danc. 2013, 84, 47–51. [Google Scholar] [CrossRef]
- Pavlovic, A.; DeFina, L.F.; Natale, B.L.; Thiele, S.E.; Walker, T.J.; Craig, D.W.; Vint, G.R.; Leonard, D.; Haskell, W.L.; Kohl, H.W. Keeping children healthy during and after COVID-19 pandemic: Meeting youth physical activity needs. BMC Public Health 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kohl, H.W., III; Cook, H.D. (Eds.) Educating the Student Body: Taking Physical Activity and Physical Education to School; National Academy of Sciences, Institute of Medicine: Washington DC, USA, 2013. [Google Scholar]
- Goh, T.L.; Hannon, J.C.; Webster, C.A.; Podlog, L. Classroom teachers’ experiences implementing a movement integration program: Barriers, facilitators, and continuance. Teach. Teach. Educ. 2017, 66, 88–95. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montoye, A.H.; Begum, M.; Henning, Z.; Pfeiffer, K.A. Comparison of linear and non-linear models for predicting energy expenditure from raw accelerometer data. Physiol. Meas. 2017, 38, 343. [Google Scholar] [CrossRef] [PubMed]
- Maitland, A. How many scale points should I include for attitudinal questions? Surv. Pract. 2009, 2, 2950. [Google Scholar] [CrossRef] [Green Version]
- Love, R.; Adams, J.; van Sluijs, E.M.; Foster, C.; Humphreys, D. A cumulative meta-analysis of the effects of individual physical activity interventions targeting healthy adults. Obes. Rev. 2018, 19, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Meyers, L.S.; Gamst, G.; Guarino, A.J. Applied Multivariate Research: Design and Interpretation; Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Tudor-Locke, C.E.; Myers, A.M. Methodological considerations for researchers and practitioners using pedometers to measure physical (ambulatory) activity. Res. Q. Exerc. Sport 2001, 72, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011-2012. Jama 2014, 311, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.W.; Popkin, B.M. Time use and physical activity: A shift away from movement across the globe. Obes. Rev. 2012, 13, 659–680. [Google Scholar] [CrossRef] [Green Version]
- Lamanauskas, V. Teacher health literacy: Why does it matter? Probl. Educ. 21st Century 2018, 76, 4–6. [Google Scholar] [CrossRef]
- Miller, R.T.; Murnane, R.J.; Willett, J.B. Do teacher absences impact student achievement? Longitudinal evidence from one urban school district. Educ. Eval. Policy Anal. 2008, 30, 181–200. [Google Scholar] [CrossRef] [Green Version]
- Weaver, R.G.; Webster, C.A.; Beets, M.W.; Brazendale, K.; Chandler, J.; Schisler, L.; Aziz, M. Initial outcomes of a participatory-based, competency-building approach to increasing physical education teachers’ physical activity promotion and students’ physical activity: A pilot study. Health Educ. Behav. 2018, 45, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Bajorek, Z.; Gulliford, J.; Taskila, T. Healthy Teachers, Higher Marks. Establishing a Link between Teacher Health & Well-Being, and Student Outcomes; The Work Foundation: London, UK, 2014; p. 34. [Google Scholar]
- Zach, S.; Harari, I.; Harari, N. Changes in teaching efficacy of preservice teachers in physical education. Phys. Educ. Sport Pedagog. 2012, 17, 447–462. [Google Scholar] [CrossRef]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sport. Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Braithwaite, R.E.; Biddle, S.J.; van Sluijs, E.M.; Atkin, A.J. Associations between sedentary behaviour and physical activity in children and adolescents: A meta-analysis. Obes. Rev. 2014, 15, 666–675. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Item No | Item |
|---|---|
| Brief Name | ACTIVE YOU—Preparing teachers to be health promoters in schools by building self-efficacy and reflecting on their participation in physical activity as a health-protective factor. |
| Why? | Reasons why this intervention matters at this time:
|
| What? | The intervention group participated in learning activities designed to increase personal and student participation in physical activity: (a) measurement, evaluation, and reflection on their physical fitness and physical activity participation; (b) planning and teaching a movement integration (MI) activity in the classroom using a task card from Promoting Physical Activity and Health in the Classroom (Pangrazi, Beighle, and Pangrazi, 2021); (c) vicarious experience a whole-of-school-approach through fieldwork; and (d) conducting a model teach with elementary school children and engaging in cognitive coaching debriefing with the cooperating teacher and teacher educator. |
| Who provided? | A single faculty member from one large university in the southern portion of the United States delivered the content across the six sections for the feasibility and proof of concept study. In the fieldwork, there were 15 co-teachers trained in mentoring and cognitive coaching. |
| How? | The students met on campus for 180 min per week in a classroom with an attached open space where they could participate in MI and were in a public school where they co-taught in schools for 10 h per week. |
| Where? | The primary delivery of the content occurred on the university campus, with the preservice teachers designing and delivering their lessons in public elementary schools in a predominantly metropolitan area. |
| Tailoring? | The only individualization or tailoring that occurred was accommodation by the preservice teachers to allow ALL K-6 students in their fieldwork to participate in the physical activity lesson they created. |
| Modifications? | In parallel with the 2018 Physical Activity Guidelines for Americans, each study participant was expected to engage in 150 min of moderate-to-vigorous physical activity each week. |
| How well? | Fidelity to the treatment was confirmed in multiple ways: (a) the same instructor delivered the content in all sections; (b) the physical activity logs and reflections were submitted electronically through the courseware website and were time-stamped; and (c) the same prompts were released at the same time for the fall and spring sections. There were no disruptions in the schedule (e.g., school or class cancellations). |
| Variables | (n = 233) (M [SD]) |
|---|---|
| Age (years; M [SD]) | 20.17 [2.60] |
| Gender (female, n [%]) | 211 [90.55] |
| Race (n [%]) | |
| White | 129 [55.36] |
| Hispanic | 73 [31.33] |
| Asian | 19 [8.15] |
| Black | 8 [3.43] |
| More than 1 race | 4 [1.71] |
| Year in Teacher Education (n [%]) | 39 [16.73] |
| 1st year | 84 [36.05] |
| 2nd year | 65 [27.89] |
| 3rd year | 30 [12.87] |
| 4th year | 15 [6.43] |
| 5th year | 22.38 [3.68] |
| BMI 1 (kg/m2; M [SD]) | |
| Physical Activity Level (steps; M [SD]) | 7880.32 [2861.66] |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| BMI (kg/m2) | - | |||||
| Physical Activity Level | 0.01 | - | ||||
| Past PA Experience | −0.08 | 0.06 | - | |||
| Perceived PA Competence | −0.11 | 0.28 b | 0.44 b | - | ||
| Attitudes toward PA Promotion | −0.17 b | 0.15 a | 0.33 b | 0.29 b | - | |
| Self-Efficacy toward PA Promotion | −0.07 | 0.06 | 0.21 b | 0.24 b | 0.27 | - |
| Predictor | R2 | β | t | p Value | |
|---|---|---|---|---|---|
| First step | Attitudes toward PA | ||||
| Previous PA Experience | 0.13 | 0.24 | 3.62 | 0.010 | |
| Perceived PA Competence | 0.17 | 2.60 | 0.001 | ||
| Second step | Previous PA Experience | 0.16 | 0.25 | 3.27 | 0.001 |
| Perceived PA Competence | 0.14 | 1.97 | 0.049 | ||
| Daily PA Level (steps) | 0.15 | 2.04 | 0.042 | ||
| BMI (Kg/m2) | −0.15 | −2.45 | 0.015 | ||
| First Step | Self-Efficacy toward PA | 0.07 | |||
| Previous PA Experience | 0.10 | 1.40 | 0.16 | ||
| Perceived PA Competence | 0.18 | 2.54 | 0.01 | ||
| Second step | Previous PA Experience | 0.08 | 0.09 | 1.32 | 0.19 |
| Perceived PA Competence | 0.19 | 2.47 | 0.01 | ||
| Daily PA Level (steps) | 0.08 | 1.23 | 0.22 | ||
| BMI (Kg/m2) | 0.00 | 0.01 | 0.99 |
| Predictor | Β | SE | Odds Ratio | 95% CI | p Value |
|---|---|---|---|---|---|
| BMI Classification | |||||
| PA level (steps) | −0.01 | 0.01 | 0.99 | (0.99–0.99) | 0.001 |
| Perceived PA Competence | −0.18 | 0.08 | 0.83 | (0.71–0.96) | 0.017 |
| Previous PA Experience | 0.11 | 0.08 | 1.11 | (0.95–1.29) | 0.17 |
| Attitudes toward PA | −0.04 | 0.06 | 0.99 | (0.85–1.07) | 0.54 |
| Self-Efficacy toward PA | −0.01 | 0.01 | 0.96 | (0.97–1.01) | 0.44 |
| Daily PA Level | |||||
| BMI (Kg/m2) | 0.01 | 0.05 | 1.01 | (0.91–1.12) | 0.80 |
| Perceived PA Competence | −0.37 | 0.08 | 0.69 | (0.58–0.82) | 0.001 |
| Previous PA Experience | 0.14 | 0.08 | 1.14 | (0.97–1.34) | 0.09 |
| Attitudes toward PA | 0.01 | 0.01 | 1.00 | (0.98–1.01) | 0.90 |
| Self-Efficacy toward PA | −0.2 | 0.07 | 0.98 | (0.85–1.12) | 0.88 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Centeio, E.E.; Jung, Y.; Castelli, D.M. ACTIVE YOU: Teacher Attributes and Attitudes Predicting Physical Activity Promotion. Behav. Sci. 2023, 13, 210. https://doi.org/10.3390/bs13030210
Centeio EE, Jung Y, Castelli DM. ACTIVE YOU: Teacher Attributes and Attitudes Predicting Physical Activity Promotion. Behavioral Sciences. 2023; 13(3):210. https://doi.org/10.3390/bs13030210
Chicago/Turabian StyleCenteio, Erin E., Yeonhak Jung, and Darla M. Castelli. 2023. "ACTIVE YOU: Teacher Attributes and Attitudes Predicting Physical Activity Promotion" Behavioral Sciences 13, no. 3: 210. https://doi.org/10.3390/bs13030210