
Pain Perceptions, Suffering and Pain Behaviours of Professional and Pre-Professional Dancers towards Pain and Injury: A Qualitative Review


Abstract
:1. Introduction
2. Material and Methods
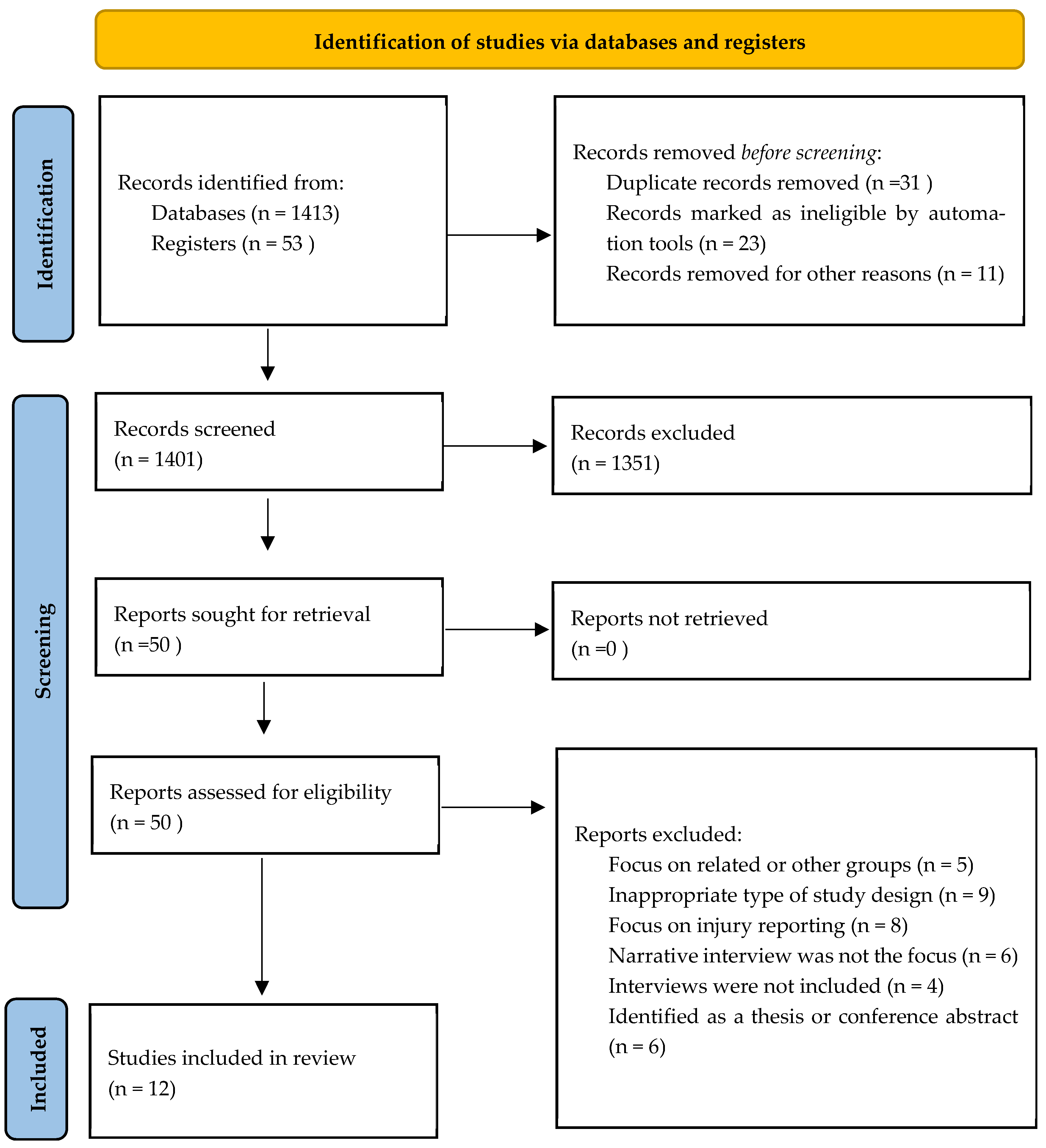
2.1. Stage 1: Systematic Search
2.1.1. Inclusion Criteria
2.1.2. Data Sources
2.1.3. Electronic Search Strategy
2.1.4. Study Screening Methods and Data Extraction
2.2. Stage 2: Quality Appraisal
2.3. Stage 3: Synthesis
3. Results
3.1. Demographics
3.2. Critical Appraisal
3.3. Synthesis
4. Theme 1: Developing Positive and Adapted Perceptions and Behaviours Relating to Pain
4.1. Sub-Theme 1: The Perception of Pain (Moderate CerQual Evidence Rating)
4.2. Sub-Theme 2: The Experience of Pain (Low CerQual Evidence Rating)
4.3. Sub-Theme 3: Cognitive Strategies Used to Enhance Performance and Cope with Pain (Moderate CerQual Evidence Rating)
5. Theme 2: The Impact and Danger of Embracing Pain and the Risk of Injury
5.1. Sub-Theme 1: The Ability to Recognise and Manage Pain and Injury (Low CerQual Evidence Rating)
5.2. Sub-Theme 2: The Cost of Being out of Performance (Low CerQual Evidence Rating)
6. Theme 3: Factors That Influenced the Response to Injury and Ability to Perform
6.1. Sub-Theme 1: The Ability to Self-Manage (Moderate CerQual Evidence Rating)
6.2. Sub-Theme 2: Pain Threshold and the Culture of Hardiness (Moderate CerQual Evidence)
6.3. Sub-Theme 3: Fear-Related Preconceptions (Low CerQual Evidence)
6.4. Sub-Theme 4: Performance Pressures (Moderate CerQual Evidence)
7. Discussion
7.1. Practical Implications
7.2. Limitations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McEwen, K.; Young, K. Ballet and pain: Reflections on a risk-dance culture. Qual. Res. Sport Exerc. Health 2011, 3, 152–173. [Google Scholar] [CrossRef]
- Aalten, A. Listening to the dancer’s body. Sociol. Rev. Monogr. 2007, 55, 109–125. [Google Scholar] [CrossRef]
- Blanchfield, D. The Gale Encyclopedia of Children’s Health: Infancy through Adolescence, 3rd ed.; Gale, Cengage Learning: Farmington Hills, MI, USA, 2016. [Google Scholar]
- Hincapié, C.A.; Morton, E.J.; Cassidy, J.D. Musculoskeletal Injuries and Pain in Dancers: A Systematic Review. Arch. Phys. Med. Rehabil. 2008, 89, 1819–1829. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H.; Tarr, J. Dancers’ Perceptions of Pain and Injury: Positive and Negative Effects. J. Danc. Med. Sci. 2009, 13, 51–59. [Google Scholar]
- Harrison, C.; Ruddock-Hudson, M. Perceptions of Pain, Injury, and Transition-Retirement: The Experiences of Professional Dancers. J. Danc. Med. Sci. 2017, 21, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Liederbach, M.; Hagins, M.; Gamboa, J.M.; Welsh, T.M. Assessing and reporting dancer capacities, risk factors and injuries. Recommendations from the IADMS standard measures consensus initiative. J. Danc. Med. Sci. 2012, 15, 139–153. [Google Scholar]
- Mainwaring, L.M.; Finney, C. Psychological Risk Factors and Outcomes of Dance Injury: A Systematic Review. J. Danc. Med. Sci. 2017, 21, 87–96. [Google Scholar] [CrossRef]
- Heil, J.; Fine, P. Pain in sport: A biopsychological perspective. Psychol. Bases Sport Inj. 1999, 2, 13–28. [Google Scholar]
- Vassallo, A.; Pappas, E.; Stamatakis, E.; Hiller, C. Injury Fear, Stigma, and Reporting in Professional Dancers. Saf. Health Work. 2019, 10, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Mainwaring, L.; Krasnow, D.; Kerr, G. And the Dance Goes On Psychological Impact of Injury. J. Danc. Med. Sci. 2001, 5, 105–115. [Google Scholar]
- Petty, N.; Thomson, O.; Stew, G. Ready for a paradigm shift? Part 1: Introducing the philosophy of qualitative research. Man. Ther. 2012, 17, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Petty, N.; Thomson, O.; Stew, G. Ready for a paradigm shift? Part 2: Introducing qualitative research methodologies and methods. Man. Ther. 2012, 17, 378–384. [Google Scholar] [CrossRef] [Green Version]
- Wainwright, S.; Turner, B. Reflections on embodiment and vulnerability. J. Med. Ethics Med. Humanit. 2003, 29, 4–7. [Google Scholar] [CrossRef] [Green Version]
- Allen, N.; Ribbans, W.; Nevill, A.; Wyon, M. Musculoskeletal Injuries in Dance: A Systematic Review. Int. J. Phys. Med. Rehabil. 2014, 3, 1–8. [Google Scholar]
- Markula, P. (Im)Mobile bodies: Contemporary semi-professional dancers experiences with injuries. Int. Rev. Sociol. Sport 2015, 50, 840–864. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, A.; Flemming, K.; Mclnnes, E.; Oliver, S.; Craig, J. Enhancing the transparency in report the synthesis of qualitative research. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, C.; Mays, N.; Popay, J. Synthesizing Qualitative and Quantitative Health Research: A Guide to Methods; McGraw-Hill Education: London, UK, 2007. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER Tool for Qualitative Evidence Synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Dance Spirit. The Age Equation 2012. Available online: https://www.dancespirit.com/the-age-equation-2326145152.html. (accessed on 8 July 2022).
- Pollard-Smith, T.; Thomson, O.P. Professional ballet dancers’ experience of injury and osteopathic treatment in the UK: A qualitative study’. J. Bodyw. Mov. Ther. 2016, 21, 148–156. [Google Scholar] [CrossRef]
- Steen, M.; Downe, S.; Bamford, N.; Edozien, L. Not-patient and not-visitor: A metasynthesis fathers encounters with pregnancy, birth and maternity care. Midwifery 2012, 28, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Soundy, A.; Roskell, C.; Elder, T.; Collett, J.; Dawes, H. The Psychological Processes of Adaptation and Hope in Patients with Multiple Sclerosis: A Thematic Synthesis. Open J. Ther. Rehabil. 2016, 4, 22–47. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, C.; Booth, A. Quality assessment of qualitative evidence for systematic review and synthesis: Is it meaningful, and if so, how should it be performed? Res. Synth. Methods 2015, 6, 149–154. [Google Scholar] [CrossRef]
- Dixon-Woods, M.; Fitzpatrick, R. Qualitative research in systematic reviews. Br. Med. J. 2001, 323, 765–766. [Google Scholar] [CrossRef]
- Bernard, H.; Wutich, A.; Ryan, G. Analyzing Qualitative Data Systematic Approaches, 2nd ed.; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Boeije, H. Analysis in Qualitative Research; SAGE Publications Ltd.: London, UK, 2001. [Google Scholar]
- Campbell, R.; Pound, P.; Morgan, M.; Daker-White, G.; Britten, N.; Pill, R.; Yardley, L.; Pope, C.; Donovan, J. Evaluating Meta-ethnography: Systematic Analysis and Synthesis of Qualitative Research. Health Technol. Assess. 2011, 15, 1–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewin, S.; Booth, A.; Glenton, C.; Munthe-Kaas, H.; Rashidian, A.; Wainwright, M.; Bohren, M.A.; Tunçalp, Ö.; Colvin, C.J.; Garside, R.; et al. Applying GRADE-CERQual to qualitative evidence synthesis findings: Introduction to the series. Implement. Sci. 2018, 13, 2. [Google Scholar] [CrossRef] [Green Version]
- Aalten, A. In the presence of the body: Theorizing training, injuries and pain in Ballet. Danc. Res. J. 2005, 37, 55–72. [Google Scholar] [CrossRef]
- Bolling, C.; van Rijn, R.M.; Pasman, H.R.; van Mechelen, W.; Stubbe, J.H. In your shoes: A qualitative study on the perspectives of professional dancers and staff regarding dance injury and its prevention. Transit. Sports Med. 2020, 4, 386–394. [Google Scholar] [CrossRef]
- Tarr, J.; Thomas, H. Mapping embodiment: Methodologies for representing pain and injury. Qual. Res. 2011, 11, 141–157. [Google Scholar] [CrossRef]
- Tarr, J.; Thomas, H. Good pain, bad pain: Dancers, injury and listening to the body. Danc. Res. 2021, 39, 53–71. [Google Scholar] [CrossRef]
- Wainwright, S.; Turner, B. ‘Just Crumbling to Bits’? An Exploration of the Body, Ageing, Injury and Career in Classical Ballet Dancers. Sociology 2006, 40, 237–255. [Google Scholar] [CrossRef]
- Wainwright, S.; Williams, C.; Turner, B. Fractured identities: Injury and the balletic body. Health Interdiscip. J. Soc. Study Health Illn. Med. 2005, 9, 49–66. [Google Scholar] [CrossRef] [Green Version]
- Arvinen-Barrow, M.; Massey, W.V.; Hemmings, B. Role of Sport Medicine Professionals in Addressing Psychosocial Aspects of Sport-Injury Rehabilitation: Professional Athletes Views. J. Athl. Train. 2014, 49, 764–772. [Google Scholar] [CrossRef] [Green Version]
- Encarnacion, M.; Meyers, M.; Ryan, N.; Pease, D. Pain Coping Styles of Ballet Performers. Med. Sci. Sports Exerc. 1999, 31, S217. [Google Scholar] [CrossRef]
- Allen, J. Written in the body: Reflections on encounters with somatic practices in postgraduate dance training. J. Danc. Somat. Pract. 2009, 1, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Wulff, H. Ballet Across Borders: Career and Culture in the World of Dancers; Berg Publishers: Oxford, UK, 1998. [Google Scholar]
- Young, K. Violence, Risk, and Liability in Male Sports Culture. Sociol. Sport J. 1993, 10, 373–396. [Google Scholar] [CrossRef]
- Roderick, M.; Waddington, I.; Parker, G. Playing Hurt: Managing Injuries in English Professional Football. Int. Rev. Sociol. Sport 2000, 35, 165–180. [Google Scholar] [CrossRef]
- Weinberg, R.B.; Vernau, D.P.; Horn, T.S. Playing through pain and injury: Psychosocial considerations. J. Clin. Sport Psychol. 2013, 7, 41–59. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, L. Advice for Dancers: Emotional Counsel and Practical Strategies; Jossey-Bass Publishers: San Francisco, CA, USA, 1998. [Google Scholar]
- Anderson, R.; Hanrahan, S. Dancing in pain: Pain appraisal and coping in dancers. J. Danc. Med. Sci. 2008, 12, 9–16. [Google Scholar]
- Mallett, R.; Hagen-Zanker, J.; Slater, R.; Duvendack, M. The benefits and challenges of using systematic reviews in international development research. J. Dev. Eff. 2012, 4, 445–455. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study | Participants, Sampling, Setting and Aim | Methodology, Methods and Analysis |
|---|---|---|
| Aalten [2] | Participants: 25 female professional ballet dancers. 9 dance students at professional ballet schools. Male and Female students (numbers not identified). Age: Not detailed. Sampling: Snowball. Setting: Public meeting places or at the participants home. Aim: To analyse the meaning of injuries and pain in the context of ballet culture. Geographical location: The Netherlands. | Methodology: Ethnography. Outcome measures: Formal and informal interviews. Observations Biographical interviews. Analysis: Phenomenological approach. |
| Aalten [33] | Participants: 25 female professional ballet dancers. 9 dance students at professional ballet schools (no gender breakdown given). Age: Not detailed. Sampling: Snowball. Setting: Public meeting places or at the participants home. Aim: To analyse the meaning of injuries and pain in the context of ballet, drawing on the understanding of social identity and how the body is understood by the dancers. Geographical location: The Netherlands. | Methodology: Ethnography. Outcome measures: Formal and informal interviews. Observations. Biographical interviews. Autobiographies of dancers. Analysis: Sociological approach focused on the body. |
| Bolling et al. [34] | Participants: 10 professional ballet dancers (6 female, 4 male). Age: Average 27 years (range 20–35 years) Sampling: Maximum variation. Setting: Not identified. Aim: To consider the dancers’ perceptions of injury. Geographical location: The Netherlands. | Methodology: Grounded theory. Outcome measures: Focus groups. Analysis: Grounded theory analysis. |
| Harrison & Ruddock-Hudson [6] | Participants: 20 professional dancers (9 males, 11 female). Age: Average 35 years. Sampling: Convenience. Setting: Not identified. Aim: To explore the perceptions and experiences of injury, pain and retirement among professional dancers. Geographical location: Australia. | Methodology: Not identified (likely a type of phenomenology). Outcome measures: Semi-structured interview. Analysis: Content analysis. |
| Markula [16] | Participants: 14 contemporary dancers (no gender breakdown). Age: Range 18–30 years (no mean given). Sampling: Convenience. Setting: Not identified. Aim: To understand how contemporary dancers experience injuries. Geographical location: Canada. | Methodology: Deleuzian theoretical concepts used. Outcome measures: Formal face-to-face interviews. Analysis: Textual analysis. |
| Pollard-Smith & Thomson [23] | Participants: 8 ballet dancers (3 male, 5 female). Sampling: Snowball initially, followed by purposive and theoretical. Setting: No details. Aim: To explore the decision-making process of dancers who are seeking treatment for injuries. Geographical location: England. | Methodology: Grounded theory. Outcome measures: In-depth interviews. Analysis: Grounded theory analysis. |
| McEwen & Young [1] | Participants: 15 professional ballet dancers (13 female, 2 male). Age: Mean was 21 years. Sampling: Snowball. Setting: Selected by dancers’ public locations or homes of dancers. Aim: To explore how elements of risk-taking behaviours affect physical and emotional health of dancers. Geographical location: Canada. | Methodology: Unclear, likely a type of phenomenology. Outcome measures: Semi-structured interviews. Analysis: Thematic analysis. |
| Tarr & Thomas [35] | Participants: 205 (30 male, 175 female) 167 dancers (85 professional, 82 pre-professional (students). Gender breakdown of dancers not given. Age: 51% aged between 20–29 years. Sampling: Convenience and snowball. Setting: University. Aim: To consider the cultural and embodied experience of dancers in relation to pain. Geographical location: United Kingdom | Methodology: Cultural phenomenology. Outcome measures: Questionnaire. Semi-structured interviews. Analysis: Thematic analysis. |
| Tarr & Thomas [36] | Participants: 205 (30 male, 175 female). 85 professional, 82 pre-professional (students). Age: 51% aged between 20–29 years. Sampling: Convenience and snowball. Setting: University. Aim: 3 main aims: (1) identify how dancers distinguish between pain and injury and what this means for a cultural understanding of pain, (2) consideration of how visual representation of pain helps the understanding of injury and (3) how does movement style affect pain and injury. Geographical location: United Kingdom | Methodology: Cultural phenomenology. Outcome measures: Semi-structured interviews. Analysis: Thematic analysis. |
| Wainwright and Turner [14] | Participants: 22 professional dancers. Age: Not detailed. Sampling: Convenience. Setting: Royal Opera House and University. Aim: To understand interactions between injuries, dancers’ experiences of discomfort and social support. Geographical location: United Kingdom. | Methodology: Grounded theory. Outcome measures: Semi-structured interviews. Analysis: Grounded theory. |
| Wainwright et al. [38] | Participants: 22 professional dancers. Age: Not detailed. Sampling: Convenience. Setting: Royal Opera House and a University. Aim: Understanding the impact injuries can have on individual identities. Geographical location: United Kingdom. | Methodology: Unclear, likely grounded theory. Outcome measures: Semi-structured interviews. Analysis: Grounded theory. |
| Wainwright & Turner [37] | Participants: 22 professional dancers. Age: Not detailed. Sampling: Convenience. Setting: Royal Opera House and a University. Aim: Illuminate the embodiment of classical ballet. Geographical location: United Kingdom. | Methodology: Ethnographic. Outcome measures: Semi-structure interviews. Observations. Analysis: Thematic analysis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soundy, A.; Lim, J.Y. Pain Perceptions, Suffering and Pain Behaviours of Professional and Pre-Professional Dancers towards Pain and Injury: A Qualitative Review. Behav. Sci. 2023, 13, 268. https://doi.org/10.3390/bs13030268
Soundy A, Lim JY. Pain Perceptions, Suffering and Pain Behaviours of Professional and Pre-Professional Dancers towards Pain and Injury: A Qualitative Review. Behavioral Sciences. 2023; 13(3):268. https://doi.org/10.3390/bs13030268
Chicago/Turabian StyleSoundy, Andrew, and Ja Yee Lim. 2023. "Pain Perceptions, Suffering and Pain Behaviours of Professional and Pre-Professional Dancers towards Pain and Injury: A Qualitative Review" Behavioral Sciences 13, no. 3: 268. https://doi.org/10.3390/bs13030268
APA StyleSoundy, A., & Lim, J. Y. (2023). Pain Perceptions, Suffering and Pain Behaviours of Professional and Pre-Professional Dancers towards Pain and Injury: A Qualitative Review. Behavioral Sciences, 13(3), 268. https://doi.org/10.3390/bs13030268