
Relationship between Racial Diversity in Medical Staff and Hospital Operational Efficiency: An Empirical Study of 3870 U.S. Hospitals

 , ,
, ,
Abstract
:1. Introduction
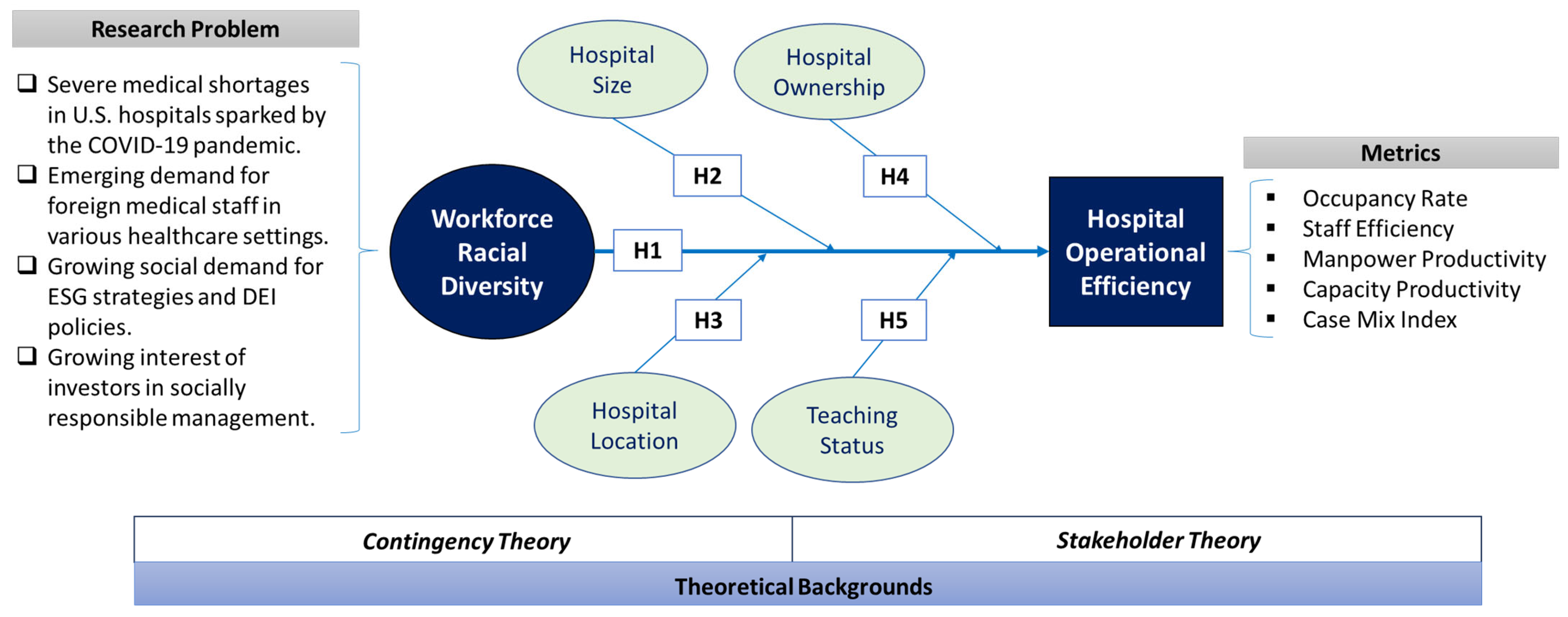
1.1. COVID-19 Pandemic and Workforce Racial Diversity
1.2. Research Outline
2. Theoretical Backgrounds and Hypotheses
2.1. Literature Review
2.2. Workforce Racial Diversity and Hospital Operational Efficiency
2.3. Workforce Racial Diversity, Hospital Efficiency, and Hospital Size
2.4. Workforce Racial Diversity, Hospital Efficiency, and Hospital Location
2.5. Workforce Racial Diversity, Hospital Efficiency, and Hospital Ownership
2.6. Workforce Racial Diversity, Hospital Efficiency, and Teaching Status
3. Methodology
3.1. Data Collection and Sampling
3.2. Staff Efficiency (STAFF_E)
3.3. Capacity Productivity (CP)
3.4. Manpower Productivity (MP)
3.5. Occupancy Rate (OCCP)
3.6. Case Mix Index (CMI)
4. Data Analysis
4.1. Results on Hospital Efficiency by Diversity
4.2. Results on the Control Effect of Hospital Size
4.3. Results on the Control Effect of Hospital Location
4.4. Results on the Control Effect of Hospital Ownership
4.5. Results on the Control Effect of Hospital Teaching Status
5. Discussion
5.1. Implications for Theory
5.2. Implications for Practice
5.3. Limitations and Future Research Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dolan, K.; Hunt, V.; Prince, S.; Sancier-Sultan, S. Diversity still matters. McKinsey Q. 2020, 19. [Google Scholar]
- Ellingrud, K.; Krishnan, M.; Krivkovich, A.; Kukla, K.; Mendy, A.; Robinson, N.; Sancier-Sultan, S.; Yee, L. Diverse Employees Are Struggling the Most during COVID-19—Here’s How Companies Can Respond; McKinsey Global Institute: Washington, DC, USA, 2020. [Google Scholar]
- Hansen, F. Diversity’s Business Case: Doesn’t Add Up. Workforce 2013, 82, 28–29. [Google Scholar]
- Gaumer, G.; Coulam, R. Geographic variation in minority participation in hospital management in the United States. Hosp. Top. 2009, 87, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Gomez, L.E.; Bernet, P. Diversity improves performance and outcomes. J. Natl. Med. Assoc. 2019, 111, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Ancarani, A.; Ayach, A.; Di Mauro, C.; Gitto, S.; Mancuso, P. Does religious diversity in health team composition affect efficiency? Evidence from Dubai. Br. J. Manag. 2016, 27, 740–759. [Google Scholar] [CrossRef]
- Newhouse, J.J. Hospital strategic planning diversity integration based on organizational type and CEO tenure. Hosp. Top. 2007, 85, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Tiemann, O.; Schreyögg, J. Changes in hospital efficiency after privatization. Health Care Manag. Sci. 2012, 15, 310–326. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.; Chang, G.H. An investigation of economic efficiency in California hospitals. J. Gov. Nonprofit Account. 2017, 6, 30–51. [Google Scholar] [CrossRef] [Green Version]
- Bradley, E.H. Diversity, inclusive leadership, and health outcomes. Int. J. Health Policy Manag. 2020, 9, 266. [Google Scholar] [CrossRef] [Green Version]
- Ehli, N. Hospitals Recruit International Nurses to Fill Pandemic Shortages. Kaiser Health News, 7 January 2022. [Google Scholar]
- Homroy, S.; Soo, K.T. Team diversity and individual performance. Manch. Sch. 2020, 88, 507–530. [Google Scholar] [CrossRef]
- Blouch, R.; Malik, F.A. Effects of perceived diversity on perceived organizational performance: Mediating role of perceived organizational justice. Empl. Relat. 2019, 41, 1079–1097. [Google Scholar] [CrossRef]
- Singal, M. The business case for diversity management in the hospitality industry. Int. J. Hosp. Manag. 2014, 40, 10–19. [Google Scholar] [CrossRef]
- Ye, J.; Zhang, H.; Cao, C.; Wei, F.; Namunyak, M. Boardroom gender diversity on stock liquidity: Empirical evidence from chinese c-share market. Emerg. Mark. Financ. Trade 2021, 57, 3236–3253. [Google Scholar] [CrossRef]
- Tamimi, N.; Sebastianelli, R. Transparency among S&P 500 companies: An analysis of ESG disclosure scores. Manag. Decis. 2017, 55, 1660–1680. [Google Scholar] [CrossRef]
- Schueth, S. Socially responsible investing in the United States. J. Bus. Ethics 2003, 43, 189–194. [Google Scholar] [CrossRef]
- Velte, P. Does ESG performance have an impact on financial performance? Evidence from Germany. J. Glob. Responsib. 2017, 8, 169–178. [Google Scholar] [CrossRef]
- Fiedler, F.E. A contingency model of leadership effectiveness. In Advances in Experimental Social Psychology; Academic Press: Cambridge, MA, USA, 1964; Volume 1, pp. 149–190. [Google Scholar]
- Freeman, R.E. Strategic Management: A Stakeholder Approach; Pitman: Boston, MA, USA, 1984. [Google Scholar]
- Donaldson, L. The Contingency Theory of Organizations; Sage: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Freeman, R.E.; McVea, J. A Stakeholder Approach to Strategic Management. In The Blackwell Handbook of Strategic Management; Wiley: Hoboken, NJ, USA, 2005; Available online: https://ssrn.com/abstract=263511 (accessed on 3 June 2023). [CrossRef]
- Manita, R.; Bruna, M.G.; Dang, R.; Houanti, L.H. Board gender diversity and ESG disclosure: Evidence from the USA. J. Appl. Account. Res. 2018, 19, 206–224. [Google Scholar] [CrossRef]
- Nirino, N.; Santoro, G.; Miglietta, N.; Quaglia, R. Corporate controversies and company’s financial performance: Exploring the moderating role of ESG practices. Technol. Forecast. Soc. Chang. 2021, 162, 120341. [Google Scholar] [CrossRef]
- White, K.R.; Ozcan, Y.A. Church ownership and hospital efficiency. Hosp. Health Serv. Adm. 1996, 41, 297–310. [Google Scholar]
- Coyne, J.S.; Richards, M.T.; Short, R.; Shultz, K.; Singh, S.G. Hospital cost and efficiency: Do hospital size and ownership type really matter? J. Healthc. Manag. 2009, 54, 163–175. [Google Scholar] [CrossRef]
- Smith, D.B. The racial segregation of hospital care revisited: Medicare discharge patterns and their implications. Am. J. Public Health 1998, 88, 461–463. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, A.K.; Unruh, M.A.; Ibrahim, S.; Shapiro, M.F. Association between patient diversity in hospitals and racial/ethnic differences in patient length of stay. J. Gen. Intern. Med. 2022, 37, 723–729. [Google Scholar] [CrossRef]
- Garcia-Lacalle, J.; Martin, E. Rural vs urban hospital performance in a ‘competitive’ public health service. Soc. Sci. Med. 2010, 71, 1131–1140. [Google Scholar] [CrossRef]
- Sun, Q.; Zhao, M.; Haley, D.R.; Wei, X. Hospital performance in China: Do location and hospital level matter? Nurs. Econ. 2014, 32, 148–156. [Google Scholar] [PubMed]
- Jehu-Appiah, C.; Sekidde, S.; Adjuik, M.; Akazili, J.; Almeida, S.D.; Nyonator, F.; Baltussen, R.; Asbu, E.Z.; Kirigia, J.M. Ownership and technical efficiency of hospitals: Evidence from Ghana using data envelopment analysis. Cost Eff. Resour. Alloc. 2014, 12, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stock, G.N.; McDermott, C. Operational and contextual drivers of hospital costs. J. Health Organ. Manag. 2011, 25, 142–158. [Google Scholar] [CrossRef] [PubMed]
- Tiemann, O.; Schreyögg, J. Effects of ownership on hospital efficiency in Germany. Bus. Res. 2009, 2, 115–145. [Google Scholar] [CrossRef] [Green Version]
- Messina, D.J.; Scotti, D.J.; Caney, R.; Zipp, G.P. The relationship between patient satisfaction and inpatient admissions across teaching and nonteaching hospitals. J. Healthc. Manag. 2009, 54, 177–190. [Google Scholar] [CrossRef]
- Shahian, D.M.; Nordberg, P.; Meyer, G.S.; Blanchfield, B.B.; Mort, E.A.; Torchiana, D.F.; Normand, S.L. Contemporary performance of U.S. teaching and nonteaching hospitals. Acad. Med. 2012, 87, 701–708. [Google Scholar] [CrossRef]
- Wallace, P.E.; Ermer, C.M., Jr.; Motshabi, D.N. Managing diversity: A senior management perspective. Hosp. Health Serv. Adm. 1996, 41, 91–104. [Google Scholar]
- Watkins, A. Hospital financial ratio classification patterns revisited: Upon considering non-financial information. J. Account. Public Policy 2000, 19, 73–95. [Google Scholar] [CrossRef]
- Elsass, P.M.; Graves, L.M. Demographic diversity in decision-making groups: The experiences of women and people of color. Acad. Manag. Rev. 1997, 22, 946–973. [Google Scholar] [CrossRef]
- Phillips, K.W.; Medin, D.; Lee, C.D.; Bang, M.; Bishop, S.; Lee, D.N. How diversity works. Sci. Am. 2014, 311, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Rao, K.; Tilt, C. Board composition and corporate social responsibility: The role of diversity, gender, strategy and decision making. J. Bus. Ethics 2016, 138, 327–347. [Google Scholar] [CrossRef]
- Yuan, H.; Ma, D. Gender differences in the relationship between interpersonal trust and innovative behavior: The mediating effects of affective organizational commitment and knowledge-sharing. Behav. Sci. 2022, 12, 145. [Google Scholar] [CrossRef]
- Tran, K.T.; Nguyen, P.V.; Dang, T.T.; Ton, T.N. The impacts of the high-quality workplace relationships on job performance: A perspective on staff nurses in Vietnam. Behav. Sci. 2018, 8, 109. [Google Scholar] [CrossRef] [Green Version]
- Lušňáková, Z.; Benda-Prokeinová, R.; Juríčková, Z. Attitudes and Involvement of Employees in the Process of Implementing Innovations and Changes in Companies. Behav. Sci. 2022, 12, 174. [Google Scholar] [CrossRef]
- Rangachari, P.; Woods, J.L. Preserving organizational resilience, patient safety, and staff retention during COVID-19 requires a holistic consideration of the psychological safety of healthcare workers. Int. J. Environ. Res. Public Health 2020, 17, 4267. [Google Scholar] [CrossRef]
- Brambilla, A.; Sun, T.-Z.; Elshazly, W.; Ghazy, A.; Barach, P.; Lindahl, G.; Capolongo, S. Flexibility during the COVID-19 Pandemic Response: Healthcare Facility Assessment Tools for Resilient Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 11478. [Google Scholar] [CrossRef]
- Gašić, D.; Berber, N. The Mediating Role of Employee Engagement in the Relationship between Flexible Work Arrangements and Turnover Intentions among Highly Educated Employees in the Republic of Serbia. Behav. Sci. 2023, 13, 131. [Google Scholar] [CrossRef]
- Miller, T.; del Carmen Triana, M. Demographic diversity in the boardroom: Mediators of the board diversity–firm performance relationship. J. Manag. Stud. 2009, 46, 755–786. [Google Scholar] [CrossRef]
- Wu, Z.; Tian, H.; Xu, D.; Chen, J.; Hu, Y.; Wang, X.; Zhou, S. Influencing Factors and Symbiotic Mechanism of the Integration of Medical Care and Disease Prevention during the COVID-19 Pandemic: A Cross-Sectional Survey of Public Hospital Employees. Int. J. Environ. Res. Public Health 2023, 20, 241. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.R., Jr. From affirmative action to affirming diversity. Harv. Bus. Rev. 1990, 68, 107–117. [Google Scholar]
- Furtado, J.V.; Moreira, A.C.; Mota, J. Gender affirmative action and management: A systematic literature review on how diversity and inclusion management affect gender equity in organizations. Behav. Sci. 2021, 11, 21. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Filtering Criteria | Before Filtering | Outliers | After Filtering | ||||
|---|---|---|---|---|---|---|---|---|
| N1 | SK | KT | N2 | SK | KT | |||
| STAFF_E | STAFF_E < 13.2 | 2466 | 2.112 | 9.123 | 168 | 2298 | 0.504 | −0.293 |
| OCCP | OCCP < 1.11 | 2466 | 0.086 | 0.554 | 8 | 2458 | −0.143 | −0.512 |
| MP | MP ≤ 26.3 | 2135 | 0.987 | 2.727 | 33 | 2102 | 0.348 | −0.418 |
| CP | CP ≤ 158 | 2135 | 0.716 | 2.764 | 35 | 2100 | −0.092 | −0.320 |
| CMI | 0.87 ≤ CMI ≤ 2.33 | 2135 | 0.860 | 1.892 | 82 | 2053 | 0.212 | −0.200 |
| Variable | Mean | Median | SD | Min | Max | Skewness | Kurtosis | DF | K-S Statistic |
|---|---|---|---|---|---|---|---|---|---|
| STAFF_E | 6.494 | 6.185 | 2.519 | 1.22 | 13.16 | 0.504 | −0.293 | 2298 | 0.053 *** |
| OCCP | 0.558 | 0.572 | 0.187 | 0.059 | 1.075 | −0.143 | −0.512 | 2458 | 0.038 *** |
| MP | 12.414 | 12.053 | 4.994 | 0.588 | 26.294 | 0.348 | −0.418 | 2104 | 0.043 *** |
| CP | 76.065 | 77.803 | 28.015 | 4.488 | 153.107 | −0.092 | −0.320 | 2100 | 0.032 *** |
| CMI | 1.627 | 1.615 | 0.269 | 0.917 | 2.329 | 0.212 | −0.200 | 2053 | 0.022 * |
| Efficiency | Diversity | N | Mean | SD | MR | MWU | Z | One-Tailed p |
|---|---|---|---|---|---|---|---|---|
| STAFF_E | Less | 1813 | 6.497 | 2.532 | 1148.54 | 437,910.5 | −0.134 | 0.447 |
| More | 485 | 6.481 | 2.472 | 1153.09 | ||||
| OCCP | Less | 1947 | 0.541 | 0.187 | 1166.12 | 374,053.0 | −8.643 | <0.001 |
| More | 511 | 0.621 | 0.176 | 1471.00 | ||||
| MP | Less | 1625 | 12.154 | 4.997 | 1020.43 | 337,066.0 | −4.461 | <0.001 |
| More | 479 | 13.297 | 4.884 | 1161.31 | ||||
| CP | Less | 1618 | 74.351 | 28.243 | 1015.00 | 332,495.0 | −4.916 | <0.001 |
| More | 482 | 81.819 | 26.464 | 1169.68 | ||||
| CMI | Less | 1585 | 1.609 | 0.272 | 984.03 | 302,787.5 | −6.044 | <0.001 |
| More | 468 | 1.685 | 0.249 | 1172.52 |
| Frequency | Percent | Valid Percent | Cumulative % | |
|---|---|---|---|---|
| Small (6–99 beds) | 900 | 36.5 | 36.5 | 36.5 |
| Medium (100–399 beds) | 1171 | 47.5 | 47.5 | 84.00 |
| Large (≥400 beds) | 395 | 16.0 | 16.0 | 100.00 |
| Total | 2466 | 100.0 | 100.0 |
| Efficiency | Bed Size | Diversity | N | Mean | SD | MR | MWU | Z | p |
|---|---|---|---|---|---|---|---|---|---|
| STAFF_E | Small | Less | 685 | 7.248 | 2.735 | 390.10 | 32,124.0 | −0.035 | 0.486 |
| More | 94 | 7.219 | 2.720 | 389.24 | |||||
| Medium | Less | 890 | 5.839 | 2.207 | 570.35 | 111,118.0 | −0.787 | 0.431 | |
| More | 258 | 5.964 | 2.263 | 588.81 | |||||
| Large | Less | 238 | 6.799 | 2.413 | 182.90 | 15,089.0 | −0.745 | 0.228 | |
| More | 133 | 6.965 | 2.468 | 191.55 | |||||
| OCCP | Small | Less | 791 | 0.423 | 0.174 | 440.14 | 34,911.5 | −2.655 | 0.004 |
| More | 105 | 0.479 | 0.205 | 511.51 | |||||
| Medium | Less | 906 | 0.600 | 0.149 | 575.37 | 110,410.0 | −1.811 | 0.035 | |
| More | 263 | 0.619 | 0.143 | 618.19 | |||||
| Large | Less | 250 | 0.704 | 0.111 | 187.51 | 15,503.0 | −2.189 | 0.015 | |
| More | 143 | 0.730 | 0.124 | 213.59 | |||||
| MP | Small | Less | 501 | 9.565 | 4.651 | 285.93 | 17,499.0 | −1.312 | 0.095 |
| More | 77 | 10.119 | 4.223 | 312.74 | |||||
| Medium | Less | 875 | 13.171 | 4.747 | 553.39 | 100,964.0 | −2.843 | 0.002 | |
| More | 261 | 14.078 | 4.870 | 619.16 | |||||
| Large | Less | 249 | 13.796 | 4.544 | 197.74 | 16,996.0 | −0.522 | 0.301 | |
| More | 141 | 13.587 | 4.575 | 191.54 | |||||
| CP | Small | Less | 491 | 64.294 | 30.054 | 281.54 | 17,449.0 | −0.910 | 0.182 |
| More | 76 | 66.852 | 27.619 | 299.91 | |||||
| Medium | Less | 877 | 75.299 | 26.619 | 559.33 | 105,531.0 | −2.091 | 0.018 | |
| More | 263 | 79.988 | 25.886 | 607.74 | |||||
| Large | Less | 250 | 90.777 | 20.882 | 193.60 | 17,026.0 | −0.784 | 0.217 | |
| More | 143 | 93.142 | 21.859 | 202.94 | |||||
| CMI | Small | Less | 481 | 1.454 | 0.281 | 279.38 | 17,613.5 | −0.328 | 0.372 |
| More | 75 | 1.426 | 0.226 | 272.85 | |||||
| Medium | Less | 871 | 1.621 | 0.212 | 550.44 | 99,675.5 | −3.193 | <0.001 | |
| More | 263 | 1.661 | 0.196 | 624.01 | |||||
| Large | Less | 233 | 1.887 | 0.210 | 182.15 | 15,109.0 | −0.038 | 0.485 | |
| More | 130 | 1.885 | 0.192 | 181.72 |
| Frequency | Percent | Valid Percent | Cumulative % | |
|---|---|---|---|---|
| Rural | 265 | 10.7 | 10.7 | 10.7 |
| Microcity | 466 | 18.9 | 18.9 | 29.6 |
| Metropolitan | 1735 | 70.4 | 70.4 | 100.00 |
| Total | 2466 | 100.0 | 100.0 |
| Efficiency | Location | Diversity | N | Mean | SD | MR | MWU | Z | p |
|---|---|---|---|---|---|---|---|---|---|
| STAFF_E | Rural | Less | 205 | 6.606 | 3.0687 | 112.59 | 1966.0 | −0.654 | 0.257 |
| More | 21 | 7.066 | 2.861 | 122.38 | |||||
| Microcity | Less | 347 | 6.728 | 2.805 | 209.94 | 11,473.5 | −0.546 | 0.293 | |
| More | 69 | 6.482 | 2.911 | 201.28 | |||||
| Metropolitan | Less | 1261 | 6.416 | 2.347 | 826.22 | 246,174.5 | −0.346 | 0.365 | |
| More | 395 | 6.450 | 2.369 | 835.77 | |||||
| OCCP | Rural | Less | 238 | 0.447 | 0.199 | 130.62 | 2647.0 | −0.591 | 0.278 |
| More | 24 | 0.459 | 0.203 | 140.21 | |||||
| Microcity | Less | 389 | 0.455 | 0.166 | 229.15 | 13,283.0 | −1.399 | 0.081 | |
| More | 76 | 0.493 | 0.193 | 252.72 | |||||
| Metropolitan | Less | 1320 | 0.584 | 0.176 | 818.29 | 208,286.0 | −7.117 | <0.001 | |
| More | 411 | 0.655 | 0.153 | 1019.22 | |||||
| MP | Rural | Less | 92 | 7.311 | 3.096 | 50.14 | 335.0 | −1.407 | 0.080 |
| More | 10 | 9.364 | 4.428 | 64.00 | |||||
| Microcity | Less | 304 | 8.839 | 3.610 | 184.08 | 9601.0 | −0.547 | 0.292 | |
| More | 66 | 9.145 | 3.758 | 192.03 | |||||
| Metropolitan | Less | 1229 | 13.338 | 4.819 | 799.18 | 226,363 | −2.592 | 0.005 | |
| More | 403 | 14.075 | 4.671 | 869.31 | |||||
| CP | Rural | Less | 92 | 40.990 | 24.776 | 50.79 | 395.0 | −0.226 | 0.411 |
| More | 9 | 42.590 | 25.304 | 53.11 | |||||
| Microcity | Less | 304 | 55.666 | 22.941 | 184.72 | 9796.0 | −0.300 | 0.382 | |
| More | 66 | 56.870 | 24.648 | 189.08 | |||||
| Metropolitan | Less | 1222 | 81.510 | 25.649 | 793.92 | 222,921.0 | −3.134 | 0.001 | |
| More | 407 | 86.732 | 23.671 | 878.28 | |||||
| CMI | Rural | Less | 91 | 1.2652 | 0.1592 | 49.69 | 336.0 | −1.353 | 0.176 |
| More | 10 | 1.366 | 0.260 | 62.90 | |||||
| Microcity | Less | 304 | 1.447 | 0.200 | 186.31 | 9786.0 | −0.312 | 0.378 | |
| More | 66 | 1.444 | 0.209 | 181.77 | |||||
| Metropolitan | Less | 1190 | 1.676 | 0.257 | 761.27 | 197,271.0 | −4.585 | <0.001 | |
| More | 392 | 1.734 | 0.224 | 883.26 |
| Frequency | Percent | Valid Percent | Cumulative % | |
|---|---|---|---|---|
| Government (Govt) | 359 | 14.6 | 14.6 | 14.6 |
| Non-government, not-for-profit (NG-NFP) | 1765 | 71.6 | 71.6 | 86.1 |
| Investor Owned, for-profit (For-Profit) | 342 | 13.9 | 13.9 | 100.00 |
| Total | 2466 | 100.0 | 100.0 |
| Efficiency | OLE | Diversity | N | Mean | SD | MR | MWU | Z | p |
|---|---|---|---|---|---|---|---|---|---|
| STAFF_E | Govt | Less | 266 | 7.086 | 2.744 | 161.85 | 7541.5 | −0.267 | 0.395 |
| More | 58 | 7.154 | 2.233 | 165.47 | |||||
| NG-NFP | Less | 1305 | 6.631 | 2.449 | 810.01 | 204,898.5 | −2.173 | 0.015 | |
| More | 340 | 6.904 | 2.376 | 872.86 | |||||
| For-Profit | Less | 242 | 5.132 | 2.262 | 174.72 | 8174.5 | −3.092 | 0.001 | |
| More | 87 | 4.384 | 1.844 | 137.96 | |||||
| OCCP | Govt | Less | 298 | 0.519 | 0.211 | 173.56 | 7170.0 | −2.599 | 0.005 |
| More | 61 | 0.596 | 0.197 | 211.46 | |||||
| NG-NFP | Less | 1395 | 0.563 | 0.178 | 828.38 | 181,874.5 | −8.211 | <0.001 | |
| More | 362 | 0.648 | 0.164 | 1074.08 | |||||
| For-Profit | Less | 254 | 0.451 | 0.178 | 160.19 | 8302.0 | −3.596 | <0.001 | |
| More | 88 | 0.528 | 0.174 | 204.16 | |||||
| MP | Govt | Less | 209 | 8.955 | 3.700 | 127.90 | 4787.0 | −2.091 | 0.019 |
| More | 56 | 10.358 | 4.012 | 152.02 | |||||
| NG-NFP | Less | 1185 | 12.293 | 4.760 | 748.55 | 184,331.0 | −2.470 | 0.007 | |
| More | 341 | 12.973 | 4.635 | 815.44 | |||||
| For-Profit | Less | 231 | 14.341 | 5.755 | 147.57 | 7292.0 | −3.095 | 0.001 | |
| More | 82 | 16.654 | 4.673 | 183.57 | |||||
| CP | Govt | Less | 210 | 63.479 | 29.087 | 129.46 | 5031.0 | −1.660 | 0.049 |
| More | 56 | 71.592 | 27.405 | 148.66 | |||||
| NG-NFP | Less | 1183 | 77.085 | 26.812 | 729.72 | 162,928.0 | −5.269 | <0.001 | |
| More | 339 | 86.049 | 25.921 | 872.39 | |||||
| For-Profit | Less | 225 | 70.122 | 31.732 | 153.58 | 9131.0 | −0.919 | 0.179 | |
| More | 87 | 71.921 | 23.626 | 164.05 | |||||
| CMI | Govt | Less | 200 | 1.521 | 0.277 | 121.14 | 4128.0 | −2.474 | 0.007 |
| More | 53 | 1.637 | 0.286 | 149.11 | |||||
| NG-NFP | Less | 1173 | 1.619 | 0.259 | 717.25 | 152,783.5 | −5.852 | <0.001 | |
| More | 330 | 1.705 | 0.243 | 875.52 | |||||
| For-Profit | Less | 212 | 1.638 | 0.317 | 146.60 | 8500.5 | −0.762 | 0.223 | |
| More | 85 | 1.639 | 0.241 | 154.99 |
| Frequency | Percent | Valid Percent | Cumulative % | |
|---|---|---|---|---|
| Teaching | 212 | 8.6 | 8.6 | 8.6 |
| Non-teaching | 2254 | 91.4 | 91.4 | 100.0 |
| Total | 2466 | 100.0 | 100.0 |
| Efficiency | Teaching | Diversity | N | Mean | SD | MR | MWU | Z | p |
|---|---|---|---|---|---|---|---|---|---|
| STAFF_E | Teaching | Less | 123 | 8.1201 | 2.275 | 94.08 | 3946.0 | −0.482 | 0.315 |
| More | 67 | 8.215 | 2.172 | 98.10 | |||||
| NT | Less | 1690 | 6.379 | 2.510 | 1061.55 | 341,292.5 | −1.1070 | 0.143 | |
| More | 418 | 6.204 | 2.407 | 1025.99 | |||||
| OCCP | Teaching | Less | 136 | 0.747 | 0.109 | 102.24 | 4588 | −1.354 | 0.088 |
| More | 76 | 0.768 | 0.116 | 114.13 | |||||
| NT | Less | 1811 | 0.526 | 0.183 | 1074.77 | 305,635 | −7.267 | <0.001 | |
| More | 435 | 0.596 | 0.172 | 1326.39 | |||||
| MP | Teaching | Less | 136 | 12.262 | 3.974 | 108.68 | 4736.0 | −0.857 | 0.196 |
| More | 75 | 11.879 | 3.541 | 101.15 | |||||
| NT | Less | 1489 | 12.145 | 5.082 | 914.16 | 251,879.0 | −5.018 | <0.001 | |
| More | 404 | 13.560 | 5.055 | 1068.04 | |||||
| CP | Teaching | Less | 133 | 97.869 | 18.299 | 101.17 | 4544.0 | −1.064 | 0.144 |
| More | 75 | 100.183 | 18.494 | 110.41 | |||||
| NT | Less | 1485 | 72.244 | 28.024 | 921.91 | 265,677.0 | −3.740 | <0.001 | |
| More | 407 | 78.435 | 26.336 | 1036.23 | |||||
| CMI | Teaching | Less | 115 | 1.945 | 0.2487 | 88.75 | 3536.5 | −0.088 | 0.465 |
| More | 62 | 1.957 | 0.212 | 89.46 | |||||
| NT | Less | 1470 | 1.583 | 0.256 | 905.00 | 249,159.5 | −5.097 | <0.001 | |
| More | 406 | 1.644 | 0.227 | 1059.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.C.; Cho, Y.S.; Breen, D.; Monroy, J.; Seo, D.; Min, Y.-T. Relationship between Racial Diversity in Medical Staff and Hospital Operational Efficiency: An Empirical Study of 3870 U.S. Hospitals. Behav. Sci. 2023, 13, 564. https://doi.org/10.3390/bs13070564
Lee CC, Cho YS, Breen D, Monroy J, Seo D, Min Y-T. Relationship between Racial Diversity in Medical Staff and Hospital Operational Efficiency: An Empirical Study of 3870 U.S. Hospitals. Behavioral Sciences. 2023; 13(7):564. https://doi.org/10.3390/bs13070564
Chicago/Turabian StyleLee, C. Christopher, Young Sik Cho, Diosmedy Breen, Jessica Monroy, Donghwi Seo, and Yong-Taek Min. 2023. "Relationship between Racial Diversity in Medical Staff and Hospital Operational Efficiency: An Empirical Study of 3870 U.S. Hospitals" Behavioral Sciences 13, no. 7: 564. https://doi.org/10.3390/bs13070564
APA StyleLee, C. C., Cho, Y. S., Breen, D., Monroy, J., Seo, D., & Min, Y.-T. (2023). Relationship between Racial Diversity in Medical Staff and Hospital Operational Efficiency: An Empirical Study of 3870 U.S. Hospitals. Behavioral Sciences, 13(7), 564. https://doi.org/10.3390/bs13070564