The Roles of Personal and Environmental Resources in Predicting Work–Family Facilitation and Mental Health among Employed Parents of Children with Disabilities in Croatia




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Analytical Strategies
3. Results and Discussion
3.1. Preliminary Analyses
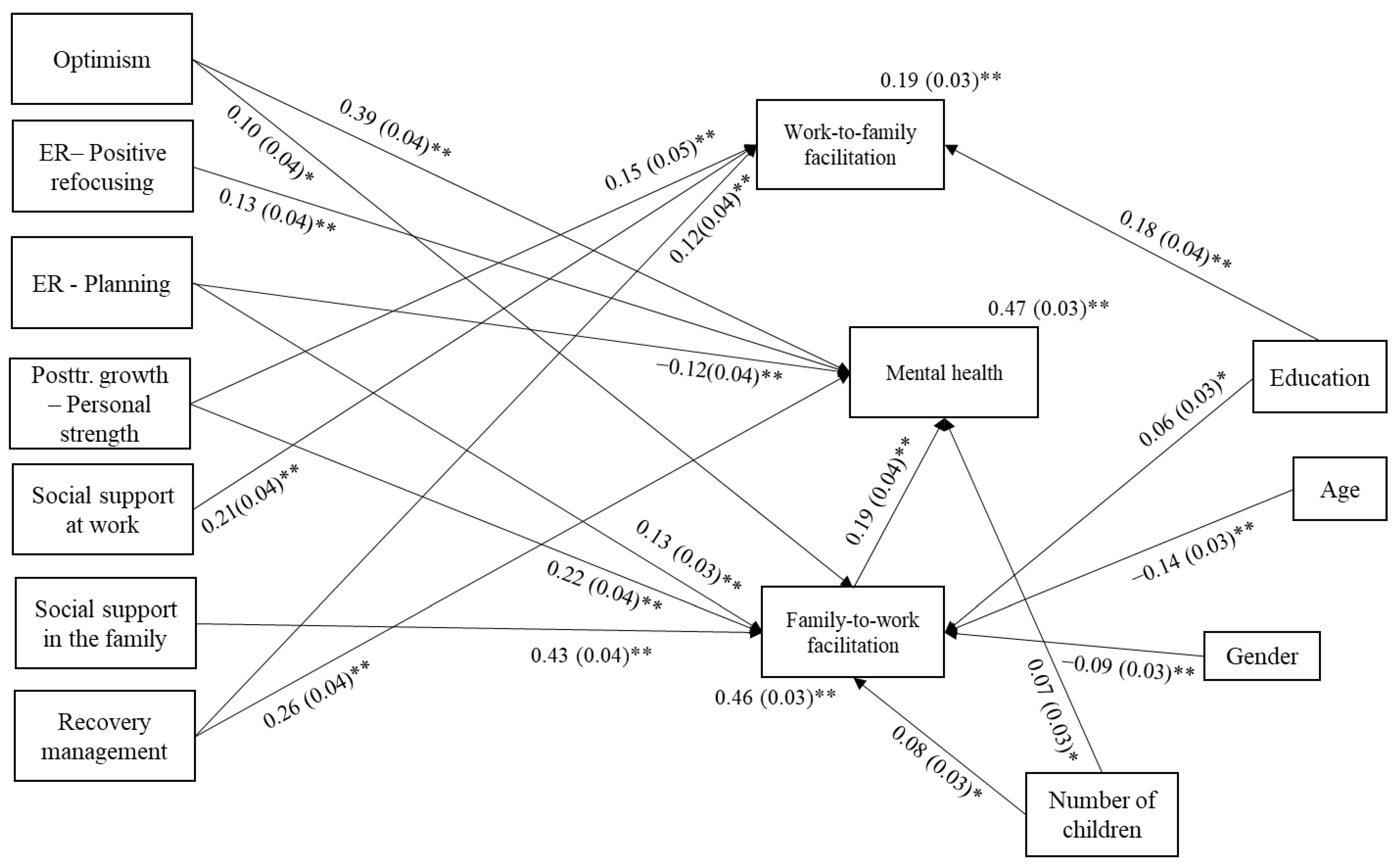
3.2. Testing the Hypothesized Model
Interpreting the Model Results
4. Discussion
4.1. Predicting Work-to-Family Facilitation and Family-to-Work Facilitation in Parents of Children with Disabilities in Croatia
4.2. Predicting Mental Health in Parents of Children with Disabilities in Croatia and the Mediational Roles of Work-to-Family Facilitation and Family-to-Work Facilitation
4.3. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mental Health. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed on 6 July 2023).
- Ionio, C.; Colombo, C.; Brazzoduro, V.; Mascheroni, E.; Confalonieri, E.; Castoldi, F.; Lista, G. Mothers and Fathers in NICU: The Impact of Preterm Birth on Parental Distress. Eur. J. Psychol. 2016, 12, 604–621. [Google Scholar] [CrossRef]
- Starc, B. Parenting in the Best Interests of the Child and Support to Parents|UNICEF. Available online: https://www.unicef.org/croatia/en/reports/parenting-best-interests-child-and-support-parents (accessed on 6 July 2023).
- Gérain, P.; Zech, E. Does Informal Caregiving Lead to Parental Burnout? Comparing Parents Having (or Not) Children with Mental and Physical Issues. Front. Psychol. 2018, 9, 884. [Google Scholar] [CrossRef]
- Stewart, L.M.; Sellmaier, C.; Brannan, A.M.; Brennan, E.M. Employed Parents of Children with Typical and Exceptional Care Responsibilities: Family Demands and Workplace Supports. J. Child Fam. Stud. 2023, 32, 1048–1064. [Google Scholar] [CrossRef]
- Brown, T.J.; Clark, C. Employed Parents of Children with Disabilities and Work Family Life Balance: A Literature Review. Child Youth Care Forum 2017, 46, 857–876. [Google Scholar] [CrossRef]
- Morris, L.A. The Impact of Work on the Mental Health of Parents of Children with Disabilities. Fam. Relat. 2014, 63, 101–121. [Google Scholar] [CrossRef]
- Bulger, C.A.; Hoffman, M.E. Segmentation/Integration of Work and Nonwork Domains: Global Considerations. In The Cambridge Handbook of the Global Work–Family Interface; Cambridge University Press: New York, NY, USA, 2018; pp. 701–719. ISBN 978-1-108-40126-5. [Google Scholar]
- Lewis, S.; Beauregard, T.A. The Meanings of Work–Life Balance: A Cultural Perspective. In The Cambridge Handbook of the Global Work–Family Interface; Shockley, K.M., Johnson, R.C., Shen, W., Eds.; Cambridge Handbooks in Psychology; Cambridge University Press: Cambridge, UK, 2018; pp. 720–732. ISBN 978-1-108-41597-2. [Google Scholar]
- Williams, J.C.; Berdahl, J.L.; Vandello, J.A. Beyond Work-Life “Integration. ” Annu. Rev. Psychol. 2016, 67, 515–539. [Google Scholar] [CrossRef]
- Slišković, A.; Tokić, A.; Šimunić, A.; Ombla, J.; Nikolić Ivanišević, M. Dobrobit Zaposlenih Roditelja Djece s Teškoćama u Razvoju: Pregled Dosadašnjih Spoznaja, Smjernice Za Daljnja Istraživanja i Praktične Implikacije. Suvremena Psychol. 2022, 25, 47–69. [Google Scholar]
- Mahmic, S.; Kern, M.L.; Janson, A. Identifying and Shifting Disempowering Paradigms for Families of Children with Disability Through a System Informed Positive Psychology Approach. Front. Psychol. 2021, 12, 663640. [Google Scholar] [CrossRef]
- Wehmeyer, M.L. The Oxford Handbook of Positive Psychology and Disability. Oxford Library of Psychology; Oxford University Press: Oxford, UK, 2013; ISBN 978-0-19-539878-6. [Google Scholar]
- Beighton, C.; Wills, J. How Parents Describe the Positive Aspects of Parenting Their Child Who Has Intellectual Disabilities: A Systematic Review and Narrative Synthesis. J. Appl. Res. Intellect. Disabil. 2019, 32, 1255–1279. [Google Scholar] [CrossRef]
- Lodewyks, M.R. Parent and Child Perceptions of the Positive Effects That a Child with a Disability Has on the Family; University of Manitoba: Winnipeg, MB, Canada, 2009. [Google Scholar]
- Lodewyks, M.R. Strength in Diversity: Positive Impacts of Children with Disabilities. Transition 2015, 45. Available online: https://vanierinstitute.ca/strength-in-diversity-positive-impacts-of-children-with-disabilities/ (accessed on 6 July 2023).
- Manor-Binyamini, I. Positive Aspects of Coping among Mothers of Adolescent Children with Developmental Disability in the Druze Community in Israel. J. Intellect. Dev. Disabil. 2016, 41, 97–106. [Google Scholar] [CrossRef]
- Sheldon, J.P.; Oliver, M.; Yashar, B.M. Rewards and Challenges of Parenting a Child with Down Syndrome: A Qualitative Study of Fathers’ Perceptions. Disabil. Rehabil. 2021, 43, 3562–3573. [Google Scholar] [CrossRef]
- Strecker, S.; Hazelwood, Z.J.; Shakespeare-Finch, J. Postdiagnosis Personal Growth in an Australian Population of Parents Raising Children with Developmental Disability. J. Intellect. Dev. Disabil. 2014, 39, 1–9. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Shakespeare-Finch, J.; Taku, K.; Calhoun, L.G. Components of the Theoretical Model of Posttraumatic Growth. In Posttraumatic Growth; Routledge: London, UK, 2018; ISBN 978-1-315-52745-1. [Google Scholar]
- Janoff-Bulman, R. Posttraumatic Growth: Three Explanatory Models. Psychol. Inq. 2004, 15, 30–34. [Google Scholar]
- Stewart, M.; Knight, T.; McGillivray, J.; Forbes, D.; Austin, D.W. Through a Trauma-Based Lens: A Qualitative Analysis of the Experience of Parenting a Child with an Autism Spectrum Disorder. J. Intellect. Dev. Disabil. 2017, 42, 212–222. [Google Scholar] [CrossRef]
- Counselman-Carpenter, E.A. The Presence of Posttraumatic Growth (PTG) in Mothers Whose Children Are Born Unexpectedly with Down Syndrome. J. Intellect. Dev. Disabil. 2017, 42, 351–363. [Google Scholar] [CrossRef]
- Young, S.; Shakespeare-Finch, J.; Obst, P. Raising a Child with a Disability: A One-Year Qualitative Investigation of Parent Distress and Personal Growth. Disabil. Soc. 2019, 35, 629–653. [Google Scholar] [CrossRef]
- Barnett, D.; Clements, M.; Kaplan-Estrin, M.; Fialka, J. Building New Dreams: Supporting Parents’ Adaptation to Their Child with Special Needs. Infants Young Child. 2003, 16, 184–200. [Google Scholar] [CrossRef]
- Krakovich, T.; Mcgrew, J.; Yu, Y.; Ruble, L. Stress in Parents of Children with Autism Spectrum Disorder: An Exploration of Demands and Resources. J. Autism Dev. Disord. 2016, 46, 2042–2053. [Google Scholar] [CrossRef]
- Gérain, P.; Zech, E. Informal Caregiver Burnout? Development of a Theoretical Framework to Understand the Impact of Caregiving. Front. Psychol. 2019, 10, 1748. [Google Scholar] [CrossRef]
- Tahmouresi, N.; Bender, C.; Schmitz, J.; Baleshzar, A.; Tuschen-Caffier, B. Similarities and Differences in Emotion Regulation and Psychopathology in Iranian and German School-Children: A Cross-Cultural Study. Int. J. Prev. Med. 2014, 5, 52–60. [Google Scholar]
- Garnefski, N.; Kraaij, V. Cognitive Emotion Regulation Questionnaire-Development of a Short 18-Item Version (CERQ-Short). Personal. Individ. Differ. 2006, 41, 1045–1053. [Google Scholar] [CrossRef]
- Woodman, A.C.; Hauser-Cram, P. The Role of Coping Strategies in Predicting Change in Parenting Efficacy and Depressive Symptoms among Mothers of Adolescents with Developmental Disabilities. J. Intellect. Disabil. Res. 2013, 57, 513–530. [Google Scholar] [CrossRef]
- Craig, A.; Cooper, R.E. 11—Symptoms of Acute and Chronic Fatigue. In State and Trait; Smith, A.P., Jones, D.M., Eds.; Academic Press: London, UK, 1992; pp. 289–339. ISBN 978-0-12-650353-1. [Google Scholar]
- Headrick, L.; Newman, D.A.; Park, Y.A.; Liang, Y. Recovery Experiences for Work and Health Outcomes: A Meta-Analysis and Recovery-Engagement-Exhaustion Model. J. Bus. Psychol. 2023, 38, 821–864. [Google Scholar] [CrossRef]
- Geurts, S.A.E.; Sonnentag, S. Recovery as an Explanatory Mechanism in the Relation between Acute Stress Reactions and Chronic Health Impairment. Scand. J. Work Environ. Health 2006, 32, 482–492. [Google Scholar] [CrossRef]
- McEwen, B.S. Stress, Adaptation, and Disease. Allostasis and Allostatic Load. Ann. N. Y Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef]
- Sonnentag, S.; Fritz, C. The Recovery Experience Questionnaire: Development and Validation of a Measure for Assessing Recuperation and Unwinding from Work. J. Occup. Health Psychol. 2007, 12, 204–221. [Google Scholar] [CrossRef]
- Sonnentag, S.; Venz, L.; Casper, A. Advances in Recovery Research: What Have We Learned? What Should Be Done Next? J. Occup. Health Psychol. 2017, 22, 365–380. [Google Scholar] [CrossRef]
- Ombla, J.; Slišković, A.; Nikolić Ivanišević, M.; Šimunić, A.; Ljubičić, M. Kako zaposleni roditelji djece s teškoćama u razvoju usklađuju zahtjeve radne i obiteljske uloge? Kvalitativno istraživanje. Rev. Sociol. 2023, 53, 67–97. [Google Scholar] [CrossRef]
- Kurtz-Nelson, E.; McIntyre, L.L. Optimism and Positive and Negative Feelings in Parents of Young Children with Developmental Delay. J. Intellect. Disabil. Res. 2017, 61, 719–725. [Google Scholar] [CrossRef]
- Rafferty, D.; Preston, M.; Sullivan, W.; Ekas, N. Chaotic Family Environments and Depressive Symptoms in Parents of Autistic Children: The Protective Role of Optimism. Res. Autism Spectr. Disord. 2022, 96, 102000. [Google Scholar] [CrossRef]
- Khusaifan, S.J.; El Keshky, M.E.S. Social Support as a Protective Factor for the Well-Being of Parents of Children with Autism in Saudi Arabia. J. Pediatr. Nurs. 2021, 58, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.J. Work-Family Facilitation and Conflict, Working Fathers and Mothers, Work-Family Stressors and Support. J. Fam. Issues 2005, 26, 793–819. [Google Scholar] [CrossRef]
- Holmes, E.K.; Thomas, C.R.; Petts, R.J.; Hill, E.J. Chapter 10—The Work-Family Interface. In Cross-Cultural Family Research and Practice; Halford, W.K., van de Vijver, F., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 323–354. ISBN 978-0-12-815493-9. [Google Scholar]
- Frone, M.R. Work-Family Balance. In Handbook of Occupational Health Psychology; American Psychological Association: Washington, DC, USA, 2003; pp. 143–162. ISBN 978-1-55798-927-7. [Google Scholar]
- Grzywacz, J.G.; Bass, B.L. Work, Family, and Mental Health: Testing Different Models of Work-Family Fit. J. Marriage Fam. 2003, 65, 248–261. [Google Scholar] [CrossRef]
- Wayne, J.H.; Grzywacz, J.G.; Carlson, D.S.; Kacmar, K.M. Work–Family Facilitation: A Theoretical Explanation and Model of Primary Antecedents and Consequences. Hum. Resour. Manag. Rev. 2007, 17, 63–76. [Google Scholar] [CrossRef]
- Karatepe, O.M.; Bekteshi, L. Antecedents and Outcomes of Work–Family Facilitation and Family–Work Facilitation among Frontline Hotel Employees. Int. J. Hosp. Manag. 2008, 27, 517–528. [Google Scholar] [CrossRef]
- Agrawal, M.; Mahajan, R. The Effect of Optimism on the Work-Family Interface and Psychological Health of Indian Police. Polic. Int. J. 2021, 44, 725–740. [Google Scholar] [CrossRef]
- Wepfer, A.G.; Allen, T.D.; Brauchli, R.; Jenny, G.J.; Bauer, G.F. Work-Life Boundaries and Well-Being: Does Work-to-Life Integration Impair Well-Being through Lack of Recovery? J. Bus. Psychol. 2018, 33, 727–740. [Google Scholar] [CrossRef]
- Rotondo, D.M.; Kincaid, J.F. Conflict, Facilitation, and Individual Coping Styles across the Work and Family Domains. J. Manag. Psychol. 2008, 23, 484–506. [Google Scholar] [CrossRef]
- Al-Yagon, M.; Cinamon, R.G. Work–Family Relations among Mothers of Children with Learning Disorders. Eur. J. Spec. Needs Educ. 2008, 23, 91–107. [Google Scholar] [CrossRef]
- Parchomiuk, M. Work-Family Balance and Satisfaction with Roles in Parents of Disabled Children. Community Work Fam. 2022, 25, 353–373. [Google Scholar] [CrossRef]
- Slišković, A. Kratki upitnik mentalnog zdravlja. In Zbirka Psihologijskih Skala i Upitnika, Svezak 10; Ćubela-Adorić, V., Burić, I., Macuka, I., Nikolić Ivanišević, M., Slišković, A., Eds.; Morepress: Zadar, Croatia, 2020; pp. 27–38. [Google Scholar]
- Wayne, J.H.; Musisca, N.; Fleeson, W. Considering the Role of Personality in the Work–Family Experience: Relationships of the Big Five to Work–Family Conflict and Facilitation. J. Vocat. Behav. 2004, 64, 108–130. [Google Scholar] [CrossRef]
- Buljan, T. Prediktori Usklađivanja Obiteljske i Radne Uloge za Vrijeme Pandemije Koronavirusa. Master Thesis, University of Zagreb, Zagreb, Croatia, 2020. [Google Scholar]
- Penezić, Z. SKALA OPTIMIZMA-PESIMIZMA (O-P skala). In Zbirka Psihologijskih Skala i Upitnika, Svezak 1; Lacković-Grgin, K., Proroković, A., Ćubela, V., Penezić, Z., Eds.; Morepress: Zadar, Croatia, 2002; pp. 15–17. [Google Scholar]
- Chang, E.C.; D’Zurilla, T.J.; Maydeu-Olivares, A. Assessing the Dimensionality of Optimism and Pessimism Using a Multimeasure Approach. Cogn. Ther. Res. 1994, 18, 143–160. [Google Scholar] [CrossRef]
- Garnefski, N.; Kraaij, V.; Spinhoven, P. Negative Life Events, Cognitive Emotion Regulation and Emotional Problems. Personal. Individ. Differ. 2001, 30, 1311–1327. [Google Scholar] [CrossRef]
- Soldo, L.; Vulić-Prtorić, A. Upitnik Kognitivne Emocionalne Regulacije (CERQ). In Zbirka Psihologijskih Skala i Upitnika, Svezak 9; Slišković, A., Burić, I., Ćubela-Adorić, V., Nikolić, M., Tucak Junaković, I., Eds.; Morepress: Zadar, Croatia, 2018; pp. 47–58. [Google Scholar]
- Macuka, I. Upitnik posttraumatskog rasta. In Zbirka Psihologijskih Skala i Upitnika, Svezak 10; Ćubela-Adorić, V., Burić, I., Macuka, I., Nikolić Ivanišević, M., Slišković, A., Eds.; Morepress: Zadar, Croatia, 2020; pp. 121–130. [Google Scholar]
- Tedeschi, R.G.; Calhoun, L.G. The Posttraumatic Growth Inventory: Measuring the Positive Legacy of Trauma. J. Trauma. Stress 1996, 9, 455–471. [Google Scholar] [CrossRef]
- Šimunić, A.; Gregov, L.; Proroković, A. Skala socijalne podrške na poslu i u obitelji. In Zbirka Psihologijskih Skala i Upitnika 8; Tucak Junaković, I., Burić, I., Ćubela-Adorić, V., Proroković, A., Slišković, A., Eds.; Morepress: Zadar, Croatia, 2016; pp. 45–53. [Google Scholar]
- TIBCO® Data Science-Workbench 14.1.0. Available online: https://docs.tibco.com/products/tibco-data-science-workbench-14-1-0 (accessed on 6 July 2023).
- Mplus User’s Guide. Available online: https://www.statmodel.com/html_ug.shtml (accessed on 6 July 2023).
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Danks, N.P.; Ray, S. An Introduction to Structural Equation Modeling. In Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R: A Workbook; Hair, J.F., Jr., Hult, G.T.M., Ringle, C.M., Sarstedt, M., Danks, N.P., Ray, S., Eds.; Classroom Companion: Business; Springer International Publishing: Cham, Switzerland, 2021; pp. 1–29. ISBN 978-3-030-80519-7. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford Publications: New York, NY, USA, 2005; ISBN 978-1-59385-075-3. [Google Scholar]
- Lapierre, L.M.; Li, Y.; Kwan, H.K.; Greenhaus, J.H.; DiRenzo, M.S.; Shao, P. A Meta-Analysis of the Antecedents of Work–Family Enrichment. J. Organ. Behav. 2018, 39, 385–401. [Google Scholar] [CrossRef]
- Stryzhak, O. The Relationship between Education, Income, Economic Freedom and Happiness. SHS Web Conf. 2020, 75, 03004. [Google Scholar] [CrossRef]
- Ratniewski, J. Antecedents of Work-Family Facilitation: The Role of Coping Styles, Organizational and Family Support, and Gender Role Attitudes. Diss. Abstr. Int. Sect. B Sci. Eng. 2013, 74. Available online: https://psycnet.apa.org/record/2013-99160-268 (accessed on 6 July 2023).
- Lapierre, L.M.; Allen, T.D. Control at Work, Control at Home, and Planning Behavior: Implications for Work–Family Conflict. J. Manag. 2012, 38, 1500–1516. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H. A Happy Person, a Healthy Person? J. Am. Geriatr. Soc. 2000, 48, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Ciglar, J. Rodne Razlike u Ravnoteži Između Posla i Obitelji i Predikcija Zadovoljstva Životom. Master Thesis, University of Zagreb, Zagreb, Croatia, 2021. [Google Scholar]
- Kimura, M. Social Determinants of Self-Rated Health among Japanese Mothers of Children with Disabilities. Prev. Med. Rep. 2018, 10, 129–135. [Google Scholar] [CrossRef]
- Kimura, M.; Yamazaki, Y. Having Another Child without Intellectual Disabilities: Comparing Mothers of a Single Child with Disability and Mothers of Multiple Children with and without Disability. J. Intellect. Disabil. 2019, 23, 216–232. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F. Dispositional Optimism. Trends Cogn. Sci. 2014, 18, 293–299. [Google Scholar] [CrossRef]
- Laranjeira, C.; Querido, A. Hope and Optimism as an Opportunity to Improve the “Positive Mental Health” Demand. Front. Psychol. 2022, 13, 827320. [Google Scholar] [CrossRef] [PubMed]
- Bourke-Taylor, H.M.; Joyce, K.S.; Morgan, P.; Reddihough, D.S.; Tirlea, L. Maternal and Child Factors Associated with the Health-Promoting Behaviours of Mothers of Children with a Developmental Disability. Res. Dev. Disabil. 2021, 118, 104069. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.; Willis, K.; Bismark, M.; Smallwood, N. A Time for Self-Care? Frontline Health Workers’ Strategies for Managing Mental Health during the COVID-19 Pandemic. SSM-Mental Health 2021, 2, 100053. [Google Scholar] [CrossRef]
- Luis, E.; Bermejo-Martins, E.; Martinez, M.; Sarrionandia, A.; Cortes, C.; Oliveros, E.Y.; Garces, M.S.; Oron, J.V.; Fernández-Berrocal, P. Relationship between Self-Care Activities, Stress and Well-Being during COVID-19 Lockdown: A Cross-Cultural Mediation Model. BMJ Open 2021, 11, e048469. [Google Scholar] [CrossRef]
- Avasthi, A.; Sahoo, S. Impact, Role, and Contribution of Family in the Mental Health of Industrial Workers. Ind. Psychiatry J. 2021, 30, S301–S304. [Google Scholar] [CrossRef]
- Masten, A.S.; Coatsworth, J.D. The Development of Competence in Favorable and Unfavorable Environments. Lessons from Research on Successful Children. Am. Psychol. 1998, 53, 205–220. [Google Scholar] [CrossRef]
- Masten, A.S. Resilience Theory and Research on Children and Families: Past, Present, and Promise. J. Fam. Theory Rev. 2018, 10, 12–31. [Google Scholar] [CrossRef]
- Hill, E.J.; Allen, S.; Jacob, J.; Bair, A.F.; Bikhazi, S.L.; Van Langeveld, A.; Martinengo, G.; Parker, T.T.; Walker, E. Work—Family Facilitation: Expanding Theoretical Understanding Through Qualitative Exploration. Adv. Dev. Hum. Resour. 2007, 9, 507–526. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | Descriptive Parameters |
|---|---|
| Age | M = 40.9, SD = 6.15, Min = 23, Max = 66 |
| Education | Elementary school (n = 4); Secondary school (n = 237); Bachelor’s degree (n = 90) Master’s degree (n = 205) Doctoral degree (n = 35) |
| Marital status | Extramarital union (n = 57) Married (n = 450) Separated or divorced (n = 46) Single (n = 14) Widow/er (n = 4) |
| Number of children | Mode = 2 (f = 267), Min = 1, Max = 6 |
| Number of children with disabilities | Mode = 1 (f = 514); Min = 1, Max = 4 |
| Highest degree of disability among children | 4th— most severe level of impairment (n = 204) 3rd—severe level of impairment (n = 158) 2nd—moderate level of impairment (n = 70) 1st—mild level of impairment (n = 35) Do not know/not sure (n = 104) |
| Employment sector | Public (n = 265) Private (n = 306) |
| Partner’s employment | Yes (n = 463) No (n = 24) Caregiver (n = 20) |
| N | M | SD | Min | Max | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|---|
| Gender (0—men; 1—women) | 571 | 0.91 | 0.29 | 0.00 | 1.00 | −2.78 | 5.74 |
| Age | 564 | 40.90 | 6.15 | 23.00 | 66.00 | 0.27 | 0.24 |
| Education | 571 | 3.05 | 1.02 | 1.00 | 5.00 | 0.20 | −1.35 |
| Number of children | 571 | 2.20 | 0.99 | 1.00 | 6.00 | 1.05 | 1.57 |
| Optimism | 571 | 3.62 | 0.70 | 1.00 | 5.00 | −0.76 | 1.09 |
| Emotional regulation—positive refocusing | 571 | 3.24 | 0.86 | 1.00 | 5.00 | −0.26 | −0.09 |
| Emotional regulation—planning | 571 | 4.05 | 0.64 | 1.00 | 5.00 | −0.62 | 1.34 |
| Posttraumatic growth—personal strength | 571 | 3.31 | 1.09 | 0.00 | 5.00 | −0.92 | 0.88 |
| Recovery management | 568 | 2.80 | 1.06 | 1.00 | 5.00 | 0.15 | −0.68 |
| Social support at work | 565 | 4.98 | 1.26 | 1.00 | 7.00 | −0.72 | 0.61 |
| Social support in the family | 566 | 5.27 | 1.27 | 1.25 | 7.00 | −0.66 | −0.15 |
| Work-to-family facilitation | 566 | 2.91 | 0.83 | 1.00 | 5.00 | −0.06 | −0.09 |
| Family-to-work facilitation | 563 | 3.41 | 0.82 | 1.00 | 5.00 | −0.27 | −0.03 |
| Mental health | 571 | 3.75 | 0.86 | 1.00 | 6.00 | −0.49 | 0.09 |
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| −0.10 | −0.01 | −0.04 | 0.04 | 0.04 | 0.06 | 0.05 | −0.15 | −0.00 | −0.08 | 0.00 | −0.09 | −0.09 |
| - | 0.10 | 0.12 | −0.07 | −0.04 | −0.05 | −0.05 | 0.09 | −0.07 | −0.08 | 0.01 | −0.17 | −0.04 |
| - | −0.15 | −0.04 | −0.10 | −0.01 | −0.10 | −0.05 | 0.03 | −0.00 | 0.15 | 0.00 | −0.05 | |
| - | 0.16 | 0.12 | 0.09 | 0.13 | 0.04 | 0.05 | 0.06 | −0.02 | 0.13 | 0.17 | ||
| - | 0.47 | 0.34 | 0.52 | 0.35 | 0.36 | 0.39 | 0.27 | 0.45 | 0.58 | |||
| - | 0.19 | 0.38 | 0.23 | 0.16 | 0.20 | 0.17 | 0.26 | 0.40 | ||||
| - | 0.26 | 0.05 | 0.13 | 0.15 | 0.11 | 0.29 | 0.11 | |||||
| - | 0.26 | 0.22 | 0.25 | 0.25 | 0.42 | 0.44 | ||||||
| - | 0.32 | 0.38 | 0.26 | 0.29 | 0.46 | |||||||
| - | 0.48 | 0.33 | 0.35 | 0.29 | ||||||||
| - | 0.18 | 0.56 | 0.42 | |||||||||
| - | 0.35 | 0.18 | ||||||||||
| - | 0.42 | |||||||||||
| - |
| Model Relationship | Standardized Estimate (STDYX) | Standard Error (STDYX) | Two-Tailed p-Value (STDYX) |
|---|---|---|---|
| Non-significant path coefficients | |||
| Optimism → Work-to-family facilitation | 0.090 | 0.050 | 0.084 |
| Work-to-family facilitation → Mental health | −0.073 | 0.037 | 0.051 |
| Indirect Effects: | Non-Standardized Estimates of the Indirect Effect | 95% Confidence Interval (k = 1000) |
|---|---|---|
| Optimism → Family-to-work facilitation → Mental health | 0.020 | 0.005; 0.046 |
| Emotional regulation: Planning → Family-to-work facilitation → Mental health | 0.042 | 0.019; 0.074 |
| Posttraumatic growth: Personal strength → Family-to-work facilitation → Mental health | 0.041 | 0.021; 0.069 |
| Social support in the family → Family-to-work facilitation → Mental health | 0.070 | 0.040; 0.105 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šimunić, A.; Slišković, A.; Tokić, A.; Ombla, J.; Stewart, L. The Roles of Personal and Environmental Resources in Predicting Work–Family Facilitation and Mental Health among Employed Parents of Children with Disabilities in Croatia. Behav. Sci. 2023, 13, 710. https://doi.org/10.3390/bs13090710
Šimunić A, Slišković A, Tokić A, Ombla J, Stewart L. The Roles of Personal and Environmental Resources in Predicting Work–Family Facilitation and Mental Health among Employed Parents of Children with Disabilities in Croatia. Behavioral Sciences. 2023; 13(9):710. https://doi.org/10.3390/bs13090710
Chicago/Turabian StyleŠimunić, Ana, Ana Slišković, Andrea Tokić, Jelena Ombla, and Lisa Stewart. 2023. "The Roles of Personal and Environmental Resources in Predicting Work–Family Facilitation and Mental Health among Employed Parents of Children with Disabilities in Croatia" Behavioral Sciences 13, no. 9: 710. https://doi.org/10.3390/bs13090710
APA StyleŠimunić, A., Slišković, A., Tokić, A., Ombla, J., & Stewart, L. (2023). The Roles of Personal and Environmental Resources in Predicting Work–Family Facilitation and Mental Health among Employed Parents of Children with Disabilities in Croatia. Behavioral Sciences, 13(9), 710. https://doi.org/10.3390/bs13090710