
Virtual Reality Utilized for Safety Skills Training for Autistic Individuals: A Review

 ,
,
Abstract
1. Introduction
- What is the appropriate age for ASD patients to apply VR for safety skills training?
- Are VR treatments effective, and does the level of VR immersion affect the effectiveness of the intervention and its effect on generalization?
- How can we use VR technology to implement personalized safety skills training for people with autism?
2. Materials and Methods
2.1. Inclusion Criteria and Exclusion Criteria
- The study had to be published in a peer-reviewed article.
- The study had to include at least one patient diagnosed by a clinician or identified as having ASD using a standardized diagnostic tool.
- The study had to use virtual reality for ASD intervention or training to provide effectiveness or feasibility results.
- The study had to implement skill-specific interventions that improved the independence and safety of people with ASD.
- The intervention means had to be VR devices with different levels of immersion (immersive, semi-immersive, non-immersive), and the intervention content had to include a variety of safety skills.
- Studies that did not include a therapeutic intervention as the independent variable were excluded.
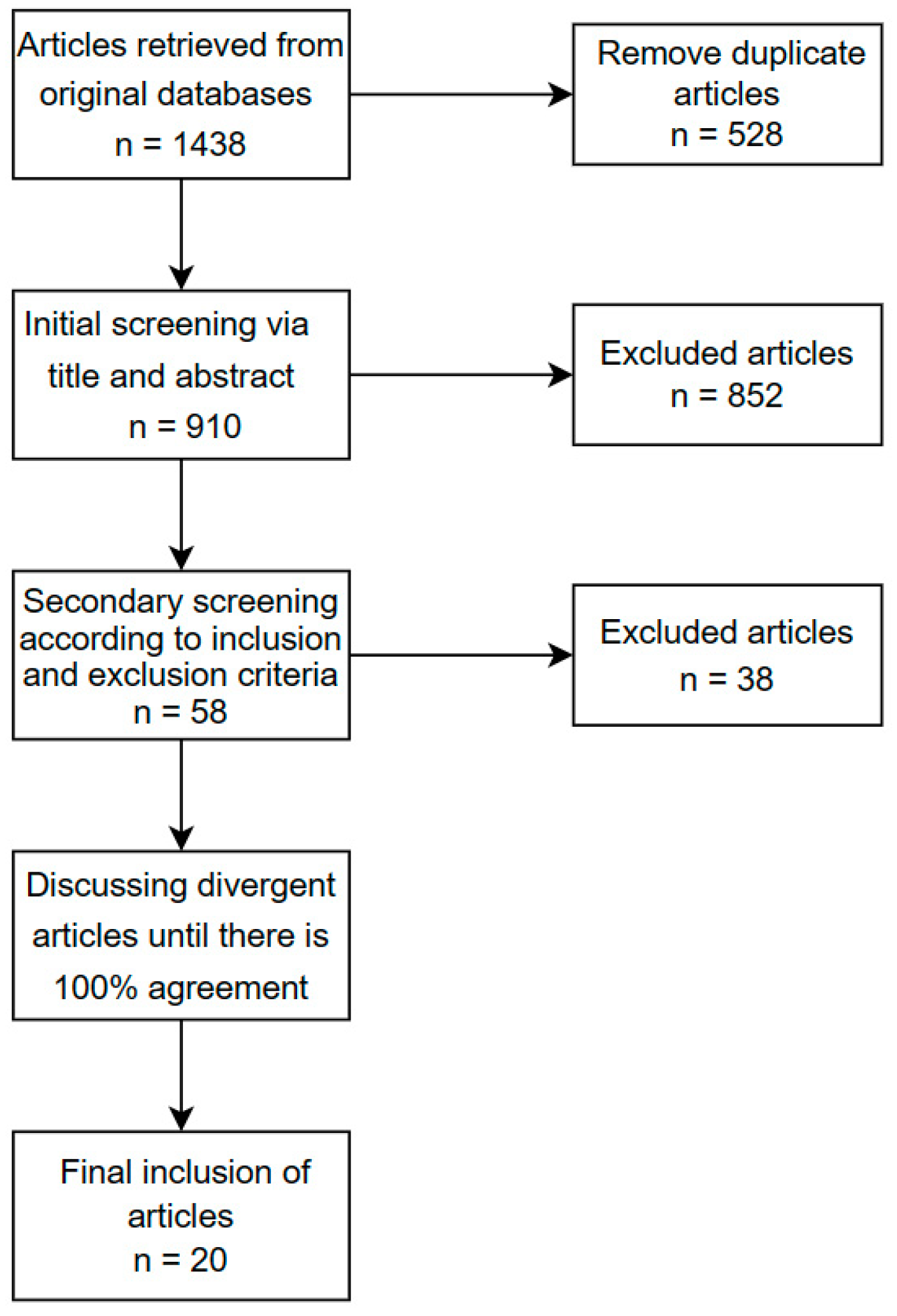
2.2. Research Process
3. Results
3.1. Intervention Purpose
3.2. Intervention Subjects
3.3. Application of Virtual Reality
3.3.1. Application of Immersive Virtual Reality
3.3.2. Application of Semi-Immersive Virtual Reality
3.3.3. Application of Non-Immersive Virtual Reality
3.4. Research Methods
3.5. Skill Generalization
4. Discussion
4.1. Appropriate Age for Safety Skills Training Using VR in ASD Patients
4.2. Effectiveness of VR Interventions and the Relationship between the Immersion Level of VR and the Intervention and Generalization Effects
4.3. Using VR Technology to Provide Personalized Safety Skills Interventions for Individuals with Autism Spectrum Disorder
4.4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Lolk, A. Neurokognitive lidelser. In Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Maenner, M.J.; Warren, Z.; Williams, A.R.; Amoakohene, E.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Fitzgerald, R.T.; Furnier, S.M.; Hughes, M.M.; et al. Prevalence and Characteristics of Autism Spectrum Disorder among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. Morb. Mortal. Wkly. Rep. 2023, 72, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.C.; Harrington, R.A.; Chang, J.J.; Connors, S.L. Increased Risk of Injury in Children with Developmental Disabilities. Res. Dev. Disabil. 2008, 29, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Guan, J.; Li, G. Injury Mortality in Individuals with Autism. Am. J. Public Health 2017, 107, 791–793. [Google Scholar] [CrossRef]
- Dixon, D.R.; Bergstrom, R.; Smith, M.N.; Tarbox, J. A Review of Research on Procedures for Teaching Safety Skills to Persons with Developmental Disabilities. Res. Dev. Disabil. 2010, 31, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Brok, W.L.J.E.D.; Sterkenburg, P.S. Self-Controlled Technologies to Support Skill Attainment in Persons with an Autism Spectrum Disorder and/or an Intellectual Disability: A Systematic Literature Review. Disabil. Rehabil. Assist. Technol. 2014, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mesa-Gresa, P.; Oltra-Badenes, R.; Lozano-Quilis, J.-A.; Gil-Gómez, J.-A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.; Newbutt, N. Autism and Virtual Reality Head-Mounted Displays: A State of the Art Systematic Review. J. Enabling Technol. 2018, 12, 101–113. [Google Scholar] [CrossRef]
- Di Natale, A.F.; Repetto, C.; Riva, G.; Villani, D. Immersive Virtual Reality in K-12 and Higher Education: A 10-year Systematic Review of Empirical Research. Br. J. Educ. Technol. 2020, 51, 2006–2033. [Google Scholar] [CrossRef]
- Burdea, G.; Coiffet, P. Virtual Reality Technology. Presence Teleoperators Virtual Environ. 2003, 12, 663–664. [Google Scholar] [CrossRef]
- Bozgeyikli, L.; Raij, A.; Katkoori, S.; Alqasemi, R. A Survey on Virtual Reality for Individuals with Autism Spectrum Disorder: Design Considerations. IEEE Trans. Learn. Technol. 2018, 11, 133–151. [Google Scholar] [CrossRef]
- Smith, M.J.; Ginger, E.J.; Wright, M.; Wright, K.; Humm, L.B.; Olsen, D.E.; Bell, M.D.; Fleming, M.F. Virtual Reality Job Interview Training for Individuals with Psychiatric Disabilities. J. Nerv. Ment. Dis. 2014, 202, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Kandalaft, M.R.; Didehbani, N.; Krawczyk, D.C.; Allen, T.T.; Chapman, S.B. Virtual Reality Social Cognition Training for Young Adults with High-Functioning Autism. J. Autism Dev. Disord. 2012, 43, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.U.; Rosenthal, M.Z.; Gwaltney, M.; Jarrold, W.; Hatt, N.; McIntyre, N.S.; Swain, L.; Solomon, M.; Mundy, P. A Virtual Joy-Stick Study of Emotional Responses and Social Motivation in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2014, 45, 3891–3899. [Google Scholar] [CrossRef]
- Nubia, R.M.; Fabian, G.R.; Wilson, R.A.; Wilmer, P.B. Development of a Mobile Application in Augmented Reality to Improve the Communication Field of Autistic Children at a Neurorehabilitar Clinic. In Proceedings of the 2015 Workshop on Engineering Applications—International Congress on Engineering (WEA), Bogota, Colombia, 28–30 October 2015. [Google Scholar]
- Tzanavari, A.; Charalambous-Darden, N.; Herakleous, K.; Poullis, C. Effectiveness of an Immersive Virtual Environment (CAVE) for Teaching Pedestrian Crossing to Children with PDD-NOS. In Proceedings of the 2015 IEEE 15th International Conference on Advanced Learning Technologies, Hualien, Taiwan, 6–9 July 2015. [Google Scholar]
- Saiano, M.; Garbarino, E.; Lumachi, S.; Solari, S.; Sanguineti, V. Effect of Interface Type in the VR-Based Acquisition of Pedestrian Skills in Persons with ASD. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015. [Google Scholar]
- Saiano, M.; Pellegrino, L.; Casadio, M.; Summa, S.; Garbarino, E.; Rossi, V.; Dall’Agata, D.; Sanguineti, V. Natural Interfaces and Virtual Environments for the Acquisition of Street Crossing and Path Following Skills in Adults with Autism Spectrum Disorders: A Feasibility Study. J. Neuroeng. Rehabil. 2015, 12, 17. [Google Scholar] [CrossRef] [PubMed]
- Dixon, D.R.; Miyake, C.; Nohelty, K.; Novack, M.N.; Granpeesheh, D. Evaluation of an Immersive Virtual Reality Safety Training Used to Teach Pedestrian Skills to Children with Autism Spectrum Disorder. Behav. Anal. Pract. 2019, 13, 631–640. [Google Scholar] [CrossRef]
- Tan, Q.P.; Huang, L.; Xu, D.; Cen, Y.; Cao, Q. Serious Game for VR Road Crossing in Special Needs Education. Electronics 2022, 11, 2568. [Google Scholar] [CrossRef]
- Fornasari, L.; Chittaro, L.; Ieronutti, L.; Cottini, L.; Dassi, S.; Cremaschi, S.; Molteni, M.; Fabbro, F.; Brambilla, P. Navigation and Exploration of an Urban Virtual Environment by Children with Autism Spectrum Disorder Compared to Children with Typical Development. Res. Autism. Spectr. Disord. 2013, 7, 956–965. [Google Scholar] [CrossRef]
- Cox, D.J.; Brown, T.S.; Ross, V.; Moncrief, M.; Schmitt, R.; Gaffney, G.R.; Reeve, R. Can Youth with Autism Spectrum Disorder Use Virtual Reality Driving Simulation Training to Evaluate and Improve Driving Performance? An Exploratory Study. J. Autism. Dev. Disord. 2017, 47, 2544–2555. [Google Scholar] [CrossRef]
- Fan, J.; Wade, J.; Bian, D.; Key, A.P.; Warren, Z.; Mion, L.C.; Sarkar, N. A Step towards EEG-Based Brain Computer Interface for Autism Intervention. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015. [Google Scholar]
- Zhang, L.; Wade, J.; Bian, D.; Fan, J.; Swanson, A.; Weitlauf, A.; Warren, Z.; Sarkar, N. Cognitive Load Measurement in a Virtual Reality-Based Driving System for Autism Intervention. IEEE Trans. Affect. Comput. 2017, 8, 176–189. [Google Scholar] [CrossRef]
- Wade, J.; Zhang, L.; Bian, D.; Fan, J.; Swanson, A.; Weitlauf, A.; Sarkar, M.S.; Warren, Z.; Sarkar, N. A Gaze-Contingent Adaptive Virtual Reality Driving Environment for Intervention in Individuals with Autism Spectrum Disorders. ACM Trans. Interact. Intell. Syst. 2016, 6, 1–23. [Google Scholar] [CrossRef]
- Ross, V.; Cox, D.J.; Reeve, R.; Brown, T.L.; Moncrief, M.; Schmitt, R.; Gaffney, G.R. Measuring the Attitudes of Novice Drivers with Autism Spectrum Disorder as an Indication of Apprehensive Driving: Going beyond Basic Abilities. Autism 2017, 22, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Wade, J.; Key, A.P.; Warren, Z.; Sarkar, N. EEG-Based Affect and Workload Recognition in a Virtual Driving Environment for ASD Intervention. IEEE Trans. Biomed. Eng. 2018, 65, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Patrick, K.E.; Schultheis, M.T.; Agate, F.T.; McCurdy, M.R.; Daly, B.P.; Tarazi, R.A.; Chute, D.L.; Hurewitz, F. Executive Function “Drives” Differences in Simulated Driving Performance between Young Adults with and without Autism Spectrum Disorder. Child Neuropsychol. 2020, 26, 649–665. [Google Scholar] [CrossRef] [PubMed]
- Baker-Ericzén, M.J.; Smith, L.; Tran, A.N.; Scarvie, K.M. A Cognitive Behavioral Intervention for Driving for Autistic Teens and Adults: A Pilot Study. Autism Adulthood 2021, 3, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Bian, D.; Wade, J.; Swanson, A.; Weitlauf, A.; Warren, Z.; Sarkar, N. Design of a Physiology-Based Adaptive Virtual Reality Driving Platform for Individuals with ASD. ACM Trans. Access. Comput. 2019, 12, 1–24. [Google Scholar] [CrossRef]
- Miller, I.; Wiederhold, B.K.; Miller, C.S.; Wiederhold, M.D. Virtual Reality Air Travel Training with Children on the Autism Spectrum: A Preliminary Report. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.; Miller, C.S.; Wiederhold, M.D.; Wiederhold, B.K. Virtual Reality Air Travel Training Using Apple iPhone X and Google Cardboard: A Feasibility Report with Autistic Adolescents and Adults. Autism Adulthood 2020, 2, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Glaser, N. Investigating the Usability and Learner Experience of a Virtual Reality Adaptive Skills Intervention for Adults with Autism Spectrum Disorder. Educ. Technol. Res. Dev. 2021, 69, 1665–1699. [Google Scholar] [CrossRef]
- Simões, M.; Bernardes, M.; Barros, F.J.; Castelo-Branco, M. Virtual Travel Training for Autism Spectrum Disorder: Proof-of-Concept Interventional Study. JMIR Serious Games 2018, 6, e5. [Google Scholar] [CrossRef]
- Schmidt, M.; Glaser, N.; Schmidt, C.; Kaplan, R.; Palmer, H.; Cobb, S. Programming for Generalization: Confronting Known Challenges in the Design of Virtual Reality Interventions for Autistic Users. Comput. Educ. 2023, 2, 100013. [Google Scholar] [CrossRef]
- Loomes, R.; Hull, L.; Mandy, W. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry. 2017, 56, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Carreon, A.; Smith, S.J.; Mosher, M.; Rao, K.; Rowland, A. A Review of Virtual Reality Intervention Research for Students with Disabilities in K–12 Settings. J. Spec. Educ. Technol. 2020, 37, 82–99. [Google Scholar] [CrossRef]
- Monahan, M.; Classen, S.; Helsel, P.V. Pre-Driving Evaluation of a Teen with Attention Deficit Hyperactivity Disorder and Autism Spectrum Disorder. Can. J. Occup. Ther. 2013, 80, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Cox, N.B.; Reeve, R.E.; Cox, S.; Cox, D.J. Brief Report: Driving and Young Adults with ASD: Parents’ Experiences. J. Autism Dev. Disord. 2012, 42, 2257–2262. [Google Scholar] [CrossRef] [PubMed]
- Daly, B.P.; Nicholls, E.; Patrick, K.E.; Brinckman, D.D.; Schultheis, M.T. Driving Behaviors in Adults with Autism Spectrum Disorders. J. Autism Dev. Disord. 2014, 44, 3119–3128. [Google Scholar] [CrossRef] [PubMed]
- Glaser, N.; Schmidt, M.; Schmidt, C. Learner Experience and Evidence of Cybersickness: Design Tensions in a Virtual Reality Public Transportation Intervention for Autistic Adults. Virtual Real. 2022, 26, 1705–1724. [Google Scholar] [CrossRef]
- Carreon, A.; Smith, S.J.; Frey, B.B.; Rowland, A.; Mosher, M. Comparing Immersive VR and Non-Immersive VR on Social Skill Acquisition for Students in Middle School with ASD. J. Res. Technol. Educ. 2023, 1–14. [Google Scholar] [CrossRef]
- Malihi, M.; Nguyen, J.; Cardy, R.E.; Eldon, S.; Petta, C.; Kushki, A. Data-Driven Discovery of Predictors of Virtual Reality Safety and Sense of Presence for Children with Autism Spectrum Disorder: A Pilot Study. Front. Psychiatry. 2020, 11, 669. [Google Scholar] [CrossRef]
- Shu, Y.; Huang, Y.Z.; Shu, C.; Chen, M.-Y. Do Virtual Reality Head-Mounted Displays Make a Difference? A Comparison of Presence and Self-Efficacy between Head-Mounted Displays and Desktop Computer-Facilitated Virtual Environments. Virtual Real. 2018, 23, 437–446. [Google Scholar] [CrossRef]
- Miller, H.L.; Bugnariu, N.L. Level of Immersion in Virtual Environments Impacts the Ability to Assess and Teach Social Skills in Autism Spectrum Disorder. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 246–256. [Google Scholar] [CrossRef]
- Cobb, S.; Beardon, L.; Eastgate, R.; Glover, T.; Kerr, S.; Neale, H.; Parsons, S.; Benford, S.; Hopkins, E.; Mitchell, P.; et al. Applied Virtual Environments to Support Learning of Social Interaction Skills in Users with Asperger’s Syndrome. Digit. Creat. 2002, 13, 11–22. [Google Scholar] [CrossRef]
- Šalkevičius, J.; Damaševičius, R.; Maskeliūnas, R.; Laukienė, I. Anxiety Level Recognition for Virtual Reality Therapy System Using Physiological Signals. Electronics 2019, 8, 1039. [Google Scholar] [CrossRef]
- Rahman, M.A.; Brown, D.J.; Mahmud, M.; Harris, M.C.; Shopland, N.; Heym, N.; Sumich, A.; Turabee, Z.B.; Standen, B.; Downes, D.; et al. Enhancing Biofeedback-Driven Self-Guided Virtual Reality Exposure Therapy through Arousal Detection from Multimodal Data Using Machine Learning. Brain Inform. 2023, 10, 14. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author | Sample Size | Age and Sex | VR Device | Level of Immersion | Intervention Purpose | Skill Generalization | Intervention Protocol |
|---|---|---|---|---|---|---|---|
| Fornasari, L., et al. [21] | 16 ASD 16 TD | 7–14 | Mouse and computer | Non-immersive | Street-crossing skills | 2 sessions, each of 45 min | |
| Tzanavari, A., et al. [16] | 6 ASD | 8–11 | VR CAVE | Immersive | Street-crossing skills | The experiment would end with a final session on a different day, at a real pedestrian crossing, to examine whether the children could generalize what they had learned. | 8 sessions |
| Saiano, M., et al. [18] | 7 ASD | 9–44 all males | Natural interfaces | Semi-immersive | Street-crossing skills | Parents/legal guardians were also required to complete a questionnaire to assess to what extent they considered that subjects had improved their behavior in real-life situations. | 10 sessions: familiarization (1–5) training (7–9) assessment (6 and 10) completion of questionnaire familiarization phase (30 min practice vocabulary of gestures) train phase (45 min) |
| Saiano, M., et al. [17] | 10 ASD GP group (n = 6) NI group (n = 4) | NI group 19–44 GP group 19–31 | Gamepad device and natural interfaces | Non-immersive and semi-immersive | Compare a modality of interaction with virtual environments based on the use of a classic gamepad with a modality based on a natural interface (Kinect) in the context of the acquisition of pedestrian skills | Parents/legal guardians were also required to complete a questionnaire to assess to what extent they considered that subjects had improved their behavior in real-life situations. | 10 sessions, each session with a maximum duration of 45 min |
| Fan, J.F., et al. [23] | 16 ASD | 13–18 all males | Driving skill training | 6 sessions, each of 60 min | |||
| Zhang, L., et al. [25] | 20 ASD | 13–18 | Non-immersive | Real-time gaze-contingent driving Simulator capable of providing individualized feedback about how drivers scan their visual environment while driving | |||
| Cox, D.J., et al. [22] | 51 ASD | 15.5–25 mostly males | A realistic driver’s cockpit with side and rear-view mirrors. | Non-immersive | Driving skill training | Driving-specific EF and general tactical assessments occurred at baseline and after 3 months of training. | 14 sessions: 12 sessions for training and 2 assessments |
| Zhang, L., et al. [24] | 20 ASD | 13–18 mostly males | Non-immersive | Driving skill training | 6 sessions, each of 60 min | ||
| Ross, V., et al. [26] | 16–25 | Semi-immersive | Driving skill training | 8–12 sessions | |||
| Fan, J., et al. [27] | 20 ASD | Mean age 15.29 years, mostly males | Driving skill training | 6 sessions, each of 60 min | |||
| Simões, M., et al. [34] | 10 ASD 10 TD | ASD Mean age 18.8 TD Mean age 21.9 years | Oculus Rift | Immersive | Teaching transportation skills | 3 sessions, 20–40 min for each session | |
| Dixon, D.R., et al. [19] | 3 ASD | 4, 6, 10 years old, mostly males | Oculus Rift headset and sensors | Immersive | Street-crossing skills | 5 sessions, each session lasted 3–5 min | |
| Bian, D., et al. [30] | 23 ASD | Mean age 15.18, 21 males and 2 females | Computer | Non-immersive | Driving skill training | ||
| BA, L.M., et al. [31] | 5 ASD | 4–8 4 males and one female | Smartphone and Google Cardboard | Immersive | Air travel skills | The fourth and final session was a real-world rehearsal | 4 sessions |
| BA, L.M., et al. [32] | 7 ASD | Mean age 18.28, 6 males and 1 female | iPhone X and Google Cardboard | Immersive | Air travel skills | 3 sessions, 20 min for each session | |
| Patrick, K.E., et al. [28] | 48 ASD 48 TD | 16–26 | Driving skill training | ||||
| Schmidt, M., et al. [33] | 5 ASD | 22–34 | Google Cardboard | Immersive | Teaching transportation skills | In the fourth stage, participants practiced skills in the real world with trained staff. | |
| Baker-Ericze’n, M.J., et al. [29] | 19 ASD | 15–29, mostly males | Driving skill training | 8 sessions, 90 min for each session | |||
| Tan, Q.P., et al. [20] | 5 ASD | 5–12 | Natural interface Kinect/keyboard/mouse/touchscreen | Semi-immersive | Street-crossing skills | ||
| Schmidt, M., et al. [35] | 6 ASD | Mean age 26.6, all males | Google Cardboard (HMD) and HTC Vive or Oculus Rift HMD | Immersive | Teaching transportation skills | 3 sessions, 60 min for each session |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, L.; Yao, X.; Chen, J.; Zhang, K.; Liu, L.; Wang, G.; Ling, Y. Virtual Reality Utilized for Safety Skills Training for Autistic Individuals: A Review. Behav. Sci. 2024, 14, 82. https://doi.org/10.3390/bs14020082
Liu L, Yao X, Chen J, Zhang K, Liu L, Wang G, Ling Y. Virtual Reality Utilized for Safety Skills Training for Autistic Individuals: A Review. Behavioral Sciences. 2024; 14(2):82. https://doi.org/10.3390/bs14020082
Chicago/Turabian StyleLiu, Lili, Xinyu Yao, Jingying Chen, Kun Zhang, Leyuan Liu, Guangshuai Wang, and Yutao Ling. 2024. "Virtual Reality Utilized for Safety Skills Training for Autistic Individuals: A Review" Behavioral Sciences 14, no. 2: 82. https://doi.org/10.3390/bs14020082
APA StyleLiu, L., Yao, X., Chen, J., Zhang, K., Liu, L., Wang, G., & Ling, Y. (2024). Virtual Reality Utilized for Safety Skills Training for Autistic Individuals: A Review. Behavioral Sciences, 14(2), 82. https://doi.org/10.3390/bs14020082