
Latent Profile Analysis of Suicidal Ideation in Chinese Individuals with Bipolar Disorder


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Psychometric Tools
2.2.1. Screener: M.I.N.I.
2.2.2. Profile Indicator 1: HAMD-24
2.2.3. Profile Indicator 2: YMRS
2.2.4. Outcome: BSSI
2.3. Statistical Analysis
3. Results
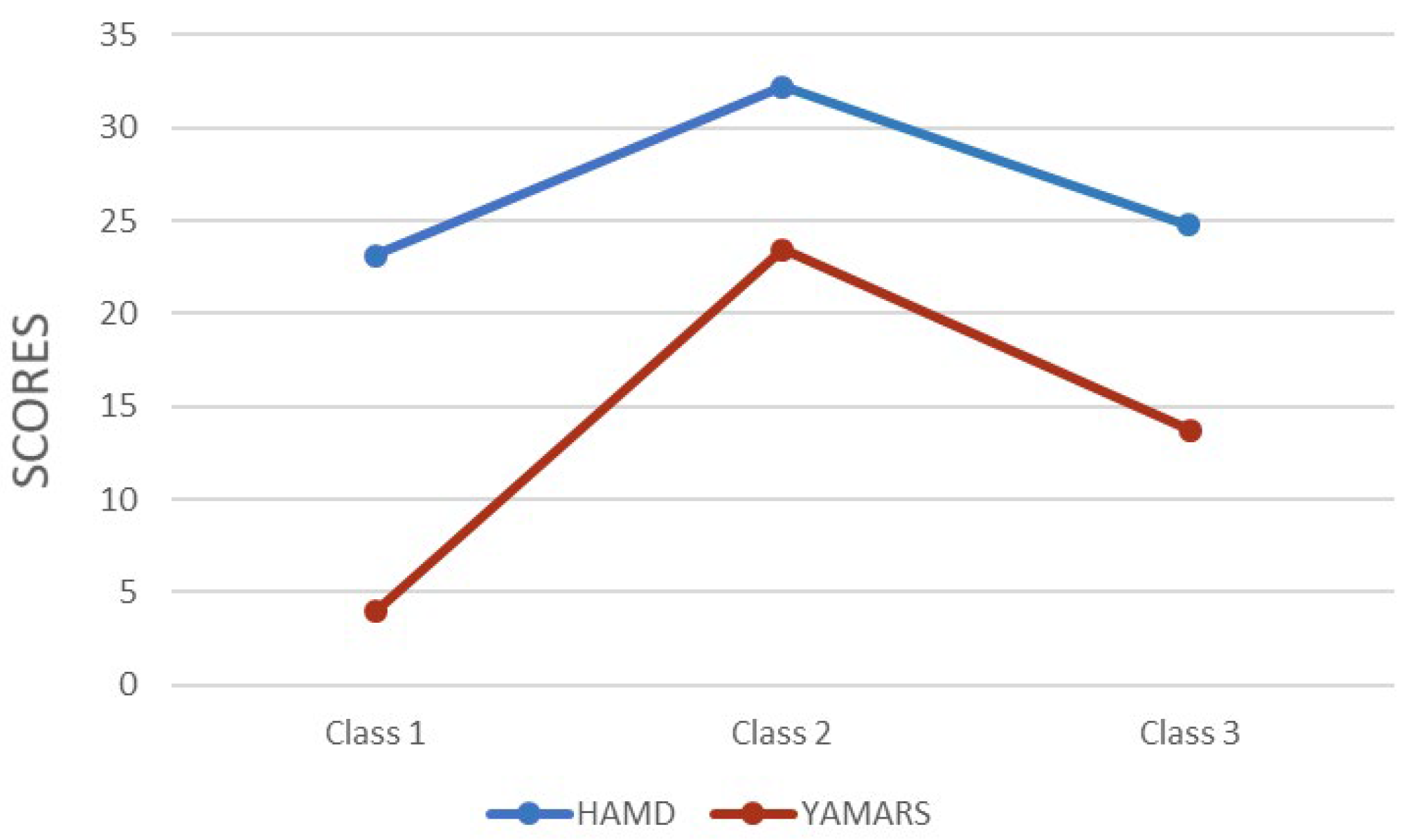
3.1. Latent Profile Analysis: Number of Divided Classes
3.2. Demographic and Clinical Profiles
3.3. Clinical Details of the Three Classes
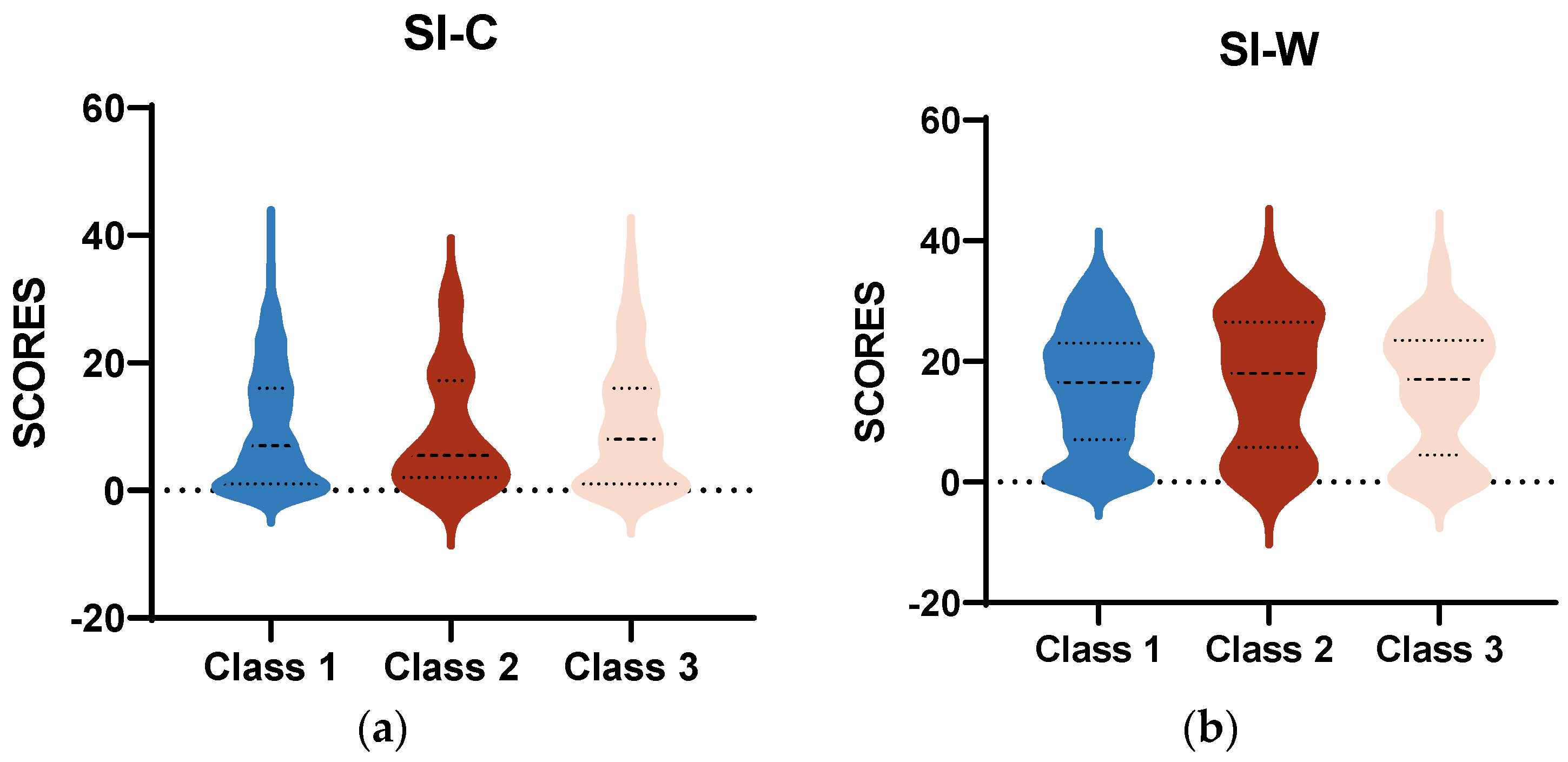
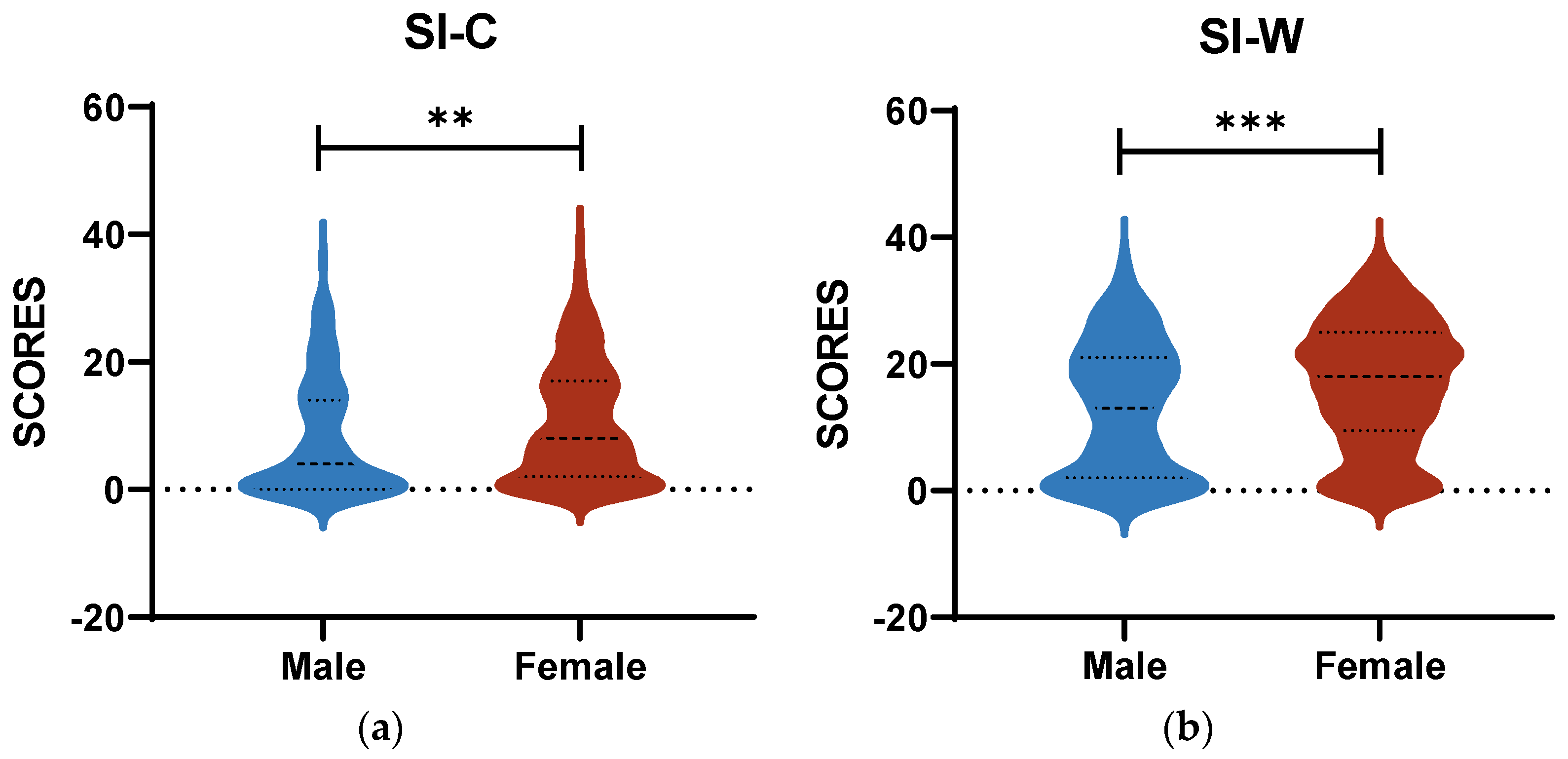
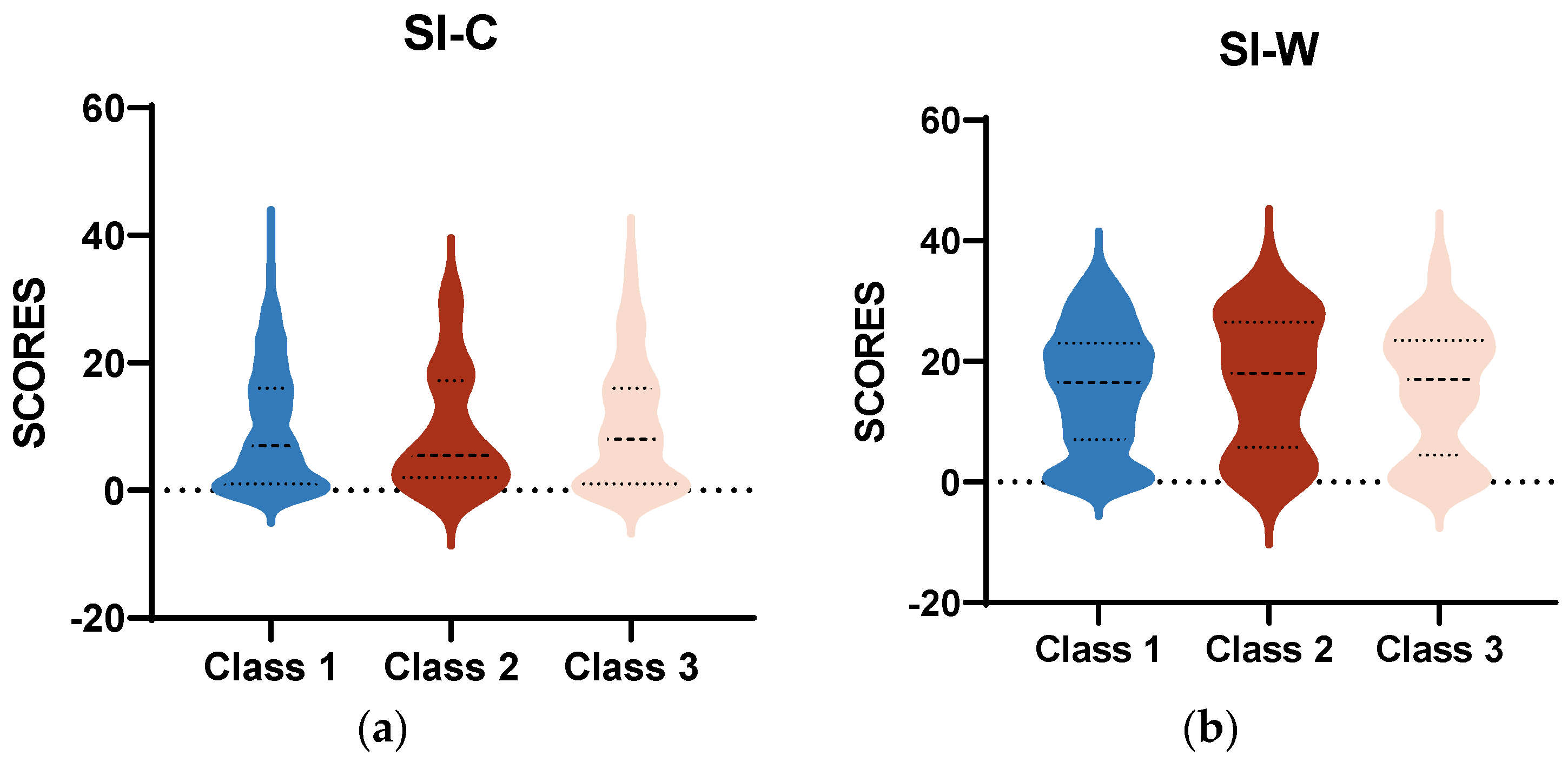
3.4. Contrasts in SI among the Three Classes
4. Discussion
4.1. The Association between Suicide Risk and Different Classes
4.2. Clinical Significance
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, J.K.N.; Tong, C.H.Y.; Wong, C.S.M.; Chen, E.Y.H.; Chang, W.C. Life expectancy and years of potential life lost in bipolar disorder: Systematic review and meta-analysis. Br. J. Psychiatry 2022, 221, 567–576. [Google Scholar] [CrossRef]
- Pan, Y.J.; Yeh, L.L.; Chan, H.Y.; Chang, C.K. Excess mortality and shortened life expectancy in people with major mental illnesses in Taiwan. Epidemiol. Psychiatr. Sci. 2020, 29, e156. [Google Scholar] [CrossRef]
- Chan, J.K.N.; Wong, C.S.M.; Yung, N.C.L.; Chen, E.Y.H.; Chang, W.C. Excess mortality and life-years lost in people with bipolar disorder: An 11-year population-based cohort study. Epidemiol. Psychiatry Sci. 2021, 30, e39. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Lu, L.; Zhang, L.; Zhang, Q.; Ungvari, G.S.; Ng, C.H.; Yuan, Z.; Xiang, Y.; Wang, G.; Xiang, Y.T. Prevalence of suicide attempts in bipolar disorder: A systematic review and meta-analysis of observational studies. Epidemiol. Psychiatry Sci. 2019, 29, e63. [Google Scholar] [CrossRef]
- Biazus, T.B.; Beraldi, G.H.; Tokeshi, L.; Rotenberg, L.D.S.; Dragioti, E.; Carvalho, A.F.; Solmi, M.; Lafer, B. All-cause and cause-specific mortality among people with bipolar disorder: A large-scale systematic review and meta-analysis. Mol. Psychiatry 2023, 28, 2508–2524. [Google Scholar] [CrossRef]
- Jayatilleke, N.; Hayes, R.D.; Dutta, R.; Shetty, H.; Hotopf, M.; Chang, C.K.; Stewart, R. Contributions of specific causes of death to lost life expectancy in severe mental illness. Eur. Psychiatry J. Assoc. Eur. Psychiatry 2017, 43, 109–115. [Google Scholar] [CrossRef]
- Plans, L.; Barrot, C.; Nieto, E.; Rios, J.; Schulze, T.G.; Papiol, S.; Mitjans, M.; Vieta, E.; Benabarre, A. Association between completed suicide and bipolar disorder: A systematic review of the literature. J. Affect Disord. 2019, 242, 111–122. [Google Scholar] [CrossRef]
- Valtonen, H.M.; Suominen, K.; Haukka, J.; Mantere, O.; Leppämäki, S.; Arvilommi, P.; Isometsä, E.T. Differences in incidence of suicide attempts during phases of bipolar I and II disorders. Bipolar. Disord. 2008, 10, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Nierenberg, A.A.; Agustini, B.; Köhler-Forsberg, O.; Cusin, C.; Katz, D.; Sylvia, L.G.; Peters, A.; Berk, M. Diagnosis and Treatment of Bipolar Disorder: A Review. JAMA 2023, 330, 1370–1380. [Google Scholar] [CrossRef]
- Xu, Y.E.; Barron, D.A.; Sudol, K.; Zisook, S.; Oquendo, M.A. Suicidal behavior across a broad range of psychiatric disorders. Mol. Psychiatry 2023, 28, 2764–2810. [Google Scholar] [CrossRef]
- Zandi, P.P.; Wang, Y.H.; Patel, P.D.; Katzelnick, D.; Turvey, C.L.; Wright, J.H.; Ajilore, O.; Coryell, W.; Schneck, C.D.; Guille, C.; et al. Development of the National Network of Depression Centers Mood Outcomes Program: A Multisite Platform for Measurement-Based Care. Psychiatry Serv. 2020, 71, 456–464. [Google Scholar] [CrossRef]
- Holma, K.M.; Haukka, J.; Suominen, K.; Valtonen, H.M.; Mantere, O.; Melartin, T.K.; Sokero, T.P.; Oquendo, M.A.; Isometsä, E.T. Differences in incidence of suicide attempts between bipolar I and II disorders and major depressive disorder. Bipolar. Disord. 2014, 16, 652–661. [Google Scholar] [CrossRef]
- Tietbohl-Santos, B.; Chiamenti, P.; Librenza-Garcia, D.; Cassidy, R.; Zimerman, A.; Manfro, G.G.; Kapczinski, F.; Passos, I.C. Risk factors for suicidality in patients with panic disorder: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2019, 105, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Swann, A.C.; Lafer, B.; Perugi, G.; Frye, M.A.; Bauer, M.; Bahk, W.M.; Scott, J.; Ha, K.; Suppes, T. Bipolar mixed states: An international society for bipolar disorders task force report of symptom structure, course of illness, and diagnosis. Am. J. Psychiatry 2013, 170, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Valtonen, H.M.; Suominen, K.; Mantere, O.; Leppämäki, S.; Arvilommi, P.; Isometsä, E. Suicidal behaviour during different phases of bipolar disorder. J. Affect Disord. 2007, 97, 101–107. [Google Scholar] [CrossRef]
- Benazzi, F. Bipolar disorder—Focus on bipolar II disorder and mixed depression. Lancet 2007, 369, 935–945. [Google Scholar] [CrossRef] [PubMed]
- Baldessarini, R.J.; Undurraga, J.; Vázquez, G.H.; Tondo, L.; Salvatore, P.; Ha, K.; Khalsa, H.M.; Lepri, B.; Ha, T.H.; Chang, J.S.; et al. Predominant recurrence polarity among 928 adult international bipolar I disorder patients. Acta Psychiatry Scand. 2012, 125, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Pallaskorpi, S.; Suominen, K.; Ketokivi, M.; Valtonen, H.; Arvilommi, P.; Mantere, O.; Leppämäki, S.; Isometsä, E. Incidence and predictors of suicide attempts in bipolar I and II disorders: A 5-year follow-up study. Bipolar. Disord. 2017, 19, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Fiedorowicz, J.G.; Persons, J.E.; Assari, S.; Ostacher, M.J.; Zandi, P.; Wang, P.W.; Thase, M.E.; Frye, M.A.; Coryell, W. Depressive symptoms carry an increased risk for suicidal ideation and behavior in bipolar disorder without any additional contribution of mixed symptoms. J. Affect Disord. 2019, 246, 775–782. [Google Scholar] [CrossRef]
- Fiedorowicz, J.G.; Persons, J.E.; Assari, S.; Ostacher, M.J.; Goes, F.S.; Nurnberger, J.I.; Coryell, W.H. Moderators of the association between depressive, manic, and mixed mood symptoms and suicidal ideation and behavior: An analysis of the National Network of Depression Centers Mood Outcomes Program. J. Affect Disord. 2021, 281, 623–630. [Google Scholar] [CrossRef]
- Hou, B.; Zhang, H. Latent profile analysis of depression among older adults living alone in China. J. Affect Disord. 2023, 325, 378–385. [Google Scholar] [CrossRef]
- Zheng, C.; Zhang, H. Latent profile analysis of depression among empty nesters in China. J. Affect Disord. 2024, 347, 541–548. [Google Scholar] [CrossRef]
- Barr, N.; Corral Rodríguez, A. Latent profile analysis of veterans’ psychological risk and protective factors: Associations with nonroutine military discharge. Psychol. Trauma Theory Res. Pract. Policy 2023, 15, 1355–1366. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The Development and Validation of a Structured Diagnostic Psychiatric Interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20). [Google Scholar]
- Korte, K.J.; Jaguga, F.; Kim, H.H.; Stroud, R.E.; Stevenson, A.; Akena, D.; Atwoli, L.; Gichuru, S.; James, R.; Kwobah, E.; et al. Psychometric properties of the mini international neuropsychiatric interview (MINI) psychosis module: A Sub-Saharan Africa cross country comparison. Psychol. Med. 2023, 53, 7042–7052. [Google Scholar] [CrossRef] [PubMed]
- Duncan, L.; Georgiades, K.; Wang, L.; Van Lieshout, R.J.; MacMillan, H.L.; Ferro, M.A.; Lipman, E.L.; Szatmari, P.; Bennett, K.; Kata, A.; et al. Psychometric evaluation of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). Psychol. Assess 2018, 30, 916–928. [Google Scholar] [CrossRef]
- Pettersson, A.; Modin, S.; Wahlström, R.; Af Winklerfelt Hammarberg, S.; Krakau, I. The Mini-International Neuropsychiatric Interview is useful and well accepted as part of the clinical assessment for depression and anxiety in primary care: A mixed-methods study. BMC Fam. Pract. 2018, 19, 19. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Carrozzino, D.; Patierno, C.; Fava, G.A.; Guidi, J. The Hamilton Rating Scales for Depression: A Critical Review of Clinimetric Properties of Different Versions. Psychother. Psychosom. 2020, 89, 133–150. [Google Scholar] [CrossRef]
- Mazure, C.; Nelson, J.C.; Price, L.H. Reliability and validity of the symptoms of major depressive illness. Arch. Gen. Psychiatry 1986, 43, 451–456. [Google Scholar] [CrossRef]
- Rabinowitz, J.; Young, R.C.; Yavorsky, C.; Williams, J.B.; Sedway, J.; Marino, P.; Matteo, C.; Mahableshwarkar, A.; Kott, A.; Hefting, N.; et al. Consistency checks to improve measurement with the Young Mania Rating Scale (YMRS). J. Affect Disord. 2024, 345, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- de Beurs, D.P.; Fokkema, M.; de Groot, M.H.; de Keijser, J.; Kerkhof, A.J.F.M. Longitudinal measurement invariance of the Beck Scale for Suicide Ideation. Psychiatry Res. 2015, 225, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Ranieri, W.F. Scale for Suicide Ideation: Psychometric properties of a self-report version. J. Clin. Psychol. 1988, 44, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.K.; Beck, A.T.; Steer, R.A.; Grisham, J.R. Risk factors for suicide in psychiatric outpatients: A 20-year prospective study. J. Consult. Clin. Psychol. 2000, 68, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Model. Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Dziak, J.J.; Coffman, D.L.; Lanza, S.T.; Li, R.; Jermiin, L.S. Sensitivity and specificity of information criteria. Brief. Bioinform. 2019, 21, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Băjenaru, L.; Balog, A.; Dobre, C.; Drăghici, R.; Prada, G.I. Latent profile analysis for quality of life in older patients. BMC Geriatr. 2022, 22, 848. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.L.; Simsek, B.; Kupfer, D.J.; Swartz, H.A.; Fagiolini, A.; Frank, E. An Approach to Revealing Clinically Relevant Subgroups Across the Mood Spectrum. J. Affect Disord. 2016, 203, 265–274. [Google Scholar] [CrossRef]
- Lim, K.; Smucny, J.; Barch, D.M.; Lam, M.; Keefe, R.S.E.; Lee, J. Cognitive Subtyping in Schizophrenia: A Latent Profile Analysis. Schizophr. Bull. 2020, 47, 712–721. [Google Scholar] [CrossRef]
- Vaillancourt-Morel, M.P.; Labadie, C.; Charbonneau-Lefebvre, V.; Sabourin, S.; Godbout, N. A latent profile analysis of romantic attachment anxiety and avoidance. J. Marital Fam. Ther. 2022, 48, 391–410. [Google Scholar] [CrossRef] [PubMed]
- Perich, T.; Hadzi-Pavlovic, D.; Frankland, A.; Breakspear, M.; Loo, C.; Roberts, G.; Holmes-Preston, E.; Mitchell, P.B. Are there subtypes of bipolar depression? Acta Psychiatr. Scand. 2016, 134, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Au, J.S.; Martinez de Andino, A.; Mekawi, Y.; Silverstein, M.W.; Lamis, D.A. Latent class analysis of bipolar disorder symptoms and suicidal ideation and behaviors. Bipolar. Disord. 2021, 23, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Kliem, S.; Lohmann, A.; Mößle, T.; Brähler, E. German Beck Scale for Suicide Ideation (BSS): Psychometric properties from a representative population survey. BMC Psychiatry 2017, 17, 389. [Google Scholar] [CrossRef]
- Wu, R.; Zhu, H.; Wang, Z.J.; Jiang, C.L. A Large Sample Survey of Suicide Risk among University Students in China. BMC Psychiatry 2021, 21, 474. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, I.; Everaert, J.; Dainer-Best, J.; Loeys, T.; Beevers, C.G.; Koster, E.H.W. Specificity and overlap of attention and memory biases in depression. J. Affect Disord. 2018, 225, 404–412. [Google Scholar] [CrossRef]
- Dillon, D.G.; Pizzagalli, D.A. Mechanisms of Memory Disruption in Depression. Trends Neurosci. 2018, 41, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Watkins, H.B.; Meyer, T.D. Is there an empirical link between impulsivity and suicidality in bipolar disorders? A review of the current literature and the potential psychological implications of the relationship. Bipolar. Disord. 2013, 15, 542–558. [Google Scholar] [CrossRef]
- Najt, P.; Perez, J.; Sanches, M.; Peluso, M.A.M.; Glahn, D.; Soares, J.C. Impulsivity and bipolar disorder. Eur. Neuropsychopharmacol. 2007, 17, 313–320. [Google Scholar] [CrossRef]
- da Silva Costa, L.; Alencar, Á.P.; Neto, P.J.N.; dos Santos, M.D.S.V.; da Silva, C.G.L.; Pinheiro, S.D.F.L.; Silveira, R.T.; Bianco, B.A.V.; Júnior, R.F.F.P.; de Lima, M.A.P.; et al. Risk factors for suicide in bipolar disorder: A systematic review. J. Affect Disord. 2015, 170, 237–254. [Google Scholar] [CrossRef]
- Simon, G.E.; Hunkeler, E.; Fireman, B.; Lee, J.Y.; Savarino, J. Risk of suicide attempt and suicide death in patients treated for bipolar disorder1. Bipolar. Disord. 2007, 9, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Sanches, M.; Nguyen, L.K.; Chung, T.H.; Nestadt, P.; Wilcox, H.C.; Coryell, W.H.; Soares, J.C.; Selvaraj, S. Anxiety Symptoms and Suicidal Thoughts and Behaviors Among Patients with Mood Disorders. J. Affect Disord. 2022, 307, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.N.; Black, D.W. Bipolar Disorder and Suicide: A Review. Curr. Psychiatry Rep. 2020, 22, 6. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; Bauer, M.S. Excess Mortality in Bipolar Disorders. Curr. Psychiatry Rep. 2014, 16, 499. [Google Scholar] [CrossRef] [PubMed]
- Grunebaum, M.F.; Keilp, J.; Li, S.; Ellis, S.P.; Burke, A.K.; Oquendo, M.A.; Mann, J.J. Symptom components of standard depression scales and past suicidal behavior. J. Affect Disord. 2005, 87, 73–82. [Google Scholar] [CrossRef]
- Dziak, J.J.; Lanza, S.T.; Tan, X. Effect Size, Statistical Power, and Sample Size Requirements for the Bootstrap Likelihood Ratio Test in Latent Class Analysis. Struct. Equ Model Multidiscip. J. 2014, 21, 534–552. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Model | Log-Likelihood | AIC | BIC | aBIC | Entropy | Smallest Class% | LMR p-Value | BLRT p-Value |
|---|---|---|---|---|---|---|---|---|
| 1 | −3581.24 | 7170.49 | 7187.48 | 7174.78 | ||||
| 2 | −3510.09 | 7034.18 | 7063.91 | 7041.69 | 0.86 | 17.02 | 0.0033 | <0.0001 |
| 3 | −3479.10 | 6978.20 | 7020.68 | 6988.94 | 0.88 | 5.80 | 0.0034 | <0.0001 |
| 4 | −3474.28 | 6974.57 | 7029.79 | 6988.53 | 0.70 | 5.80 | 0.3551 | 0.1111 |
| 5 | −3462.37 | 6956.73 | 7024.70 | 6973.92 | 0.75 | 1.55 | 0.0333 | 0.0128 |
| 6 | −3456.43 | 6950.86 | 7031.58 | 6971.27 | 0.79 | 1.74 | 0.8293 | 1.0000 |
| Characteristics | Class 1 | Class 2 | Class 3 | Total | p Value |
|---|---|---|---|---|---|
| Sample size | 382 (73.89%) | 30 (5.80%) | 105 (20.31%) | 517 | |
| Age (year) | 21.76 ± 7.31 | 23.17 ± 7.71 | 23.04 ± 8.58 | 22.10 ± 7.61 | 0.232 |
| Gender | 0.125 | ||||
| Female | 266 (51.45%) | 23 (4.45%) | 64 (12.38%) | 354 (68.47%) | |
| Male | 116 (22.44%) | 7 (1.35%) | 41 (7.93%) | 163 (31.53%) | |
| Height (cm) | 166.32 ± 8.37 | 165.8 ± 7.95 | 166.69 ± 9.06 | 166.37 ± 8.48 | 0.864 |
| Weight (kg) | 59.76 ± 13.47 | 58.73 ± 13.75 | 61.03 ± 13.64 | 59.95 ± 13.50 | 0.619 |
| Marriage | 0.233 | ||||
| Yes | 58 (11.22%) | 3 (0.58%) | 19 (3.68%) | 80 (15.47%) | |
| No | 324 (62.67%) | 27 (5.22%) | 86 (16.63%) | 422 (81.62%) | |
| Education (year) | 12.59 ± 3.34 | 14.07 ± 4.37 | 12.75 ± 3.37 | 12.71 ± 3.42 | 0.080 |
| Family history | 0.194 | ||||
| Yes | 56 (10.83%) | 4 (0.77%) | 23 (4.25%) | 83 (16.05%) | |
| No | 326 (63.06%) | 26 (5.03%) | 82 (15.86%) | 434 (83.95%) | |
| First episode | 0.681 | ||||
| Depression | 251 (48.55%) | 16 (3.09%) | 57 (11.03%) | 324 (62.67%) | |
| Mania/hypomania | 22 (4.26%) | 1 (0.19%) | 4 (0.77%) | 27 (5.22%) | |
| Unknown | 109 (21.08%) | 13 (2.51%) | 44 (8.51%) | 166 (32.11%) | |
| Disease course (year) | 4.41 ± 4.69 | 4.83 ± 4.20 | 4.21 ± 4.09 | 4.39 ± 4.55 | 0.818 |
| Source | Dependent Variable | Type III Sum of Squares | df | Mean Square | F | p Value |
|---|---|---|---|---|---|---|
| Corrected Model | SI-C | 589.283 | 5 | 117.857 | 1.482 | 0.194 |
| SI-W | 1006.027 | 5 | 201.205 | 2.123 | 0.062 | |
| Intercept | SI-C | 147.791 | 1 | 147.791 | 1.859 | 0.173 |
| SI-W | 1243.187 | 1 | 1243.187 | 13.115 | 0 | |
| Class | SI-C | 227.435 | 2 | 113.718 | 1.43 | 0.24 |
| SI-W | 50.579 | 2 | 25.29 | 0.267 | 0.766 | |
| Gender | SI-C | 451.181 | 1 | 451.181 | 5.674 | 0.018 |
| SI-W | 455.674 | 1 | 455.674 | 4.807 | 0.029 | |
| Class × Gender | SI-C | 194.033 | 2 | 97.017 | 1.22 | 0.296 |
| SI-W | 53.939 | 2 | 26.97 | 0.285 | 0.753 | |
| Error | SI-C | 38,644.39 | 486 | 79.515 | ||
| SI-W | 46,068.37 | 486 | 94.791 | |||
| Total | SI-C | 86,454 | 492 | |||
| SI-W | 179,147 | 492 | ||||
| Corrected Total | SI-C | 39,233.68 | 491 | |||
| SI-W | 47,074.4 | 491 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, Y.; Wang, H.; Geng, Y.; Lai, J.; Hu, S. Latent Profile Analysis of Suicidal Ideation in Chinese Individuals with Bipolar Disorder. Behav. Sci. 2024, 14, 360. https://doi.org/10.3390/bs14050360
Pan Y, Wang H, Geng Y, Lai J, Hu S. Latent Profile Analysis of Suicidal Ideation in Chinese Individuals with Bipolar Disorder. Behavioral Sciences. 2024; 14(5):360. https://doi.org/10.3390/bs14050360
Chicago/Turabian StylePan, Yanmeng, Huaizhi Wang, Yimeng Geng, Jianbo Lai, and Shaohua Hu. 2024. "Latent Profile Analysis of Suicidal Ideation in Chinese Individuals with Bipolar Disorder" Behavioral Sciences 14, no. 5: 360. https://doi.org/10.3390/bs14050360
APA StylePan, Y., Wang, H., Geng, Y., Lai, J., & Hu, S. (2024). Latent Profile Analysis of Suicidal Ideation in Chinese Individuals with Bipolar Disorder. Behavioral Sciences, 14(5), 360. https://doi.org/10.3390/bs14050360