
Effects of Practicing Closed- vs. Open-Skill Exercises on Executive Functions in Individuals with Attention Deficit Hyperactivity Disorder (ADHD)—A Meta-Analysis and Systematic Review


Abstract
1. Introduction
2. Methods
2.1. Retrieval Strategy
2.2. Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria
- Patients or population: people with ADHD who have been diagnosed by a doctor or who meet the criteria of the International Classification of Diseases (ICD), the Chinese Classification of Mental Disorders (CCMD), and the National Diagnostic and Manual of Mental Disorders (DSM).
- Type of intervention: acute or prolonged closed- or open-skill exercise interventions of moderate or higher intensity with a defined exercise program.
- Type of contrast: ADHD patients who are controlled by physical activity, with baseline values consistent with the experimental group.
- Type of outcomes: reporting outcome measures for neurocognitive tasks using executive function (EF) (i.e., Stroop test, N-Back task, and odd–even size test, etc.)
- Type of studies: RCT (Randomized control trial) or NRS (Non-randomized studies).
2.2.2. Exclusion Criteria
- Patient has co-morbidities or an abnormal IQ, i.e., IQ below 80.
- Studies applying other combined interventions (e.g., exercise plus nutrition program, use of electronics for exercise).
- Based on observational studies (i.e., cross-sectional studies, qualitative studies, letters, news reports, guidelines, conference abstracts, dissertations, etc.).
- Full text was not available, or data could be extracted for studies without available data, and studies lacked pre-test or post-test data.
2.3. Data Extraction and Classification
2.3.1. Data Extraction
2.3.2. Classification
2.4. Quality Assessment
2.5. Meta-Analysis
2.6. Moderator Analysis
3. Results
3.1. Literature Selection Results
3.2. Eligible Research Features
3.3. Methodological Quality Evaluation
3.4. Meta-Analysis Results
3.4.1. Closed Skill Types
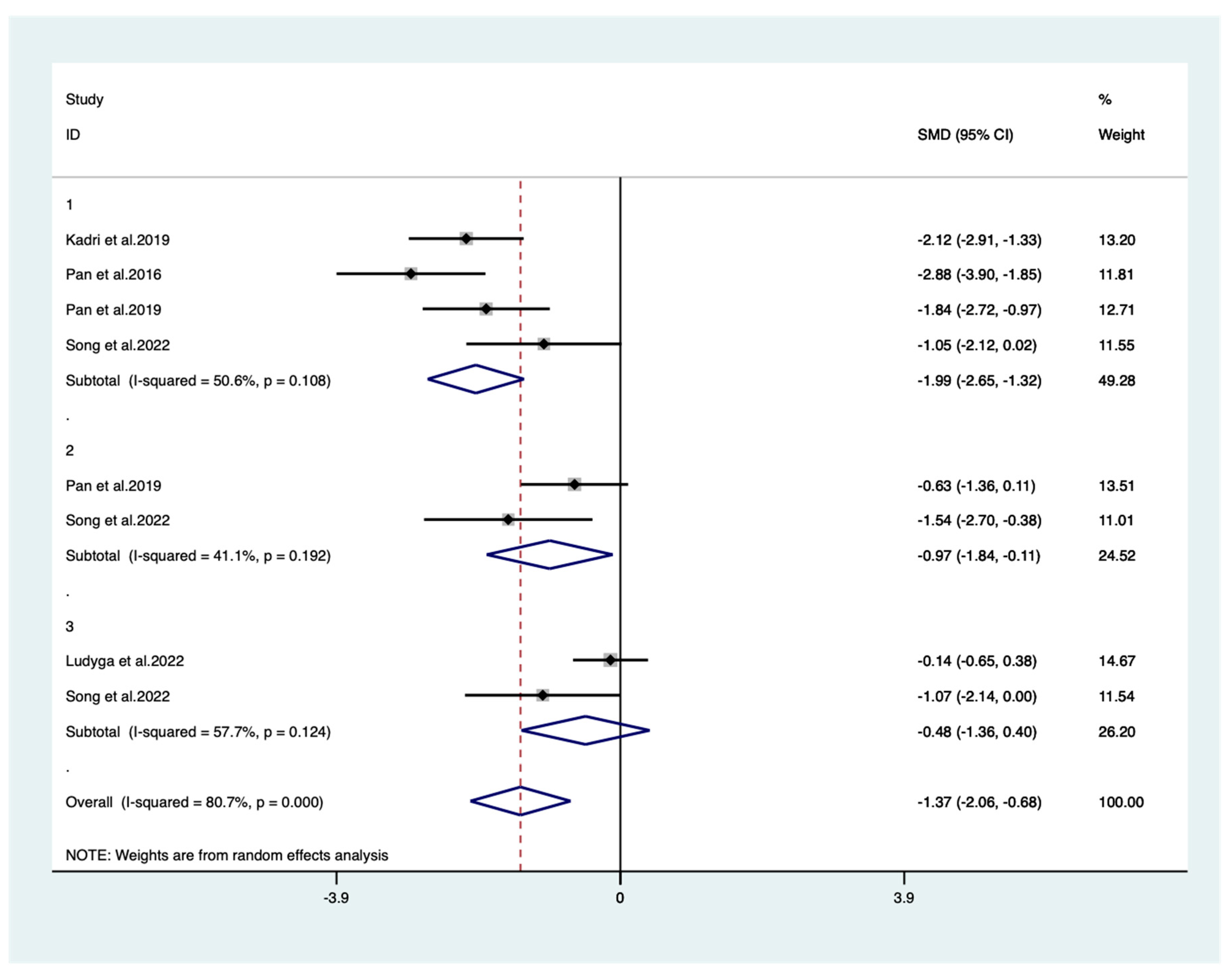
3.4.2. Open Skill Types
3.5. Moderation Effect Analysis
3.6. Sensitivity Analysis
3.7. Tests for Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Web of Science Search Strategy

| Search | Query | Total |
|---|---|---|
| #1 | class = “history-span” > (TS = (Exercise OR Exercises OR Physical Activity OR Activities, Physical OR Activity, Physical OR Physical Activities OR Exercise, Physical OR Exercises, Physical OR Physical Exercise OR Physical Exercises OR Acute Exercise OR Acute Exercises OR Exercise, Acute OR Exercises, Acute OR Exercise, Isometric OR Exercises, Isometric OR Isometric Exercises OR Isometric Exercise OR Exercise, Aerobic OR Aerobic Exercise OR Aerobic Exercises OR Exercises, Aerobic OR Exercise Training OR Exercise Trainings OR Training, Exercise OR Trainings, Exercise) | 878,324 |
| #2 | class = “history-span” > (TS = (Executive Function OR Inhibition, Psychological OR Multitasking Behavior OR Memory, Short-Term OR Executive Functions OR Function, Executive OR Functions, Executive OR Executive Control OR Executive Controls OR Inhibitions, Psychological OR Psychological Inhibitions OR Psychological Inhibition OR Inhibition, Psychology OR Inhibitions, Psychology OR Psychology Inhibition OR Psychology Inhibitions OR Inhibition Psychology OR Inhibitions Psychology OR Behavior, Multitasking OR Behaviors, Multitasking OR Multitasking Behaviors OR Multi-Tasking Behavior OR Behavior, Multi-Tasking OR Behaviors, Multi-Tasking OR Multi-Tasking Behavior OR Multi-Tasking Behaviors OR task switching OR cognitive flexibility OR Memories, Short-Term OR Memory, Short Term OR Short-Term Memories OR Short-Term Memory OR Memory, Short-term OR Memories, Short term OR Short term Memories OR Short-term Memory OR Working Memory OR Working Memories OR Memory, Immediate OR Immediate Memories OR Immediate Memory OR Memories, Immediate OR Immediate Recall OR Immediate Recalls OR Recall, Immediate OR Recalls, Immediate)) | 330,605 |
| #3 | class = “history-span” > TS = (Attention Deficit Disorder with Hyperactivity OR Attention Deficit Disorders with Hyperactivity OR ADHD OR Attention Deficit Hyperactivity Disorder OR Hyperkinetic Syndrome OR Syndromes, Hyperkinetic OR Attention Deficit-Hyperactivity Disorder OR Attention Deficit-Hyperactivity Disorders OR Deficit-Hyperactivity Disorder, Attention OR Deficit-Hyperactivity Disorders, Attention OR Disorder, Attention Deficit-Hyperactivity OR Disorders, Attention Deficit-Hyperactivity OR adds OR Attention Deficit Hyperactivity Disorders OR Attention Deficit Disorder OR Attention Deficit Disorders OR Deficit Disorder, Attention OR Deficit Disorders, Attention OR Disorder, Attention Deficit OR Disorders, Attention Deficit OR Brain Dysfunction, Minimal OR Dysfunction, Minimal Brain OR Minimal Brain Dysfunction) | 1,223,786 |
| #4 | class = “history-span” > (#1 AND #2 AND #3) class = “history-span” > LANGUAGE:(English AND Chinese) Indexes = Web of Science Core Collection | 598 |
Appendix B. Open- and Closed-Skill Classification Methods
| Classification | Closed Skills | Open Skills |
|---|---|---|
| Environmental factors | Stable | Dynamic |
| and predictable | and unpredictable | |
| Movement control | Pre-plannable | According to environmental changes |
| Feedback information | Proprioceptor | Multiple sensory receptors |
| Typical movement | Swimming; running; weightlifting | Table tennis; judo; taekwondo |
Appendix C. Sensitivity Analysis of Meta-Analysis

Appendix D. Publication Bias Analysis in Meta-Analysis—Funnel Plot

References
- Nuckols, C.C.; Nuckols, C.C. The Diagnostic and Statistical Manual of Mental Disorders, (DSM-5); American Psychiatric Association: Philadelphia, PA, USA, 2013. [Google Scholar]
- Conejero, I.; Jaussent, I.; Lopez, R.; Guillaume, S.; Olié, E.; Hebbache, C.; Cohen, R.F.; Kahn, J.P.; Leboyer, M.; Courtet, P.; et al. Association of symptoms of attention deficit-hyperactivity disorder and impulsive-aggression with severity of suicidal behavior in adult attempters. Sci. Rep. 2019, 9, 4593. [Google Scholar] [CrossRef]
- Ren, Y.; Fang, X.; Fang, H.; Pang, G.; Cai, J.; Wang, S.; Ke, X. Predicting the Adult Clinical and Academic Outcomes in Boys with ADHD: A 7- to 10-Year Follow-Up Study in China. Front. Pediatr. 2021, 9, 634633. [Google Scholar] [CrossRef]
- Faraone, S.V.; Biederman, J. What is the prevalence of adult ADHD? Results of a population screen of 966 adults. J. Atten. Disord. 2005, 9, 384–391. [Google Scholar] [CrossRef]
- Polanczyk, G.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef]
- Wang, T.; Liu, K.; Li, Z.; Xu, Y.; Liu, Y.; Shi, W.; Chen, L. Prevalence of attention deficit/hyperactivity disorder among children and adolescents in China: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 32. [Google Scholar] [CrossRef]
- Walitza, S.; Romanos, M.; Greenhill, L.; Banaschewski, T. Attention-deficit/hyperactivity disorders. In Psychiatric Drugs in Children and Adolescents: Basic Pharmacology and Practical Applications; Springer: Vienna, Austria, 2014; pp. 369–381. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.J.; Brandeis, D.; Cortese, S.; Daley, D.; Ferrin, M.; Holtmann, M.; Stevenson, J.; Danckaerts, M.; van der Oord, S.; Döpfner, M.; et al. Nonpharmacological interventions for ADHD: Systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. Am. J. Psychiatry 2013, 170, 275–289. [Google Scholar] [CrossRef]
- Cortese, S.; Kelly, C.; Chabernaud, C.; Proal, E.; Di Martino, A.; Milham, M.P.; Castellanos, F.X. Toward systems neuroscience of ADHD: A meta-analysis of 55 fMRI studies. Am. J. Psychiatry 2012, 169, 1038–1055. [Google Scholar] [CrossRef]
- Faraone, S.V.; Asherson, P.; Banaschewski, T.; Biederman, J.; Buitelaar, J.K.; Ramos-Quiroga, J.A.; Rohde, L.A.; Sonuga-Barke, E.J.; Tannock, R.; Franke, B. Attention-deficit/hyperactivity disorder. Nat. Rev. Dis. Primers 2015, 1, 15020. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef]
- Dawson, P.; Guare, R. Executive Skills in Children and Adolescents: A Practical Guide to Assessment and Intervention; Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- Sonuga-Barke, E.J.S. Causal Models of Attention-Deficit/Hyperactivity Disorder: From Common Simple Deficits to Multiple Developmental Pathways. Biol. Psychiatry 2005, 57, 1231–1238. [Google Scholar] [CrossRef]
- Cotman, C.W.; Berchtold, N.C. Exercise: A behavioral intervention to enhance brain health and plasticity. Trends Neurosci. 2002, 25, 295–301. [Google Scholar] [CrossRef]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Voss, M.W.; Vivar, C.; Kramer, A.F.; van Praag, H. Bridging animal and human models of exercise-induced brain plasticity. Trends Cogn. Sci. 2013, 17, 525–544. [Google Scholar] [CrossRef]
- Buck, S.M.; Hillman, C.H.; Castelli, D.M. The relation of aerobic fitness to stroop task performance in preadolescent children. Med. Sci. Sports Exerc. 2008, 40, 166–172. [Google Scholar] [CrossRef]
- Gapin, J.; Etnier, J.L. The relationship between physical activity and executive function performance in children with attention-deficit hyperactivity disorder. J. Sport. Exerc. Psychol. 2010, 32, 753–763. [Google Scholar] [CrossRef]
- Pontifex, M.B.; Saliba, B.J.; Raine, L.B.; Picchietti, D.L.; Hillman, C.H. Exercise improves behavioral, neurocognitive, and scholastic performance in children with attention-deficit/hyperactivity disorder. J. Pediatr. 2013, 162, 543–551. [Google Scholar] [CrossRef]
- Liang, X.; Li, R.; Wong, S.H.S.; Sum, R.K.W.; Sit, C.H.P. The impact of exercise interventions concerning executive functions of children and adolescents with attention-deficit/hyperactive disorder: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 68. [Google Scholar] [CrossRef]
- Kluka, D.A. Motor Behavior: From Learning to Performance; Morton Pub. Co.: Englewood, CO, USA, 1999. [Google Scholar]
- Schmidt, R.A. Motor Learning and Performance, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2000. [Google Scholar]
- Huang, X.; Zhang, L.; Mao, Z. Sports Psychology, 1st ed.; East China Normal University Press: Shanghai, China, 2004. [Google Scholar]
- Formenti, D.; Trecroci, A.; Duca, M.; Cavaggioni, L.; D’Angelo, F.; Passi, A.; Longo, S.; Alberti, G. Differences in inhibitory control and motor fitness in children practicing open and closed skill sports. Sci. Rep. 2021, 11, 4033. [Google Scholar] [CrossRef]
- Gu, Q.; Zou, L.; Loprinzi, P.D.; Quan, M.; Huang, T. Effects of Open Versus Closed Skill Exercise on Cognitive Function: A Systematic Review. Front. Psychol. 2019, 10, 467457. [Google Scholar] [CrossRef]
- Feng, X.; Zhang, Z.; Jin, T.; Shi, P. Effects of open and closed skill exercise interventions on executive function in typical children: A meta-analysis. BMC Psychol. 2023, 11, 420. [Google Scholar] [CrossRef]
- Shi, P.; Tang, Y.; Zhang, Z.; Feng, X.; Li, C. Effect of Physical Exercise in Real-World Settings on Executive Function of Typical Children and Adolescents: A Systematic Review. Brain Sci. 2022, 12, 1734. [Google Scholar] [CrossRef]
- Huang, H.; Jin, Z.; He, C.; Guo, S.; Zhang, Y.; Quan, M. Chronic Exercise for Core Symptoms and Executive Functions in ADHD: A Meta-analysis. Pediatrics 2023, 151, e2022057745. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Chen, Y.L.; Sun, Y.J.; Luo, X.F. he core methods and key models in evidence-based medicine. Med. J. Peking Union Med. Coll. Hosp. 2023, 14, 1–8. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Chapter 6: Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.4; John Wiley & Sons: Chichester, UK, 2023; Available online: www.training.cochrane.org/handbook (accessed on 16 December 2023).
- Igelström, E.; Campbell, M.; Craig, P.; Katikireddi, S.V. Cochrane’s risk of bias tool for non-randomized studies (ROBINS-I) is frequently misapplied: A methodological systematic review. J. Clin. Epidemiol. 2021, 140, 22–32. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: San Diego, CA, USA, 1985. [Google Scholar]
- Chang, Y.-K.; Liu, S.; Yu, H.-H.; Lee, Y.-H. Effect of acute exercise on executive function in children with attention deficit hyperactivity disorder. Arch. Clin. Neuropsychol. 2012, 27, 225–237. [Google Scholar] [CrossRef]
- Chen, X.; Liang, G.; Li, M.; Wang, Q.; Su, M. Effects of aerobic exercise on core symptoms and executive function in children with attention deficit hyperactivity disorder. Chin. Rehabil. Theory Pract. 2022, 28, 704–709. [Google Scholar] [CrossRef]
- Fritz, K.; O’Connor, P.J. Effects of a 6 week yoga intervention on executive functioning in women screening positive for adult ADHD: A pilot study. Front. Sports Act. Living 2022, 4, 746409. [Google Scholar] [CrossRef]
- Hattabi, S.; Bouallegue, M.; Yahya, H.B.; Bouden, A. Rehabilitation of aDHD children by sport intervention: A tunisian experience réhabilitation des enfants tDaH par le sport: Une expérience tunisienne. La Tunisie Medicale 2019, 97, 874–881. [Google Scholar]
- Kadri, A.; Slimani, M.; Bragazzi, N.L.; Tod, D.; Azaiez, F. Effect of taekwondo practice on cognitive function in adolescents with attention deficit hyperactivity disorder. Int. J. Environ. Res. Public. Health 2019, 16, 204. [Google Scholar] [CrossRef]
- Kouhbanani, S.S.; Zarenezhad, S.; Arabi, S.M. Mind-body exercise affects attention switching and sustained attention in female adults with Attention Deficit/Hyperactivity Disorder: A randomized, controlled trial with 6-month follow-up. Curr. Psychol. 2023, 42, 20983–20994. [Google Scholar] [CrossRef]
- Ludyga, S.; Mücke, M.; Leuenberger, R.; Bruggisser, F.; Pühse, U.; Gerber, M.; Capone-Mori, A.; Keutler, C.; Brotzmann, M.; Weber, P. Behavioral and neurocognitive effects of judo training on working memory capacity in children with ADHD: A randomized controlled trial. NeuroImage Clin. 2022, 36, 103156. [Google Scholar] [CrossRef]
- Pan, C.-Y.; Chu, C.-H.; Tsai, C.-L.; Lo, S.-Y.; Cheng, Y.-W.; Liu, Y.-J. A racket-sport intervention improves behavioral and cognitive performance in children with attention-deficit/hyperactivity disorder. Res. Dev. Disabil. 2016, 57, 1–10. [Google Scholar] [CrossRef]
- Silva, L.A.D.; Doyenart, R.; Henrique Salvan, P.; Rodrigues, W.; Felipe Lopes, J.; Gomes, K.; Thirupathi, A.; Pinho, R.A.D.; Silveira, P.C. Swimming training improves mental health parameters, cognition and motor coordination in children with Attention Deficit Hyperactivity Disorder. Int. J. Environ. Health Res. 2020, 30, 584–592. [Google Scholar] [CrossRef]
- Song, Y.; Li, Y.; Liu, J.; Li, X.; Yin, T.; Wang, F.; Lu, S.; Chen, M.; Ren, Y. Effect of soccer practice on executive function in boys with attention deficit hyperactivity disorder. Chin. J. Sports Med. 2022, 41, 165–172. [Google Scholar] [CrossRef]
- Wu, M.M.; Wu, R.R.; Zhu, Y.Y. Observation on the improvement effect of cycling exercise training assisted by watching cartoons on children with attention deficit hyperactivity disorder. Sichuan J. Physiol. Sci. 2023, 45, 579–581. [Google Scholar]
- Chang, Y.-K.; Hung, C.-L.; Huang, C.-J.; Hatfield, B.D.; Hung, T.-M. Effects of an aquatic exercise program on inhibitory control in children with ADHD: A preliminary study. Arch. Clin. Neuropsychol. 2014, 29, 217–223. [Google Scholar] [CrossRef]
- Chou, C.-C.; Huang, C.-J. Effects of an 8-week yoga program on sustained attention and discrimination function in children with attention deficit hyperactivity disorder. PeerJ 2017, 5, e2883. [Google Scholar] [CrossRef]
- Pan, C.-Y.; Tsai, C.-L.; Chu, C.-H.; Sung, M.-C.; Huang, C.-Y.; Ma, W.-Y. Effects of physical exercise intervention on motor skills and executive functions in children with ADHD: A pilot study. J. Atten. Disord. 2019, 23, 384–397. [Google Scholar] [CrossRef]
- Heilmann, F.; Weinberg, H.; Wollny, R. The impact of practicing open-vs. closed-skill sports on executive functions—A meta-analytic and systematic review with a focus on characteristics of sports. Brain Sci. 2022, 12, 1071. [Google Scholar] [CrossRef]
- Verburgh, L.; Königs, M.; Scherder, E.J.; Oosterlaan, J. Physical exercise and executive functions in preadolescent children, adolescents and young adults: A meta-analysis. Br. J. Sports Med. 2014, 48, 973–979. [Google Scholar] [CrossRef]
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E. Physical activity, cognition, and brain outcomes: A review of the 2018 physical activity guidelines. Med. Sci. Sports Exerc. 2019, 51, 1242. [Google Scholar] [CrossRef]
- Hillman, C.H.; Castelli, D.M.; Buck, S.M. Aerobic fitness and neurocognitive function in healthy preadolescent children. Med. Sci. Sports Exerc. 2005, 37, 1967. [Google Scholar] [CrossRef]
- Chapman, S.B.; Aslan, S.; Spence, J.S.; Hart, J.J., Jr.; Bartz, E.K.; Didehbani, N.; Keebler, M.W.; Gardner, C.M.; Strain, J.F.; DeFina, L.F. Neural mechanisms of brain plasticity with complex cognitive training in healthy seniors. Cereb. Cortex 2015, 25, 396–405. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef]
- Seifert, T.; Brassard, P.; Wissenberg, M.; Rasmussen, P.; Nordby, P.; Stallknecht, B.; Adser, H.; Jakobsen, A.H.; Pilegaard, H.; Nielsen, H.B. Endurance training enhances BDNF release from the human brain. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2010, 298, R372–R377. [Google Scholar] [CrossRef]
- Hung, C.-L.; Tseng, J.-W.; Chao, H.-H.; Hung, T.-M.; Wang, H.-S. Effect of acute exercise mode on serum brain-derived neurotrophic factor (BDNF) and task switching performance. J. Clin. Med. 2018, 7, 301. [Google Scholar] [CrossRef]
- Davey, C. Physical exertion and mental performance. Ergonomics 1973, 16, 595–599. [Google Scholar] [CrossRef]
- Takahashi, S.; Grove, P.M. Impact of acute open-skill exercise on inhibitory control and brain activation: A functional near-infrared spectroscopy study. PLoS ONE 2023, 18, e0276148. [Google Scholar] [CrossRef]
- Visser, A.; Büchel, D.; Lehmann, T.; Baumeister, J. Continuous table tennis is associated with processing in frontal brain areas: An EEG approach. Exp. Brain Res. 2022, 240, 1899–1909. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, A.C.; Fink, A. Intelligence and neural efficiency. Neurosci. Biobehav. Rev. 2009, 33, 1004–1023. [Google Scholar] [CrossRef] [PubMed]
- Cabral, D.F.; Rice, J.; Morris, T.P.; Rundek, T.; Pascual-Leone, A.; Gomes-Osman, J. Exercise for brain health: An investigation into the underlying mechanisms guided by dose. Neurotherapeutics 2019, 16, 580–599. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

| Author (Year) | Country /District | Study Design | Participant Characteristics | Intervention Component | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age Range; Sex-M (%); Diagnostic Methods | Sample Size (IG/CG) | Age (Control) | ADHD Subtypes (Control) | Medication Situation (Control) | Content (Control) | Intensity | Frequency | Outcome Measures | |||
| Chang (2012) [35] | Taiwan | RCT | 8–15; M-92; DSM-IV | 40 (20/20) | 10.45 ± 0.95 (10.42 ± 0.87) | I:10, HI:2, C:8 (I:4, HI:3, C:13) | 10 (10) | Treadmill (watching videos) | Moderate (50–70%HRR) | 30 mins/ 1 session | IC: ST * CF: WCST00 |
| Chang (2014) [46] | Taiwan | NRS | 5–10; M-85; DSM-IV-TR | 27 (14/13) | 8.19 ± 7.65 (8.78 ± 8.33) | I:4, HI:2, C:8 (I:3; C:10) | 7 (6) | Aquatic exercise (control) | Moderate | 90 mins/ 2 sessions/ 8 weeks | IC: GNG * |
| Chen (2022) [36] | China | RCT | 6–10; M-82; DSM-5 | 64 (32/32) | 8.37 ± 1.68 (7.89 ± 2.13) | I:6, HI:8, C:18 (I:5; HI:10; C:17) | none | Cycling (watching videos) | Moderate (60~80%HHR) | 25 mins/ 3 sessions/ 12 weeks | IC: ST * CF: OEST * WM: N-B * |
| Chou (2017) [47] | Taiwan | NRS | 8–12; M-77; psychiatric physician | 49 (24/25) | 10.71 ± 1.00 (10.30 ± 1.07) | I:12, HI:7, C:5 (I:8; HI:13; C:4) | 10 (12) | Yoga (control) | Moderate (50~60%HHR) | 40 mins/ 2 sessions/ 8 weeks | IC: DT * |
| Fritz (2022) [37] | USA | RCT | 18–24; M-0; DMS-5 | 27 (11/16) | 20.16 ± 1.46 (20.16 ± 1.46) | NR | NR | Yoga (control) | Moderate (RPE: 10.5–19) | 180 mins/ 6 weeks | IC: FT00 CF: LSWMT00 WM: DCCST00 |
| Hattabi (2019) [38] | Tunisia | RCT | 9–12; M-87; DSM-IV | 40 (20/20) | 9.95 ± 1.31 (9.75 ± 1.33) | I:4, HI:6, C:10 (I:5; HI:4; C:11) | NR | Swimming (control) | Moderate (50–70%HRR) | 90 mins/ 3 sessions/ 12 weeks | IC: ST * |
| Kouhbanani (2023) [40] | Iran | RCT | 20–50; M-0; DSM-5 | 52 (25/27) | 35.24 ± 11.49 (35.40 ± 11.01) | I:16; C:9 (I:18; C:9) | NR | Pilates (control) | Moderate | 45 mins/ 3 sessions/ 24 weeks | CF: WCST * |
| Silva (2020) [43] | Brazil | RCT | 11–14; M-70; DSM-IV | 20 (10/10) | 12.0 ± 2.0 (12.0 ± 1.0) | NR | NR | Swimming (control) | Moderate | 45 mins/ 2 sessions/ 8 weeks | CF: TT * |
| Wu (2023) [45] | China | RCT | NR; M-66; psychiatric physician | 83 (42/41) | 9.81 ± 2.90 (9.92 ± 3.03) | I:16, HI:9, C:17 (I:14; HI:8; C:19) | NR | Cycling (watching videos) | Moderate (60%HHR) | 20 mins/ 3 sessions/ 12 weeks | IC: ST * CF: OEST * WM: N-B * |
| Characteristics of included studies (Open skill). | |||||||||||
| Kadri (2019) [39] | Tunisia | RCT | 12–18; M-90; psychiatric physician | 40 (20/20) | 14.5 ± 3.5 (14.2 ± 3.0) | NR | NR | Taekwondo (control) | Moderate | 50 mins/ 2 sessions/ 78 weeks | IC: SCWT * |
| Ludyga (2022) [41] | CH/DE | RCT | 8–12; M-70; DSM-5 | 58 (29/29) | 10.0 ± 1.2 (10.8 ± 1.2) | NR | 29 (29) | Judo (control) | Moderate (RPE: 13.3 ± 0.7) | 60 mins/ 2 sessions/ 12 weeks | WM: CDPT00 |
| Pan (2016) [42] | Taiwan | RCT | 6–12; M-100; DSM-IV | 32 (16/16) | 8.93 ± 1.49 (8.87 ± 1.56) | NR | 9 (9) | Table tennis (control) | Moderate | 70 mins/ 2 sessions/ 12 weeks | IC: SCWT * |
| Pan (2019) [48] | Taiwan | NRS | 7–12; M-100; DSM-IV | 60 (15/G1: 15, G2: 30TD) | 9.08 ± 1.43 (8.90 ± 1.66) | NR | 9 (9) | Table tennis (control) | Moderate | 70 mins/ 2 sessions/ 12 weeks | IC: SCWT * CF: WCST * |
| Song (2022) [44] | China | RCT | 6.58~8.58; M-100; DMS-IV | 24 (8/G1: 8, G2: 8TD) | 7.68 ± 0.56 (7.53 ± 0.79) | I:6, HI:0, C:2 (I:5; HI:1; C:2) | NR | Football (physical education class) | Moderate | 60 mins/ 5 sessions/ 6 weeks | IC: SCWT * CF: TMT * WM: CFT * |
| Author (Year) | Confounding | Selection of Participants | Classification of Interventions | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of Reported Results | Overall |
|---|---|---|---|---|---|---|---|---|
| Chang (2014) [46] | Moderate | Low | Low | Low | Moderate | Moderate | Moderate | Moderate |
| Chou (2017) [47] | Moderate | Low | Low | Low | Moderate | Low | Low | Moderate |
| Pan (2019) [48] | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Categories | Subgroup | Outcome Variables | Qb | p | Combined Effects Test | Heterogeneity Test | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| SMD | 95% CI | p | Qw | p | I2 (%) | |||||
| Type of skills | Closed skill Open skill | Inhibitory control | 6.263 | 0.012 * | −1.020 | −1.464, −0.578 | 0.000 | 20.573 | 0.002 | 70.8 |
| −2.042 | −2.710, −1.376 | 0.000 | 6.366 | 0.095 | 52.8 | |||||
| Cognitive flexibility | 0.256 | 0.613 | −1.384 | −2.324, −0.443 | 0.004 | 58.906 | 0.000 | 91.5 | ||
| −1.039 | −1.983, −0.095 | 0.031 | 2.042 | 0.153 | 51.0 | |||||
| Working memory | 0.440 | 0.507 | −0.865 | −1.231, −0.498 | 0.000 | 2.614 | 0.271 | 23.5 | ||
| −0.521 | −1.467, 0.425 | 0.280 | 2.735 | 0.098 | 63.4 | |||||
| Frequency | ≤2 sessions/ week >2 sessions/ week | Inhibitory control | 0.003 | 0.959 | −1.344 | −2.002, −0.685 | 0.000 | 31.676 | 0.000 | 81.0 |
| −1.367 | −1.996, −0.738 | 0.000 | 10.881 | 0.012 | 72.4 | |||||
| Cognitive flexibility | 0.117 | 0.732 | −1.171 | −2.322, −0.021 | 0.046 | 22.764 | 0.000 | 86.8 | ||
| −1.442 | −2.479, −0.404 | 0.006 | 31.360 | 0.000 | 90.4 | |||||
| Working memory | 7.082 | 0.008 ** | −0.243 | −0.673, 0.186 | 0.267 | 0.534 | 0.465 | 0.0 | ||
| −0.975 | −1.301, −0.650 | 0.000 | 1.510 | 0.470 | 0.0 | |||||
| Period | <12 weeks ≥12 weeks | Inhibitory control | 8.637 | 0.003 ** | −0.759 | −1.118, −0.400 | 0.000 | 4.768 | 0.311 | 16.1 |
| −1.833 | −2.452, −1.213 | 0.000 | 23.845 | 0.000 | 79.0 | |||||
| Cognitive flexibility | 0.094 | 0.759 | −1.475 | −2.835, −0.115 | 0.034 | 25.259 | 0.000 | 88.1 | ||
| −1.212 | −2.202, −0.223 | 0.016 | 33.554 | 0.000 | 91.0 | |||||
| Working memory | 0.005 | 0.944 | −0.712 | −1.338, −0.086 | 0.026 | 0.923 | 0.337 | 0.0 | ||
| −0.681 | −1.260, −0.103 | 0.021 | 8.201 | 0.017 | 75.6 | |||||
| Age | <18 | Executive functions | 7.031 | 0.008 ** | −1.305 | −1.676, −0.934 | 0.000 | 114.768 | 0.000 | 83.4 |
| ≥18 | −0.613 | −0.965, −0.260 | 0.001 | 1.381 | 0.710 | 0.0 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, C.; Zhai, Q.; Chen, S. Effects of Practicing Closed- vs. Open-Skill Exercises on Executive Functions in Individuals with Attention Deficit Hyperactivity Disorder (ADHD)—A Meta-Analysis and Systematic Review. Behav. Sci. 2024, 14, 499. https://doi.org/10.3390/bs14060499
Qiu C, Zhai Q, Chen S. Effects of Practicing Closed- vs. Open-Skill Exercises on Executive Functions in Individuals with Attention Deficit Hyperactivity Disorder (ADHD)—A Meta-Analysis and Systematic Review. Behavioral Sciences. 2024; 14(6):499. https://doi.org/10.3390/bs14060499
Chicago/Turabian StyleQiu, Chunyue, Qun Zhai, and Shuangru Chen. 2024. "Effects of Practicing Closed- vs. Open-Skill Exercises on Executive Functions in Individuals with Attention Deficit Hyperactivity Disorder (ADHD)—A Meta-Analysis and Systematic Review" Behavioral Sciences 14, no. 6: 499. https://doi.org/10.3390/bs14060499
APA StyleQiu, C., Zhai, Q., & Chen, S. (2024). Effects of Practicing Closed- vs. Open-Skill Exercises on Executive Functions in Individuals with Attention Deficit Hyperactivity Disorder (ADHD)—A Meta-Analysis and Systematic Review. Behavioral Sciences, 14(6), 499. https://doi.org/10.3390/bs14060499