Elevated Levels of Serum IL-17A in Community-Dwelling Women with Higher Depressive Symptoms

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
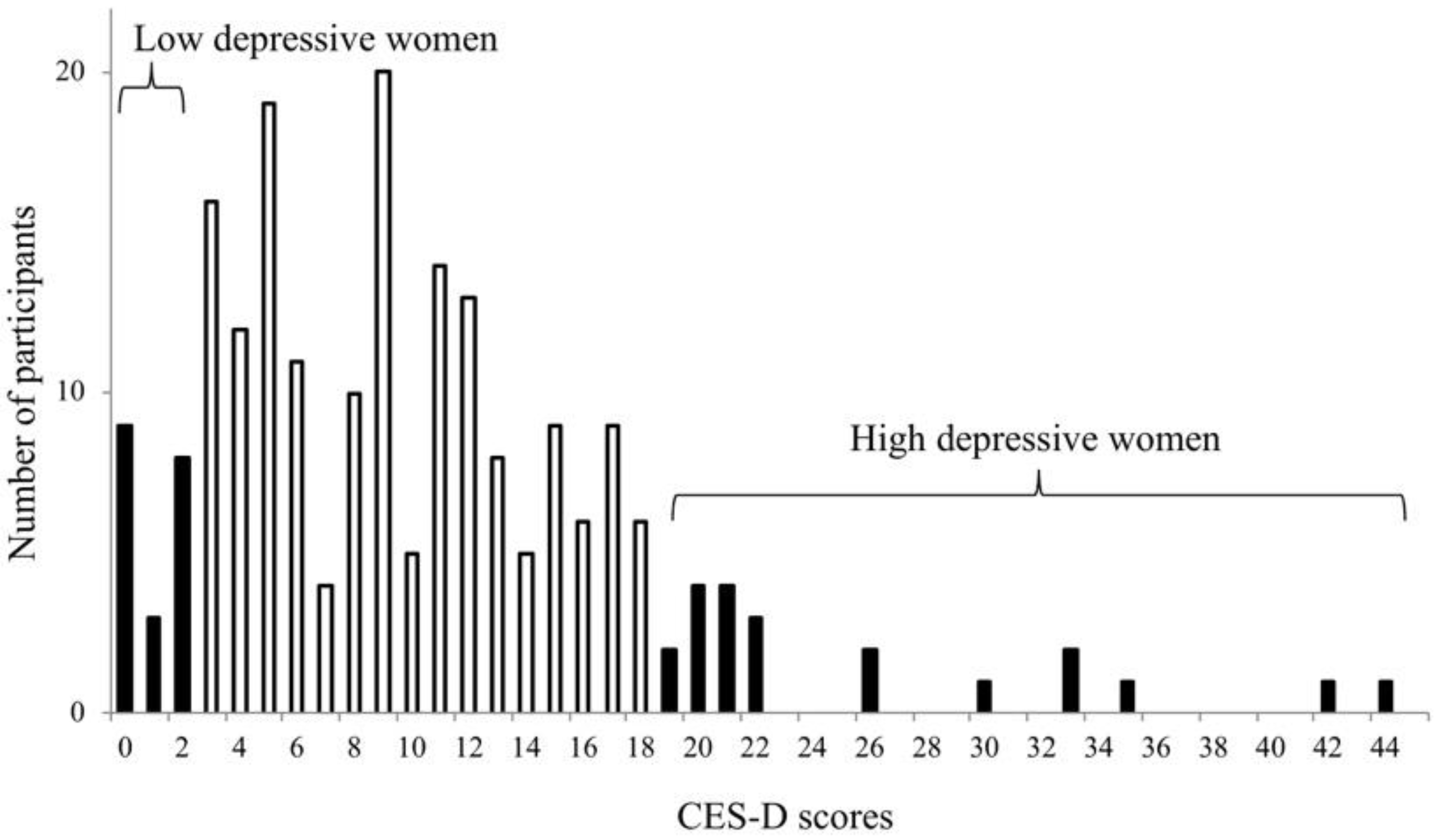
2.1. Study Population
2.2. Procedures
2.3. Blood Collection
2.4. Inflammatory Assays
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. IL-17 and Depression
4.2. IL-6 and Depression
4.3. TNF-α, IL-10, IL-12 and Depression
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rawdin, B.J.; Mellon, S.H.; Dhabhar, F.S.; Epel, E.S.; Puterman, E.; Su, Y.; Burke, H.M.; Reus, V.I.; Rosser, R.; Hamilton, S.P.; et al. Dysregulated relationship of inflammation and oxidative stress in major depression. Brain Behav. Immun. 2013, 31, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maes, M. Inflammatory and oxidative and nitrosative stress pathways underpinning chronic fatigue, somatization and psychosomatic symptoms. Curr. Opin. Psychiatry 2009, 22, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctot, K.L. A meta-analysis of cytokines in major depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Howren, M.B.; Lamkin, D.M.; Suls, J. Associations of depression with C-reactive protein, IL-1, and IL-6: A meta-analysis. Psychosom Med. 2009, 7, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Konsman, J.P.; Parnet, P.; Dantzer, R. Cytokine-induced sickness behaviour: Mechanisms and implications. Trends Neurosci. 2002, 25, 154–159. [Google Scholar] [CrossRef]
- Bufalino, C.; Hepgul, N.; Aguglia, E.; Pariante, C.M. The role of immune genes in the association between depression and inflammation: A review of recent clinical studies. Brain Behav. Immun. 2013, 31, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Park, S.E.; Dantzer, R.; Kelley, K.W.; McCusker, R.H. Central administration of insulin-like growth factor-I decreases depressive-like behavior and brain cytokine expression in mice. J. Neuroinflamm. 2011, 8, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davami, M.H.; Baharlou, R.; Ahmadi Vasmehjani, A.; Ghanizadeh, A.; Keshtkar, M.; Dezhkam, I.; Atashzar, M.R. Elevated IL-17 and TGF-beta Serum Levels: A Positive Correlation between T-helper 17 Cell-Related Pro-Inflammatory Responses with Major Depressive Disorder. Basic Clin. Neurosci. 2016, 7, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Jiang, T.; Chen, P.; Ouyang, J.; Xu, G.; Zeng, Z.; Sun, Y. Emerging tendency towards autoimmune process in major depressive patients: A novel insight from Th17 cells. Psychiatry Res. 2011, 188, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Jha, M.K.; Minhajuddin, A.; Gadad, B.S.; Greer, T.L.; Mayes, T.L.; Trivedi, M.H. Interleukin 17 selectively predicts better outcomes with bupropion-SSRI combination: Novel T cell biomarker for antidepressant medication selection. Brain Behav. Immun. 2017, 66, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Munzer, A.; Sack, U.; Mergl, R.; Schonherr, J.; Petersein, C.; Bartsch, S.; Kirkby, K.C.; Bauer, K.; Himmerich, H. Impact of antidepressants on cytokine production of depressed patients in vitro. Toxins 2013, 5, 2227–2240. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lee, H.; Lee, G.; Oh, S.J.; Shin, M.K.; Shim, I.; Bae, H. CD4+CD25+ regulatory T cell depletion modulates anxiety and depression-like behaviors in mice. PLoS ONE 2007, 7, e42054. [Google Scholar] [CrossRef] [PubMed]
- Tallerova, A.V.; Kovalenko, L.P.; Durnev, A.D.; Seredenin, S.B. Effect of antiasthenic drug ladasten on the level of cytokines and behavior in experimental model of anxious depression in C57BL/6 male mice. Eksp. Klin. Farmakol. 2011, 74, 3–5. [Google Scholar] [PubMed]
- Itoh, M.; Suganami, T.; Hachiya, R.; Ogawa, Y. Adipose tissue remodeling as homeostatic inflammation. Int. J. Inflam. 2011, 2011, 720926. [Google Scholar] [CrossRef] [PubMed]
- Athie-Morales, V.; Smits, H.H.; Cantrell, D.A.; Hilkens, C.M. Sustained IL-12 signaling is required for Th1 development. J. Immunol. (Baltimore, Md.: 1950) 2004, 172, 61–69. [Google Scholar] [CrossRef]
- Bashyam, H. Th1/Th2 cross-regulation and the discovery of IL-10. J. Exp. Med. 2007, 204, 237. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.T.; Tsujiguchi, H.; Kambayashi, Y.; Hara, A.; Miyagi, S.; Yamada, Y.; Nakamura, H.; Shimizu, Y.; Hori, D.; Suzuki, F.; et al. Relationship between Vitamin Intake and Depressive Symptoms in Elderly Japanese Individuals: Differences with Gender and Body Mass Index. Nutrients 2017, 9, 1319. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Shima, S.; Shikano, T.; Kitamura, T.; Asai, M. New self-rating scale for depression. Clin. Psychiatry 1985, 27, 717–723. [Google Scholar]
- Baumeister, D.; Ciufolini, S.; Mondelli, V. Effects of psychotropic drugs on inflammation: consequence or mediator of therapeutic effects in psychiatric treatment? Psychopharmacol 2016, 233, 1575–1589. [Google Scholar] [CrossRef] [PubMed]
- Daniele, S.; Zappelli, E.; Martini, C. Trazodone regulates neurotrophic/growth factors, mitogen-activated protein kinases and lactate release in human primary astrocytes. J. Neuroinflamm. 2015, 12, 225. [Google Scholar] [CrossRef] [PubMed]
- Covelli, V.; Passeri, M.E.; Leogrande, D.; Jirillo, E.; Amati, L. Drug targets in stress-related disorders. Curr. Med. Chem. 2005, 12, 1801–1809. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Li, L.; Meng, R.; Fan, Y.; Liu, Y.; Tao, L.; Liu, X.; Wu, C. Suppressive effect of diazepam on IFN-gamma production by human T cells. Int. Immunopharmacol. 2010, 10, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.W.; Kim, Y.K. Neuroinflammation and cytokine abnormality in major depression: Cause or consequence in that illness? World J. Psychiatry 2016, 6, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Kohler, C.A.; Freitas, T.H.; Maes, M.; de Andrade, N.Q.; Liu, C.S.; Fernandes, B.S.; Stubbs, B.; Solmi, M.; Veronese, N.; Herrmann, N.; et al. Peripheral cytokine and chemokine alterations in depression: A meta-analysis of 82 studies. Acta Psychiat. Scand. 2017, 13, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Haapakoski, R.; Mathieu, J.; Ebmeier, K.P.; Alenius, H.; Kivimaki, M. Cumulative meta-analysis of interleukins 6 and 1beta, tumour necrosis factor alpha and C-reactive protein in patients with major depressive disorder. Brain Behav. Immun. 2015, 49, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Idova, G.V.; Markova, E.V.; Gevorgyan, M.M.; Al’perina, E.L.; Zhanaeva, S.Y. Cytokine Production by Splenic Cells in C57BL/6J Mice with Depression-Like Behavior Depends on the Duration of Social Stress. Bull. Exp. Biol. Med. 2018, 164, 645–649. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | High Depressive (n = 10) | Low Depressive (n = 10) | p Value |
|---|---|---|---|
| Age | 59.7 (15.53) | 60.6 (12.8) | 0.87 |
| BMI | 21.5 (3.69) | 23.0 (3.67) | 0.37 |
| CES-D scores | 24.4 (8.1) | 0.8 (1.03) | <0.0005 |
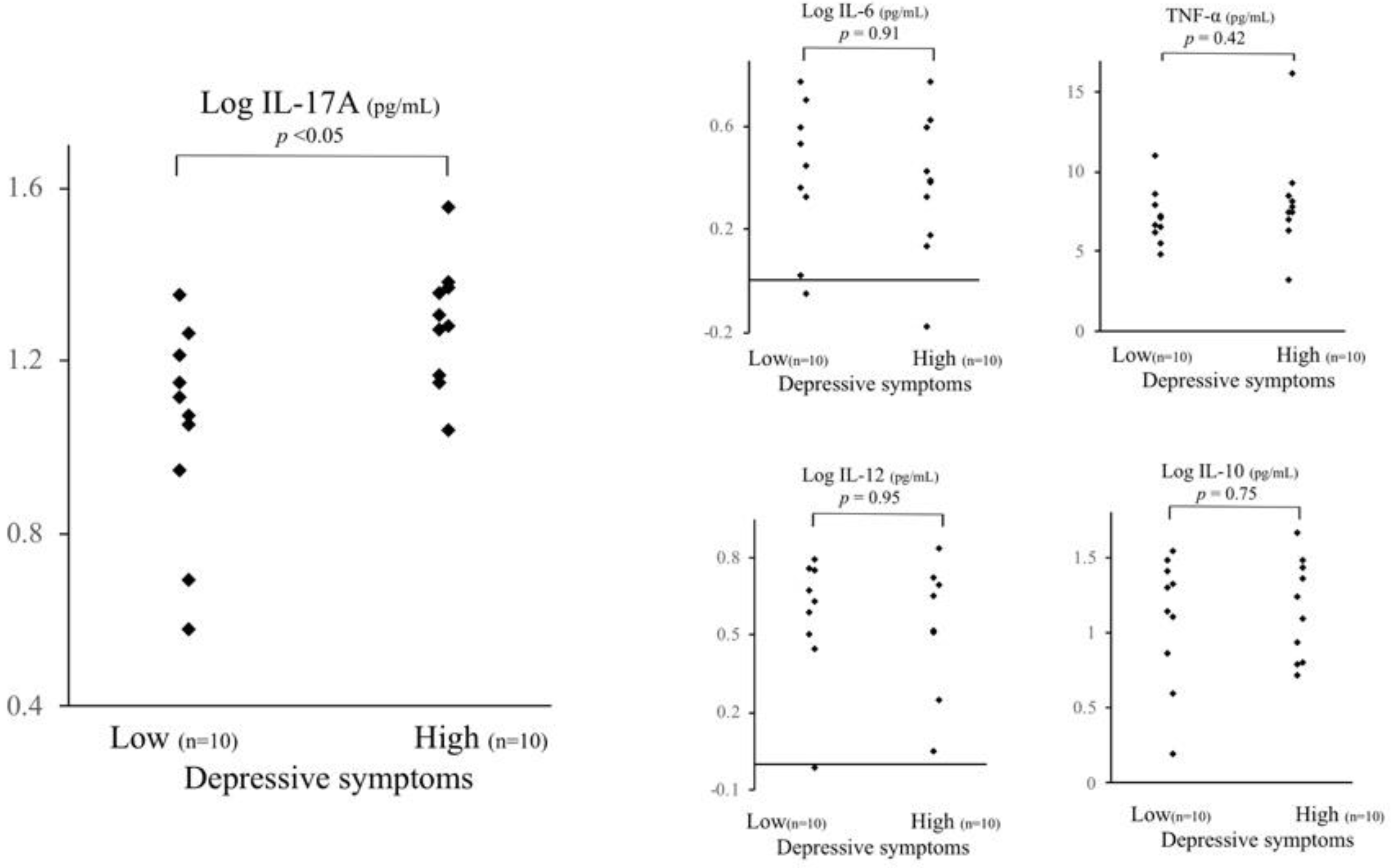
| IL-6 a (pg/mL) | 2.71 (1.555) | 2.8 (1.789) | 0.91 |
| IL-10 a (pg/mL) | 18.2 (13.27) | 17.1 (11.15) | 0.75 |
| IL-12 a (pg/mL) | 5.06 (2.982) | 4.74 (2.362) | 0.95 |
| IL-17a a (pg/mL) | 20.3 (6.93) | 12.5 (5.75) | 0.01 |
| TNF-α (pg/mL) | 8.19 (3.269) | 7.22 (1.748) | 0.42 |
| hs-CRP a (mg/dL) | 0.12 (0.238) | 0.06 (0.050) | 0.99 |
| Smoking habit | |||
| no smoker | 9 | 9 | 0.37 c |
| ex-smoker | 0 | 1 | |
| Present smoker | 1 | 0 | |
| Alcohol consumption | |||
| No habit | 7 | 8 | 0.79 c |
| Several days per week | 3 | 0 | |
| Everyday | 0 | 2 | |
| Leisure-time physical activities b | 2 | 1 | 0.50 d |
| Educational years | 11.5 (2.92) | 10.4 (1.51) | 0.31 c |
| Marital status | |||
| Married | 6 | 6 | 0.37 c |
| Single | 3 | 1 | |
| Widowed (more than three years before) | 1 | 3 | |
| Living alone | 2 | 1 | 0.50 d |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsuboi, H.; Sakakibara, H.; Minamida, Y.; Tsujiguchi, H.; Matsunaga, M.; Hara, A.; Nakamura, H. Elevated Levels of Serum IL-17A in Community-Dwelling Women with Higher Depressive Symptoms. Behav. Sci. 2018, 8, 102. https://doi.org/10.3390/bs8110102
Tsuboi H, Sakakibara H, Minamida Y, Tsujiguchi H, Matsunaga M, Hara A, Nakamura H. Elevated Levels of Serum IL-17A in Community-Dwelling Women with Higher Depressive Symptoms. Behavioral Sciences. 2018; 8(11):102. https://doi.org/10.3390/bs8110102
Chicago/Turabian StyleTsuboi, Hirohito, Hiroyuki Sakakibara, Yuuki Minamida, Hiromasa Tsujiguchi, Masahiro Matsunaga, Akinori Hara, and Hiroyuki Nakamura. 2018. "Elevated Levels of Serum IL-17A in Community-Dwelling Women with Higher Depressive Symptoms" Behavioral Sciences 8, no. 11: 102. https://doi.org/10.3390/bs8110102
APA StyleTsuboi, H., Sakakibara, H., Minamida, Y., Tsujiguchi, H., Matsunaga, M., Hara, A., & Nakamura, H. (2018). Elevated Levels of Serum IL-17A in Community-Dwelling Women with Higher Depressive Symptoms. Behavioral Sciences, 8(11), 102. https://doi.org/10.3390/bs8110102