Relevance and Clinical Significance of Magnetic Resonance Imaging of Neurological Manifestations in COVID-19: A Systematic Review of Case Reports and Case Series

 ,
,  , ,
, ,  , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
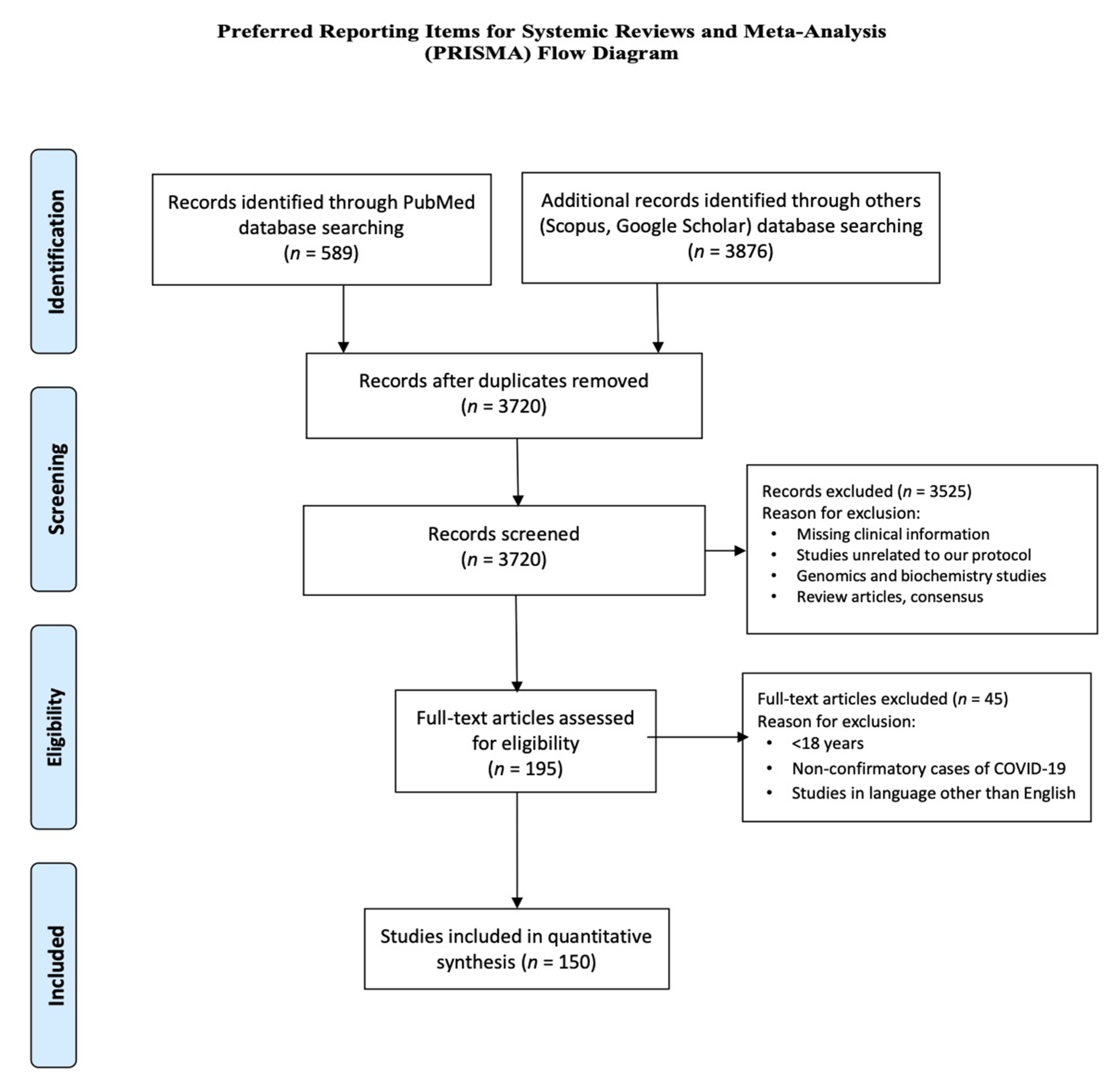
2. Material and Methods
2.1. Study Selection and Criteria
- Inclusion criteriaThe inclusion criteria for the published studies were: (1) Patient age ≥ 18 years; (2) COVID-19 diagnosis confirmed by real-time reverse transcription polymerase chain reaction (RT-PCR) nasopharyngeal or serum antibody IgG test; (3) Established neurological diagnosis in the patients with COVID-19; (4) Neuroimaging findings of CNS and PNS complications not accounted for by another neurological process.
- Exclusion criteriaThe exclusion criteria for the studies were: (1) Duplicate studies which involved repetition of cases; (2) Studies in languages other than English; (3) Studies with no individual data on severity and/or fatality of COVID-19, and (4) Studies with missing clinical information.
2.2. Quality Assessment
2.3. Data Acquisition
2.4. Data Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ADEM | Acute Disseminated Encephalomyelitis |
| AHNE | Acute Hemorrhagic Necrotizing Encephalopathy |
| CNS | Central Nervous System |
| CT | Computed Tomography |
| COVID-19 | Coronavirus infectious disease -2019 |
| CLOCC | Cytotoxic Lesion of Corpus Callosum |
| GBS | Guillain-Barré Syndrome |
| IDSA/ATS | Infectious Disease Society of America/American Thoracic Society |
| MRI | Magnetic Resonance Imaging |
| MERS | Mild encephalitis/encephalopathy with reversible splenial lesion |
| MFS | Miller-Fisher syndrome |
| MS | Multiple Sclerosis |
| nCov | Novel Coronavirus |
| ON | Optic Neuritis |
| PNS | Peripheral Nervous System |
| PET | Positron emission tomography |
| PRES | Posterior Reversible Encephalopathy Syndrome |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses |
| RT-PCR | Reverse Transcription Polymerase Chain Reaction |
| SARS-CoV-2 | Severe Acute Respiratory Distress Syndrome coronavirus 2 |
References
- Gardner, L. Available online: https://coronavirus.jhu.edu/map.html (accessed on 29 March 2020).
- Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; Cheng, Z. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.R. COVID-19 and the nervous system. J. Neurovirol. 2020, 26, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Saba, L.; Vagal, A.; Leali, M.; Rossi, A.; Gaskill, M.; Sengupta, S.; Zhang, B.; Carriero, A.; Bachir, S.; Crivelli, P. Imaging in Neurological Disease of Hospitalized COVID-19 Patients: An Italian Multicenter Retrospective Observational Study. Radiology 2020, 297, E270–E273. [Google Scholar]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munhoz, R.P.; Pedroso, J.L.; Nascimento, F.A.; Almeida, S.M.D.; Barsottini, O.G.P.; Cardoso, F.E.C.; Teive, H.A.G. Neurological complications in patients with SARS-CoV-2 infection: A systematic review. Arq. De Neuro-Psiquiatr. 2020, 78, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Kremer, S.; Lersy, F.; De Sèze, J.; Ferré, J.-C.; Maamar, A.; Carsin-Nicol, B.; Collange, O.; Bonneville, F.; Adam, G.; Martin-Blondel, G.; et al. Brain MRI Findings in Severe COVID-19: A Retrospective Observational Study. Radiology 2020, 297, E242–E251. [Google Scholar] [CrossRef]
- Chougar, L.; Shor, N.; Weiss, N.; Galanaud, D.; Leclercq, D.; Mathon, B.; Belkacem, S.; Stroër, S.; Burrel, S.; Boutolleau, D.; et al. Retrospective observational study of brain magnetic resonance imaging findings in patients with acute SARS-CoV-2 infection and neurological manifestations. Radiology 2020, 202422. [Google Scholar] [CrossRef]
- Lin, E.; Lantos, J.; Strauss, S.; Phillips, C.; Campion, T.R., Jr.; Navi, B.B.; Parikh, N.S.; Merkler, A.E.; Mir, S.; Zhang, C.; et al. Brain Imaging of Patients with COVID-19: Findings at an Academic Institution during the Height of the Outbreak in New York City. Am. J. Neuroradiol. 2020, 41, 2001–2008. [Google Scholar] [CrossRef]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 Virus Targeting the CNS: Tissue Distribution, Host–Virus Interaction, and Proposed Neurotropic Mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Chu, H.; Chan, J.F.; Yuen, T.T.; Shuai, H.; Yuan, S.; Wang, Y.; Hu, B.; Yip, C.C.; Tsang, J.O.; Huang, X.; et al. Comparative tropism, replication kinetics, and cell damage profiling of SARS-CoV-2 and SARS-CoV with implications for clinical manifestations, transmissibility, and laboratory studies of COVID-19: An observational study. Lancet Microbe 2020, 1, e14–e23. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Faculty Opinions recommendation of Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Fac. Opin. Post-Publ. Peer Rev. Biomed. Lit. 2019, 200, 45. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Joanna Briggs, I. The Joanna Briggs Institute Critical Appraisal Tools for Use in JBI Systematic Review: Checklists for Case Reports; North Adelaide, Australia The Joanna Briggs Institute: North Adelaide, Australia, 2019. [Google Scholar]
- Freeman, C.W.; Masur, J.; Hassankhani, A.; Wolf, R.L.; Levine, J.M.; Mohan, S. COVID-19-Related Disseminated Leukoencephalopathy (CRDL): A Retrospective Study of Findings on Brain MRI. Am. J. Roentgenol. 2020. [Google Scholar] [CrossRef]
- Conklin, J.; Frosch, M.P.; Mukerji, S.; Rapalino, O.; Maher, M.; Schaefer, P.W.; Lev, M.H.; Gonzalez, R.G.; Das, S.; Champion, S.N.; et al. Cerebral Microvascular Injury in Severe COVID-19. medRxiv 2020. [CrossRef]
- Hernández-Fernández, F.; Valencia, H.S.; Barbella-Aponte, R.A.; Collado-Jiménez, R.; Ayo-Martín, Ó.; Barrena, C.; Molina-Nuevo, J.D.; García-García, J.; Lozano-Setién, E.; Alcahut-Rodriguez, C.; et al. Cerebrovascular disease in patients with COVID-19: Neuroimaging, histological and clinical description. Brain 2020, 143, 3089–3103. [Google Scholar] [CrossRef]
- Giorgianni, A.; Vinacci, G.; Agosti, E.; Mercuri, A.; Baruzzi, F. Neuroradiological features in COVID-19 patients: First evidence in a complex scenario. J. Neuroradiol. 2020, 47, 474–476. [Google Scholar] [CrossRef]
- Feugeas, M.-C.H.; Gaudemer, A.; Lescure, X.; Dossier, A.; Sonneville, R.; Ehmer, C.; Choquet, C.; Raynaud-Simon, A.; Borie, R.; Amarenco, P.; et al. Covid-19 and dysregulated cerebral perfusion: Observations with multimodal MRI. medRxiv 2020. [Google Scholar] [CrossRef]
- Jain, R.; Young, M.; Dogra, S.; Kennedy, H.; Nguyen, V.; Jones, S.; Bilaloglu, S.; Hochman, K.; Raz, E.; Galetta, S.; et al. COVID-19 related neuroimaging findings: A signal of thromboembolic complications and a strong prognostic marker of poor patient outcome. J. Neurol. Sci. 2020, 414, 116923. [Google Scholar] [CrossRef]
- Delorme, C.; Paccoud, O.; Kas, A.; Hesters, A.; Bombois, S.; Shambrook, P.; Boullet, A.; Doukhi, D.; Le Guennec, L.; Godefroy, N.; et al. COVID-19-related encephalopathy: A case series with brain FDG-positron-emission tomography/computed tomography findings. Eur. J. Neurol. 2020, 27, 2651–2657. [Google Scholar] [CrossRef] [PubMed]
- Scullen, T.; Keen, J.; Mathkour, M.; Dumont, A.S.; Kahn, L. COVID-19 Associated Encephalopathies and Cerebrovascular Disease: The New Orleans Experience. World Neurosurgery. 2020. Available online: https://www.researchgate.net/profile/Mansour_Mathkour/publication/341721713_COVID-19_Associated_Encephalopathies_and_Cerebrovascular_Disease_the_New_Orleans_Experience/links/5ed2a8f392851c9c5e678d34/COVID-19-Associated-Encephalopathies-and-Cerebrovascular-Disease-the-New-Orleans-Experience.pdf (accessed on 10 October 2020).
- Radmanesh, A.; Derman, A.; Lui, Y.W.; Raz, E.; Loh, J.P.; Hagiwara, M.; Borja, M.J.; Zan, E.; Fatterpekar, G. COVID-19–associated Diffuse Leukoencephalopathy and Microhemorrhages. Radiol. 2020, 297, E223–E227. [Google Scholar] [CrossRef] [PubMed]
- Kandemirli, S.G.; Dogan, L.; Sarıkaya, Z.T.; Kara, S.; Akinci, C.; Kaya, D.; Kaya, Y.; Yildirim, D.; Tuzuner, F.; Yildirim, M.S.; et al. Brain MRI Findings in Patients in the Intensive Care Unit with COVID-19 Infection. Radiology 2020, 297, E232–E235. [Google Scholar] [CrossRef] [PubMed]
- Radmanesh, A.; Raz, E.; Zan, E.; Derman, A.; Kaminetzky, M. Brain Imaging Use and Findings in COVID-19: A Single Academic Center Experience in the Epicenter of Disease in the United States. Am. J. Neuroradiol. 2020, 41, 1179–1183. [Google Scholar] [CrossRef] [PubMed]
- Romero-Sánchez, C.M.; Díaz-Maroto, I.; Fernández-Díaz, E.; Sánchez-Larsen, Á.; Layos-Romero, A.; García-García, J.; González, E.; Redondo-Peñas, I.; Perona-Moratalla, A.B.; Del Valle-Pérez, J.A.; et al. Neurologic manifestations in hospitalized patients with COVID-19: The ALBACOVID registry. Neurology 2020. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.K.; Paliwal, V.K.; Gupta, A. Encephalopathy in patients with COVID-19: A review. J. Med Virol. 2020. [Google Scholar] [CrossRef]
- Tan, Y.-K.; Goh, C.; Leow, A.S.T.; Tambyah, P.A.; Ang, A.; Yap, E.-S.; Tu, T.-M.; Sharma, V.K.; Yeo, L.L.; Chan, B.P.L.; et al. COVID-19 and ischemic stroke: A systematic review and meta-summary of the literature. J. Thromb. Thrombolysis 2020, 50, 587–595. [Google Scholar] [CrossRef]
- Pérez, C.A. Looking ahead: The risk of neurologic complications due to COVID-19. Neurol. Clin. Pract. 2020. [Google Scholar] [CrossRef] [Green Version]
- Dogra, S.; Jain, R.; Cao, M.; Bilaloglu, S.; Zagzag, D.; Hochman, S.; Lewis, A.; Melmed, K.; Hochman, K.; Horwitz, L.I.; et al. Hemorrhagic stroke and anticoagulation in COVID-19. J. Stroke Cerebrovascular Dis. 2020, 29, 104984. [Google Scholar] [CrossRef]
- Pan, S.; Chen, W.C.; Baal, J.D.; Sugrue, L.P. Neuroradiological Features of Mild and Severe SARS-CoV-2 Infection. Acad. Radiol. 2020, 27, 1507–1514. [Google Scholar] [CrossRef]
- Benussi, A.; Pilotto, A.; Premi, E.; Libri, I.; Giunta, M.; Agosti, C.; Alberici, A.; Baldelli, E.; Benini, M.; Bonacina, S.; et al. Clinical characteristics and outcomes of inpatients with neurologic disease and COVID-19 in Brescia, Lombardy, Italy. Neurology 2020, 95, e910–e920. [Google Scholar] [CrossRef] [PubMed]
- García, L.F. Immune Response, Inflammation, and the Clinical Spectrum of COVID-19. Front. Immunol. 2020, 11, 1441. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.B.; Schwartz, N.G.; Patel, P.; Abbo, L.; Beauchamps, L.; Balan, S.; Lee, E.H.; Paneth-Pollak, R.; Geevarughese, A.; Lash, M.K.; et al. Case Series of Multisystem Inflammatory Syndrome in Adults Associated with SARS-CoV-2 Infection—United Kingdom and United States, March–August 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1450. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 1–11. [Google Scholar] [CrossRef]
- Aragao, M.; Gouveia, M.D.C.L.; Filho, O.C.; Fonseca, T.; Valenca, M. Anosmia in COVID-19 Associated with Injury to the Olfactory Bulbs Evident on MRI. Am. J. Neuroradiol. 2020, 41, 1703–1706. [Google Scholar] [CrossRef]
- Feign, V.; Lawes, C.M.M.; Bennett, D.A.; Anderson, C.S. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]
- Lee, Y.; Min, P.; Lee, S.; Kim, S.-W. Prevalence and Duration of Acute Loss of Smell or Taste in COVID-19 Patients. J. Korean Med. Sci. 2020, 35, e174. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Mean Age, SD, IQR | 53.2, 15.5, 40–64 |
| Gender * | 159 |
| Male, n (%) | 106 (66.7) |
| Female, n (%) | 53 (33.7) |
| Neurological manifestation | 171 |
| Ischemic stroke, n (%) | 62 (36.2) |
| Hemorrhagic stroke, n (%) | 41 (24) |
| Encephalitis, n (%) | 24 (14) |
| CNS inflammatory, n (%) | 44 (25.7) |
| Encephalopathy, n (%) | 11 (6.4) |
| GBS and its variant, n (%) | 3 (2) |
| Olfactory bulb enhancement, n (%) | 3 (2) |
| Other cranial nerve enhancement, n (%) | 6 (3.5) |
| Others **, n (%) | 6 (3.5) |
| Severity of COVID-19 *** | 171 |
| Severe | 96 (56.2) |
| Non-Severe | 75 (43.8) |
| Outcomes | 171 |
| Fatal | 49 (28.7) |
| Non-fatal | 122 (71.3) |
| Pathophysiology | N | Severe n (%) | Non-Severe n (%) | p-Value | Fatal n (%) | Non-Fatal n (%) | p-Value |
|---|---|---|---|---|---|---|---|
| Ischemic stroke Non-ischemic stroke | 62 109 | 35(36) 61(64) | 27(36) 48(64) | 0.951 | 25(51) 24(49) | 37(30) 85(70) | 0.011 * |
| Hemorrhagic stroke Non-hemorrhagic stroke | 41 130 | 30(31) 66(69) | 11(15) 64(85) | 0.012 * | 17(35) 32(65) | 24(20) 98(80) | 0.037 * |
| Encephalitis Non-encephalitis | 24 147 | 17(18) 79(82) | 7(9) 68(91) | 0.118 | 3(6) 46(94) | 21(17) 101(83) | 0.059 |
| CNS inflammatory Non-inflammatory | 44 127 | 24(25) 72(75) | 20(27) 55(73) | 0.805 | 11(22) 38(78) | 33(27) 89(73) | 0.534 |
| Encephalopathy Non-encephalopathy | 11 160 | 11(11) 85(89) | 0(0) 75(100) | 0.002 * | 6(12) 43(88) | 5(4) 117(96) | 0.049 * |
| GBS and its variant Non-GBS | 3 168 | 1(1) 95(99) | 2(3) 73(97) | 0.422 | 0(0) 49(100) | 3(2) 119(98) | 0.268 |
| Olfactory bulb enhancement No olfactory bulb enhancement | 3 168 | 0(0) 96(100) | 3(4) 72(96) | 0.048 * | 0(0) 49(100) | 3(2) 119(98) | 0.268 |
| Other cranial nerve enhancement Non-cranial nerve enhancement | 6 165 | 0(0) 96(100) | 6(8) 69(92) | 0.005 * | 0(0) 49(100) | 6(5) 116(95) | 0.114 |
| Others (Yes) Others (No) | 6 165 | 4(4) 92(96) | 2(3) 73(97) | 0.597 | 3(6) 46(94) | 3(2) 119(98) | 0.239 |
| Characteristics | n = 170 | Age in Years | p-Value | |
|---|---|---|---|---|
| Mean | SD | |||
| Severity | ||||
| Yes | 96 | 54.5 | 14.7 | 0.305 |
| No | 74 | 51.5 | 16.5 | |
| Fatality | ||||
| Yes | 49 | 55.2 | 15.8 | 0.331 |
| No | 121 | 52.4 | 15.4 | |
| Ischemic stroke | ||||
| Yes | 62 | 57.5 | 15.4 | 0.005 * |
| No | 108 | 50.7 | 15.1 | |
| Hemorrhagic stroke | ||||
| Yes | 41 | 51.2 | 13.1 | 0.226 |
| No | 129 | 53.8 | 16.2 | |
| Encephalitis | ||||
| Yes | 23 | 48.5 | 13.8 | 0.108 |
| No | 147 | 53.9 | 15.7 | |
| Encephalopathy | ||||
| Yes | 11 | 50.3 | 11.8 | 0.406 |
| No | 159 | 53.4 | 15.8 | |
| CNS inflammation | ||||
| Yes | 44 | 53.3 | 15.8 | 0.859 |
| No | 126 | 53.2 | 15.5 | |
| Olfactory bulb enhancement | ||||
| Yes | 3 | 29.0 | 5.3 | 0.011 * |
| No | 167 | 53.6 | 15.3 | |
| Cranial nerve enhancement | ||||
| Yes | 6 | 49.2 | 19.7 | 0.657 |
| No | 164 | 53.3 | 15.4 | |
| GBS and its variant | ||||
| Yes | 3 | 51.7 | 13.7 | 0.836 |
| No | 167 | 53.2 | 15.6 | |
| Others | ||||
| Yes | 6 | 62.3 | 10.3 | 0.147 |
| No | 164 | 52.9 | 15.6 | |
| Pathophysiology | N | Severe n (%) | Non-Severe n (%) | p-Value | Fatal n (%) | Non-Fatal n (%) | p-Value |
|---|---|---|---|---|---|---|---|
| Vascular Non-vascular | 90 81 | 53(59) 43(53) | 37(41) 38(47) | 0.445 | 34(38) 15(19) | 56(62) 66(81) | 0.005 * |
| Inflammatory Non-inflammatory | 57 114 | 36(63) 60(53) | 21(37) 54(47) | 0.191 | 17(30) 32(28) | 40(70) 82(72) | 0.811 |
| Author/Country All Studies from Year/Year Published 2020 | No. of Patients with Neuroimaging Findings | Neurological Manifestation CNS = 1, PNS = 2 | MRI Findings | Severity of COVID-19 * (Non-Severe = 1, Severe = 2) | Outcome (Non-Fatal = 1, Fatal = 2) |
|---|---|---|---|---|---|
| Freeman C.W et al. [17]/USA | 59 | 1 = 59 2 = 0 | MS = 3 Small vessel ischemic = 23 Acute infarction = 6 Subacute infarction = 4 Chronic infarction = 4 Basal ganglia hypoxia = 1 Microhemorrhage = 4 CRDL = 6 | NA | NA |
| Chougar L. et al. [9]/France | 73 | 1 = 68 2 = 2 | Acute infarction = 17 Venous infarction = 1 Microhemorrhage = 8 Perfusion abnormalities = 22 Corpus callosum cytotoxic = 3 Hypoxic Ischemic lesion = 3 Non-specific white matter and BG changes = 8 PRES = 2 Metabolic abnormalities = 3 Neuritis = 2 Meningeal enhancement = 3 Corticospinal tract flair hyperintensity = 1 | NA | NA |
| Conklin J. et al. [18] (c)/USA | 11 | 1 = 11 2 = 0 | Microbleed = Punctate and linear SWI lesions in the subcortical and deep white matter = 11 | NA | 1 = 15 2 = 1 |
| Hernández- Fernández F. et al. [19] (c)/Spain | 23 | 1 = 23 2 = 0 | cerebral ischemia = 17 Intracerebral hemorrhage = 5 PRES = 1 | 1 = 6 2 = 17 | 1 = 15 2 = 8 |
| Helms J. et al. [3] (c)/France | 13 | 1 = 13 2 = 0 | Leptomeningeal enhancement = 8/13 Perfusion abnormalities = 11/11 Ischemic stroke = 3/13 | NA | NA |
| Giorgianni A. et al. [20]/Italy | 26 | 1 = 20 2 = 0 | Ischemic = 4 Cerebral hemorrhage = 5 Encephalitis = 1 Non-acute changes = 16 | NA | NA |
| Kremer S. et al. [8] (c)/France | 37 | 1 = 37 2 = 0 | Non-hemorrhagic = 17 Hemorrhagic = 20 | NA | 1 = 32 2 = 5 |
| Feugeas MCH. et al. [21] (c)/France | 25 | 1 = 22 2 = 3 | PRES =8 Brain infarcts = 7 Microbleeds = 4 Hemorrhagic transformation of brain infarct = 1 Subacute subdural hematoma = 1 Old deep-brain hematoma = 1 Moderate or marked enlargement of optic nerve sheaths = 3 | NA | 1 fatal rest NA |
| Jain R. et al. [22] (c)/USA | 38 | 1 = 38 2 = 0 | Large infarct = 17 Lacunar = 9 hemorrhagic stroke = 9 Encephalitis = 1 Hypoxic ischemia = 2 | NA | 1 = 22 2 = 16 |
| Lin E. et al. [10] (c)/USA | 58 | 1 = 52 2 = 6 | Cerebral infarctions = 31 Parenchymal hematoma = 10 Cranial nerve = 6 Critical illness–associated Microhemorrhage = 3 PRES = 3 Non-traumatic SDH = 3 SAH = 2 | NA | NA |
| Delorme C. et al. [23] (c)/France | 4 | 1 = 4 | Encephalopathy = 4 FDG-PET/CT pattern of abnormalities, namely frontal hypometabolism and cerebellar hypermetabolism. | NA | 1 = 4 |
| Scullen T. et al. [24] (c)/USA | 27 | 1 = 27 2 = 0 | COVID-19-associated encephalopathy = 20 COVID-19–associated acute necrotizing encephalopathy = 2 COVID-19–associated vasculopathy = 5 | NA | NA |
| Radmanesh A. et al. [27] (c)/USA | 205 | 1 = 205 2 = 0 | Nonspecific white matter microangiopathy = 134 Chronic infarct = 47 Acute/subacute infarct = 13 ICH=11 | NA | NA |
| Mahammedi A. et al. [5] (c)/Italy | 51 | 1 = 48 2 = 3 | Acute ischemic infarct = 34 Intracerebral hemorrhage = 6 C.N enhancement = 1 Cauda Equina = 2 Acute encephalopathy = 1 PRES = 1 Nonspecific encephalopathy = 2 MS exacerbation = 2 Cerebral venous thrombosis = 2 | NA | NA |
| Kandemirli S. et al. [26] (c)/Turkey | 27 | 1 = 12 2 = 0 | CVT = 1 Acute ischemic infarction = 1 Cortical FLAIR MRI signal intensity abnormality =10 | NA | NA |
| Radmanesh A. et al. [25] (c)/USA | 27 | 1 = 27 2 = 0 | Diffuse Leukoencephalopathy = 4 Microbleed = 1 Combination of both = 5 Acute/subacute infarct = 11 ICH = 4 Presumed AHNE = 1 | 11/27 | 6/11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chowdhary, A.; Subedi, R.; Tandon, M.; Wen, S.; Patel, J.; Kataria, S.; Peterson, S.; Gwinn, R.; Elkhooly, M.; Prasad, A.; et al. Relevance and Clinical Significance of Magnetic Resonance Imaging of Neurological Manifestations in COVID-19: A Systematic Review of Case Reports and Case Series. Brain Sci. 2020, 10, 1017. https://doi.org/10.3390/brainsci10121017
Chowdhary A, Subedi R, Tandon M, Wen S, Patel J, Kataria S, Peterson S, Gwinn R, Elkhooly M, Prasad A, et al. Relevance and Clinical Significance of Magnetic Resonance Imaging of Neurological Manifestations in COVID-19: A Systematic Review of Case Reports and Case Series. Brain Sciences. 2020; 10(12):1017. https://doi.org/10.3390/brainsci10121017
Chicago/Turabian StyleChowdhary, Anisa, Roshan Subedi, Medha Tandon, Sijin Wen, Jenil Patel, Saurabh Kataria, Sarah Peterson, Ronald Gwinn, Mahmoud Elkhooly, Apoorv Prasad, and et al. 2020. "Relevance and Clinical Significance of Magnetic Resonance Imaging of Neurological Manifestations in COVID-19: A Systematic Review of Case Reports and Case Series" Brain Sciences 10, no. 12: 1017. https://doi.org/10.3390/brainsci10121017
APA StyleChowdhary, A., Subedi, R., Tandon, M., Wen, S., Patel, J., Kataria, S., Peterson, S., Gwinn, R., Elkhooly, M., Prasad, A., Nirwan, L., Adcock, A., & Sriwastava, S. (2020). Relevance and Clinical Significance of Magnetic Resonance Imaging of Neurological Manifestations in COVID-19: A Systematic Review of Case Reports and Case Series. Brain Sciences, 10(12), 1017. https://doi.org/10.3390/brainsci10121017