Balance Training with Electromyogram-Triggered Functional Electrical Stimulation in the Rehabilitation of Stroke Patients

Abstract
:1. Introduction
2. Materials and Methods
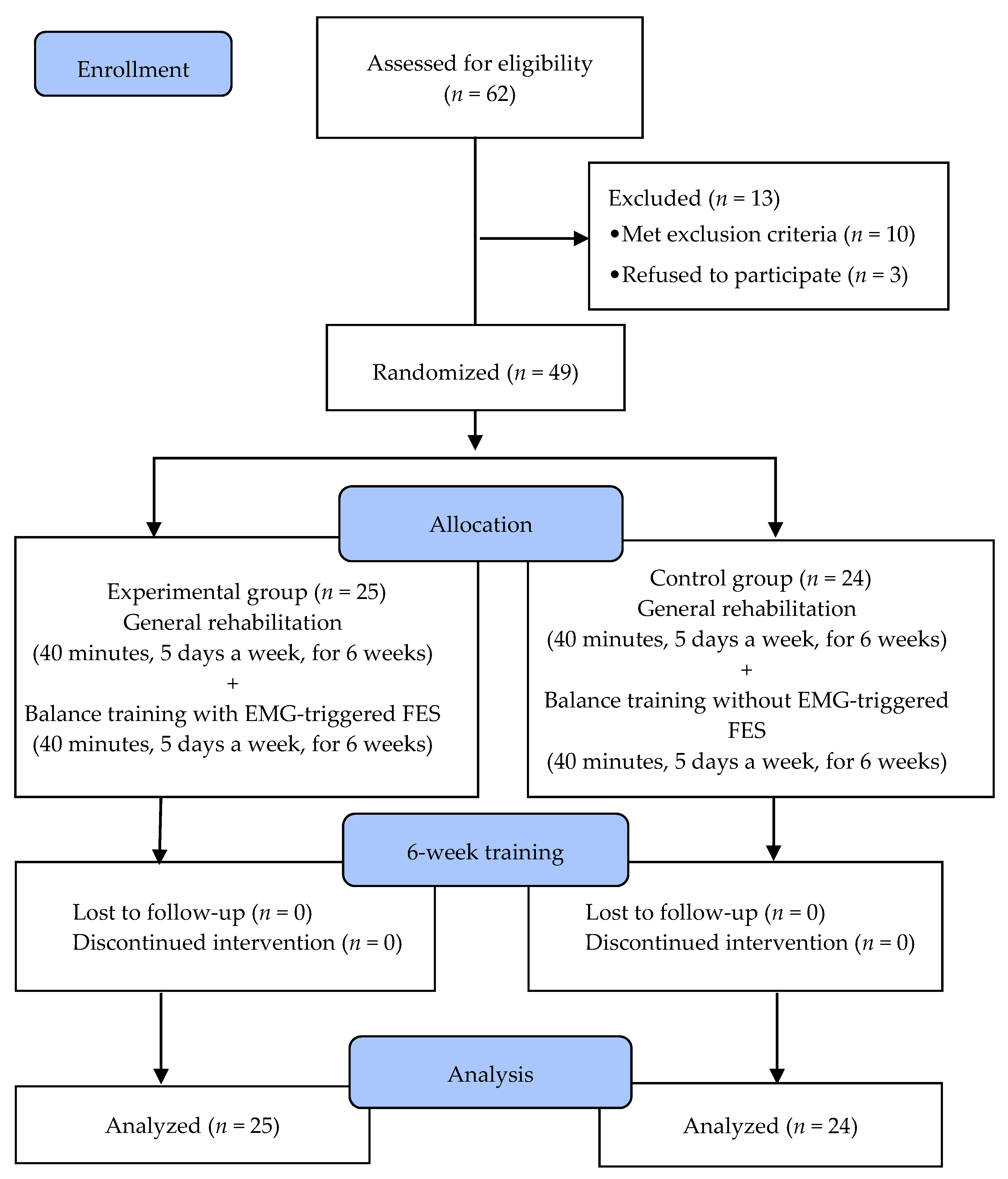
2.1. Subjects
2.2. Determination of the Sample Size
2.3. Procedure
2.4. EMG-Triggered FES
2.5. Balance Training Program
2.6. General Rehabilitation
2.7. Outcome Measurements
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Cohen, J.W.; Ivanova, T.D.; Brouwer, B.; Miller, K.J.; Bryant, D.; Garland, S.J. Do Performance Measures of Strength, Balance, and Mobility Predict Quality of Life and Community Reintegration After Stroke? Arch. Phys. Med. Rehabilitation 2018, 99, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Arene, N.; Hidler, J. Understanding Motor Impairment in the Paretic Lower Limb After a Stroke: A Review of the Literature. Top. Stroke Rehabilitation 2009, 16, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Flansbjer, U.-B.; Downham, D.; Lexell, J. Knee Muscle Strength, Gait Performance, and Perceived Participation After Stroke. Arch. Phys. Med. Rehabilitation 2006, 87, 974–980. [Google Scholar] [CrossRef] [Green Version]
- Lexell, J.; Flansbjer, U.B. Muscle strength training, gait performance and physiotherapy after stroke. Minerva Med 2008, 99, 353–368. [Google Scholar] [PubMed]
- Kwong, P.W.H.; Ng, S.S.M.; Chung, R.C.K.; Ng, G.Y.F. A structural equation model of the relationship between muscle strength, balance performance, walking endurance and community integration in stroke survivors. PLoS ONE 2017, 12, e0185807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ada, L.; Dorsch, S.; Canning, C.G. Strengthening interventions increase strength and improve activity after stroke: a systematic review. Aust. J. Physiother. 2006, 52, 241–248. [Google Scholar] [CrossRef] [Green Version]
- Van Duijnhoven, H.J.; Heeren, A.; Peters, M.A.; Veerbeek, J.M.; Kwakkel, G.; Geurts, A.C.; Weerdesteyn, V. Effects of exercise therapy on balance capacity in chronic stroke: Systematic review and meta-analysis. Stroke 2016, 47, 2603–2610. [Google Scholar] [CrossRef] [Green Version]
- Horak, F.B.; Nashner, L.M. Central programming of postural movements: Adaptation to altered support-surface configurations. J. Neurophysiol. 1986, 55, 1369–1381. [Google Scholar] [CrossRef]
- Horak, F.B.; Shupert, C.L.; Mirka, A. Components of postural dyscontrol in the elderly: A review. Neurobiol. Aging 1989, 10, 727–738. [Google Scholar] [CrossRef]
- Gatev, P.; Thomas, S.; Kepple, T.; Hallett, M. Feedforward ankle strategy of balance during quiet stance in adults. J. Physiol. 1999, 514, 915–928. [Google Scholar] [CrossRef]
- Almeida, G.; Carvalho, R.; Talis, V. Postural strategy to keep balance on the seesaw. Gait Posture 2006, 23, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Dujović, S.D.; Malešević, J.; Malešević, N.; Vidaković, A.S.; Bijelić, G.; Keller, T.; Konstantinović, L. Novel multi-pad functional electrical stimulation in stroke patients: A single-blind randomized study. Neurorehabilit. 2017, 41, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Sun, Q.; Wang, H.; Xie, G. Influence of transcutaneous electrical nerve stimulation on spasticity, balance, and walking speed in stroke patients: A systematic review and meta-analysis. J. Rehabil. Med. 2018, 50, 3–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, M.; Klawansky, S.; Stason, W.; Berkey, C.; Chalmers, T.C. Functional electrostimulation in poststroke rehabilitation: A meta-analysis of the randomized controlled trials. Arch. Phys. Med. Rehabil. 1996, 77, 549–553. [Google Scholar] [CrossRef]
- Kesar, T.M.; Perumal, R.; Jancosko, A.; Reisman, D.S.; Rudolph, K.S.; Higginson, J.S.; Binder-Macleod, S.A. Novel Patterns of Functional Electrical Stimulation Have an Immediate Effect on Dorsiflexor Muscle Function During Gait for People Poststroke. Phys. Ther. 2010, 90, 55–66. [Google Scholar] [CrossRef] [Green Version]
- Everaert, D.G.; Stein, R.B.; Abrams, G.M.; Dromerick, A.W.; Francisco, G.E.; Hafner, B.J.; Huskey, T.N.; Munin, M.C.; Nolan, K.J.; Kufta, C.V. Effect of a foot-drop stimulator and ankle-foot orthosis on walking performance after stroke: A multicenter randomized controlled trial. Neurorehabil. Neural. Repair 2013, 27, 579–591. [Google Scholar] [CrossRef]
- Mitsutake, T.; Sakamoto, M.; Horikawa, E. The effects of electromyography-triggered neuromuscular electrical stimulation plus tilt sensor functional electrical stimulation training on gait performance in patients with subacute stroke: A randomized controlled pilot trial. Int. J. Rehabil. Res. 2019, 42, 358–364. [Google Scholar] [CrossRef]
- Burridge, J.H.; Ladouceur, M. Clinical and Therapeutic Applications of Neuromuscular Stimulation: A Review of Current Use and Speculation into Future Developments. Neuromodulation: Technol. Neural Interface 2001, 4, 147–154. [Google Scholar] [CrossRef]
- Kirac-Unal, Z.; Gencay-Can, A.; Karaca-Umay, E.; Cakci, F.A. The effect of task-oriented electromyography-triggered electrical stimulation of the paretic wrist extensors on upper limb motor function early after stroke: A pilot randomized controlled trial. Int. J. Rehabil. Res. 2019, 42, 74–81. [Google Scholar] [CrossRef]
- Meilink, A.; Hemmen, B.; Seelen, H.; Kwakkel, G. Impact of EMG-triggered neuromuscular stimulation of the wrist and finger extensors of the paretic hand after stroke: A systematic review of the literature. Clin. Rehabil. 2008, 22, 291–305. [Google Scholar] [CrossRef]
- Eng, J.J. Fitness and mobility exercise (fame) program for stroke. Top Geriatr. Rehabil. 2010, 26, 310–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, S.S.; Hui-Chan, C.W. The Timed Up & Go Test: Its Reliability and Association With Lower-Limb Impairments and Locomotor Capacities in People With Chronic Stroke. Arch. Phys. Med. Rehabil. 2005, 86, 1641–1647. [Google Scholar] [PubMed]
- Katz-Leurer, M.; Fisher, I.; Neeb, M.; Schwartz, I.; Carmeli, E. Reliability and validity of the modified functional reach test at the sub-acute stage post-stroke. Disabil. Rehabil. 2009, 31, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.; Wood-Dauphinee, S.; I Williams, J. The Balance Scale: reliability assessment with elderly residents and patients with an acute stroke. Scand. J. Rehabil. Med. 1995, 27, 27–36. [Google Scholar] [PubMed]
- O Berg, K.; Wood-Dauphinee, S.L.; I Williams, J.; Maki, B. Measuring balance in the elderly: validation of an instrument. Can. J. Public Heal. 1992, 83, S7-11. [Google Scholar]
- Sardaru, D.P.; Matei, D.; Zaharia-Kezdi, D.; Pendefunda, L. Effects of biofeedback versus switch-triggered functional electrical stimulation on sciatica-related foot drop. J. Back Musculoskelet. Rehabil. 2018, 31, 239–245. [Google Scholar] [CrossRef]
- Chung, Y.; Kim, J.-H.; Cha, Y.; Hwang, S. Therapeutic effect of functional electrical stimulation-triggered gait training corresponding gait cycle for stroke. Gait Posture 2014, 40, 471–475. [Google Scholar] [CrossRef]
- Hara, Y.; Obayashi, S.; Tsujiuchi, K.; Muraoka, Y. The effects of electromyography-controlled functional electrical stimulation on upper extremity function and cortical perfusion in stroke patients. Clin. Neurophysiol. 2013, 124, 2008–2015. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar]
- Iruthayarajah, J.; McIntyre, A.; Cotoi, A.; Macaluso, S.; Teasell, R. The use of virtual reality for balance among individuals with chronic stroke: A systematic review and meta-analysis. Top. Stroke Rehabil. 2017, 24, 68–79. [Google Scholar] [CrossRef]
- Haruyama, K.; Kawakami, M.; Otsuka, T. Effect of core stability training on trunk function, standing balance, and mobility in stroke patients. Neurorehabil. Neural. Repair. 2017, 31, 240–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Experimental Group (n = 25) | Control Group (n = 24) | χ2/t | p | |
|---|---|---|---|---|
| Age (year) | 62.16 ± 8.13 | 64.88 ± 10.35 | 1.023 | 0.311 |
| Height (cm) | 163.36 ± 8.80 | 164.88 ± 7.86 | 0.634 | 0.529 |
| Weight (kg) | 63.14 ± 6.37 | 65.42 ± 8.07 | 1.099 | 0.278 |
| BMI (point) | 23.79 ± 3.15 | 24.05 ± 2.32 | 0.322 | 0.749 |
| Time since stroke (month) | 16.00 ± 6.49 | 15.25 ± 6.89 | 0.392 | 0.697 |
| MMSE | 25.92 ± 1.22 | 25.75 ± 0.94 | 0.543 | 0.589 |
| Gender (male/female) | 17/8 | 15/9 | 0.686 | 0.163 |
| Paretic side (right/left) | 16/9 | 14/10 | 0.684 | 0.166 |
| Stroke type (infarction/hemorrhage) | 17/8 | 13/11 | 0.686 | 0.163 |
| Variables | Experimental Group (n = 25) | Control Group (n = 24) | Significance of Change Scores | ||||
|---|---|---|---|---|---|---|---|
| Baseline | Post | Change Score | Baseline | Post | Change Score | t | |
| Static balance ability | |||||||
| EO-MLS (mm/s) | 4.04 ± 1.36 | 2.95 ± 0.69 | −1.08 ± 1.01 * | 3.68 ± 1.16 | 3.19 ± 0.88 | −0.49 ± 0.83 * | 2.225 † |
| EO-APS (mm/s) | 5.97 ± 1.55 | 4.74 ± 1.52 | −1.23 ± 0.75 * | 5.81 ± 1.14 | 5.10 ± 1.25 | −0.71 ± 0.63 * | 2.614 † |
| EO-VM (mm/s2) | 4.32 ± 1.47 | 2.84 ± 1.47 | −1.47 ± 0.73 * | 3.96 ± 1.08 | 3.18 ± 1.24 | −0.78 ± 1.02 * | 2.737 † |
| EC-MLS (mm/s) | 4.35 ± 1.45 | 3.21 ± 0.96 | −1.13 ± 0.79 * | 4.39 ± 1.17 | 3.87 ± 1.38 | −0.52 ± 0.70 * | 2.870 † |
| EC-APS (mm/s) | 6.05 ± 1.55 | 5.12 ± 1.50 | −0.93 ± 0.75 * | 5.61 ± 1.14 | 5.14 ± 1.04 | −0.47 ± 0.63 * | 2.700 † |
| EC-VM (mm/s2) | 5.12 ± 2.08 | 3.69 ± 1.58 | −1.43 ± 0.98 * | 4.63 ± 2.02 | 4.06 ± 1.97 | −0.57 ± 1.03 * | 2.989 † |
| Dynamic balance ability | |||||||
| TUG (sec) | 31.56 ± 7.12 | 29.41 ± 6.25 | −2.15 ± 2.39 * | 29.53 ±3.89 | 28.68 ±4.14 | −0.85 ± 1.70 * | 2.193 † |
| BBS (point) | 44.48 ± 3.44 | 45.88 ± 4.10 | 1.40 ± 1.53 * | 43.38 ± 3.52 | 43.83 ± 3.40 | 0.46 ± 0.93 * | 2.592 † |
| FRT (mm) | 189.99 ± 54.35 | 222.24 ± 57.13 | 32.24 ± 24.56 * | 192.32 ± 73.28 | 203.49 ± 78.48 | 11.17 ± 17.39 * | 3.454 † |
| Leg muscle activation | |||||||
| Tibialis anterior affected (µV) | 5.59 ± 3.69 | 10.79 ± 3.99 | 5.20 ± 1.30 * | 6.93 ± 2.17 | 7.72 ± 2.60 | 0.80 ± 1.80 | 9.693 † |
| Tibialis anterior unaffected (µV) | 33.77 ± 15.20 | 32.64 ± 14.67 | −1.13 ± 3.67 | 31.16 ± 16.91 | 32.09 ± 15.76 | 0.93 ± 3.07 | 2.121 † |
| Gastrocnemius affected (µV) | 11.99 ± 8.29 | 19.11 ± 8.35 | 7.12 ± 1.32 * | 11.92 ± 5.81 | 9.98 ± 5.19 | −1.94 ± 8.21 | 5.446 † |
| Gastrocnemius unaffected (µV) | 59.46 ± 40.63 | 58.75 ± 40.62 | −0.71 ± 2.19 | 64.78 ± 28.06 | 64.91 ± 27.95 | 0.13 ± 1.31 | 1.623 † |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K. Balance Training with Electromyogram-Triggered Functional Electrical Stimulation in the Rehabilitation of Stroke Patients. Brain Sci. 2020, 10, 80. https://doi.org/10.3390/brainsci10020080
Lee K. Balance Training with Electromyogram-Triggered Functional Electrical Stimulation in the Rehabilitation of Stroke Patients. Brain Sciences. 2020; 10(2):80. https://doi.org/10.3390/brainsci10020080
Chicago/Turabian StyleLee, Kyeongjin. 2020. "Balance Training with Electromyogram-Triggered Functional Electrical Stimulation in the Rehabilitation of Stroke Patients" Brain Sciences 10, no. 2: 80. https://doi.org/10.3390/brainsci10020080
APA StyleLee, K. (2020). Balance Training with Electromyogram-Triggered Functional Electrical Stimulation in the Rehabilitation of Stroke Patients. Brain Sciences, 10(2), 80. https://doi.org/10.3390/brainsci10020080