
Objective Knowledge Mediates the Relationship between the Use of Social Media and COVID-19-Related False Memories

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Statistical Analyses
3. Results
3.1. Data Cleaning
3.2. True and False Memories for COVID-19-Related News
3.3. Correlation Analysis
3.4. Predictors of True and False Memory Scores
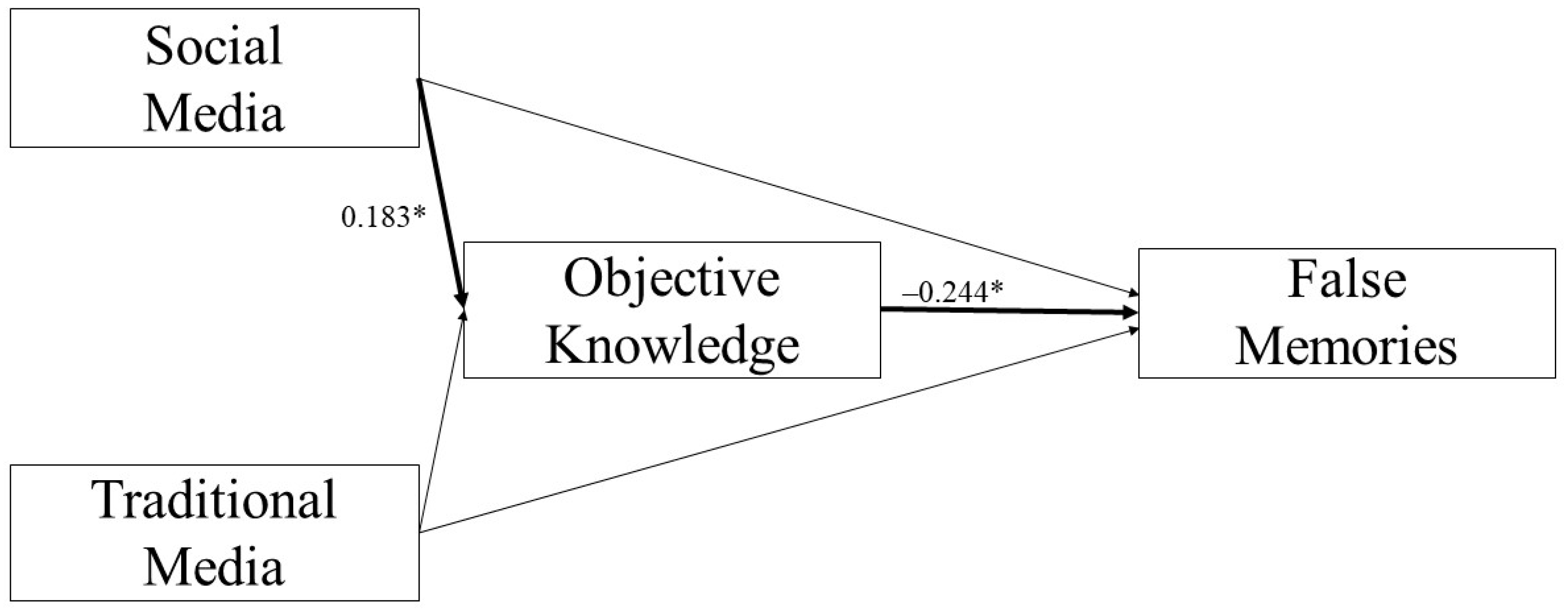
3.5. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Fake News




Appendix A.2. True News




References
- Roediger, H.L.; McDermott, K.B. Creating false memories: Remembering words not presented in lists. J. Exp. Psychol. Learn. Mem. Cogn. 1995, 21, 803–814. [Google Scholar] [CrossRef]
- Austin, J.L.; Strange, D.M. Television produces more false recognition for news than newspapers. Psychol. Pop. Media Cult. 2012, 1, 167–175. [Google Scholar] [CrossRef]
- O’Connell, A.; Greene, C.M. Not strange but not true: Self-reported interest in a topic increases false memory. Memory 2017, 25, 969–977. [Google Scholar] [CrossRef] [PubMed]
- Apuke, O.D.; Omar, B. Fake news and COVID-19: Modelling the predictors of fake news sharing among social media users. Telemat. Inform. 2021, 56, 101475. [Google Scholar] [CrossRef]
- Mehta, R.; Hoegg, J.; Chakravarti, A. Knowing too much: Expertise-induced false recall effects in product comparison. J. Consum. Res. 2011, 38, 535–554. [Google Scholar] [CrossRef]
- Frenda, S.J.; Knowles, E.D.; Saletan, W.; Loftus, E.F. False memories of fabricated political events. J. Exp. Soc. Psychol. 2013, 49, 280–286. [Google Scholar] [CrossRef]
- Greene, C.M.; Murphy, G. Individual differences in susceptibility to false memories for COVID-19 fake news. Cogn. Res. Princ. Implic. 2020, 5, 63. [Google Scholar] [CrossRef]
- Chi, M.T.H.; Glaser, R.; Farr, M.J. The Nature of Expertise; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Johnson, M.K.; Hashtroudi, S.; Lindsay, D.S. Source monitoring. Psychol. Bull. 1993, 114, 3–28. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, K.J.; Johnson, M.K. Source monitoring: Attributing mental experiences. In The Oxford Handbook of Memory; Tulving, E., Ed.; Oxford University Press: New York, NY, USA, 2000; pp. 179–195. [Google Scholar]
- McGaugh, J.L. The amygdala modulates the consolidation of memories of emotionally arousing experiences. Annu. Rev. Neurosci. 2004, 27, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, R.L.; Van Damme, I.; Levine, L.J.; Loftus, E.F. Emotion and false memory. Emot. Rev. 2015, 8, 8–13. [Google Scholar] [CrossRef]
- English, S.M.; Nielson, K.A. Reduction of the misinformation effect by arousal induced after learning. Cognition 2010, 117, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Bless, H. The interplay of affect and cognition: The mediating role of general knowledge structures. In Feeling and Thinking: The Role of Affect in Social Cognition; Studies in emotion and social interaction; 2nd Series; Cambridge University Press: New York, NY, USA, 2000; pp. 201–222. [Google Scholar]
- Storbeck, J.; Clore, G.L. With sadness comes accuracy; with happiness, false memory: Mood and the false memory effect. Psychol. Sci. 2005, 16, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Chen, C.; Loftus, E.F.; Lin, C.; He, Q.; Chen, C.; Li, H.; Xue, G.; Lu, Z.; Dong, Q. Individual differences in false memory from misinformation: Cognitive factors. Memory 2010, 18, 543–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howe, M.L.; Malone, C. Mood-congruent true and false memory: Effects of depression. Memory 2011, 19, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Gudjonsson, G.H. The relationship of intelligence and memory to interrogative suggestibility: The importance of range effects. Br. J. Clin. Psychol. 1988, 27, 185–187. [Google Scholar] [CrossRef]
- Babore, A.; Lombardi, L.; Viceconti, M.L.; Pignataro, S.; Marino, V.; Crudele, M.; Candelori, C.; Bramanti, S.M.; Trumello, C. Psychological effects of the COVID-2019 pandemic: Perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020, 293, 113366. [Google Scholar] [CrossRef] [PubMed]
- Rettie, H.; Daniels, J. Coping and tolerance of uncertainty: Predictors and mediators of mental health during the COVID-19 pandemic. Am. Psychol. 2021, 76, 427–437. [Google Scholar] [CrossRef]
- Pennycook, G.; Rand, D.G. Lazy, not biased: Susceptibility to partisan fake news is better explained by lack of reasoning than by motivated reasoning. Cognition 2019, 188, 39–50. [Google Scholar] [CrossRef]
- Powers, P.A.; Andriks, J.L.; Loftus, E.F. Eyewitness accounts of females and males. J. Appl. Psychol. 1979, 64, 339–347. [Google Scholar] [CrossRef]
- Salthouse, T.A.; Siedlecki, K.L. An individual difference analysis of false recognition. Am. J. Psychol. 2007, 120, 429–458. [Google Scholar] [CrossRef]
- Nichols, R.M.; Loftus, E.F. Who is susceptible in three false memory tasks? Memory 2019, 27, 962–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, D.L. President Bush’s false [flashbulb] memory of 9/11/01. Appl. Cogn. Psychol. 2004, 18, 363–370. [Google Scholar] [CrossRef]
- Murphy, G.; Loftus, E.F.; Grady, R.H.; Levine, L.J.; Greene, C.M. False memories for fake news during ireland’s abortion referendum. Psychol. Sci. 2019, 30, 1449–1459. [Google Scholar] [CrossRef] [PubMed]
- Greene, C.M.; Nash, R.A.; Murphy, G. Misremembering brexit: Partisan bias and individual predictors of false memories for fake news stories among Brexit voters. Memory 2021, 29, 587–604. [Google Scholar] [CrossRef] [PubMed]
- Ilardi, A.; Chieffi, S.; Iavarone, A.; Ilardi, C.R. SARS-CoV-2 in Italy: Population density correlates with morbidity and mortality. Jpn. J. Infect. Dis. 2020, 74, 61–64. [Google Scholar] [CrossRef]
- Ilardi, A.; Chieffi, S.; Ilardi, C.R. Predictive role of population density and use of public transport for major outcomes of SARS-CoV-2 infection in the Italian population: An ecological study. J. Res. Health Sci. 2021, 21, e00518. [Google Scholar] [CrossRef]
- Maggi, G.; Baldassarre, I.; Barbaro, A.; Cavallo, N.D.; Cropano, M.; Nappo, R.; Santangelo, G. Mental health status of Italian elderly subjects during and after quarantine for the COVID-19 pandemic: A cross-sectional and longitudinal study. Psychogeriatrics 2021, 21, 540–551. [Google Scholar] [CrossRef]
- Santangelo, G.; Baldassarre, I.; Barbaro, A.; Cavallo, N.D.; Cropano, M.; Maggi, G.; Nappo, R.; Trojano, L.; Raimo, S. Subjective cognitive failures and their psychological correlates in a large Italian sample during quarantine/self-isolation for COVID-19. Neurol. Sci. 2021, 42, 2625–2635. [Google Scholar] [CrossRef]
- Pennycook, G.; McPhetres, J.; Zhang, Y.; Lu, J.G.; Rand, D.G. Fighting COVID-19 misinformation on social media: Experimental evidence for a scalable accuracy-nudge intervention. Psychol. Sci. 2020, 31, 770–780. [Google Scholar] [CrossRef]
- O’Connor, C.; Murphy, M. Going viral: Doctors must tackle fake news in the COVID-19 pandemic. BMJ 2020, 369, 1587. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Lazer, D.M.J.; Baum, M.A.; Benkler, Y.; Berinsky, A.J.; Greenhill, K.M.; Menczer, F.; Metzger, M.J.; Nyhan, B.; Pennycook, G.; Rothschild, D.; et al. The science of fake news. Science 2018, 359, 1094–1096. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Global Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- Auxier, B.; Anderson, M. Social Media Use in 2021; Pew Research Center: Washington, DC, USA, 2021; pp. 1–19. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garofalo, E.; Iavarone, A.; Chieffi, S.; Carpinelli Mazzi, M.; Gamboz, N.; Ambra, F.I.; Sannino, M.; Galeone, F.; Esposito, S.; Ronga, B.; et al. Italian version of the Starkstein Apathy Scale (SAS-I) and a shortened version (SAS-6) to assess “pure apathy” symptoms: Normative study on 392 individuals. Neurol. Sci. 2021, 42, 1065–1072. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A. Beck Anxiety Inventory (BAI). In Überblick über Reliabilitäts-und Validitätsbefunde von klinischen und außerklinischen Selbst-und Fremdbeurteilungsverfahren; Ratzek, M., von Hauenschild, L., Eds.; Public Health Editions, 1988; Volume 7. [Google Scholar]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An Inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Sica, C.; Magni, C.; Ghisi, M.; Altoè, G.; Sighinolfi, C.; Chiri, L.R.; Franceschini, S. Coping orientation to problems experienced-nuova versione italiana (COPE-NVI): Uno strumento per la misura degli stili di coping. Psicoter. Cogn. E Comport. 2008, 14, 27–53. [Google Scholar]
- Foà, C.; Tonarelli, A.; Caricati, L.; Fruggeri, L. COPE-NVI-25: Validazione italiana della versione ridotta della Coping Orientation to the Problems Experienced (COPE-NVI). Psicol. Della Salut. 2015, 2, 123–140. [Google Scholar]
- Della Sala, S.; MacPherson, S.E.; Phillips, L.H.; Sacco, L.; Spinnler, H. How many camels are there in Italy? Cognitive estimates standardised on the Italian population. Neurol. Sci. 2003, 24, 10–15. [Google Scholar] [CrossRef]
- Strange, D.; Garry, M.; Bernstein, D.M.; Lindsay, D.S. Photographs cause false memories for the news. Acta Psychol. 2011, 136, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Ilardi, C.R.; Garofalo, E.; Chieffi, S.; Gamboz, N.; La Marra, M.; Iavarone, A. Daily exposure to digital displays may affect the clock-drawing test: From psychometrics to serendipity. Neurol. Sci. 2020, 41, 3683–3690. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Contemporary approaches to assessing mediation in communication research. In The SAGE Sourcebook of Advanced Data Analysis Methods for Communication Research; Sage Publications: Thousand Oaks, CA, USA, 2008; pp. 13–54. [Google Scholar]
- Ilardi, C.R.; Chieffi, S.; Scuotto, C.; Gamboz, N.; Galeone, F.; Sannino, M.; Garofalo, E.; La Marra, M.; Ronga, B.; Iavarone, A. The frontal assessment battery 20 years later: Normative data for a shortened version (FAB15). Neurol. Sci. 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Bookbinder, S.H.; Brainerd, C.J. Emotion and false memory: The context-content paradox. Psychol. Bull. 2016, 142, 1315–1351. [Google Scholar] [CrossRef] [PubMed]
- Gaesser, B. Constructing memory, imagination, and empathy: A cognitive neuroscience perspective. Front. Psychol. 2013, 3, 576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathur, V.A.; Harada, T.; Lipke, T.; Chiao, J.Y. Neural basis of extraordinary empathy and altruistic motivation. Neuroimage 2010, 51, 1468–1475. [Google Scholar] [CrossRef]
- Masten, C.L.; Morelli, S.A.; Eisenberger, N.I. An fMRI investigation of empathy for “social pain” and subsequent prosocial behavior. Neuroimage 2011, 55, 381–388. [Google Scholar] [CrossRef]
- Euston, D.R.; Gruber, A.J.; McNaughton, B.L. The role of medial prefrontal cortex in memory and decision making. Neuron 2012, 76, 1057–1070. [Google Scholar] [CrossRef] [Green Version]
- Corcoran, K.A.; Quirk, G.J. Recalling safety: Cooperative functions of the ventromedial prefrontal cortex and the hippocampus in extinction. CNS Spectr. 2007, 12, 200–206. [Google Scholar] [CrossRef]
- Quinn, J.J.; Ma, Q.D.; Tinsley, M.R.; Koch, C.; Fanselow, M.S. Inverse temporal contributions of the dorsal hippocampus and medial prefrontal cortex to the expression of long-term fear memories. Learn. Mem. 2008, 15, 368–372. [Google Scholar] [CrossRef] [Green Version]
- Izquierdo, I.; Furini, C.R.G.; Myskiw, J.C. Fear memory. Physiol. Rev. 2016, 96, 695–750. [Google Scholar] [CrossRef] [Green Version]
- Jasmin, L.; Granato, A.; Ohara, P.T. Rostral agranular insular cortex and pain areas of the central nervous system: A tract-tracing study in the rat. J. Comp. Neurol. 2004, 468, 425–440. [Google Scholar] [CrossRef] [PubMed]
- Villano, I.; Ilardi, C.R.; Arena, S.; Scuotto, C.; Gleijeses, M.; Messina, G.; Messina, A.; Monda, V.; Monda, M.; Iavarone, A.; et al. Obese subjects without eating disorders experience binge episodes also independently of emotional eating and personality traits among university students of southern Italy. Brain Sci. 2021, 11, 1145. [Google Scholar] [CrossRef] [PubMed]
- Hikosaka, O. The habenula: From stress evasion to value-based decision-making. Nat. Rev. Neurosci. 2010, 11, 503–513. [Google Scholar] [CrossRef] [PubMed]
- La Marra, M.; Caviglia, G.; Perrella, R. Using smartphones when eating increases caloric intake in young people: An overview of the literature. Front. Psychol. 2020, 11, 587886. [Google Scholar] [CrossRef] [PubMed]
- Itoi, K.; Sugimoto, N. The brainstem noradrenergic systems in stress, anxiety and depression. J. Neuroendocrinol. 2010, 22, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Kranz, G.S.; Kasper, S.; Lanzenberger, R. Reward and the serotonergic system. Neuroscience 2010, 166, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, L.A.; Foa, E.B.; Brigidi, B.D.; Przeworski, A. Are trauma victims susceptible to “false memories”? J. Abnorm. Psychol. 2000, 109, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Rapee, R.M.; McCallum, S.L.; Melville, L.F.; Ravenscroft, H.; Rodney, J.M. Memory bias in social phobia. Behav. Res. Ther. 1994, 32, 89–99. [Google Scholar] [CrossRef]
- Thorpe, S.J.; Salkovskis, P.M. Recall and recognition memory for spider information. J. Anxiety Disord. 2000, 14, 359–375. [Google Scholar] [CrossRef]
- Wenzel, A.; Jostad, C.; Brendle, J.R.; Ferraro, F.R.; Lystad, C.M. An investigation of false memories in anxious and fearful individuals. Behav. Cogn. Psychother. 2004, 32, 257–274. [Google Scholar] [CrossRef]
- Joormann, J.; Teachman, B.A.; Gotlib, I.H. Sadder and less accurate? False memory for negative material in depression. J. Abnorm. Psychol. 2009, 118, 412–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvillo, D.P.; Rutchick, A.M. Political knowledge reduces hindsight memory distortion in election judgements. J. Cogn. Psychol. 2014, 26, 213–220. [Google Scholar] [CrossRef]
- Alba, J.W.; Hutchinson, J.W. Knowledge calibration: What consumers know and what they think they know. J. Consum. Res. 2000, 27, 123–156. [Google Scholar] [CrossRef] [Green Version]
- Awad, S.S.; Liscum, K.R.; Aoki, N.; Awad, S.H.; Berger, D.H. Does the subjective evaluation of medical student surgical knowledge correlate with written and oral exam performance? J. Surg. Res. 2002, 104, 36–39. [Google Scholar] [CrossRef]
- Rock, E.M.; Ireland, M.; Resnick, M.D.; McNeely, C.A. A rose by any other name? Objective knowledge, perceived knowledge, and adolescent male condom use. Pediatrics 2005, 115, 667–672. [Google Scholar] [CrossRef]
- Kobos, E.; Imiela, J.; Kryczka, T.; Szewczyk, A.; Knoff, B. Actual and perceived knowledge of type 1 diabetes mellitus among school nurses. Nurse Educ. Today 2020, 87, 104304. [Google Scholar] [CrossRef]
- Han, T.I. Objective knowledge, subjective knowledge, and prior experience of organic cotton apparel. Fash. Text. 2019, 6, 4. [Google Scholar] [CrossRef] [Green Version]
- Johnson, T.J.; Kaye, B.K. Reasons to believe: Influence of credibility on motivations for using social networks. Comput. Hum. Behav. 2015, 50, 544–555. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean | SD | Range |
|---|---|---|---|
| TM score | 1.89 | 0.97 | 0–4 |
| FM score | 0.75 | 0.84 | 0–3 |
| Use of traditional media | 3.56 | 1.19 | 0–5 |
| Use of social media | 3.18 | 1.37 | 0–5 |
| PK score | 3.19 | 0.86 | 1–5 |
| OK score | 5.20 | 1.45 | 1–8 |
| Fear of contracting COVID-19 | 3.23 | 1.07 | 1–5 |
| Fear of others contracting COVID-19 | 4.42 | 0.77 | 1–5 |
| BDI score | 12.15 | 7.69 | 0–37 |
| BAI score | 15.81 | 11.65 | 0–44 |
| CET score | 20.78 | 8.99 | 3–62 |
| COPE—Avoidance Strategies | 9.48 | 3.48 | 4–21 |
| COPE—Transcendent Orientation | 5.68 | 3.35 | 4–19 |
| COPE—Positive Attitude | 24.73 | 5.11 | 11–36 |
| COPE—Social Support | 18.95 | 5.87 | 5–30 |
| COPE—Problem Solving | 21.05 | 4.67 | 7–30 |
| Responses Frequency (%) | Source Memory Frequency (%) | News | |||
|---|---|---|---|---|---|
| True news | |||||
| Surfaces | Immunization | Monoclonal antibodies | Symptoms | ||
| I do not remember this | 95 (53.7) | 146 (82.5) | 104 (58.8) | 28 (15.8) | |
| I remember this | 82 (46.3) | 31 (17.5) | 73 (41.2) | 149 (84.2) | |
| Traditional media | 47 (57.3) | 23 (74.2) | 57 (78.08) | 104 (69.8) | |
| Social media | 35 (42.7) | 8 (25.8) | 16 (21.9) | 45 (30.2) | |
| Fake news | |||||
| Flu vaccine | Serological tests | Masks | Pets | ||
| I do not remember this | 136 (76.8) | 143 (80.8) | 166 (93.8) | 131 (74.0) | |
| I remember this | 41 (23.2) | 34 (19.2) | 11 (6.2) | 46 (26.0) | |
| Traditional media | 28 (69.3) | 20 (58.8) | 8 (72.7) | 21 (45.6) | |
| Social media | 13 (31.7) | 14 (41.2) | 3 (27.3) | 25 (54.3) | |
| Predictors | Simple Regression Analysis | Multiple Regression Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| B | t | p | R2 | B | t | p | R2 | |
| True Memories | ||||||||
| Use of traditional media | 0.302 | 5.230 | <0.001 | 0.135 | 0.243 | 4.253 | <0.001 | 0.244 |
| Use of social media | 0.204 | 3.964 | <0.001 | 0.082 | 0.131 | 2.646 | 0.009 | |
| PK score | 0.126 | 1.490 | 0.138 | 0.013 | ||||
| OK score | 0.188 | 3.868 | <0.001 | 0.079 | 0.135 | 2.940 | 0.004 | |
| Fear of contracting COVID-19 | 0.159 | 2.357 | 0.020 | 0.031 | 0.146 | 1.937 | 0.064 | |
| Fear of others contracting COVID-19 | 0.204 | 2.149 | 0.030 | 0.026 | –0.017 | –0.157 | 0.875 | |
| BDI score | −0.007 | −0.765 | 0.446 | 0.003 | ||||
| BAI score | −0.004 | −0.660 | 0.510 | 0.002 | ||||
| CET score | −0.009 | −1.129 | 0.261 | 0.007 | ||||
| COPE—Avoidance Strategies | 0.013 | 0.605 | 0.546 | 0.002 | ||||
| COPE—Transcendent Orientation | −0.021 | −0.949 | 0.344 | 0.005 | ||||
| COPE—Positive Attitude | −0.018 | −1.289 | 0.199 | 0.009 | ||||
| COPE—Social Support | 0.003 | 0.265 | 0.792 | 0.000 | ||||
| COPE—Problem Solving | −0.014 | −0.911 | 0.363 | 0.005 | ||||
| False Memories | ||||||||
| Use of traditional media | 0.070 | 1.325 | 0.187 | 0.010 | 0.161 | |||
| Use of social media | 0.030 | 0.649 | 0.517 | 0.002 | ||||
| PK score | 0.072 | 0.980 | 0.329 | 0.005 | ||||
| OK score | −0.225 | −5.580 | <0.001 | 0.151 | −0.217 | −5.364 | <0.001 | |
| Fear of contracting COVID-19 | −0.088 | −1.499 | 0.136 | 0.013 | ||||
| Fear of others contracting COVID-19 | −0.164 | −2.006 | 0.046 | 0.022 | −0.111 | −1.451 | 0.149 | |
| BDI score | 0.001 | 0.138 | 0.890 | 0.000 | ||||
| BAI score | 0.005 | 0.923 | 0.357 | 0.005 | ||||
| CET score | 0.008 | 1.114 | 0.267 | 0.007 | ||||
| COPE—Avoidance Strategies | 0.007 | 0.383 | 0.702 | 0.001 | ||||
| COPE—Transcendent Orientation | −0.003 | −0.174 | 0.862 | 0.000 | ||||
| COPE—Positive Attitude | 0.007 | 0.563 | 0.574 | 0.002 | ||||
| COPE—Social Support | −0.014 | −1.321 | 0.188 | 0.010 | ||||
| COPE—Problem Solving | −0.006 | −0.456 | 0.649 | 0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scuotto, C.; Ilardi, C.R.; Avallone, F.; Maggi, G.; Ilardi, A.; Borrelli, G.; Gamboz, N.; La Marra, M.; Perrella, R. Objective Knowledge Mediates the Relationship between the Use of Social Media and COVID-19-Related False Memories. Brain Sci. 2021, 11, 1489. https://doi.org/10.3390/brainsci11111489
Scuotto C, Ilardi CR, Avallone F, Maggi G, Ilardi A, Borrelli G, Gamboz N, La Marra M, Perrella R. Objective Knowledge Mediates the Relationship between the Use of Social Media and COVID-19-Related False Memories. Brain Sciences. 2021; 11(11):1489. https://doi.org/10.3390/brainsci11111489
Chicago/Turabian StyleScuotto, Chiara, Ciro Rosario Ilardi, Francesco Avallone, Gianpaolo Maggi, Alfonso Ilardi, Giovanni Borrelli, Nadia Gamboz, Marco La Marra, and Raffaella Perrella. 2021. "Objective Knowledge Mediates the Relationship between the Use of Social Media and COVID-19-Related False Memories" Brain Sciences 11, no. 11: 1489. https://doi.org/10.3390/brainsci11111489