Abstract
(1) Background: Charcot–Marie–Tooth disease (CMT) is the most frequent form of inherited chronic motor and sensory polyneuropathy. Over 100 CMT causative genes have been identified. Previous reports found PMP22, GJB1, MPZ, and MFN2 as the most frequently involved genes. Other genes, such as BSCL2, MORC2, HINT1, LITAF, GARS, and autosomal dominant GDAP1 are responsible for only a minority of CMT cases. (2) Methods: we present here our records of CMT patients harboring a mutation in one of these rare genes (BSCL2, MORC2, HINT1, LITAF, GARS, autosomal dominant GDAP1). We studied 17 patients from 8 unrelated families. All subjects underwent neurologic evaluation and genetic testing by next-generation sequencing on an Ion Torrent PGM (Thermo Fischer) with a 44-gene custom panel. (3) Results: the following variants were found: BSCL2 c.263A > G p.Asn88Ser (eight subjects), MORC2 c.1503A > T p.Gln501His (one subject), HINT1 c.110G > C p.Arg37Pro (one subject), LITAF c.404C > G p.Pro135Arg (two subjects), GARS c.1660G > A p.Asp554Asn (three subjects), GDAP1 c.374G > A p.Arg125Gln (two subjects). (4) Expanding the spectrum of CMT phenotypes is of high relevance, especially for less common variants that have a higher risk of remaining undiagnosed. The necessity of reaching a genetic definition for most patients is great, potentially making them eligible for future experimentations.
1. Introduction
Charcot–Marie–Tooth disease (CMT) is the most frequent form of inherited chronic motor and sensory polyneuropathies and one of the most frequent genetic neuromuscular disorders, with a prevalence of 1:2500 [1]. CMT can manifest in heterogeneous ways, with variable phenotypic presentation even among subjects belonging to the same family [2]. In rare cases, the CMT phenotype could be worsened by a superimposed inflammatory process [3,4]. The classification of CMT is based on the type of inheritance (autosomal dominant, AD; autosomal recessive, AR; X-linked) and on the results of upper limb motor nerve conduction studies: CMT1, predominantly demyelinating, is characterized by nerve velocity under 38 m/s; CMT2, predominantly axonal, presents motor velocities above 38 m/s. An additional group includes intermediate CMT, with motor conduction velocities between 25 and 45 m/s [5]. Over 100 CMT causative genes have been identified. Previous reports found PMP22, GJB1, MPZ, and MFN2 as the most frequently involved genes [6,7,8,9]. Other reports of CMT patients from the Mediterranean area showed that other genes (autosomal recessive GDAP1 and HSPB1) could frequently be involved, suggesting that genetic distribution could possibly be influenced by geographical features [10,11,12,13,14]. It has been calculated that almost 90% of CMT patients harbor a mutation in one of the above-mentioned genes [1,15]. Other genes, such as BSCL2, MORC2, HINT1, LITAF, GARS1, and autosomal dominant GDAP1 are responsible of only a minority of CMT cases, with the consequence that the corresponding phenotypic presentations are less known and less defined.
BSCL2, encoding for Seipin, an integral membrane protein, has been associated with an autosomal dominant transmitted form of distal hereditary motor neuropathy (dHMNtype V) and axonal CMT (CMT2D) (Table 1) and with Silver syndrome (SS)/spastic paraplegia 17 [16]. It is also involved in autosomal recessive congenital generalized lipodystrophy type 2 [16]. The BSCL2 pathogenic variants most frequently reported are p.Asn88Ser and p.Ser90Leu, while p.Ser90Trp and p.Arg96His are less frequent [17]. Recently, two other disease-causative variants have been identified (p.Asn88Thr and p.Ser141Ala) [17]. BSCL2 patients have been reported worldwide [17,18,19,20,21,22,23,24,25]. Disease onset is between the 2nd and the 5th decade, with apparently a greater disease severity in male patients than in females [17]. Clinical examination could reveal distal motor weakness in the upper and/or lower limbs and pyramidal signs [24,25]. Sensory involvement could be present, generally of mild degree and often subclinical, and can be detected only at neurophysiological examination [16,17,18,21,22,25]. Sporadic cases of respiratory disfunction and sensory hearing loss have been reported [18,22] (Table 1).

Table 1.
Usual phenotypes and atypical features of the BSCL2, MORC2, HINT1, LITAF, GARS1, and GDAP1 genes.
A MORC2 variant associated with CMT (Table 1) has been firstly described in 2015 [26]. This gene codes for Microrchidia family CW-type zinc finger 2 (MORC2), a member of the MORC protein family, that has been postulated to regulate the DNA damage response [26]. In a recent report, MORC2 variants have been found responsible for the modification of axonal transport, neurofilament homeostasis, and the architecture of the cytoskeleton; they possibly have a role also in Schwann cell function [27]. The most frequent pathogenic variant is p.Arg252Trp, which is presents in more than 50% of cases [27]. The phenotypic manifestation correlated with this gene variant is an axonal motor and sensory polyneuropathy (CMT2Z) with an onset ranging from the congenital period, associated with a more severe clinical picture resembling Spinal Muscular Atrophy, to the juvenile age, characterized by classic distal sensory and motor symptoms and signs of disease progressively and asymmetrically spreading to proximal sites (Table 1). Pyramidal signs, cerebellar atrophy, diaphragmatic paralysis, tongue atrophy, mental retardation, and spinal cord atrophy were also reported [28] (Table 1).
HINT1 (Table 1) encodes histidine triad nucleotide-binding protein 1 (HINT1) that is involved in manifold transcriptional and signaling pathways [29]. Autosomal recessive variants of this gene have been previously reported, in particular from Central and South-East Europe, Russia, and Turkey. Four proven founder variants have been identified: p.Arg37Pro, the most common, p.Cys84Arg, p.His112Asn, and Cys38Arg [30,31]. Disease onset is frequently in the first or second decade, with a prevalent motor polyneuropathy that causes weakness in lower limbs’ muscles and gait impairment [32]. In most of the patients, neuromyotonia is also present [31,32] (Table 1). Recently, even neuro-psychiatric symptoms (late language development, social behavioral alterations) have been described [31,33] (Table 1).
Lipopolysaccharide-induced tumor necrosis factor (LITAF) is involved in an endolysosomal pathway that is required to maintain the homeostasis of late endosomes and lysosomes [34]. LITAF pathogenic variants cause an autosomal dominant chronic demyelinating polyneuropathy, classified as CMT1C [35] (Table 1), frequently but not exclusively presenting in young age [36]. The CMT1C phenotype could resemble that of CMT1A, in particular as regard the degree of sensory loss, foot deformities, and scoliosis, but muscle weakness, areflexia, and motor nerve conduction are milder [37]. Disease presentation with only sensory symptoms (limited to isolated paresthesia) could also be possible [37], as well as the presence of motor conduction blocks, postural tremors, and plantar ulcers [35,37] (Table 1).
GARS1 encodes Glycyl-tRNA synthetase, a dually (cytoplasmic and mitochondrial) localized enzyme of the aminoacyl-tRNA synthetase (aaRS) family [38,39]. Defects in this enzyme’s activity result in the reduction of aminoacylation activity, changes in axon location, and alterations in the neuropilin 1 pathway [38] and lead to a CMT2 or dHMN type V phenotype, mainly involving the upper extremities at distal sites [16] (Table 1).
Ganglioside-induced differentiation-associated protein 1 (GDAP1) is an integral mitochondrial membrane protein. It is mainly expressed in neurons of both central and peripheral nervous systems, and has the role of maintaining the normal functioning, structure, and movement of the mitochondria [40]. Autosomal recessive variants of GDAP1 have been associated with demyelinating, intermediate, and axonal CMT [41], whereas the few cases of dominant variants are mainly responsible for axonal CMT [42,43] (Table 1).
We present here our records of CMT patients harboring a mutation in one of these rare genes (BSCL2, MORC2, HINT1, LITAF, GARS1, autosomal dominant GDAP1).
2. Materials and Methods
We studied 17 patients from 8 unrelated family. All subjects underwent a neurologic evaluation and a genetic test by next-generation sequencing on an Ion Torrent PGM (Thermo Fischer, Waltham, MA, USA) with a 44-gene custom panel (see Appendix A), and we found BSCL2, MORC2, HINT1, LITAF, GARS1, or GDAP1 variants. Nerve conduction studies were performed in 12/17 patients. The pathogenicity of the found variants was investigated through the VarSome platform [44]. This study was approved and performed under the ethical guidelines issued by our institution for clinical studies (ethical Committee of the University Hospital of Messina; address: AOU “G.Martino,” via Consolare Valeria n. 1, 98125-Messina (ME), Italy. Approval Code: prot. 53, verbale n. 03/2014; approval date: 24 February 2014) and was in compliance with the Helsinki Declaration. The diagnostic procedures were conducted according to the ethics committee of our hospital, and informed written consent was obtained from all patients.
3. Results
3.1. BSCL2 (CMT2) (OMIM 606158)
We report here two unrelated three-generation families harboring the c.263A > G p.Asn88Ser heterozygous pathogenic variant of BSCL2 (Table 2 and Table 3).
Table 2.
Genetic analysis results of the eight families studied.
Table 3.
Clinical characteristics and unusual features of all of the 17 subjects.
In the first family (Figure A1), the proband (patient 1.1) presented distal motor weakness in the hands, with brisk reflexes and no sensory disturbances. However, neurophysiological study revealed a predominantly motor axonal neuropathy (Table 4); therefore, a subclinical sensitive involvement could be supposed. A neurological examination of one of her sisters (patient 1.2) revealed with pes cavus, distal motor deficits in the lower limbs, hypoesthesia and dysesthesias of the feet, and pyramidal signs (hyperreflexia and bilateral Hoffman’s sign). Another sister (patient 1.3) had brisk reflexes and bilateral Hoffman’s sign; since the age of 6, she presented visual impairment and was diagnosed with pigmentosus retinitis and bilateral cataract. The proband’s son (patient 1.4), 16 years old, showed normal features at neurological and neurophysiological examinations, except for bilateral sensory hypoacusia. The proband’s father (patient 1.5), 74 years of age, had only a bilateral pes cavus. Patients 1.2, 1.3, and 1.4 had an axonal polyneuropathy at neurophysiologic evaluation (Table 4).
Table 4.
Neurophysiological studies of 12/17 subjects.
In the second family (Figure A2), the proband (patient 2.1) was a 16-year-old boy who had presented pes cavus and hammertoes for many years. He mainly complained of cramps at his lower limbs. At neurological examination, we found bilateral pes cavus and hammertoes, with the left foot intrarotated, bilateral shortening of Achille’s tendon, proximal and distal muscular hypotrophy, and hyposthenia of the upper limbs, hyposthenia of plantar dorsiflexion, hyperreflexia of the lower limbs, and no sensory impairment. The proband’s father (patient 2.2) was 43 years old and did not complain of any symptoms, although he referred that many people had told him that his walking was not normal. At the visit, we found bilateral pes cavus with hammertoes and hypotrophy and hyposthenia of the antero-lateral legs’ muscles with pseudohypertrophy of the calves’ muscles. The patellar reflex was brisk bilaterally, but Achilles’ tendon reflex was normal. Sensory examination was normal. Neurophysiological studies revealed an axonal polyneuropathy (Table 4) and an augmentation of the central conduction time in upper limbs motor evoked potentials in both patients. The proband’s grandmother (patient 2.3), 72 years old, had only bilateral pes cavus and hammertoes.
3.2. MORC2 (CMT2) (OMIM 616661)
Our patient (patient 3.1, Table 3), a 54-year-old female, had a three-year story of paresthesia in both feet and hands and impaired walking and balance. Admitted to another Hospital, she underwent liquor analysis that revealed the presence of 114 mg/dL of protein. A diagnosis of CIDP was made, and she was treated with intravenous immunoglobulins, without benefit. When she came to our observation, a neurologic examination showed ataxic gait, deep tendon reflexes diminished in the upper limbs and absent in the lower limbs, and decreased pain and vibration sensitivity distally in the four limbs, with dysesthesias. Nerve conduction studies showed an axonal demyelinating polyneuropathy (Table 4). Genetic testing showed the presence of a c.1503A > T p.Gln501His heterozygous variant of uncertain significance (VUS) in MORC2 (Table 2).
3.3. HINT1 (CMT2) (OMIM 601314)
Our patient (patient 4.1, Table 3), a 15-year-old female of Eastern Europe origin, came to our observation with a likely positive story of neuromuscular disorder: a cousin of her mother, dead at age 34, had motor deficits in the four limbs and reduced visual acuity. The patient’s parents were not consanguineous. She had complained of gait impairment since the age of 10. Some years after, she developed difficulty in fine hands movements and balance impairment. Neurologic examination showed bilateral stepping gait, hypotrophy of hands’ and legs’ muscles, shortening of Achille’s tendons, postural tremor in both hands, moderate/severe hyposthenia of intrinsic hand muscles and of antero-lateral leg’s compartment muscles, areflexia. Neurophysiologic evaluation showed an axonal-demyelinating sensory–motor polyneuropathy, more severe in the lower limbs (Table 4). Genetic tests revealed a c.110G > C p.Arg37Pro homozygous, pathogenic variant in HINT1 (Table 2).
3.4. LITAF (CMT1) (OMIM 603795)
Our proband (patient 5.1, Table 3) (Figure A3), a 41-year-old male, presented pes cavus since adolescence. However, he did not report any kind of symptoms until the age of 37, when he developed foot paresthesia, walking difficulty, and reduced right grip strength. He underwent a neurophysiological examination that showed demyelination patterns consisting with CMT1 (Table 4). At neurological examination, he showed distal upper limbs postural tremors, impossibility of walking on heels, positive Romberg test, hyposthenia of intrinsic hand muscles (MRC 4) and of leg (MRC 4−) and calf muscles (MRC 4+), deep tendon areflexia, hypoesthesia, and hypopallesthesia of the feet. The proband’s daughter (patient 5.2), 6 years old, had complained of walking difficulties (easy falls, walking on toes) since the age of 2. A genetic test of both patients revealed the presence of the c.404C > G p.Pro135Arg heterozygous, uncertain-significance/likely pathogenic variant of LITAF (Table 2).
3.5. GARS1 (CMT2) (OMIM 600287)
We report here a two-generation family with the c.1660G > A p.Asp554Asn heterozygous, uncertain-significance/likely pathogenic variant on GARS1 (Table 2 and Table 3) (Figure A4).
The proband (patient 6.1) is a 53-year-old male that reported no family history suggestive of neuromuscular disease. For a couple of years, he had been complaining of a no better defined “pain” in the lower limbs and of a reduction of hands’ strength (i.e., he had become unable to unscrew a bottle cap). At neurological examination, he could not stay on heels and presented hypotrophy of tenar and leg muscles, with mild hyposthenia of antero-lateral leg muscles. Deep tendon reflexes were reduced/absent in the upper limbs and normal in the lower limbs. Sensory examination was normal. A neurophysiological evaluation showed an axonal polyneuropathy (Table 4). Genetic testing revealed the presence of a c.1660G > A p.Asp554Asn heterozygous variant of GARS. After genetic counselling, both proband’s sons (14 and 28 years old) (patients 6.2 and 6.3) underwent genetic testing that revealed the same variant in both: their neurological examination was normal, but the younger one complained of mild difficulty in fine hands’ movements and sporadic intentional tremor.
3.6. GDAP1 (CMT1/CMT2) (OMIM 606598)
We present two unrelated patients, both harboring the c.374G > A p.Arg125Gln heterozygous, likely pathogenic variant of GDAP1 (Table 2 and Table 3).
The first patient (patient 7.1), a 52-year-old male, referred of a walking impairment since the age of 43, that gradually worsened during the years. He did not report any family history. Clinical evaluation showed bilateral steppage, severe lower limbs’ muscles hypotrophy, severe hyposthenia of the leg muscles (MRC 2), and mild hyposthenia of the calf muscles (MRC 4). He presented also hyposthenia of the proximal lower limbs’ muscles and was able to squat only with support. Deep tendon reflexes were very brisk, except for the Achille’s tendon reflexes (absent).
The second patient (patient 8.1), a 50-year-old male, presented, since the age of 3, with a reduction of visual acuity. At the age of 20, he was diagnosed with optic nerve subatrophy and neurosensorial hypoacusia. At the age of 24, he developed a sensory–motor polyneuropathy. A neurological evaluation showed left steppage, reduction of lower limbs muscles’ tonus and trophism, mild hyposthenia of the anterolateral leg muscles (worse on the left side), and brisk reflexes in the upper limbs, with bilateral Hoffman’s sign and hypopallestesia from the anterior superior iliac spine.
Nerve conduction studies revealed an axonal polyneuropathy in both patients (Table 4).
4. Discussion
CMT genetic confirmation has always represented a challenge. Classically, clinicians could use some algorithms, based on NCV and type of inheritance, to guide the genetic testing [15]. In this way, approximately 60% of CMT patients could receive a genetic diagnosis [1]. Recently introduced innovative techniques of genome sequencing, such as next-generation sequencing (NGS) and whole-exome sequencing (WES), have rapidly increased the number of known genes associated with CMT, which are now over 100 [5]. Although some genes are more frequently found than others [6,7,8,9,10,11,12,13,14], also ‘rare among rare’ genes should be taken into consideration. In this paper, we have presented some patients harboring genetic variants of uncommon CMT genes. Almost all of them (BSCL2, MORC2, HINT1, GARS1, and autosomal dominant GDAP1) are responsible for a CMT2 phenotype, types of CMT for which genetic definition is less frequently reached. Some peculiar features that could be associated with these variants could help clinicians direct the genetic testing. For example, in our BSCL2 patients, we found the already reported pyramidal signs and neurosensorial hypoacusia. In addition, we reported pigmentosus retinitis with bilateral cataract in patient 1.3 and proximal UL weakness in pt. 2.1. Pigmentosus retinitis has been associated with PHARC syndrome [46] and with ATP6 [47] and MTMR2 gene variants [48]. Recently, a dysfunction of the endoplasmic reticulum membrane protein complex (EMC), a conserved player in the process of membrane protein biogenesis, has been reported to play a role in the pathogenesis of certain congenital diseases such as cystic fibrosis, pigmentosus retinitis, and Charcot–Marie–Tooth disease [49]. The hypothesis is that these pathologies are caused by mutations within membrane proteins that require the EMC during their production [49]. The MORC2 VUS patient had no particular abnormal characteristics, with the exception of an increase in CSF protein level that initially led to a CIDP misdiagnosis. As this gene is considered to play a role in the development of the nervous system [28], it could be supposed that it may cause an alteration of the blood–brain barrier that could justify this finding. Moreover, the absence of temporal dispersion or conduction blocks in nerve conduction studies, the slowly progressive clinical picture, and the loss of improvement after adequate therapy (intravenous immunoglobulin) made the CIDP diagnosis very improbable. In the LITAF and GARS1 patients, we confirmed the presence of foot deformities in the first and a prominent distal upper limb involvement in the second. Peculiar was the phenotype of the two patients with the GDAP1 variant, who presented with proximal/asymmetric lower limb weakness, clinical signs of first motoneuron involvement, and optic and acoustic nerve disorders.
5. Conclusions
Expanding the spectrum of CMT phenotypes is of high relevance, especially as it allows identifying less common mutations that have a higher risk of remaining undiagnosed. A better knowledge of the clinical manifestation of these rare mutations could be crucial to correctly address genetic testing, in particular considering that NGS and WES are still not widespread, especially in some health systems. Moreover, now that a phase III clinical trial (PLEO-CMT) is available for CMT patients with a specific mutation (PMP22 duplication, CMT1A) [50], the necessity of reaching a genetic definition for most of the patients is even greater, as it may make them eligible for future experimentations.
Author Contributions
Conceptualization, L.G. and M.R.; methodology, L.G., A.M., M.F., F.T., G.M.F. and M.A.; investigation, L.G., M.R., C.R., A.T., A.M., F.T., G.M.F., M.A. and M.F.; data curation, L.G.; writing—original draft preparation, L.G.; writing—review and editing, M.R., C.R., A.T., A.M., F.T., G.M.F. and M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by Ethical Committee of the University Hospital of Messina; address: AOU “G.Martino,” via Consolare Valeria n. 1, 98125-Messina (ME), Italy (Approval Code: prot. 53, verbale n. 03/2014; approval date: 24 February 2014).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We thank Sofia Turturici for her collaboration.
Conflicts of Interest
Luca Gentile is a sub-investigator in clinical trials by Alnylam, Ionis, Takeda. He also reports travel grants from Kedrion and CSL Behring to attend scientific meetings and acknowledge speaker fees and consulting honoraria from Pfizer and Sobi. Massimo Russo acknowledges receiving speaker fees and consulting honoraria from Akcea and Alnylam and a travel grant from Pfizer. Anna Mazzeo is Principal Investigator in clinical trials by Alnylam and Ionis, sub-investigator in clinical trials by Alnylam, Ionis, Takeda. She also reports travel grants from Kedrion and CSL Behring to attend scientific meetings and acknowledges speaker fees and consulting honoraria from Alnylam, Akcea, and Pfizer. Antonio Toscano is Principal Investigator in clinical trials by Takeda and Genzyme. He acknowledges speaker fees and consulting honoraria from Kedrion, CSL Behring, and Genzyme. The other authors declare no conflict of interest.
Appendix A
Genetic analysis was performed by Next-Generation Sequencing (PGM Ion Torrent DX, Thermo Fisher Scientific, Waltham, MA, USA) using a custom gene panel.
The NGS custom gene panel included 44 genes (215 Kb; 772 amplicons) more frequently associated with AD or AR, axonal, demyelinating, or intermediate CMT. It is currently used by the Centre of Genetics that performed the analysis, with a theoretical coverage of 98.5%. The genes included in the panel were: ABCA1; ATP1A1; BAG3; BICD2; BSCL2; C12orf65; DHTKD1; DNM2; DYNC1H1; EGR2; FGD4; GARS; GDAP1; GJB1; HINT1; HSPB1; HSPB8; IGHMBP2; KIF5A; LITAF; MFN2; MORC2; MPZ; MTMR2; NDRG1; NEFL; OPA1; PMP2; PMP22; POLG; PRPS1; PRX; RAB7A; REEP1; SEPT9; SETX; SH3TC2; SIGMAR1; SPAST; TFG; TRPV4; TTR; TYMP; VCP.
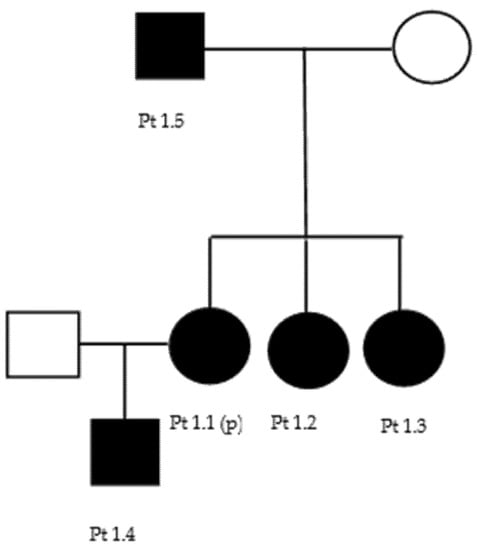
Figure A1.
Family 1 pedigree.
Figure A1.
Family 1 pedigree.
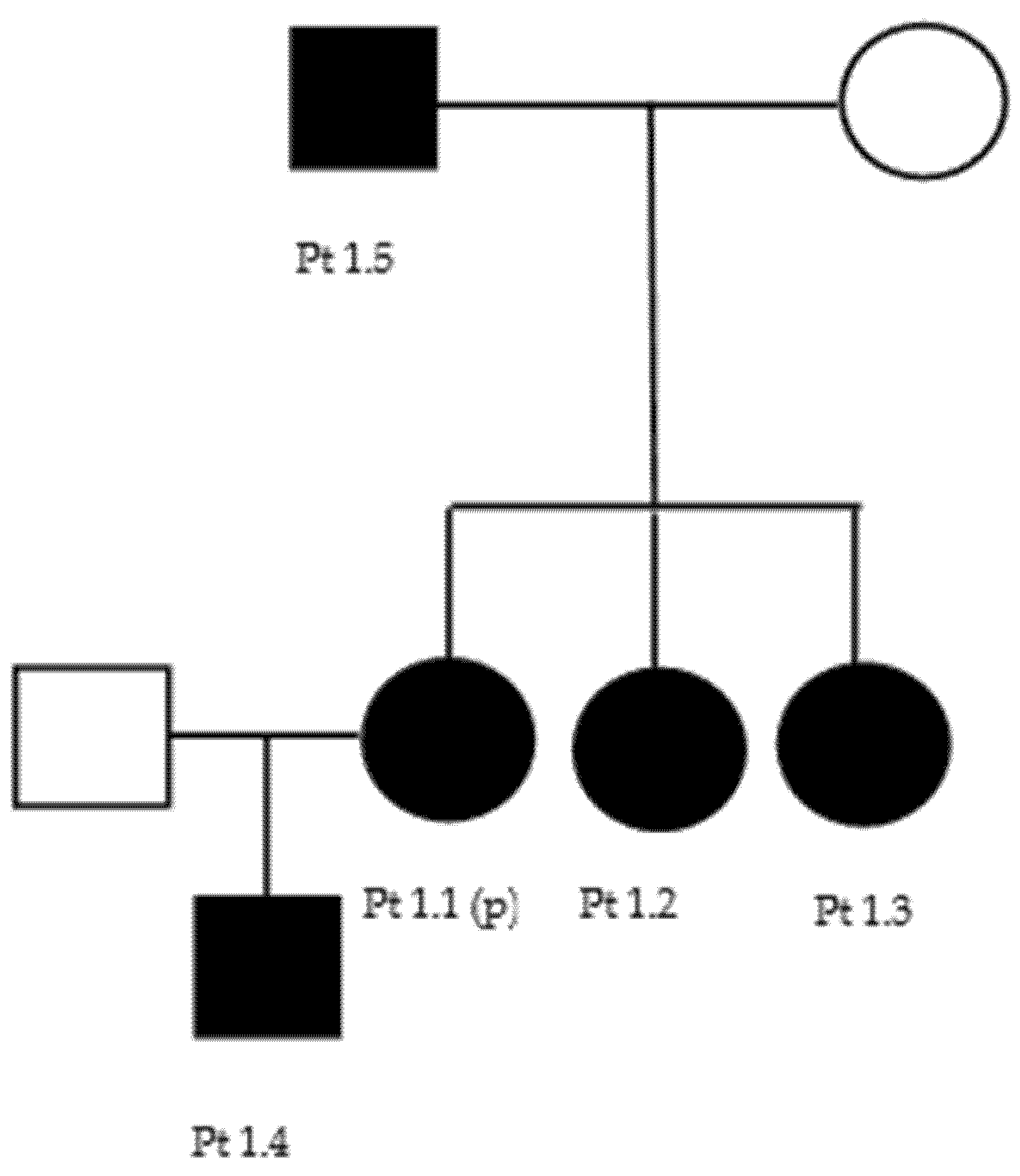
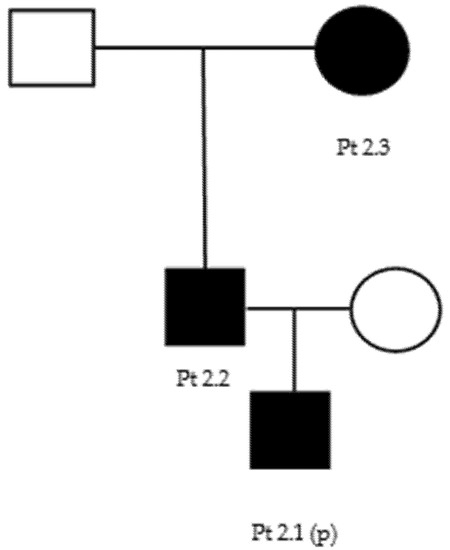
Figure A2.
Family 2 pedigree.
Figure A2.
Family 2 pedigree.
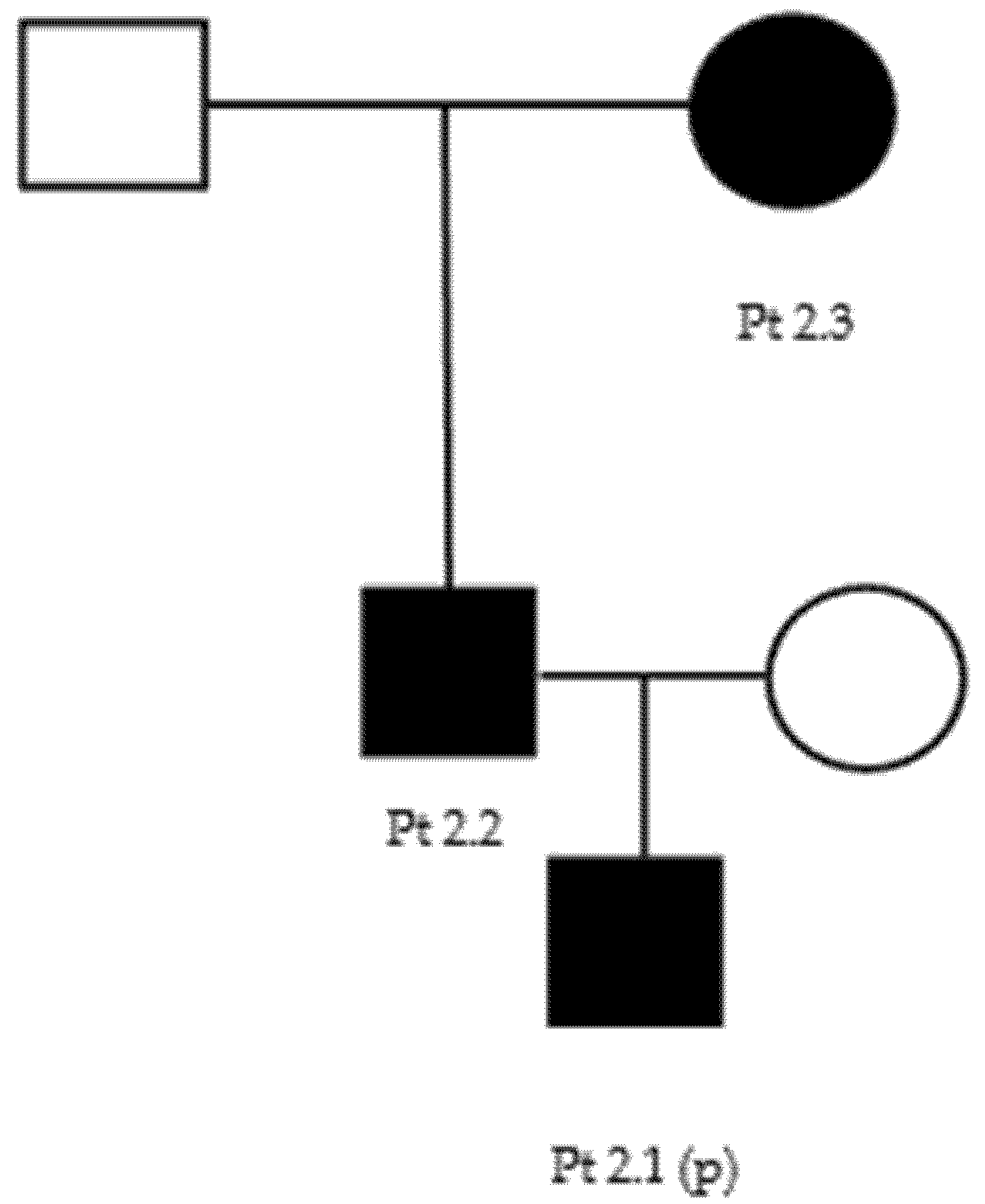
Figure A3.
Family 5 pedigree.
Figure A3.
Family 5 pedigree.
Figure A4.
Family 6 pedigree.
Figure A4.
Family 6 pedigree.
References
- Pareyson, D.; Saveri, P.; Pisciotta, C. New Developments in Charcot–Marie–Tooth Neuropathy and Related Diseases. Curr. Opin. Neurol. 2017, 30, 471–480. [Google Scholar] [CrossRef]
- Bienfait, H.M.E.; Baas, F.; Koelman, J.H.T.M.; de Haan, R.J.; van Engelen, B.G.M.; Gabreels-Festen, A.A.W.M.; Ongerboer de Visser, B.W.; Meggouh, F.; Weterman, M.A.J.; De Jonghe, P.; et al. Phenotype of Charcot-Marie-Tooth Disease Type 2. Neurology 2007, 68, 1658–1667. [Google Scholar] [CrossRef] [PubMed]
- Cardellini, D.; Zanette, G.; Taioli, F.; Bertolasi, L.; Ferrari, S.; Cavallaro, T.; Fabrizi, G.M. CIDP, CMT1B, or CMT1B plus CIDP? Neurol. Sci. 2021, 42, 1127–1130. [Google Scholar] [CrossRef]
- Mazzeo, A.; Stancanelli, C.; Russo, M.; Granata, F.; Gentile, L.; Di Leo, R.; Vita, G.; Nobile-Orazio, E.; Toscano, A. Subacute Inflammatory Demyelinating Polyneuropathy Disclosed by Massive Nerve Root Enhancement in CMT1A: Letter to the Editor. Muscle Nerve 2012, 45, 451–452. [Google Scholar] [CrossRef]
- Laurá, M.; Pipis, M.; Rossor, A.M.; Reilly, M.M. Charcot–Marie–Tooth Disease and Related Disorders: An Evolving Landscape. Curr. Opin. Neurol. 2019, 32, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.M.; Laura, M.; Fawcett, K.; Pandraud, A.; Liu, Y.-T.; Davidson, G.L.; Rossor, A.M.; Polke, J.M.; Castleman, V.; Manji, H.; et al. Charcot–Marie–Tooth Disease: Frequency of Genetic Subtypes and Guidelines for Genetic Testing. J. Neurol. Neurosurg. Psychiatry 2012, 83, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Saporta, A.S.D.; Sottile, S.L.; Miller, L.J.; Feely, S.M.E.; Siskind, C.E.; Shy, M.E. Charcot-Marie-Tooth Disease Subtypes and Genetic Testing Strategies. Ann. Neurol. 2011, 69, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Gess, B.; Schirmacher, A.; Boentert, M.; Young, P. Charcot-Marie-Tooth Disease: Frequency of Genetic Subtypes in a German Neuromuscular Center Population. Neuromuscul. Disord. 2013, 23, 647–651. [Google Scholar] [CrossRef]
- Stancanelli, C.; Taioli, F.; Testi, S.; Fabrizi, G.M.; Arena, M.G.; Granata, F.; Russo, M.; Gentile, L.; Vita, G.; Mazzeo, A. Unusual Features of Central Nervous System Involvement in CMTX Associated with a Novel Mutation of GJB1 Gene. J. Peripher. Nerv. Syst. 2012, 17, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Sivera, R.; Sevilla, T.; Vilchez, J.J.; Martinez-Rubio, D.; Chumillas, M.J.; Vazquez, J.F.; Muelas, N.; Bataller, L.; Millan, J.M.; Palau, F.; et al. Charcot-Marie-Tooth Disease: Genetic and Clinical Spectrum in a Spanish Clinical Series. Neurology 2013, 81, 1617–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manganelli, F.; Tozza, S.; Pisciotta, C.; Bellone, E.; Iodice, R.; Nolano, M.; Geroldi, A.; Capponi, S.; Mandich, P.; Santoro, L. Charcot-Marie-Tooth Disease: Frequency of Genetic Subtypes in a Southern Italy Population: Manganelli et Al. J. Peripher. Nerv. Syst. 2014, 19, 292–298. [Google Scholar] [CrossRef]
- Lorefice, L.; Murru, M.R.; Coghe, G.; Fenu, G.; Corongiu, D.; Frau, J.; Tranquilli, S.; Tacconi, P.; Vannelli, A.; Marrosu, G.; et al. Charcot–Marie–Tooth Disease: Genetic Subtypes in the Sardinian Population. Neurol. Sci. 2017, 38, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Gentile, L.; Russo, M.; Fabrizi, G.M.; Taioli, F.; Ferrarini, M.; Testi, S.; Alfonzo, A.; Aguennouz, M.; Toscano, A.; Vita, G.; et al. Charcot-Marie-Tooth Disease: Experience from a Large Italian Tertiary Neuromuscular Center. Neurol. Sci. 2020, 41, 1239–1243. [Google Scholar] [CrossRef]
- Stancanelli, C.; Fabrizi, G.M.; Ferrarini, M.; Cavallaro, T.; Taioli, F.; Di Leo, R.; Russo, M.; Gentile, L.; Toscano, A.; Vita, G.; et al. Charcot–Marie–Tooth 2F: Phenotypic Presentation of the Arg136Leu HSP27 Mutation in a Multigenerational Family. Neurol. Sci. 2015, 36, 1003–1006. [Google Scholar] [CrossRef] [PubMed]
- Ramchandren, S. Charcot-Marie-Tooth Disease and Other Genetic Polyneuropathies. Contin. Lifelong Learn. Neurol. 2017, 23, 1360–1377. [Google Scholar] [CrossRef] [PubMed]
- Rohkamm, B.; Reilly, M.M.; Lochmüller, H.; Schlotter-Weigel, B.; Barisic, N.; Schöls, L.; Nicholson, G.; Pareyson, D.; Laurà, M.; Janecke, A.R.; et al. Further Evidence for Genetic Heterogeneity of Distal HMN Type V, CMT2 with Predominant Hand Involvement and Silver Syndrome. J. Neurol. Sci. 2007, 263, 100–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Eulate, G.; Fernández-Torrón, R.; Guisasola, A.; Gaspar, M.T.I.; Diaz-Manera, J.; Maneiro, M.; Zulaica, M.; Olasagasti, V.; Formica, A.F.; Espinal, J.B.; et al. Phenotypic Correlations in a Large Single-center Cohort of Patients with BSCL2 Nerve Disorders: A Clinical, Neurophysiological and Muscle Magnetic Resonance Imaging Study. Eur. J. Neurol. 2020, 27, 1364–1373. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, S.; Okamoto, Y.; Tanabe, H.; Yoshimura, A.; Higuchi, Y.; Yuan, J.; Hashiguchi, A.; Ishiura, H.; Mitsui, J.; Suwazono, S.; et al. Clinical Features of Inherited Neuropathy with BSCL2 Mutations in Japan. J. Peripher. Nerv. Syst. 2020, 25, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Windpassinger, C.; Auer-Grumbach, M.; Irobi, J.; Patel, H.; Petek, E.; Hörl, G.; Malli, R.; Reed, J.A.; Dierick, I.; Verpoorten, N.; et al. Heterozygous Missense Mutations in BSCL2 Are Associated with Distal Hereditary Motor Neuropathy and Silver Syndrome. Nat. Genet. 2004, 36, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Zheng, R.; Luan, X.; Zhang, W.; Wang, Z.; Yuan, Y. Clincial and Pathological Study of Distal Motor Neuropathy with N88S Mutation in BSCL2. Neuropathology 2009, 29, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Ollivier, Y.; Magot, A.; Latour, P.; Perrier, J.; Mercier, S.; Maisonobe, T.; Péréon, Y. Clinical and Electrophysiological Features in a French Family Presenting with Seipinopathy. Neuromuscul. Disord. 2015, 25, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Cafforio, G.; Calabrese, R.; Morelli, N.; Mancuso, M.; Piazza, S.; Martinuzzi, A.; Bassi, M.T.; Crippa, F.; Siciliano, G. The First Italian Family with Evidence of Pyramidal Impairment as Phenotypic Manifestation of Silver Syndrome BSCL2 Gene Mutation. Neurol. Sci. 2008, 29, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.-O.; Park, M.-H.; Chung, K.W.; Woo, H.-M.; Koo, H.; Chung, H.-K.; Choi, K.-G.; Park, K.D.; Lee, H.J.; Hyun, Y.S.; et al. Clinical and Histopathological Study of Charcot-Marie-Tooth Neuropathy with a Novel S90W Mutation in BSCL2. Neurogenetics 2013, 14, 35–42. [Google Scholar] [CrossRef]
- Monteiro, A.; Real, R.; Nadais, G.; Silveira, F.; Leão, M. BSCL2 N88S Mutation in A Portuguese Patient with the Silver Syndrome. Muscle Nerve 2015, 51, 456–458. [Google Scholar] [CrossRef] [PubMed]
- Rakočević-Stojanović, V.; Milić-Rašić, V.; Perić, S.; Baets, J.; Timmerman, V.; Dierick, I.; Pavlović, S.; De Jonghe, P. N88S Mutation in the BSCL2 Gene in a Serbian Family with Distal Hereditary Motor Neuropathy Type V or Silver Syndrome. J. Neurol. Sci. 2010, 296, 107–109. [Google Scholar] [CrossRef]
- Sevilla, T.; Lupo, V.; Martínez-Rubio, D.; Sancho, P.; Sivera, R.; Chumillas, M.J.; García-Romero, M.; Pascual-Pascual, S.I.; Muelas, N.; Dopazo, J.; et al. Mutations in the MORC2 Gene Cause Axonal Charcot–Marie–Tooth Disease. Brain 2016, 139, 62–72. [Google Scholar] [CrossRef] [Green Version]
- Sancho, P.; Bartesaghi, L.; Miossec, O.; García-García, F.; Ramírez-Jiménez, L.; Siddell, A.; Åkesson, E.; Hedlund, E.; Laššuthová, P.; Pascual-Pascual, S.I.; et al. Characterization of Molecular Mechanisms Underlying the Axonal Charcot–Marie–Tooth Neuropathy Caused by MORC2 Mutations. Hum. Mol. Genet. 2019, 28, 1629–1644. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Okamoto, Y.; Yoshimura, A.; Yuan, J.-H.; Hiramatsu, Y.; Higuchi, Y.; Hashiguchi, A.; Mitsui, J.; Ishiura, H.; Fukumura, S.; et al. Clinical and Mutational Spectrum of Charcot–Marie–Tooth Disease Type 2Z Caused by MORC2 Variants in Japan. Eur. J. Neurol. 2017, 24, 1274–1282. [Google Scholar] [CrossRef]
- Peeters, K.; Chamova, T.; Tournev, I.; Jordanova, A. Axonal Neuropathy with Neuromyotonia: There Is a HINT. Brain 2016, 140, 868–877. [Google Scholar] [CrossRef] [Green Version]
- Shchagina, O.A.; Milovidova, T.B.; Murtazina, A.F.; Rudenskaya, G.E.; Nikitin, S.S.; Dadali, E.L.; Polyakov, A.V. HINT1 Gene Pathogenic Variants: The Most Common Cause of Recessive Hereditary Motor and Sensory Neuropathies in Russian Patients. Mol. Biol. Rep. 2020, 47, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Amor-Barris, S.; Høyer, H.; Brauteset, L.V.; De Vriendt, E.; Strand, L.; Jordanova, A.; Braathen, G.J.; Peeters, K. HINT1 Neuropathy in Norway: Clinical, Genetic and Functional Profiling. Orphanet J. Rare Dis. 2021, 16, 116. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Fu, J.; Lv, H.; Zhang, W.; Wang, Z.; Yuan, Y. Novel Mutations in HINT1 Gene Cause Autosomal Recessive Axonal Neuropathy with Neuromyotonia in Two Cases of Sensorimotor Neuropathy and One Case of Motor Neuropathy. Neuromuscul. Disord. 2018, 28, 646–651. [Google Scholar] [CrossRef]
- Scarpini, G.; Spagnoli, C.; Salerno, G.G.; Rizzi, S.; Frattini, D.; Fusco, C. Autosomal Recessive Axonal Neuropathy Caused by HINT1 Mutation: New Association of a Psychiatric Disorder to the Neurologic Phenotype. Neuromuscul. Disord. 2019, 29, 979. [Google Scholar] [CrossRef] [PubMed]
- Edgar, J.R.; Ho, A.K.; Laurá, M.; Horvath, R.; Reilly, M.M.; Luzio, J.P.; Roberts, R.C. A Dysfunctional Endolysosomal Pathway Common to Two Sub-Types of Demyelinating Charcot–Marie–Tooth Disease. Acta Neuropathol. Commun. 2020, 8, 165. [Google Scholar] [CrossRef] [PubMed]
- Ciotti, P.; Luigetti, M.; Geroldi, A.; Capponi, S.; Pezzini, I.; Gulli, R.; Pazzaglia, C.; Padua, L.; Massa, R.; Mandich, P.; et al. A Novel LITAF/SIMPLE Mutation within a Family with a Demyelinating Form of Charcot–Marie–Tooth Disease. J. Neurol. Sci. 2014, 343, 183–186. [Google Scholar] [CrossRef]
- Jerath, N.U.; Shy, M.E. Charcot-Marie-Tooth Disease Type 1C: Clinical and Electrophysiological Findings for the c.334G > A (p.Gly112Ser) Litaf/Simple Mutation: EDx, Clinical Findings in CMT1C. Muscle Nerve 2017, 56, 1092–1095. [Google Scholar] [CrossRef]
- Guimarães-Costa, R.; Iancu Ferfoglia, R.; Leonard-Louis, S.; Ziegler, F.; Magy, L.; Fournier, E.; Dubourg, O.; Bouche, P.; Maisonobe, T.; Lacour, A.; et al. Phenotypic Spectrum of Charcot−Marie−Tooth Disease Due to LITAF/SIMPLE Mutations: A Study of 18 Patients. Eur. J. Neurol. 2017, 24, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Vinogradova, E.S.; Nikonov, O.S.; Nikonova, E.Y. Associations between Neurological Diseases and Mutations in the Human Glycyl-TRNA Synthetase. Biochem. Mosc. 2021, 86, S12–S23. [Google Scholar] [CrossRef] [PubMed]
- Del Bo, R.; Locatelli, F.; Corti, S.; Scarlato, M.; Ghezzi, S.; Prelle, A.; Fagiolari, G.; Moggio, M.; Carpo, M.; Bresolin, N.; et al. Coexistence of CMT-2D and Distal SMA-V Phenotypes in an Italian Family with a GARS Gene Mutation. Neurology 2006, 66, 752–754. [Google Scholar] [CrossRef]
- Cantarero, L.; Juárez-Escoto, E.; Civera-Tregón, A.; Rodríguez-Sanz, M.; Roldán, M.; Benítez, R.; Hoenicka, J.; Palau, F. Mitochondria–Lysosome Membrane Contacts Are Defective in GDAP1-Related Charcot–Marie–Tooth Disease. Hum. Mol. Genet. 2021, 29, 3589–3605. [Google Scholar] [CrossRef]
- Pezzini, I.; Geroldi, A.; Capponi, S.; Gulli, R.; Schenone, A.; Grandis, M.; Doria-Lamba, L.; La Piana, C.; Cremonte, M.; Pisciotta, C.; et al. GDAP1 Mutations in Italian Axonal Charcot–Marie–Tooth Patients: Phenotypic Features and Clinical Course. Neuromuscul. Disord. 2016, 26, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Sivera, R.; Frasquet, M.; Lupo, V.; García-Sobrino, T.; Blanco-Arias, P.; Pardo, J.; Fernández-Torrón, R.; de Munain, A.L.; Márquez-Infante, C.; Villarreal, L.; et al. Distribution and Genotype-Phenotype Correlation of GDAP1 Mutations in Spain. Sci. Rep. 2017, 7, 6677. [Google Scholar] [CrossRef] [Green Version]
- Pakhrin, P.S.; Xie, Y.; Hu, Z.; Li, X.; Liu, L.; Huang, S.; Wang, B.; Yang, Z.; Zhang, J.; Liu, X.; et al. Genotype–Phenotype Correlation and Frequency of Distribution in a Cohort of Chinese Charcot–Marie–Tooth Patients Associated with GDAP1 Mutations. J. Neurol. 2018, 265, 637–646. [Google Scholar] [CrossRef]
- Kopanos, C.; Tsiolkas, V.; Kouris, A.; Chapple, C.E.; Albarca Aguilera, M.; Meyer, R.; Massouras, A. VarSome: The Human Genomic Variant Search Engine. Bioinformatics 2019, 35, 1978–1980. [Google Scholar] [CrossRef]
- Zimoń, M.; Baets, J.; Almeida-Souza, L.; De Vriendt, E.; Nikodinovic, J.; Parman, Y.; Battaloǧlu, E.; Matur, Z.; Guergueltcheva, V.; Tournev, I.; et al. Loss-of-Function Mutations in HINT1 Cause Axonal Neuropathy with Neuromyotonia. Nat. Genet. 2012, 44, 1080–1083. [Google Scholar] [CrossRef]
- Lerat, J.; Cintas, P.; Beauvais-Dzugan, H.; Magdelaine, C.; Sturtz, F.; Lia, A.-S. A Complex Homozygous Mutation in ABHD12 Responsible for PHARC Syndrome Discovered with NGS and Review of the Literature: A Complex Homozygous Mutation in ABHD12 Responsible. J. Peripher. Nerv. Syst. 2017, 22, 77–84. [Google Scholar] [CrossRef]
- Kabala, A.M.; Lasserre, J.-P.; Ackerman, S.H.; di Rago, J.-P.; Kucharczyk, R. Defining the Impact on Yeast ATP Synthase of Two Pathogenic Human Mitochondrial DNA Mutations, T9185C and T9191C. Biochimie 2014, 100, 200–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guimarães-Costa, R.; Villar-Quiles, R.-N.; Latour, P.; Sole, G.; Husson, I.; Lacour, A.; Leonard-Louis, S.; Stojkovic, T. Confounding Clinical Presentation and Different Disease Progression in CMT4B1. Neuromuscul. Disord. 2020, 30, 576–582. [Google Scholar] [CrossRef]
- Miller-Vedam, L.E.; Bräuning, B.; Popova, K.D.; Schirle Oakdale, N.T.; Bonnar, J.L.; Prabu, J.R.; Boydston, E.A.; Sevillano, N.; Shurtleff, M.J.; Stroud, R.M.; et al. Structural and Mechanistic Basis of the EMC-Dependent Biogenesis of Distinct Transmembrane Clients. ELife 2020, 9, e62611. [Google Scholar] [CrossRef] [PubMed]
- Vita, G.; Vita, G.L.; Stancanelli, C.; Gentile, L.; Russo, M.; Mazzeo, A. Genetic Neuromuscular Disorders: Living the Era of a Therapeutic Revolution. Part 1: Peripheral Neuropathies. Neurol. Sci. 2019, 40, 661–669. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).