1. Introduction
Diffusion tensor imaging (DTI) and DTI-based fiber tractography have become routine tools for estimating and visualizing the course, location, and extent of major white matter tracts, such as the corticospinal tract (CST), optic radiation (OR), and arcuate fascicle (AF), especially in neurosurgical applications. So far, the application of DTI and DTI-based fiber tractography has been shown to support the concept of maximized tumor volume resection, whilst preserving neurological functions, thereby contributing to low postoperative morbidity [
1,
2,
3,
4]. DTI-based fiber tractography allows well-estimated fiber bundle directions using common fiber tracking techniques and is still the most widely applied tractography method in the neurosurgical setting. However, there are fundamental limitations in accurately outlining major white matter tracts incorporating multi-fiber populations, and underestimating their spatial extent [
5,
6], thereby affecting the surgical decision on how to safely maximize the extent of resection.
There are several artifacts and pitfalls in diffusion weighted imaging (DWI)-based fiber tractography that one has to be aware of when applying and interpreting tractography results. These issues arise at different stages within the processing pipeline, ranging from data acquisition to visualization. The most commonly used imaging technique, echo planar imaging, itself has various artifacts such as head bulk motion and eddy currents [
7] or susceptibility artifacts [
8,
9,
10], physiological motion [
11,
12], partial volume effects due to typical low spatial resolution [
13], or a low signal-to-noise ratio [
14]. Besides the application of various fiber tractography algorithms and visualization techniques, the most crucial part, however, remains the mathematical description of the diffusion properties within each voxel. Routinely, and especially in the clinical context, a second-order tensor model (DTI) is used under the assumption of Gaussian distribution of water molecules, thus regularly failing in resolving crossing/kissing/fanning fibers [
15,
16] as well as complex fiber architectures due to the estimation of only a single diffusion direction within each voxel. Further complex and sophisticated methods of modeling diffusion properties exist, based on single- or multi-shell high-angular resolution diffusion imaging (HARDI) acquisition techniques [
17,
18], applying different models such as Q-ball imaging [
19], diffusion spectrum imaging (DSI) [
20], or compressed sensing techniques [
21,
22,
23]. In most cases, these further complex techniques coincide with longer acquisition times, which makes them unsuitable for routine clinical applications [
18].
Even though there are various modern and sophisticated methods available in basic neuroscience for reconstructing major white matter tracts in neurosurgical procedures, there is somehow a delay of integration of these methods, which might be due to complexity and time-consuming data acquisition or processing pipelines.
Diffusion kurtosis imaging (DKI), as an extension of DTI, enables the estimation of the diffusion tensor and the kurtosis tensor to characterize additional non-Gaussian diffusion properties within complex biological tissues such as white matter [
24,
25,
26]. Kurtosis describes the peakedness of the probability distribution in comparison to the Gaussian distribution [
27]. The estimation of the diffusion orientation distribution function (dODF) using both tensors, diffusion and kurtosis, is one alternative approach to resolve crossing fibers and to overcome the specific limitation of DTI-based approaches [
26,
28,
29,
30]. DKI typically makes use of an additional high b-value of about 2000 s/mm
2, thereby always enabling an estimation of the diffusion tensor and associated metrics such as fractional anisotropy (FA). Given this prerequisite, DKI might be further useful for clinical applications considering scanning time and derived parameters of interest.
Even though it is clinically applicable, so far, DKI has not been widely investigated in neurosurgical applications. In recent neuro-oncological and neurosurgical applications, DKI has mostly been evaluated for its capability of glioma grading and differentiation of gliomas from other intra-axial brain tumors [
31,
32,
33,
34], its role in molecular profiling such as its correlation with IDH1/2 mutations, ATRX or Ki-67 expression [
33,
35], its potential as a biomarker [
36], or its capability of detecting microstructural changes related to white matter alterations [
37,
38,
39]. One study used DKI for survival prediction in glioma patients by investigating the mean kurtosis as the relevant parameter [
40].
Up to now, DKI-based fiber tractography of major white matter tracts, particularly in neurosurgical applications, has been rarely investigated. In a study by Glenn et al., data of five healthy volunteers were evaluated with respect to different acquisition schemes focusing on crossing fibers [
41]. Another study by Leote et al. analyzed DKI data in a group of nine patients, showing more voluminous fiber tractography results of the CST using DKI and demonstrating the feasibility of CST visualization in healthy volunteers and a small group (n = 3) of astrocytoma patients [
42,
43]. Another study investigated three healthy volunteers for fiber tractography along the internal capsule and corpus callosum, showing improved fiber-crossing resolution [
44].
As there is still a lack of integration of sophisticated fiber tractography approaches in neurosurgical practice, DKI itself seems to be a clinically applicable and easy-to-use method, while also gaining information for standard DTI analysis. The rare previous studies only investigated initial results on tractography of the CST in glioma patients as the most widely examined white matter tract. Other neurosurgically relevant major white matter tracts such as the arcuate fascicle, associated with language processing, and optic radiation, of special interest in temporal lobe and epilepsy surgery, with several challenges in tractography algorithms were not included in those studies. Up to now, there is no gold standard available providing guidance on a suitable acquisition, model, reconstruction algorithm, and visualization that should be used for different kinds of white matter tracts.
In this study, the effect of DKI- vs. DTI-based fiber tractography of three neurosurgically relevant major white matter tracts, with different demands on the tract reconstruction, the CST, OR, and the AF, was analyzed. Analyses were performed in healthy volunteers as well as in glioma patients, specifically challenging tractography due to altered physiology (infiltration, edema), with respect to tract volume and visualization capabilities in order to evaluate DKI’s potential to support the application of fiber tractography of neurosurgically relevant white matter tracts under clinical time constraints in contrast to DTI.
4. Discussion
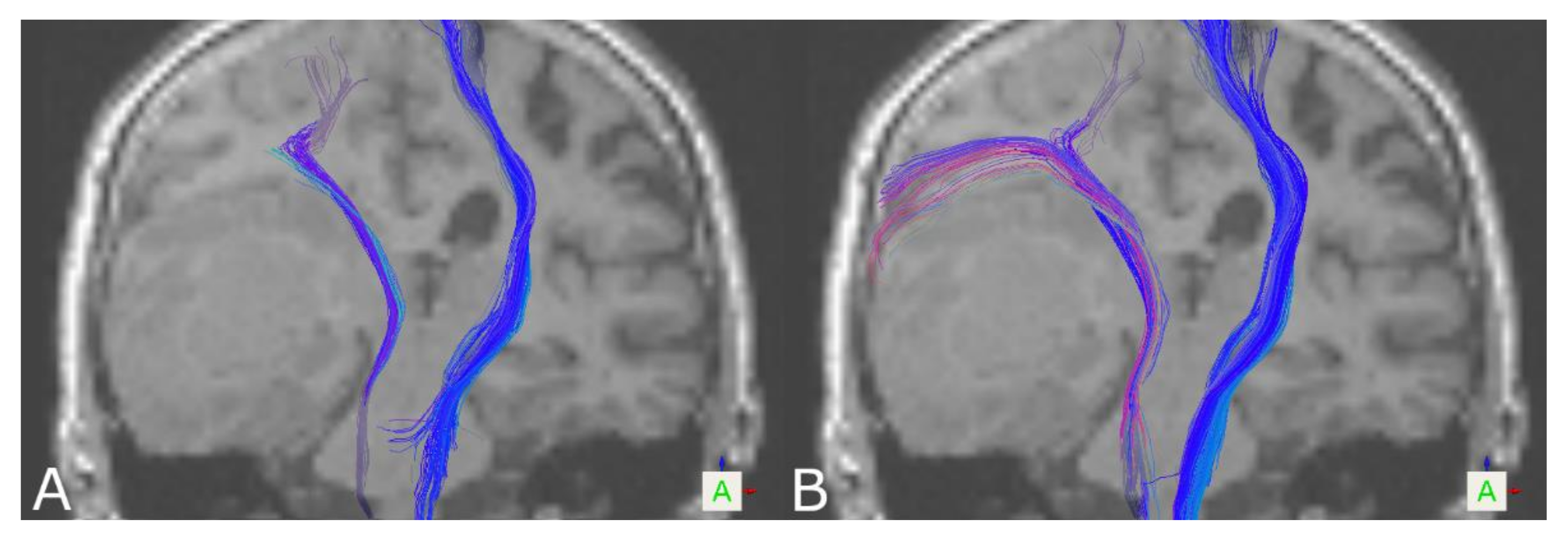
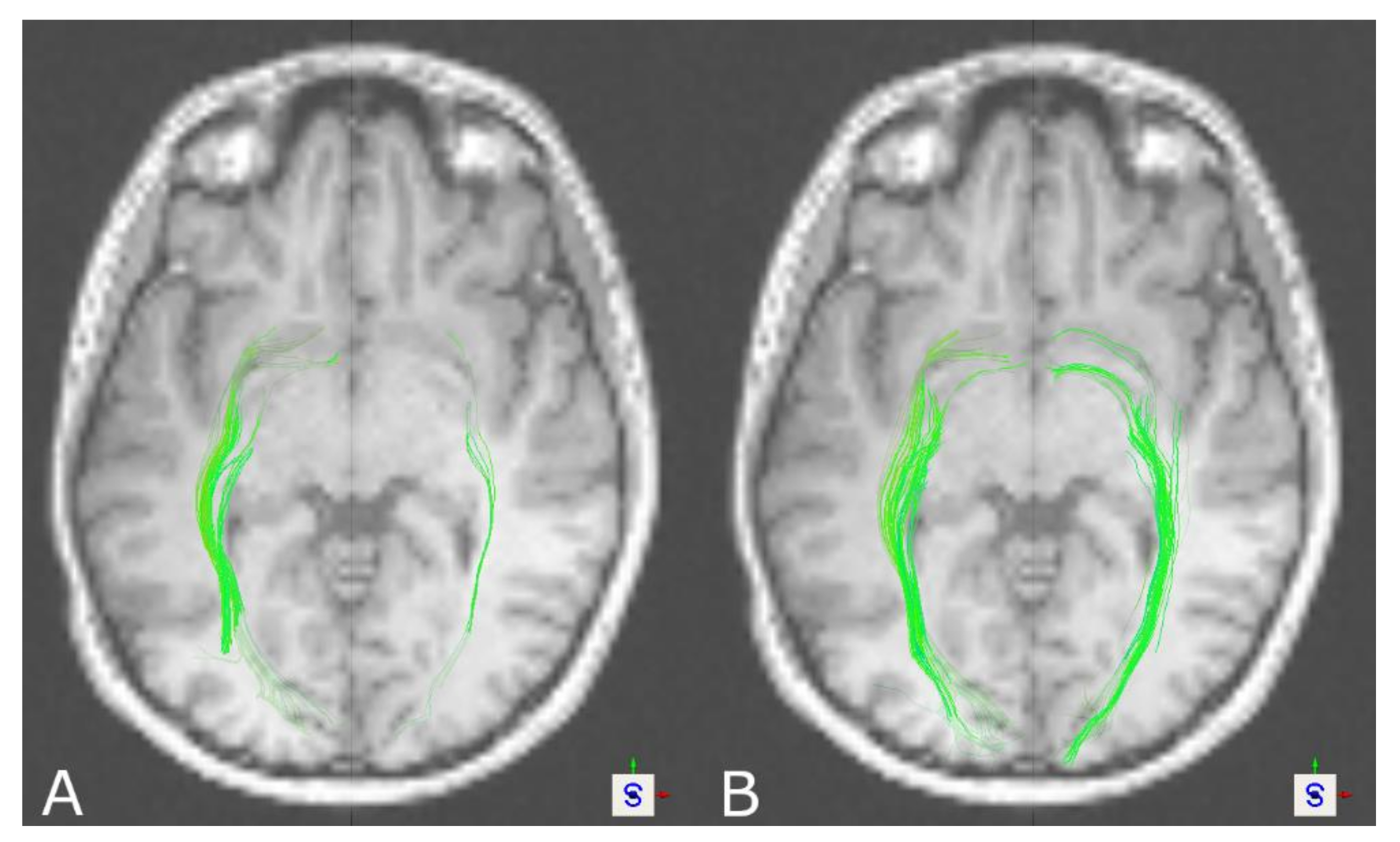
Tractography of the CST led to significantly larger tract volumes based on DKI in healthy volunteers and patients. On visual inspection of the results, reconstructions seemed more solid and compact based on DKI, which was also seen regarding tract density. Additionally, DKI-based reconstructions in contrast to DTI-based reconstructions were frequently capable of reaching a broader part of the motor cortex, in some cases connecting also to the lateral part of the motor cortex. In addition, in the case of the OR in healthy volunteers, significantly larger tract volumes were seen in DKI-based tractography. Similarly, this was seen in patients for the left, but not the right, OR. In the case of the AF, the results seem to be the opposite. Larger tract volumes, even though not significant in healthy volunteers, were seen in favor of DTI-based tractography, also going along with further neuroanatomically plausible reconstructions. Due to a lack of ground truth data to compare against for verification of the results, besides the tract volume as one of the most commonly used measures of comparing tractography results between groups or algorithms to interpret the results, tract reconstructions were assessed visually, underpinned by a measure of tract density at a representative localization.
There is a general consensus for further sophisticated methods to be applied for reconstruction and visualization of major white matter tracts in order to overcome the limitations of the routinely used DTI model [
5,
67,
68]. Several approaches exist to define which model and method to use in which scenario, and various approaches have been compared [
69,
70,
71,
72], notably showing, so far, the weakest results for DTI-based methods. Most methods therefore rely on extensive acquisition times (e.g., single-/multi-shell HARDI data) to generate complex data sets [
72,
73] not suitable for clinical use. DKI only extends DTI using an additional high b-value, approximately doubling the required acquisition time. Even though HARDI acquisition is also possible for DKI, the use of 30 directions is recommended to estimate sufficient DKI metrics at shorter acquisition times [
41,
74]. However, DKI is usually not included in these comparative studies, even though DKI extends the DTI model using kurtosis to model non-Gaussian diffusion properties.
Whereas most studies focus on DKI’s capability of detecting pathological alterations more precisely than by using DTI, studies including DKI-based tractography are, so far, rare. Leote et al. investigated DKI-based fiber tractography based on 1.5 T MRI data, not being evaluated before, for reconstructions of the CST in eight healthy volunteers as well as three glioma patients [
42]. No difference between tract sizes of patients and healthy volunteers was seen, but no comparison of DTI- and DKI-based tractography regarding tract sizes was performed. In another study, Leote et al. compared DTI- and DKI-based fiber tractography of the CST in nine patients with space-occupying lesions [
43]. Overall, more voluminous fiber tracts were seen based on DKI, as well as curvilinear fibers above the lesion not visible based on DTI in five cases, underpinning the findings of the present study. Another study compared tractography and analyzed the number of streamlines within the corpus callosum and internal capsule and showed improved fiber-crossing resolution in all three healthy subjects in the case of the corpus callosum but not of the internal capsule [
44]. Glenn et al. compared DTI, DKI, and DSI data in three healthy volunteers [
75], with a major focus on the methods’ capability of resolving complex fiber microarchitecture rather than tractography results. They showed that DKI enables the detection of crossing fibers, resulting in pronounced improvements compared to DTI. Results also indicated comparable results across DKI and DSI data, suggesting DKI can be used in a clinical setting due to reduced acquisition times. Results of DKI-based tractography regarding tract volumes of the CST are in line with the previous literature, whereas DKI-based tractography on the AF and OR is not reported so far.
Fiber tractography of the OR is notoriously challenging due to its neuroanatomical complexity, low fiber density, sharp curvature, high variability, and fan-like structure [
76,
77,
78]. In addition, the temporal stem contains multiple fibers impacting accurate delineation from each other [
79,
80,
81], and some technical aspects such as low spatial resolution, low signal-to-noise ratio, and susceptibility artifacts might compromise tractography of the OR [
78]. As previously reported, DTI-based reconstructions of the OR often suffer from inaccuracies, with several levels of success of tractography [
82,
83]. Neto Henriques et al. showed the potential of DKI to resolve fiber crossings of variable angulation in contrast to DTI. Therefore, complex fiber architectures such as the OR should also be resolved more adequately using DKI [
30]. This seems to be in concordance with the findings of this study, where at least more solid and compact reconstructions were seen using DKI compared to further sparse representations given by the DTI-based approach, which was also seen in significantly larger tract volumes and tract density in healthy volunteers (left and right OR). However, in patients, analogous results regarding tract volume were only seen for the left but not the right hemisphere. This might be caused by the study cohort that included cases with tumors especially affecting this tract and thereby possibly lowering the effect. Brain tumors cause histological distortion and increase microstructure complexity [
24]. Leote et al. postulated in the case of the CST that especially in regions affected by a brain tumor, DTI metrics are more affected than DKI metrics, leading to the hypothesis that DKI-based tractography is more suitable to characterize the underlying microstructure [
42].
Surprisingly, in the case of the AF, larger tract volumes were seen in favor of DTI-based tractography yielding no significant differences in healthy volunteers but in patients. In DKI-based fiber tractography, reconstructions often stopped early and frequently did not connect the ROIs properly. With a lack of other studies on DKI-based tractography of the AF, results can be explained only speculatively. Neto Henriques et al. analyzed the 3D geometry of the diffusion kurtosis tensor and proposed that tractography results might depend on the orientation of the fiber bundle and its curvature. Ascending fibers seem to follow more concave and convex pathways and should reflect small fanning angles to be better resolved by DKI-based approaches [
30], which might not be the case for the AF, with its close relation to other language-related tracts, such as the superior longitudinal fascicle. Lazar et al. hypothesized that with the increasing number of fiber directions, especially almost perpendicular crossings can be resolved better than crossings with small angles [
26]. In the case of the AF with other tracts running nearby with similar fiber directions, visualizing those tracts might be affected. In this way, DKI-based tractography might not be suitable for the AF. This might also be in line with results reported by Loucao et al., who compared DTI- and DKI-based tractography in different ROIs and showed opposed results in favor of DTI or DKI [
44], or results reported by Neto Henriques et al., who compared the kurtosis tensor vs. DKI-based tractography, leading to opposed results in different regions (corpus callosum, internal capsule) [
30]. This also supports the above-mentioned idea on defining which model and method to use in which scenario in order to find the best-fitting approach for every patient [
69,
70,
71,
72].
Even though DKI-based tractography of the CST and OR seems to possibly overcome some drawbacks of the DTI-based approach, tract appearance (visual inspection regarding fanning/curvature, tract density) varied across the cases, e.g., not all cases showing fanning within the motor cortex in healthy volunteers and patients. Besides tract-specific demands on tractography algorithms, there might also be subject-specific challenges in the tractography approach, such as decreased/altered white matter integrity related to pathological conditions (tumor, edema) or aging (reduced FA [
84]), as patients in this retrospective study were significantly older than the cohort of heathy volunteers. In addition, post-processing-related issues could be considered, such as artifacts and registration inaccuracies. In the case of the AF, contrary to the CST and OR, DKI seems to be even less capable of resolving the AF, while the DTI-based approach in these cases leads to plausible results. This even further supports the idea of individualized approaches depending on the specific subject’s and tract’s demands and incorporating shortcomings of image processing steps. Even though not for all tracts, DKI seems to be one possible approach to overcoming some drawbacks of DTI under clinical time constraints, worthy to be further investigated for specific white matter tracts, such as the CST and OR, while other approaches need to be investigated for other tracts such as the AF.
However, there is a need for approaches considering not only physiological challenges but also clinical constraints (compliance, short acquisition times). Considering various sophisticated approaches already available in basic neuroscience, there is still a delay of integration in neurosurgical procedures, mainly due to time-consuming data acquisition and complex processing pipelines. DKI, however, still provides short acquisition times, easily being integrated in the clinical workflow, and working as an extension of DTI, it still provides an estimation of the diffusion tensor and DTI-associated metrics used in routine clinical practice. Supported by the results of this study, especially in case of the CST but also the OR, DKI seems to support the neuroanatomically plausible visualization of fiber tract resection, even when DTI only leads to sparse reconstruction or even fails to provide plausible reconstructions at all, and could thereby be a valuable complement to DTI-based tractography.
So far, there is no real general gold standard for acquisition, parameter definition, or post-processing pipelines (post-processing, model, tractography algorithm, visualization, etc.) for the analysis of DWI data and fiber tractography. In this way, for example, even scanner manufacturer, field strength, and MR acquisition parameters influence DTI-derived parameters that are used for fiber tractography, such as scan repetitions, choice of the maximum b-value, number of diffusion-encoding gradients, the gradient-sampling scheme, image resolution, and echo and repetition times [
85], and have to be kept in mind when analyzing and interpreting study results. Another important general issue arises from the use of the b-matrix, usually automatically generated by the scanning system. These typically do not consider, e.g., imaging gradient effects and coupling of imaging and diffusion gradients and provide constant b-matrix values across the whole imaging volume, leading to systematic errors, as previously described by Borkowski et al. [
86] and Krzyzak et al. [
87]. In those studies, a new approach called b-matrix spatial distribution in DTI (BSD-DTI) was presented investigating an anisotropic phantom with ground truth knowledge of spatial distribution of the diffusion tensor to gain information about the voxel-by-voxel spatial dependence of the b-matrix, independent of sequence-specific parameters. Comparing the application of the traditional scanner-related b-matrix and the BSD-DTI-based b-matrix, systematic intra- and interslice deviations are seen, leading to a more accurate determination of diffusion coefficients as well as the orientation of the diffusion tensor, thereby also affecting DTI-based parameters and related fiber tractography results. Even though only applied in some recent studies [
88,
89], applying a BSD-DTI phantom-based approach to accurately defining the b-matrix and therefore also to more accurately estimating the diffusion tensor characteristics and related information could, in general, be considered to reduce uncertainty within the data.
However, certain limitations of the study should be mentioned that should be addressed in further investigations to support and broadly quantify these findings. First, limitations could be found in DWI data themselves, such as low spatial resolution, reduced signal-to-noise ratio, and artifacts due to susceptibility or pulsation, that might be accounted for to reduce physiological and physical bias. For example, a higher TE due to an increased maximum b-value, as used here, in comparison to acquisition of a standard DTI data set (maximum b-value of 1000 s/mm
2) might lead to a lower signal-to-noise ratio and increased susceptibility and distortion artifacts and thereby also might affect scalar parameters such as the FA, typically used for fiber tractography [
85,
90,
91]. Non-linear geometric distortions, for example, could be addressed as they are supposed to affect the tractography of all three tracts, which can be accounted for by acquisition of additional DWI data with an inverse phase encoding direction. Additionally, the patient cohort was heterogeneous due to the location of the space-occupying lesion, with tracts variably being affected by a tumor or not. In addition, in this retrospective study, age significantly varied between healthy volunteers and patients, affecting diffusion parameters, even though no direct comparison was performed. Finally, there was a lack of a true gold standard to verify and validate fiber tractography, as tract volume, tract density, and tract appearance, not yielding immediate quantitative information on anatomical correctness. To validate the results, phantom studies (simulation or hardware model) or ex vivo specimens (e.g., postmortem MRI and dissection) can be used [
92], but nevertheless, the application and evaluation in vivo needs to be further investigated, for example, using intrasurgical mapping techniques in a larger cohort of patients.
5. Conclusions
In this study, DKI- and DTI-based fiber tractography of three major white matter tracts, the CST, OR, and AF, was investigated in healthy volunteers and glioma patients to evaluate the potential of DKI to overcome limitations of DTI-based fiber tractography, often underestimating the spatial extent of major white matter tracts. The resulting fiber tracts were inspected visually due to neuroanatomical plausibility and appearance, as well as objectively compared using tract volume and fiber density.
In the case of the CST, DKI-based tractography led to more solid and compound tracts with a larger tract volume, also, in part, being capable of visualizing fibers connecting to the lateral motor cortex. Even in the absence of comparable studies in the case of the OR, our results are also in line with the theory of DKI’s capability to resolve multi-fiber populations, especially of tracts crossing more or less perpendicularly, leading to enhanced tract visualization based on DKI. For the AF, inverse results were found, with DTI-based fiber tractography seeming to be comparable or even more plausible than DKI-based tractography according to visual inspection and tract volume. Particularly in patients, this effect is more considerable. As DKI-based fiber tractography of the AF has not been investigated so far, one can only speculate that DKI might be compromised in cases of multi-fiber populations crossing in small angles and in cases of strong curvature, such as for the AF.
These results (solid and compact vs. sparse reconstructions, along with larger tract volumes) indicate that DKI-based tractography possesses the potential to contribute to improved fiber tractography of the CST and OR in routine clinical practice, especially under clinical time constraints, compared to DTI but needs to be further investigated and evaluated in clinical applications (e.g., intraoperative stimulation for verification). However, for the AF, alternative approaches need to be explored to overcome the limitations of DTI-based fiber tractography, supporting the general consensus to define specific models and methods for application of single tract reconstructions to optimize white matter tract visualization. Nevertheless, DKI seems to be a promising method, complementary to DTI, to provide robust visualization of selected major white matter tracts such as the CST and OR.


 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}