
Impact of Moderate Individually Tailored Physical Activity in Multiple Sclerosis Patients with Fatigue on Functional, Cognitive, Emotional State, and Postural Stability




Abstract
:1. Introduction
2. Materials and Methods
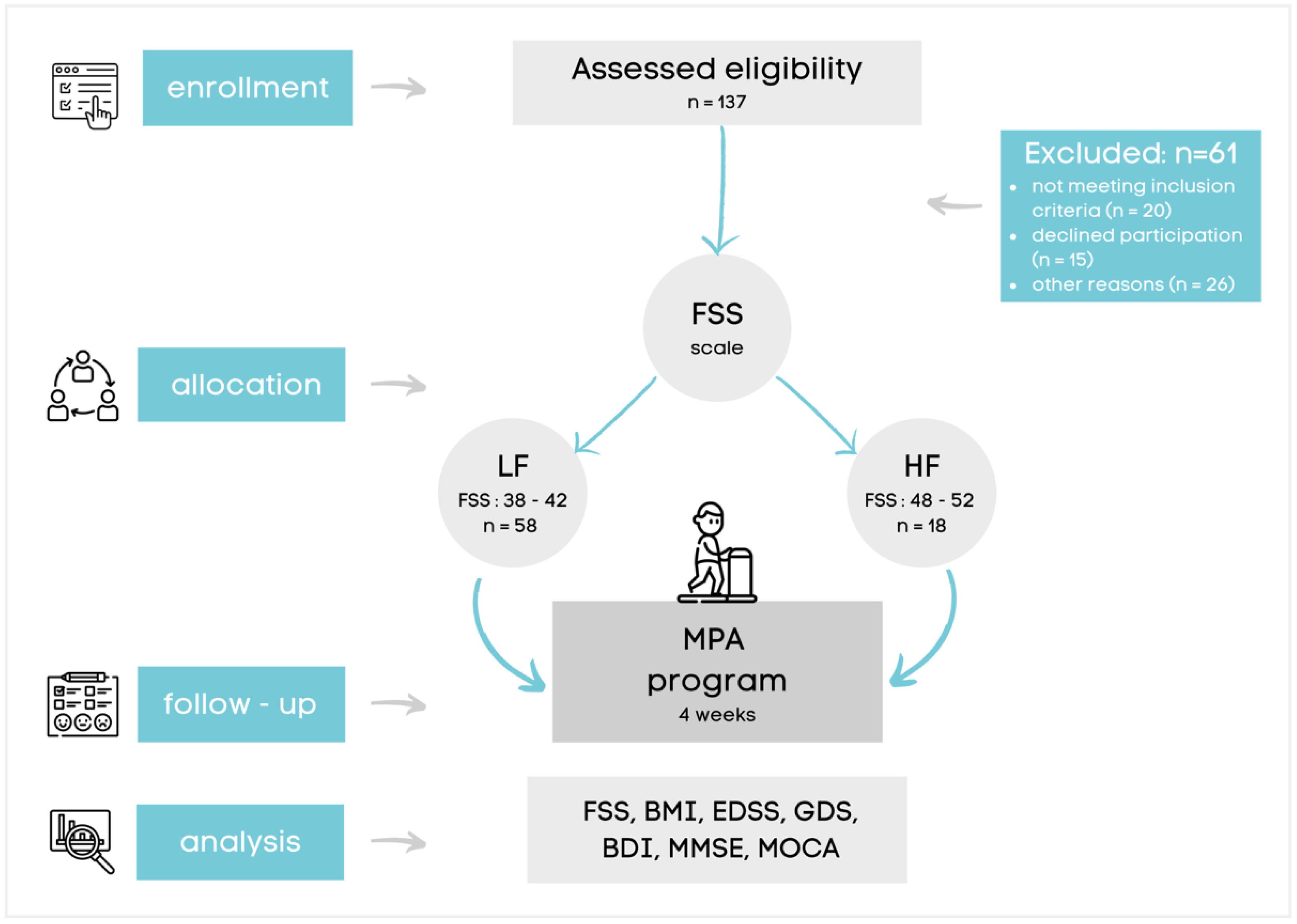
2.1. Participants
2.2. Clinical Scales
2.3. Stabilometric Assessment
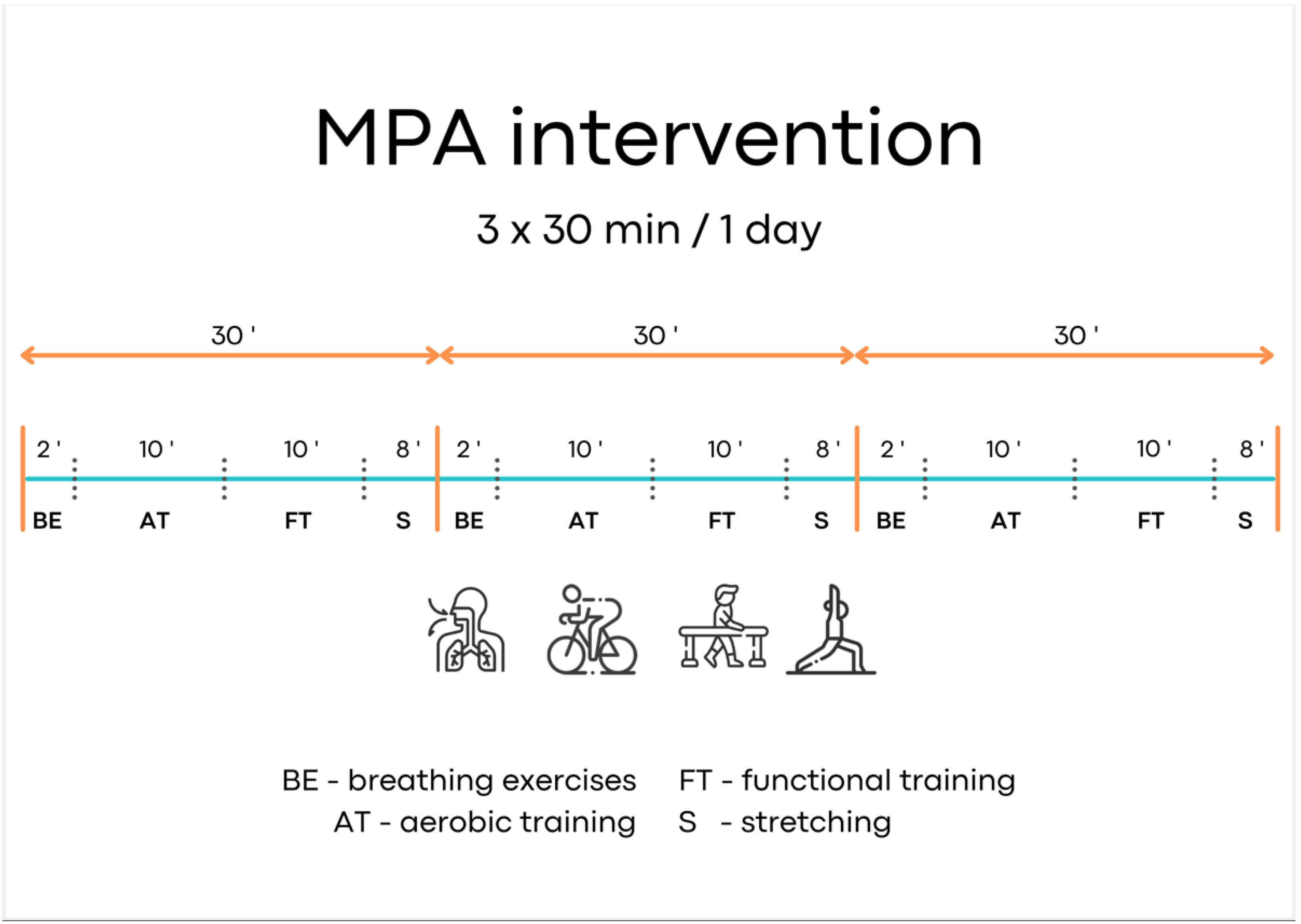
2.4. Moderate Physical Activity (MPA)
2.5. Statistical Analysis
3. Results
3.1. MPA and Emotional Status
3.2. MPA and Cognitive Function
3.3. MPA and Functional State
3.4. MPA and Stabilometric Evaluation
3.5. Spearman Correlation
4. Discussion
5. Limitations and Strengths of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Miller, E. Multiple sclerosis. Adv. Exp. Med. Biol. 2012, 724, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Giovannoni, G. Multiple sclerosis related fatigue. J. Neurol. Neurosurg. Psychiatry 2006, 77, 2–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christogianni, A.; Bibb, R.; Davis, S.L.; Jay, O.; Barnett, M.; Evangelou, N.; Filingeri, D. Temperature sensitivity in multiple sclerosis: An overview of its impact on sensory and cognitive symptoms. Temperature 2018, 5, 208–223. [Google Scholar] [CrossRef] [PubMed]
- Igra, M.S.; Paling, D.; Wattjes, M.P.; Connolly, D.J.A.; Hoggard, N. Multiple sclerosis update: Use of MRI for early diagnosis, disease monitoring and assessment of treatment related complications. Br. J. Radiol. 2017, 90, 20160721. [Google Scholar] [CrossRef]
- Manjaly, Z.M.; Harrison, N.A.; Critchley, H.D.; Do, C.T.; Stefanics, G.; Wenderoth, N.; Lutterotti, A.; Müller, A.; Stephan, K.E. Pathophysiological and cognitive mechanisms of fatigue in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Braley, T.J.; Chervin, R.D. Fatigue in multiple sclerosis: Mechanisms, evaluation, and treatment. Sleep 2010, 33, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Rammohan, K.W.; Lynn, D.J. Modafinil for fatigue in MS: A randomized placebo-controlled double-blind study. Neurology 2005, 65, 1995–1997. [Google Scholar]
- Miller, E.; Kostka, J.; Włodarczyk, T.; Dugué, B. Whole-body cryostimulation (cryotherapy) provides benefits for fatigue and functional status in multiple sclerosis patients. A case-control study. Acta Neurol. Scand. 2016, 134, 420–426. [Google Scholar] [CrossRef]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef] [PubMed]
- Pilutti, L.A.; Greenlee, T.A.; Motl, R.W.; Nickrent, M.S.; Petruzzello, S.J. Effects of exercise training on fatigue in multiple sclerosis: A meta-analysis. Psychosom. Med. 2013, 75, 575–580. [Google Scholar] [CrossRef] [PubMed]
- National Multiple Sclerosis Society: Exercise and Physical Activity Recommendations for ALL People with MS: Guidelines and Videos Available. Available online: https://www.nationalmssociety.org/About-the-Society/News/Exercise-and-Physical-Activity-Recommendations-for (accessed on 11 August 2021).
- Broch, L.; Simonsen, C.S.; Flemmen, H.; Berg-Hansen, P.; Skardhamar, Å.; Ormstad, H.; Celius, E.G. High prevalence of fatigue in contemporary patients with multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2021, 7, 2055217321999826. [Google Scholar] [CrossRef] [PubMed]
- Flachenecker, P.; Kümpfel, T.; Kallmann, B.; Gottschalk, M.; Grauer, O.; Rieckmann, P.; Trenkwalder, C.; Toyka, K.V. Fatigue in multiple sclerosis: A comparison of different rating scales and correlation to clinical parameters. Mult. Scler. 2002, 8, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, J.L.; Fan, Y.C.; Huang, Y.L.; Wang, J.; Chen, W.H.; Chiu, H.C.; Bai, C.H. Improved predictive ability of the Montreal Cognitive Assessment for diagnosing dementia in a community-based study. Alzheimers Res. Ther. 2015, 7, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pottie, K.; Rahal, R.; Jaramillo, A.; Birtwhistle, R.; Thombs, B.D.; Singh, H.; Gorber, S.C.; Dunfield, L.; Shane, A.; Bacchus, M.; et al. Recommendations on screening for cognitive impairment in older adults. CMAJ 2016, 188, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, Y.; Sato, N.; Ota, M.; Maikusa, N.; Maekawa, T.; Sone, D.; Enokizono, M.; Sugiyama, A.; Imabayashi, E.; Matsuda, H.; et al. A structural MRI study of cholinergic pathways and cognition in multiple sclerosis. eNeurologicalSci 2017, 8, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Hind, D.; Kaklamanou, D.; Beever, D.; Webster, R.; Lee, E.; Barkham, M.; Cooper, C. The assessment of depression in people with multiple sclerosis: A systematic review of psychometric validation studies. BMC Psychiatry 2016, 16, 278. [Google Scholar] [CrossRef] [Green Version]
- Kawahara, Y.; Ikeda, M.; Deguchi, K.; Hishikawa, N.; Kono, S.; Omote, Y.; Matsuzono, K.; Yamashita, T.; Ikeda, Y.; Abe, K. Cognitive and affective assessments of multiple sclerosis (MS) and neuromyelitis optica (NMO) patients utilizing computerized touch panel-type screening tests. Intern. Med. 2014, 53, 2281–2290. [Google Scholar] [CrossRef] [Green Version]
- Coquart, J.B.; Tourny-Chollet, C.; Lemaître, F.; Lemaire, C.; Grosbois, J.M.; Garcin, M. Relevance of the measure of perceived exertion for the rehabilitation of obese patients. Ann. Phys. Rehabil. Med. 2012, 55, 623–640. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.H.; Wylie, G.R.; Sandroff, B.M.; Dacosta-Aguayo, R.; DeLuca, J.; Genova, H.M. Neural mechanisms underlying state mental fatigue in multiple sclerosis: A pilot study. J. Neurol. 2020, 267, 2372–2382. [Google Scholar] [CrossRef]
- Zielińska-Nowak, E.; Włodarczyk, L.; Kostka, J.; Miller, E. New Strategies for Rehabilitation and Pharmacological Treatment of Fatigue Syndrome in Multiple Sclerosis. J. Clin. Med. 2020, 9, 3592. [Google Scholar] [CrossRef] [PubMed]
- Kargarfard, M.; Shariat, A.; Ingle, L.; Cleland, J.A.; Kargarfard, M. Randomized Controlled Trial to Examine the Impact of Aquatic Exercise Training on Functional Capacity, Balance, and Perceptions of Fatigue in Female Patients With Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2018, 99, 234–241. [Google Scholar] [CrossRef] [PubMed]
- McCullagh, R.; Fitzgerald, A.P.; Murphy, R.P.; Cooke, G. Long-term benefits of exercising on quality of life and fatigue in multiple sclerosis patients with mild disability: A pilot study. Clin. Rehabil. 2008, 22, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Giesser, B.S. Exercise in the management of persons with multiple sclerosis. Ther. Adv. Neurol. Disord. 2015, 8, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadovnick, A.D.; Remick, R.A.; Allen, J.; Swartz, E.; Yee, I.M.; Eisen, K.; Farquhar, R.; Hashimoto, S.A.; Hooge, J.; Kastrukoff, L.F.; et al. Depression and multiple sclerosis. Neurology 1996, 46, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Ensari, I.; Motl, R.W.; Pilutti, L.A. Exercise training improves depressive symptoms in people with multiple sclerosis: Results of a meta-analysis. J. Psychosom. Res. 2014, 76, 465–471. [Google Scholar] [CrossRef]
- Turner, A.P.; Hartoonian, N.; Sloan, A.P.; Benich, M.; Kivlahan, D.R.; Hughes, C.; Hughes, A.J.; Haselkorn, J.K. Improving fatigue and depression in individuals with multiple sclerosis using telephone-administered physical activity counseling. J. Consult. Clin. Psychol. 2016, 84, 297–309. [Google Scholar] [CrossRef]
- Mayo, C.D.; Miksche, K.; Attwell-Pope, K.; Gawryluk, J.R. The relationship between physical activity and symptoms of fatigue, mood, and perceived cognitive impairment in adults with multiple sclerosis. J. Clin. Exp. Neuropsychol. 2019, 41, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Oreja-Guevara, C.; Ayuso Blanco, T.; Brieva Ruiz, L.; Hernández Pérez, M.; Meca-Lallana, V.; Ramió-Torrentà, L. Cognitive Dysfunctions and Assessments in Multiple Sclerosis. Front. Neurol. 2019, 10, 581. [Google Scholar] [CrossRef]
- Bakshi, R.; Shaikh, Z.A.; Miletich, R.S.; Czarnecki, D.; Dmochowski, J.; Henschel, K.; Janardhan, V.; Dubey, N.; Kinkel, P.R. Fatigue in multiple sclerosis and its relationship to depression and neurologic disability. Mult. Scler. 2000, 6, 181–185. [Google Scholar] [CrossRef]
- Krupp, L.B.; Alvarez, L.A.; LaRocca, N.G.; Scheinberg, L.C. Fatigue in multiple sclerosis. Arch. Neurol 1988, 45, 435–437. [Google Scholar] [CrossRef]
- Rasova, K.; Havrdova, E.; Brandejsky, P.; Zálisová, M.; Foubikova, B.; Martinkova, P. Comparison of the influence of different rehabilitation programmes on clinical, spirometric and spiroergometric parameters in patients with multiple sclerosis. Mult. Scler. 2006, 12, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Rampello, A.; Franceschini, M.; Piepoli, M.; Antenucci, R.; Lenti, G.; Olivieri, D.; Chetta, A. Effect of aerobic training on walking capacity and maximal exercise tolerance in patients with multiple sclerosis: A randomized crossover controlled study. Phys. Ther. 2007, 87, 545–555. [Google Scholar] [CrossRef]
- Huisinga, J.M.; Filipi, M.L.; Stergiou, N. Elliptical exercise improves fatigue ratings and quality of life in patients with multiple sclerosis. J. Rehabil. Res. Dev. 2011, 48, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Edwards, T.; Pilutti, L.A. The effect of exercise training in adults with multiple sclerosis with severe mobility disability: A systematic review and future research directions. Mult. Scler. Relat. Disord. 2017, 16, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Garg, H.; Bush, S.; Gappmaier, E. Associations Between Fatigue and Disability, Functional Mobility, Depression, and Quality of Life in People with Multiple Sclerosis. Int. J. MS Care 2016, 18, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.E.; Cantwell, C.; Vowels, L.; Dodd, K. Changes in gait and fatigue from morning to afternoon in people with multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2002, 72, 361–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebert, J.R.; Corboy, J.R. The association between multiple sclerosis-related fatigue and balance as a function of central sensory integration. Gait Posture 2013, 38, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Tramontano, M.; Martino Cinnera, A.; Manzari, L.; Tozzi, F.F.; Caltagirone, C.; Morone, G.; Pompa, A.; Grasso, M.G. Vestibular rehabilitation has positive effects on balance, fatigue and activities of daily living in highly disabled multiple sclerosis people: A preliminary randomized controlled trial. Restor. Neurol. Neurosci. 2018, 36, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.R.; Corboy, J.R.; Manago, M.M.; Schenkman, M. Effects of vestibular rehabilitation on multiple sclerosis-related fatigue and upright postural control: A randomized controlled trial. Phys. Ther. 2011, 91, 1166–1183. [Google Scholar] [CrossRef] [PubMed]
- Torrejón, A.; Balsalobre-Fernández, C.; Haff, G.G.; García-Ramos, A. The load-velocity profile differs more between men and women than between individuals with different strength levels. Sports Biomech. 2019, 18, 245–255. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| HF (n = 18) | LF (n = 58) | Total (n = 76) | |
|---|---|---|---|
| Gender (Male/Female) | 9/9 | 27/31 | 36/40 |
| Age (Years) | 63.50 (53.83–65.17) | 57.00 (50.73–57.89) | 60.00 (52.51–58.57) |
| Body Height (cm) | 168.50 (163.45–175.11) | 170.00 (167.82–172.22) | 169.50 (167.74–171.94) |
| Body Mass (kg) | 79.90 (70.39–87.64) | 75.15 (72.29–79.39) | 76.00 (73.29–79.89) |
| BMI (kg/m2) | 25.50 (22.17–29.26) | 26.00 (24.99–26.96) | 26.00 (24.84–26.99) |
| MS Duration (years) | 10.72 (7.8–9.62) | 11.2 (6.43–8.69) | 10.96 (7.11–9.15) |
| MS Type (RR/SP) | 19/26 | 21/10 | 40/36 |
| Antidepressants (no. of patients) | 7 | 5 | 12 |
| Muscle relaxants (no. of patients) | 36 | 9 | 45 |
| All | LF | HF | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | Changes | Before | After | Changes | Before | After | Changes | |
| EDSS (↑ 65 years) | 6.38 ± 0.71 | 6.07 ± 0.55 ***M | 0.28 ± 0.30 (0.15–0.42) | 6.35 ± 0.69 | 6.04 ± 0.52 **M | 0.31 ± 0.25 (0.15–0.46) | 6.37 ± 0.79 | 6.12 ± 5.59 | 0.25 ± 0.38 (−0.06–0.56) |
| EDSS (↓ 65 years) | 5.60 ± 1.38 | 5.34 ± 1.36 ***S | 0.25 ± 0.33 (0.16–0.34) | 5.70 ± 1.37 | 5.42 ± 1.35 ***S | 0.28 ± 0.33 (0.18–0.38) | 5.15 ± 1.41 | 5.00 ± 1.39 | 0.15 ± 0.34 (−0.09–0.39) |
| GDS (↑ 65 years) | 4.19 ± 7.20 | 3.62 ± 5.83 S | 0.57 ± 4.06 (0.97–6.27) | 6.15 ± 8.57 | 5.69 ± 6.63 S | 0.46 ± 5.11 (−2.62–3.55) | 1.00 ± 1.85 | 0.25 ± 0.71 M | 0.75 ± 1.48 (−0.49–1.99) S |
| BDI (↓ 65 years) n = 53 | 8.60 ± 8.08 | 6.34 ± 6.87 ***M | 2.25 ± 4.45 (1.05–3.46) | 8.47 ± 8.36 | 6.62 ± 7.16 *S | 1.84 ± 4.70 (0.43–3.26) | 9.20 ± 7.07 | 5.10 ± 5.51 ***M | 4.10 ± 2.47 (2.33–5.87) M |
| MMSE (↑ 65 years) | 21.20 ± 5.87 | 23.20 ± 5.96 *S | −0.95 ± 2.22 (−1.96–0.06) | 21.85 ± 7.30 | 25.40 ± 2.60 ***S | −1.00 ± 2.58 (−2.56–0.56) | 19.62 ± 8.13 | 20.15 ± 2.22 S | 2.39 ± 0.74 (1.77–3.01) |
| MOCA (↓ 65 years) n = 53 | 20.36 ± 8.07 | 23.13 ± 8.85 ***M | −2.76 ± 2.62 (−3.47–−2.05) | 20.62 ± 8.08 | 23.62 ± 8.83 ***M | −3.00 ± 2.26 (−3.68–−2.32) | 19.20 ± 8.36 | 20.90 ± 9.06 S | −1.70 ± 3.86 (−4.46–1.06) M |
| LOW FATIGUE Group (LF) | HIGH FATIGUE Group (HF) | |||||
|---|---|---|---|---|---|---|
| Before MPA | After MPA | p | Before MPA | After MPA | p | |
| MAAP-EO | 4.25 (4.08–5.74) | 3.05 (2.94–4.33) | 0.0001 M | 5.35 (3.81–9.11) | 3.30 (3.15–6.42) | 0.102 M |
| MAML-EO | 2.30 (2.90–5.41) | 2.10 (2.48–4.90) | 0.008 | 3.20 (2.47–6.98) | 2.35 (1.84–4.52) | 0.024 M |
| MDDB-EO left leg | 49.00 (45.84–50.88) | 48.50 (47.67–51.63) | 0.401 | 47.50 (44.07–52.26) | 47.50 (44.64–51.80) | 0.887 |
| MDDB-EO right leg | 51.00 (49.12–54.16) | 51.50 (48.35–52.31) | 0.399 | 52.50 (47.73–55.93) | 52.50 (48.20–55.36) | 0.887 |
| MAAP-EC | 3.90 (3.96–5.76) | 2.40 (2.67–4.28) | 0.0001 M | 4.00 (3.03–10.10) | 2.90 (2.13–7.66) | 0.009 S |
| MAML-EC | 1.90 (2.25–4.14) | 1.50 (1.46–4.61) | 0.0002 S | 2.40 (1.04–8.56) | 1.50 (0.66–7.27) | 0.108 S |
| MDDB-EC left leg | 49.00 (46.25–51.65) | 49.00 (47.58–51.92) | 0.556 | 47.00 (44.90–52.04) | 49.00 (47.85–53.09) | 0.116 M |
| MDDB-EC right leg | 51.00 (48.35–53.75) | 51.00 (48.07–52.41) | 0.992 | 53.00 (47.96–55.10) | 51.00 (46.87–52.07) | 0.551 M |
| Variable | ALL | LOW FATIGURE Group | HIGH FATIGUE Group | |||
|---|---|---|---|---|---|---|
| BDI Changes | MOCCA Changes | BDI Changes | MOCCA Changes | BDI Changes | MOCCA Changes | |
| MAAP-EO changes | 0.115 | −0.06 | 0.104 | −0.09 | 0.085 | 0.011 |
| MAML-EO changes | 0.273 | 0.065 | 0.288 | 0.006 | −0.035 | 0.239 |
| MDDB-EO left leg changes | 0.093 | −0.186 | 0.086 | −0.25 | −0.377 | −0.047 |
| MDDB-EO right leg changes | −0.093 | 0.186 | −0.086 | 0.25 | 0.377 | 0.047 |
| MAAP-EC changes | 0.093 | −0.161 | 0.093 | −0.205 | 0.281 | 0.014 |
| MAML-EC changes | 0.233 | −0.202 | 0.301 | −0.246 | 0.267 | 0.331 |
| MDDB-EC 1 left leg changes | −0.077 | −0.149 | −0.045 | −0.123 | 0.088 | 0.136 |
| MDDB-EC 2 right leg changes | 0.073 | 0.14 | 0.045 | 0.123 | 0.373 | −0.021 |
| Variable | ALL | LOW FATIGURE Group | HIGH FATIGUE Group | |||
|---|---|---|---|---|---|---|
| GDS Changes | MMSE Changes | GDS Changes | MMSE Changes | GDS Changes | MMSE Changes | |
| MAAP-EO changes | 0.039 | −0.048 | 0.041 | −0.271 | −0.371 | 0.372 |
| MAML-EO changes | −0.071 | 0.056 | −0.116 | 0.221 | 0.034 | −0.034 |
| MDDB-EO left leg changes | 0.13 | 0.02 | 0.067 | 0.208 | 0.428 | −0.429 |
| MDDB-EO right leg changes | −0.13 | −0.02 | −0.067 | −0.208 | −0.429 | 0.429 |
| MAAP-EC changes | 0.115 | −0.155 | −0.107 | 0.066 | 0.676 | −0.676 |
| MAML-EC changes | 0.277 | −0.23 | 0.206 | −0.251 | 0.446 | −0.446 |
| MDDB-EC 1 left leg changes | −0.035 | 0.134 | −0.11 | 0.234 | −0.135 | 0.135 |
| MDDB-EC 2 right leg changes | 0.186 | −0.297 | 0.11 | −0.234 | 0.541 | −0.541 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Redlicka, J.; Zielińska-Nowak, E.; Lipert, A.; Miller, E. Impact of Moderate Individually Tailored Physical Activity in Multiple Sclerosis Patients with Fatigue on Functional, Cognitive, Emotional State, and Postural Stability. Brain Sci. 2021, 11, 1214. https://doi.org/10.3390/brainsci11091214
Redlicka J, Zielińska-Nowak E, Lipert A, Miller E. Impact of Moderate Individually Tailored Physical Activity in Multiple Sclerosis Patients with Fatigue on Functional, Cognitive, Emotional State, and Postural Stability. Brain Sciences. 2021; 11(9):1214. https://doi.org/10.3390/brainsci11091214
Chicago/Turabian StyleRedlicka, Justyna, Ewa Zielińska-Nowak, Anna Lipert, and Elżbieta Miller. 2021. "Impact of Moderate Individually Tailored Physical Activity in Multiple Sclerosis Patients with Fatigue on Functional, Cognitive, Emotional State, and Postural Stability" Brain Sciences 11, no. 9: 1214. https://doi.org/10.3390/brainsci11091214
APA StyleRedlicka, J., Zielińska-Nowak, E., Lipert, A., & Miller, E. (2021). Impact of Moderate Individually Tailored Physical Activity in Multiple Sclerosis Patients with Fatigue on Functional, Cognitive, Emotional State, and Postural Stability. Brain Sciences, 11(9), 1214. https://doi.org/10.3390/brainsci11091214