
Efficacy of Sound Therapy for Tinnitus Using an Enriched Acoustic Environment with Hearing-Loss Matched Broadband Noise




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Measurements
2.2. Tinnitus Treatment
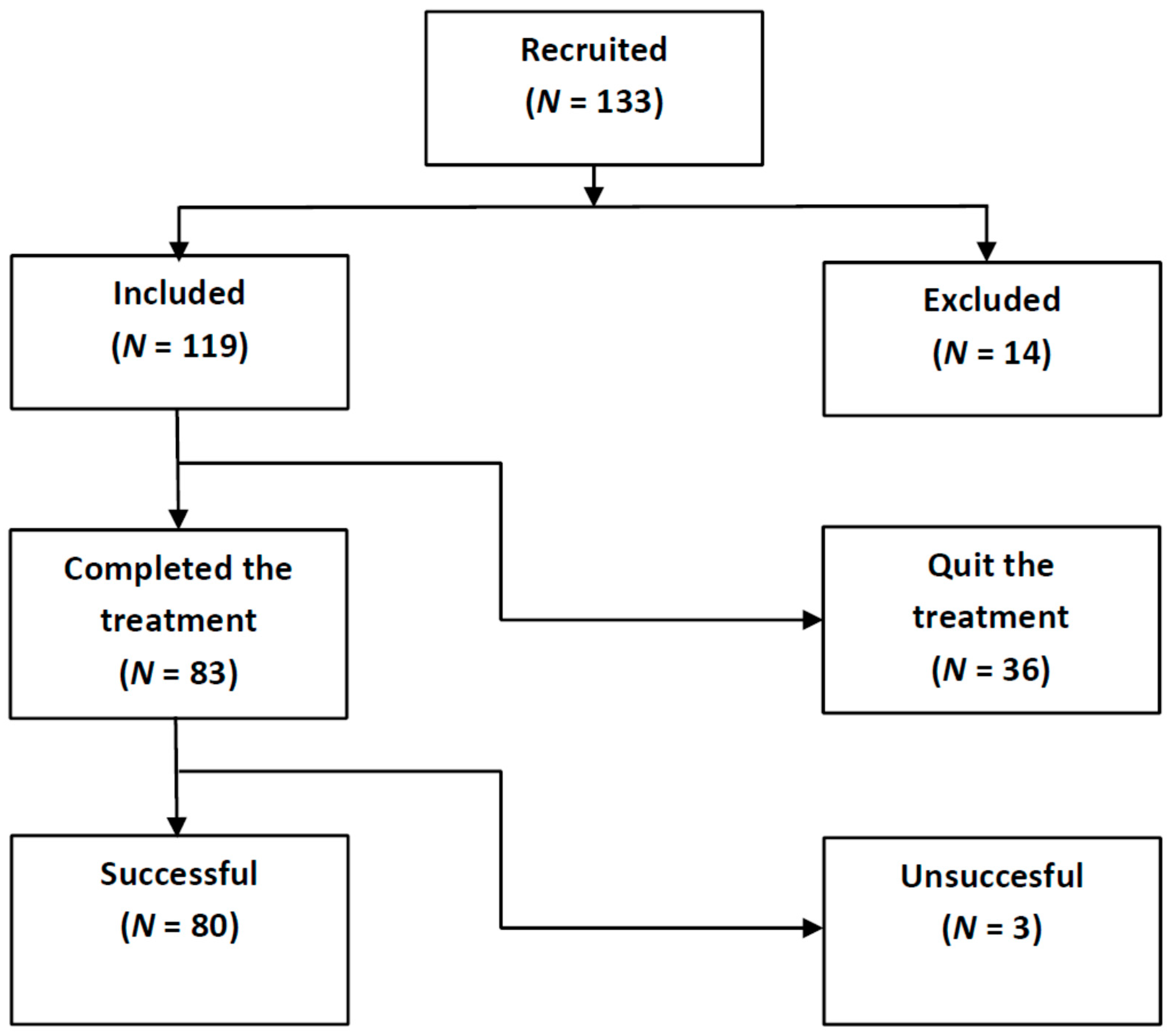
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Eggermont, J.J.; Tass, P.A. Maladaptive neural synchrony in tinnitus: Origin and restoration. Front. Neurol. 2015, 6, 29. [Google Scholar] [CrossRef] [Green Version]
- Hall, D.A.; Haider, H.; Kikidis, D.; Mielczarek, M.; Mazurek, B.; Szczepek, A.J.; Cederroth, C.R. Toward a global consensus on outcome measures for clinical trials in tinnitus. Trends Hear. 2015, 19, 2331216515580272. [Google Scholar]
- McFerran, D.J.; Stockdale, D.; Holme, R.; Large, C.H.; Baguley, D.M. Why Is There No Cure for Tinnitus? Front. Neurosci. 2019, 13, 802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Heyning, P.; Meeus, O.; Blaivie, C.; Vermeire, K.; Boudewyns, A.; De Ridder, D. Tinnitus: A multidisciplinary clinical approach. B-ENT 2007, 3, 3–10. [Google Scholar]
- Vio, M.M.; Holme, R.H. Hearing loss and tinnitus: 250 million people and US$10 billion potential market. Drug Discov. Today 2005, 10, 1263–1265. [Google Scholar] [CrossRef]
- Cobo, P. Tinnitus: Mechanisms, measures and sound treatments. Loquens 2015, 2, e024. [Google Scholar] [CrossRef]
- Eggermont, J.J. Noise and the Brain; Academic Press: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Schecklmann, M.; Vielsmeier, V.; Steffens, T.; Landgrebe, M.; Langguth, B.; Kleinjung, T. Relationship between audiometric slope and tinnitus pitch in tinnitus patients: Insights into the mechanisms of tinnitus generation. PLoS ONE 2012, 7, e34878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sereda, M.; Hall, D.H.; Bosnyak, D.J.; Edmondson-Jones, M.; Roberts, L.E.; Adjamian, P.; Palmer, A.R. Re-examining the relationship between audiometric profile and tinnitus pitch. Int. J. Audiol. 2011, 50, 303–312. [Google Scholar] [CrossRef] [Green Version]
- Shekhawat, G.S.; Searchfield, G.D.; Stinear, C.M. The relationship between tinnitus pitch and hearing sensitivity. Eur. Arch. Otolaryngol. 2014, 271, 41–48. [Google Scholar] [CrossRef]
- Cuesta, M.; Cobo, P. Relating tinnitus features and audiometric characteristics in a cohort of 34 tinnitus subjects. Loquens 2018, 5, e054. [Google Scholar] [CrossRef] [Green Version]
- Eggermont, J.J. The Neuroscience of Tinnitus; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Cederroth, C.R.; Gallus, S.; Hall, D.A.; Kleinjung, T.; Langguth, B.; Maruotti, A.; Meyer, M.; Noreña, A.; Probst, T.; Pryss, R.; et al. Editorial: Towards an understanding of tinnitus heterogeneity. Front. Aging Neurosci. 2019, 11, 53. [Google Scholar] [CrossRef] [Green Version]
- Jastreboff, P.J. 25 years of tinnitus retraining therapy. HNO 2015, 63, 307–311. [Google Scholar] [CrossRef]
- Henry, J.A.; Schechter, M.A.; Zaugg, T.L.; Griest, S.; Jastreboff, P.J.; Vernon, J.A.; Kaelin, C.; Meikle, M.B.; Lyons, K.S.; Stewart, B.J. Outcomes of clinical trial: Tinnitus masking versus tinnitus retraining therapy. J. Am. Acad. Audiol. 2006, 17, 104–132. [Google Scholar] [CrossRef] [Green Version]
- Formby, C.; Scherer, R. TRTT Study Group. Rationale for the tinnitus retraining therapy trial. Noise Health 2013, 15, 134–142. [Google Scholar] [CrossRef]
- Bauer, C.A.; Berry, J.L.; Brozowski, T.J. The effect of Tinnitus Retraining Therapy on chronic tinnitus: A controlled trial. Laryngoscope Investig. Otolaryngol. 2017, 2, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Jastreboff, P.J.; Jastreboff, M.M. Tinnitus retraining therapy for patients with tinnitus and decreased sound tolerance. Otolaryngol. Clin. N. Am. 2003, 36, 321–336. [Google Scholar] [CrossRef]
- Fuller, T.; Cima, R.; Langguth, B.; Mazurek, B.; Vlaeyen, J.W.; Hoare, D.J. Cognitive behavioural therapy for tinnitus. Cochrane Database Syst. Rev. 2020, 1, CD012614. [Google Scholar] [CrossRef]
- Cuesta, M.; Cobo, P. Broadband sound equalized by the hearing loss curves as an improved stimulus for tinnitus retraining therapy-A pilot, non-controlled observational study. J. Int. Adv. Otol. 2020, 16, 207–212. [Google Scholar] [CrossRef]
- Herráiz, C.; Hernández Calvín, F.J.; Plaza, G.; Tapia, M.C.; De los Santos, G. Handicap Assessment in Tinnitus Patients. Acta Otorrinolaringol. Esp. 2001, 52, 142–145. (In Spanish) [Google Scholar]
- Pienkowski, M. Rationale and efficacy of sound therapies for tinnitus and hyperacusis. Neuroscience 2019, 407, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Searchfield, G.D.; Durai, M.; Linford, T. A state-of-the-art review: Personalization of tinnitus sound therapy. Front. Psychol. 2017, 8, 1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaette, R.; Kempter, R. Development of tinnitus-related neuronal hyperactivity through homeostatic plasticity after hearing loss: A computational model. Eur. J. Neurosci. 2006, 23, 3124–3138. [Google Scholar] [CrossRef] [PubMed]
- Cobo, P.; Cuesta, M.; De la Colina, C. Customised enriched acoustic environment for sound therapy of tinnitus. Acta Acustica 2021, 5, 34. [Google Scholar] [CrossRef]
- Newman, C.W.; Sandridge, S.A.; Jacobson, G.P. Psychometric adequacy of the Tinnitus Handicap Inventory (THI) for evaluating treatment outcome. J. Am. Acad. Audiol. 1998, 9, 153–160. [Google Scholar] [PubMed]
- McCombe, A.; Baguley, D.; Coles, R.; McKeyna, L.; McKinney, C.; Windle-Taylor, P. Guidelines for the grading of tinnitus severity: The results of a working group commissioned by the British Association of Otolaryngologists, Head and Neck Surgeons, 1999. Clin. Otolaryngol. Allied Sci. 2001, 26, 388–393. [Google Scholar] [CrossRef]
- Bauer, C.A.; Berry, J.; Brozowski, T.J. Clinical trials supported by the Tinnitus Research Consortium: Lessons learned, the Southern Illinois University experience. Hear. Res. 2016, 334, 65–671. [Google Scholar] [CrossRef]
- Jastreboff, P.J.; Jastreboff, M.M. How TRT derives from the neurophysiological model. In Proceedings of the 6th International Tinnitus Seminar, London, UK, 5–9 September 1999; pp. 87–91. [Google Scholar]
- Cuesta, M.; Cobo, P. Audiometric Characteristics and Tinnitus Features in a Cohort of 170 Spanish Patients. Audiol. Res. 2021, 11, 594–602. [Google Scholar] [CrossRef]
- Lindblad, A.C.; Rosenhall, U.; Oloffson, A.; Hagerman, B. Tinnitus and other auditory problems—Occupational noise exposure below risk limits may cause inner ear dysfunction. PLoS ONE 2014, 9, e97377. [Google Scholar] [CrossRef] [Green Version]
- Weisz, N.; Hartmann, T.; Dohrmann, K.; Schlee, W.; Noreña, A. High-frequency tinnitus without hearing loss does not mean absence of deafferentation. Hear. Res. 2006, 222, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Liberman, M.C.; Kujawa, S.G. Cochlear synaptopathy in acquired sensorineural hearing loss: Manifestations and mechanisms. Hear. Res. 2017, 349, 138–147. [Google Scholar] [CrossRef]
- Henry, J.A.; Rheinsburg, B.; Zaugg, T. Comparison of custom sounds for achieving tinnitus relief. J. Am. Acad. Audiol. 2004, 15, 585–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barozzi, S.; Del Bo, L.; Crocetti, A.; Dyrlind, O.; Passoni, S.; Zolin, A.; Painicucci, E.; Mancuso, A.; Kaur, M.; Searchfield, G.D. A comparison of nature and technical sounds for tinnitus therapy. Acta Acust. United Acust. 2016, 102, 540–546. [Google Scholar] [CrossRef]
- Kim, B.J.; Chung, S.W.; Jung, J.Y.; Suh, M.W. Effect of different sounds on the treatment outcome of tinnitus retraining therapy. Clin. Exp. Otorhinolaryngol. 2014, 7, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Oishi, N.; Shinden, S.; Kanzaki, S.; Saito, K.; Inoue, Y.; Ogawa, K. Effects of Tinnitus Retraining Therapy involving monaural noise generators. Eur. Arch. Otorhinolaryngol. 2013, 270, 443–448. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Schlee, W.; Vanneste, S.; Londero, A.; Weisz, N.; Kleinjung, T.; Shekhawat, G.S.; Elgoyhen, A.B.; Song, J.J.; Andersson, G.; et al. Tinnitus and tinnitus disorder: Theoretical and operational definitions (an international multidisciplinary proposal). Prog. Brain Res. 2021, 260, 1–25. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Tinnitus Duration (Years) | ||||
|---|---|---|---|---|---|
| Group | N | Mean | SD | Mean | SD |
| All | 83 | 51.6 | 9.1 | 6.3 | 8.8 |
| Male | 52 | 52.9 | 8.9 | 7.2 | 9.3 |
| Female | 31 | 49.4 | 9.6 | 5.0 | 7.8 |
| AAT (dB) | AATLF (dB) | AATHF (dB) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Left Ear | Right Ear | Left Ear | Right Ear | Left Ear | Right Ear | ||||||||
| Group | N | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| All | 83 | 24 | 15 | 24 | 19 | 16 | 13 | 18 | 19 | 37 | 22 | 34 | 23 |
| NH | 22 | 11 | 5 | 10 | 5 | 9 | 6 | 9 | 6 | 15 | 6 | 13 | 7 |
| HI | 61 | 29 | 14 | 29 | 20 | 19 | 14 | 21 | 21 | 45 | 20 | 42 | 22 |
| Tinnitus Location (%) | Tinnitus Sound (%) | Tinnitus Pitch (Hz) | Initial THI | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | N | Left | Right | Bilateral | Hissing | Ringing | Tonal | Mean | SD | Mean | SD |
| All | 83 | 36 | 21 | 43 | 44 | 26 | 30 | 5213 | 3054 | 50 | 23 |
| NH | 22 | 43 | 14 | 43 | 38 | 43 | 19 | 4475 | 3870 | 52 | 23 |
| HI | 61 | 34 | 24 | 42 | 46 | 20 | 34 | 5479 | 2695 | 48 | 22 |
| Severity Scale | N | THIini | THIfin | ΔTHI |
|---|---|---|---|---|
| Mild | 32 | 29 | 15 | −14 |
| Moderate | 20 | 47 | 27 | −20 |
| Severe | 14 | 67 | 36 | −31 |
| Catastrophic | 14 | 87 | 45 | −42 |
| All | 80 | 50 | 27 | −23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuesta, M.; Garzón, C.; Cobo, P. Efficacy of Sound Therapy for Tinnitus Using an Enriched Acoustic Environment with Hearing-Loss Matched Broadband Noise. Brain Sci. 2022, 12, 82. https://doi.org/10.3390/brainsci12010082
Cuesta M, Garzón C, Cobo P. Efficacy of Sound Therapy for Tinnitus Using an Enriched Acoustic Environment with Hearing-Loss Matched Broadband Noise. Brain Sciences. 2022; 12(1):82. https://doi.org/10.3390/brainsci12010082
Chicago/Turabian StyleCuesta, María, Christiam Garzón, and Pedro Cobo. 2022. "Efficacy of Sound Therapy for Tinnitus Using an Enriched Acoustic Environment with Hearing-Loss Matched Broadband Noise" Brain Sciences 12, no. 1: 82. https://doi.org/10.3390/brainsci12010082
APA StyleCuesta, M., Garzón, C., & Cobo, P. (2022). Efficacy of Sound Therapy for Tinnitus Using an Enriched Acoustic Environment with Hearing-Loss Matched Broadband Noise. Brain Sciences, 12(1), 82. https://doi.org/10.3390/brainsci12010082