
High-Level Executive Functions: A Possible Role of Sex and Weight Condition in Planning and Decision-Making Performances

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcomes
2.2.1. Demographic and Clinical Information
2.2.2. Executive Functions
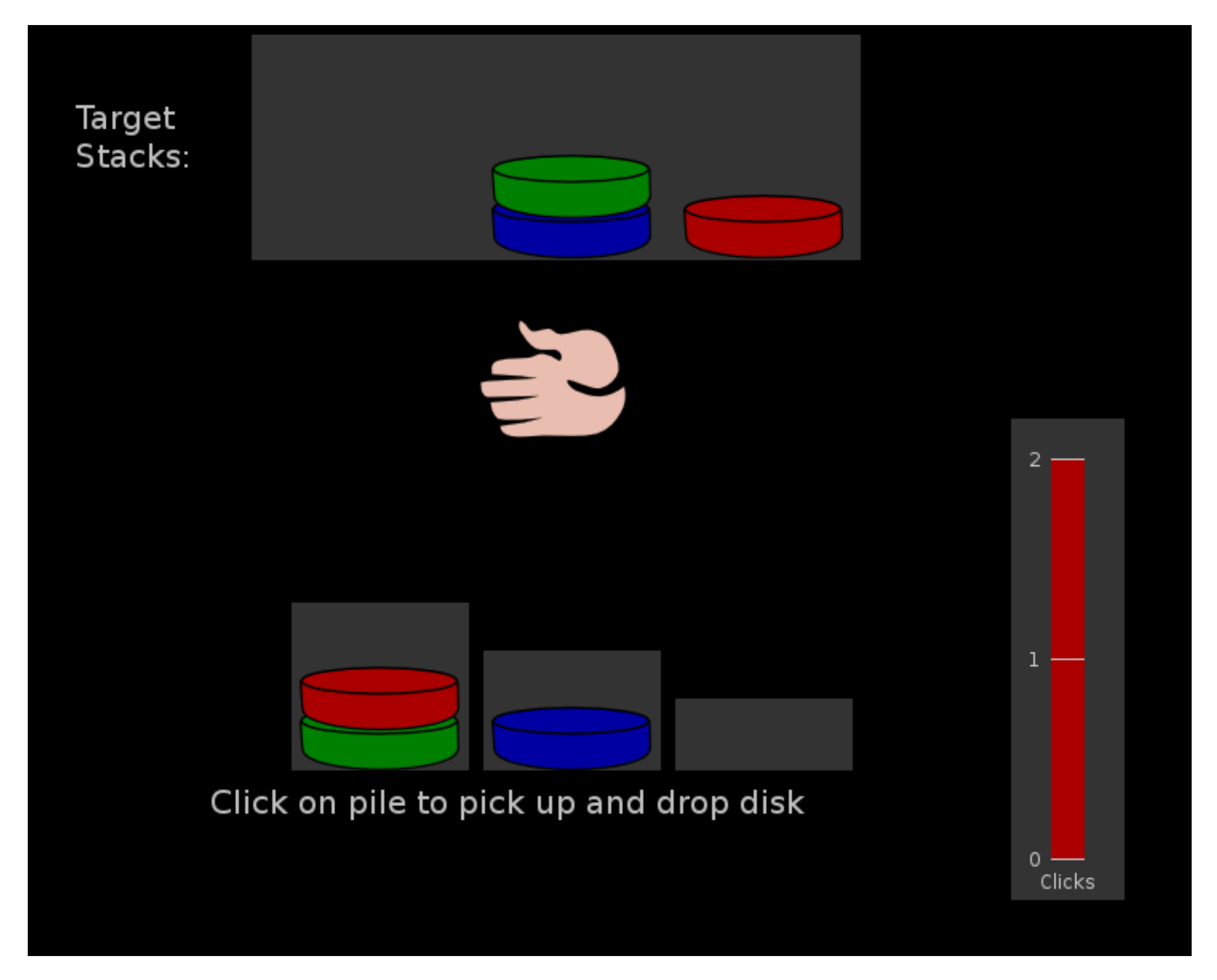
2.3. Apparatus
2.4. General Procedure
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, S.Z.; Lu, W.; Zong, X.F.; Ruan, H.Y.; Liu, Y. Obesity and hypertension. Exp. Ther. Med. 2016, 12, 2395–2399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauner, H. Obesity and diabetes. In Textbook of Diabetes; Holt, R.I.G., Cockram, C., Flyvbjerg, A., Goldstein, B.J., Eds.; University of Nottingham: Nottingham, UK, 2017; pp. 215–228. [Google Scholar]
- Littleton, S.W. Impact of obesity on respiratory function. Respirology 2012, 17, 43–49. [Google Scholar] [CrossRef]
- Carey, M.; Small, H.; Yoong, S.L.; Boyes, A.; Bisquera, A.; Sanson-Fisher, R. Prevalence of comorbid depression and obesity in general practice: A cross-sectional survey. Br. J. Gen. Pract. 2014, 64, e122–e127. [Google Scholar] [CrossRef]
- Gariepy, G.; Nitka, D.; Schmitz, N. The association between obesity and anxiety disorders in the population: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 407–419. [Google Scholar] [CrossRef] [Green Version]
- Favieri, F.; Forte, G.; Casagrande, M. The executive functions in overweight and obesity: A systematic review of neuropsychological cross-sectional and longitudinal studies. Front. Psychol. 2019, 10, 2126. [Google Scholar] [CrossRef]
- Kolotkin, R.L.; Meter, K.; Williams, G.R. Quality of life and obesity. Obes. Rev. 2001, 2, 219–229. [Google Scholar] [CrossRef]
- Rotge, J.Y.; Poitou, C.; Fossati, P.; Aron-Wisnewsky, J.; Oppert, J.M. Decision-making in obesity without eating disorders: A systematic review and meta-analysis of Iowa gambling task performances. Obes. Rev. 2017, 18, 936–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Europe. Health for All Database [Online Database]. Copenhagen: WHO Regional Office for Europe. Available online: http://www.euro.who.int/hfadb (accessed on 15 June 2021).
- Mobbs, O.; Crépin, C.; Thiéry, C.; Golay, A.; Van der Linden, M. Obesity and the four facets of impulsivity. Patient Educ. Couns. 2010, 79, 372–377. [Google Scholar] [PubMed] [Green Version]
- Casagrande, M.; Boncompagni, I.; Forte, G.; Guarino, A.; Favieri, F. Emotion and overeating behavior: Effects of alexithymia and emotional regulation on overweight and obesity. Eat. Weight Disord. 2020, 5, 1333–1345. [Google Scholar] [CrossRef]
- Favieri, F.; Forte, G.; Marotta, A.; Casagrande, M. Food-related attentional bias in individuals with normal weight and overweight: A study with a flicker task. Nutrients 2020, 12, 492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharifi, N.; Mahdavi, R.; Ebrahimi-Mameghani, M. Perceived barriers to weight loss programs for overweight or obese women. Health Promot. Perspect. 2013, 3, 11. [Google Scholar]
- Fitzpatrick, S.; Gilbert, S.; Serpell, L. Systematic review: Are overweight and obese individuals impaired on behavioural tasks of executive functioning? Neuropsychol. Rev. 2013, 23, 138–156. [Google Scholar] [CrossRef] [PubMed]
- Stinson, E.J.; Krakoff, J.; Gluck, M.E. Depressive symptoms and poorer performance on the Stroop Task are associated with weight gain. Physiol. Behav. 2018, 186, 25–30. [Google Scholar] [CrossRef]
- Galioto, R.; Bond, D.; Gunstad, J.; Pera, V.; Rathier, L.; Tremont, G. Executive functions predict weight loss in a medically supervised weight loss programme. Obes. Sci. Pract. 2016, 2, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, L.; Colzato, L.S. Overweight and cognitive performance: High body mass index is associated with impairment in reactive control during task switching. Front. Nutri. 2017, 4, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldschmidt, A.B.; O’Brien, S.; Lavender, J.M.; Pearson, C.M.; Le Grange, D.; Hunter, S.J. Executive functioning in a racially diverse sample of children who are overweight and at risk for eating disorders. Appetite 2018, 124, 43–49. [Google Scholar] [CrossRef]
- Perpiñá, C.; Segura, M.; Sánchez-Reales, S. Cognitive flexibility and decision-making in eating disorders and obesity. Eat. Weight Disord. 2017, 22, 435–444. [Google Scholar] [CrossRef]
- Kroll, D.S.; Feldman, D.E.; Biesecker, C.L.; McPherson, K.L.; Manza, P.; Joseph, P.V.; Wang, G.J. Neuroimaging of Sex/Gender Differences in Obesity: A Review of Structure, Function, and Neurotransmission. Nutrients 2020, 12, 1942. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.J.; Gupta, S.R.; Moustafa, A.F.; Chao, A.M. Sex/Gender Differences in Obesity Prevalence, Comorbidities, and Treatment. Curr. Obes. Rep. 2021, 10, 458–466. [Google Scholar] [CrossRef]
- Sie, J.H.; Chen, Y.H.; Shiau, Y.H.; Chu, W.C. Gender-and age-specific differences in resting-state functional connectivity of the central autonomic network in adulthood. Front. Human Neurosci. 2019, 13, 369. [Google Scholar] [CrossRef] [Green Version]
- Bechara, A.; Damasio, A.R.; Damasio, H.; Anderson, S.W. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 1994, 50, 7–15. [Google Scholar] [CrossRef]
- Brogan, A.; Hevey, D.; O’Callaghan, G.; Yoder, R.; O’Shea, D. Impaired decision making among morbidly obese adults. J. Psychosom. Res. 2011, 70, 189–196. [Google Scholar] [CrossRef]
- Fagundo, A.B.; De la Torre, R.; Jiménez-Murcia, S.; Agüera, Z.; Granero, R.; Tárrega, S. Executive functions profile in extreme eating/weight conditions: From anorexia nervosa to obesity. PLoS ONE 2012, 7, e43382. [Google Scholar] [CrossRef] [Green Version]
- Pignatti, R.; Bertella, L.; Albani, G.; Mauro, A.; Molinari, E.; Semenza, C. Decision-making in obesity: A study using the Gambling Task. Eat. Weight Disord. 2006, 11, 126–132. [Google Scholar] [CrossRef]
- Navas, J.F.; Vilar-López, R.; Perales, J.C.; Steward, T.; Fernández-Aranda, F.; Verdejo-García, A. Altered decision-making under risk in obesity. PLoS ONE 2016, 11, e0155600. [Google Scholar] [CrossRef] [Green Version]
- Danner, U.N.; Ouwehand, C.; Van Haastert, N.L.; Hornsveld, H.; De Ridder, D.T. Decision-making impairments in women with binge eating disorder in comparison with obese and normal weight women. Eur. Eat. Disord. Rev. 2012, 20, e56–e62. [Google Scholar] [CrossRef]
- Bechara, A.; Tranel, D.; Damasio, H. Characterization of the Decision-Making Deficit of Patients with Ventromedial Prefrontal Cortex Lesions. Brain 2000, 123, 2189–2202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qavam, S.E.; Anisan, A.; Fathi, M.; Pourabbasi, A. Study of relationship between obesity and executive functions among high school students in Bushehr. Iran. J. Diabetes Obes. 2015, 14, 79. [Google Scholar] [CrossRef] [Green Version]
- Byrne, K.A.; Worthy, D.A. Toward a mechanistic account of gender differences in reward-based decision-making. J. Neurosci. Psychol. Econ. 2016, 9, 157. [Google Scholar] [CrossRef] [Green Version]
- Forte, G.; Morelli, M.; Casagrande, M. Heart Rate Variability and Decision-Making: Autonomic Responses in Making Decisions. Brain Sciences 2021, 11, 243. [Google Scholar] [CrossRef] [PubMed]
- Shallice, T. Specific impairments of planning. Philos. Trans. R. Soc. Lond. Biol. 1982, 298, 199–209. [Google Scholar] [PubMed]
- Maffeis, C.; Banzato, C.; Talamini, G. Waist-to-height ratio, a useful index to identify high metabolic risk in overweight children. J. Pediatr. 2008, 152, 207–213. [Google Scholar] [CrossRef]
- Mueller, S.T.; Piper, B.J. The psychology experiment building language (PEBL) and PEBL test battery. J. Neurosci. Methods 2014, 222, 250–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Watanabe, R.M. A better index of body adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Dohle, S.; Diel, K.; Hofmann, W. Executive functions and the self-regulation of eating behavior: A review. Appetite 2018, 124, 4–9. [Google Scholar] [CrossRef]
- Yang, Y.; Shields, G.S.; Guo, C.; Liu, Y. Executive function performance in obesity and overweight individuals: A meta-analysis and review. Neurosci. Biobehav. Rev. 2018, 84, 225–244. [Google Scholar] [CrossRef]
- Orsini, C.A.; Willis, M.L.; Gilbert, R.J.; Bizon, J.L.; Setlow, B. Sex differences in a rat model of risky decision making. Behav. Neurol. 2016, 130, 50. [Google Scholar] [CrossRef] [PubMed]
- Van den Bos, R.; Harteveld, M.; Stoop, H. Stress and decision-making in humans: Performance is related to cortisol reactivity, albeit differently in men and women. Psychoneuroendocrinology 2009, 34, 1449–1458. [Google Scholar] [CrossRef]
- Cazzato, V.; Basso, D.; Cutini, S.; Bisiacchi, P. Gender differences in visuospatial planning: An eye movements study. Behav. Brain Res. 2010, 206, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Damasio, A.R. On some functions of the human prefrontal cortex. Ann. N. Y. Acad. Sci. 1995, 769, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Brockmeyer, T.; Simon, J.J.; Becker, A.; Friederich, H.C. Reward-related decision making and long-term weight loss maintenance. Physiol. Behav. 2017, 181, 69–74. [Google Scholar] [CrossRef]
- De Meira Leite, C.; Rubio, K. Social Aspects as Maintenance Factors of the Obesity Condition: The Somatic Marker Hypothesis. Int. J. Appl. Sci. 2014, 4, 25–30. [Google Scholar]
- Verbeken, S.; Braet, C.; Bosmans, G.; Goossens, L. Comparing decision making in average and overweight children and adolescents. Int. J. Obes. 2014, 38, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Patte, K.; Levitan, R.; Reid, C.; Tweed, S.; Curtis, C. From motivation to behaviour: A model of reward sensitivity, overeating, and food preferences in the risk profile for obesity. Appetite 2007, 48, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Derntl, B.; Pintzinger, N.; Kryspin-Exner, I.; Schöpf, V. The impact of sex hormone concentrations on decision-making in females and males. Front. Neurosci. 2014, 8, 352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thayer, J.F.; Lane, R.D. A model of neurovisceral integration in emotion regulation and dysregulation. J. Affect. Disord. 2000, 61, 201–216. [Google Scholar] [CrossRef] [Green Version]
- Morelli, M.; Casagrande, M.; Forte, G. Decision Making: A Theoretical Review. Integr. Psychol. Behav. Sci. 2021, 1–21. [Google Scholar] [CrossRef]
- Chao, A.M.; Loughead, J.; Bakizada, Z.M.; Hopkins, C.M.; Geliebter, A.; Gur, R.C.; Wadden, T.A. Sex/gender differences in neural correlates of food stimuli: A systematic review of functional neuroimaging studies. Obes. Rev. 2017, 18, 687–699. [Google Scholar] [CrossRef]
- Sweat, V.; Yates, K.F.; Migliaccio, R.; Convit, A. Obese adolescents show reduced cognitive processing speed compared with healthy weight peers. Child. Obes. 2017, 13, 190–196. [Google Scholar] [CrossRef]
- Favieri, F.; Chen, E.; Casagrande, M. Executive Functions and Body Weight at Different Ages: A Preliminary Study. Nutrients 2021, 13, 1174. [Google Scholar] [CrossRef]
- Gunstad, J.; Paul, R.H.; Cohen, R.A.; Tate, D.F.; Spitznagel, M.B.; Gordon, E. Elevated body mass index is associated with executive dysfunction in otherwise healthy adults. Compr. Psychiatry 2007, 48, 57–61. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Males | Females | |||||
|---|---|---|---|---|---|---|
| Normal Weight | Overweight | Normal Weight | Overweight | F | p | |
| N | 14 | 18 | 15 | 18 | ||
| Age (mean, sd) | 22.93 (2.56) | 25.53 (2.72) | 22.89 (1.53) | 23.28 (2.47) | 3.62 | 0.07 |
| Years of Education (mean, sd) | 16.00 (1.79) | 15.73 (2.52) | 16.83 (1.20) | 16.72 (1.60) | <1 | 0.86 |
| Physiological Measures (mean, sd) | ||||||
| Weight (kg) | 67.29 (7.54) | 86.27 (12.41) | 57.42 (7.76) | 74.18 (7.78) | <1 | 0.63 |
| Height (m) | 1.76 (0.06) | 1.79 (0.09) | 1.67 (0.07) | 1.67 (0.09) | <1 | 0.41 |
| BMI | 21.50 (1.65) | 27.07 (2.31) | 20.56 (2.04) | 26.56 (1.82) | <1 | 0.66 |
| Waist-to-Height Ratio | 0.46 (0.04) | 0.50 (0.05) | 0.44 (0.04) | 0.50 (0.05) | <1 | 0.32 |
| Body Adiposity Index | 24.10 (2.97) | 27.25 (3.99) | 26.06 (4.40) | 33.56 (3.90) | 4.45 | 0.04 |
| Systolic Blood Pressure | 127.29 (7.21) | 125.54 (6.83) | 113.17 (8.98) | 114.06 (10.07) | <1 | 0.55 |
| Diastolic Blood Pressure | 73.50 (7.40) | 74.77 (7.31) | 72.28 (8.92) | 72.00 (7.11) | <1 | 0.70 |
| Males | Females | |||||
|---|---|---|---|---|---|---|
| Normal Weight | Overweight | Normal Weight | Overweight | F | p | |
| IGT | ||||||
| Learning of Long-Term Consequences (LTC) | 21.43 (28.38) | −1.07 (22.66) | −6.11 (17.40) | 2.94 (14.91) | 8.97 | 0.004 * |
| Bias of Infrequent Loss (IFL) | 0.86 (31.77) | −1.20 (16.90) | −0.78 (12.74) | 0.47 (15.35) | <1 | 0.99 |
| TOL | ||||||
| Total Score | 25.29 (8.04) | 22.62 (6.89) | 24.50 (4.96) | 21.83 (8.60) | <1 | 0.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Favieri, F.; Forte, G.; Pazzaglia, M.; Chen, E.Y.; Casagrande, M. High-Level Executive Functions: A Possible Role of Sex and Weight Condition in Planning and Decision-Making Performances. Brain Sci. 2022, 12, 149. https://doi.org/10.3390/brainsci12020149
Favieri F, Forte G, Pazzaglia M, Chen EY, Casagrande M. High-Level Executive Functions: A Possible Role of Sex and Weight Condition in Planning and Decision-Making Performances. Brain Sciences. 2022; 12(2):149. https://doi.org/10.3390/brainsci12020149
Chicago/Turabian StyleFavieri, Francesca, Giuseppe Forte, Mariella Pazzaglia, Eunice Y. Chen, and Maria Casagrande. 2022. "High-Level Executive Functions: A Possible Role of Sex and Weight Condition in Planning and Decision-Making Performances" Brain Sciences 12, no. 2: 149. https://doi.org/10.3390/brainsci12020149
APA StyleFavieri, F., Forte, G., Pazzaglia, M., Chen, E. Y., & Casagrande, M. (2022). High-Level Executive Functions: A Possible Role of Sex and Weight Condition in Planning and Decision-Making Performances. Brain Sciences, 12(2), 149. https://doi.org/10.3390/brainsci12020149