
Entrapment of Binaural Auditory Beats in Subjects with Symptoms of Insomnia


Abstract
:1. Introduction
2. Materials and Methods
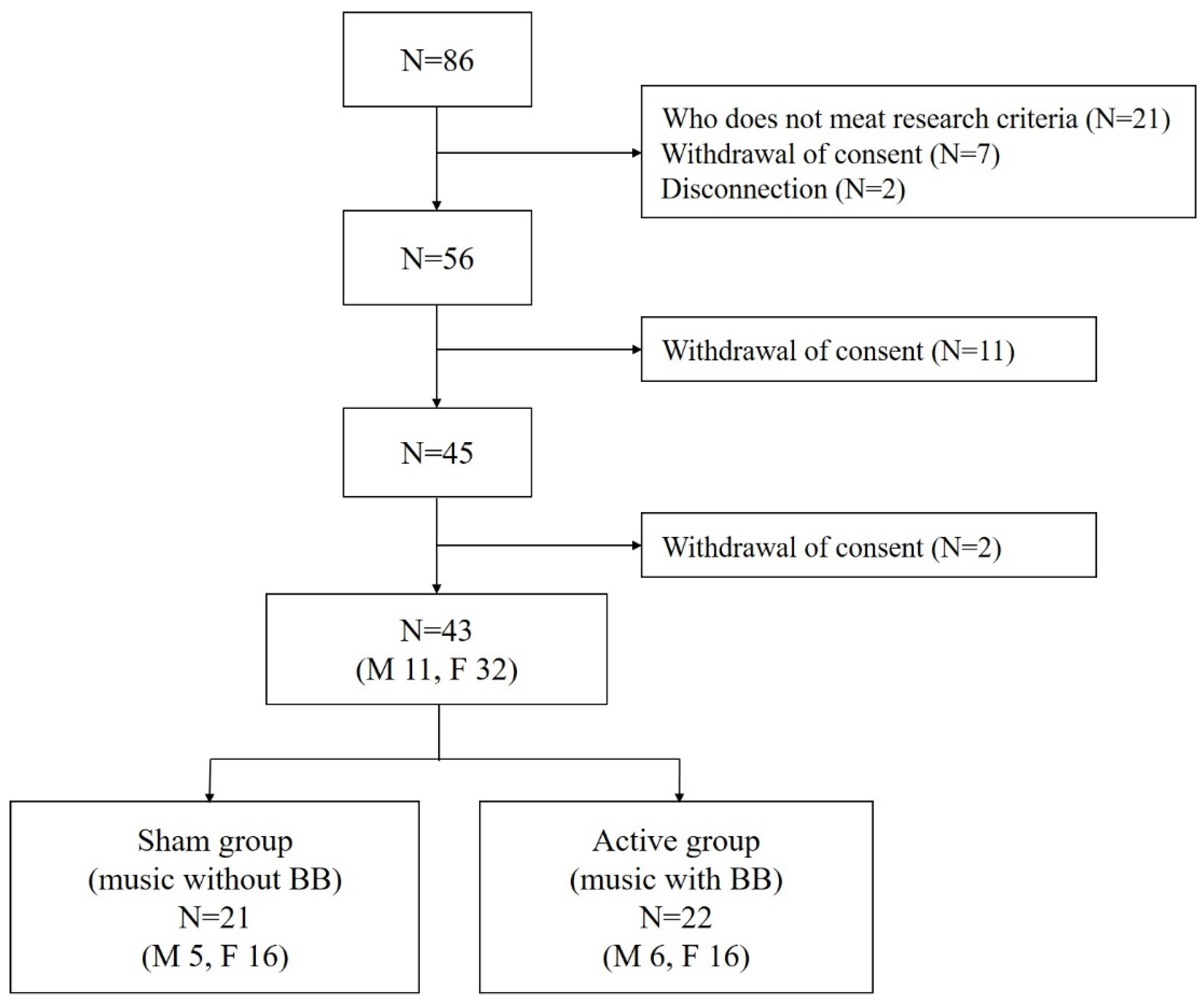
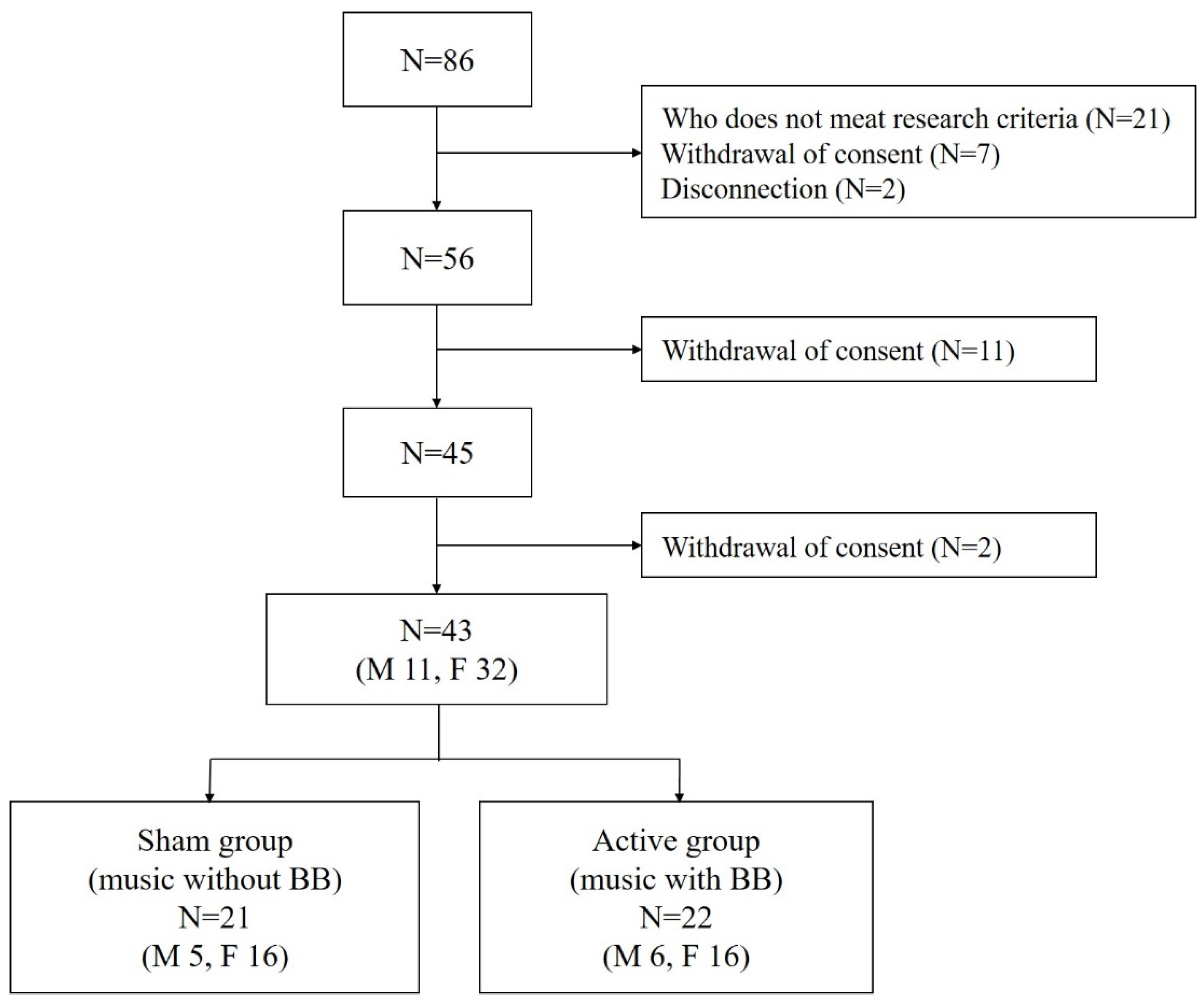
2.1. Participants
2.2. Procedure
2.3. Quantitative Electroencephalography (QEEG)
2.4. Spectral Analysis
2.5. Protocol
2.6. Statistical Analysis
3. Results
3.1. Demographic, Clinical Characteristic and Polysomnographic Findings
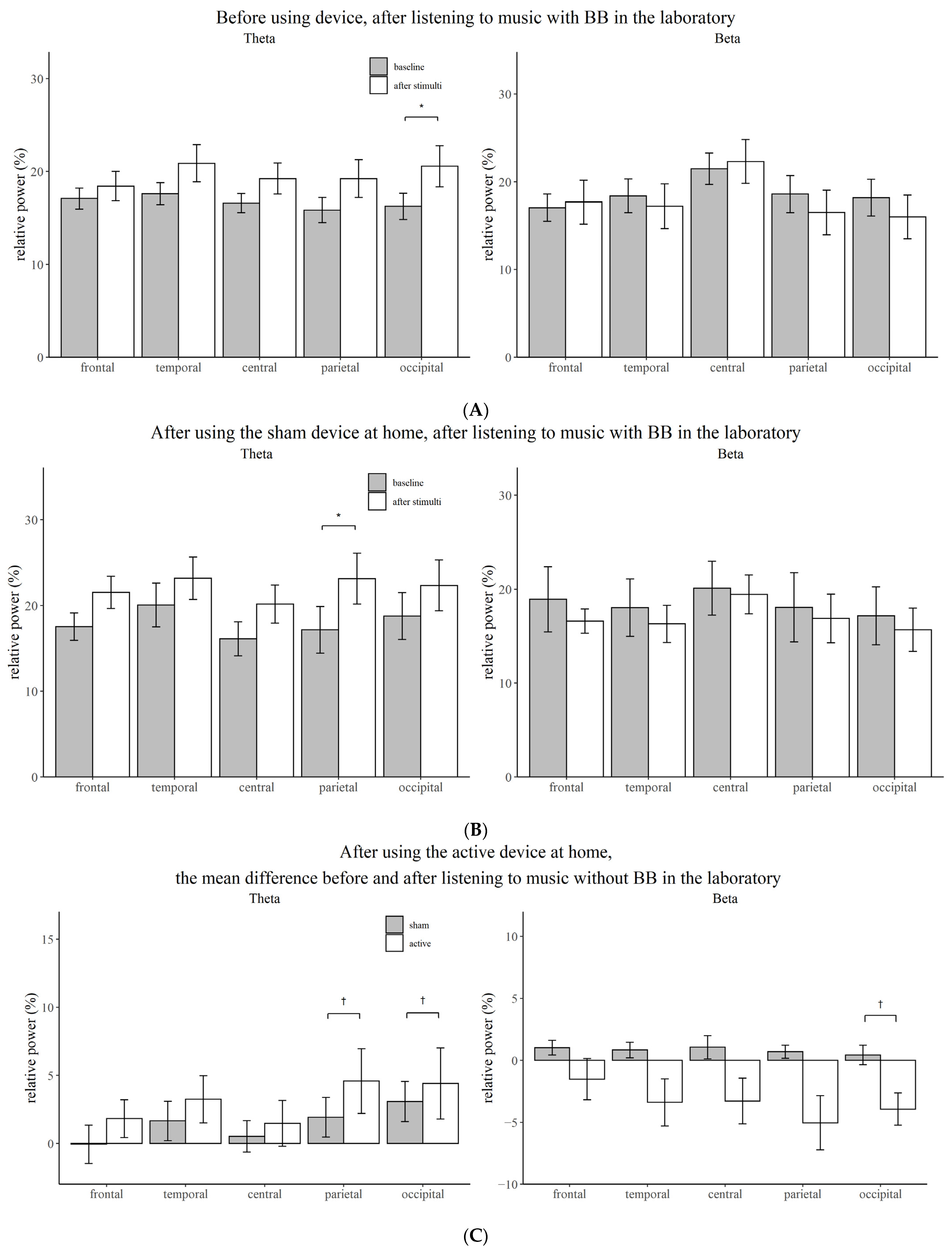
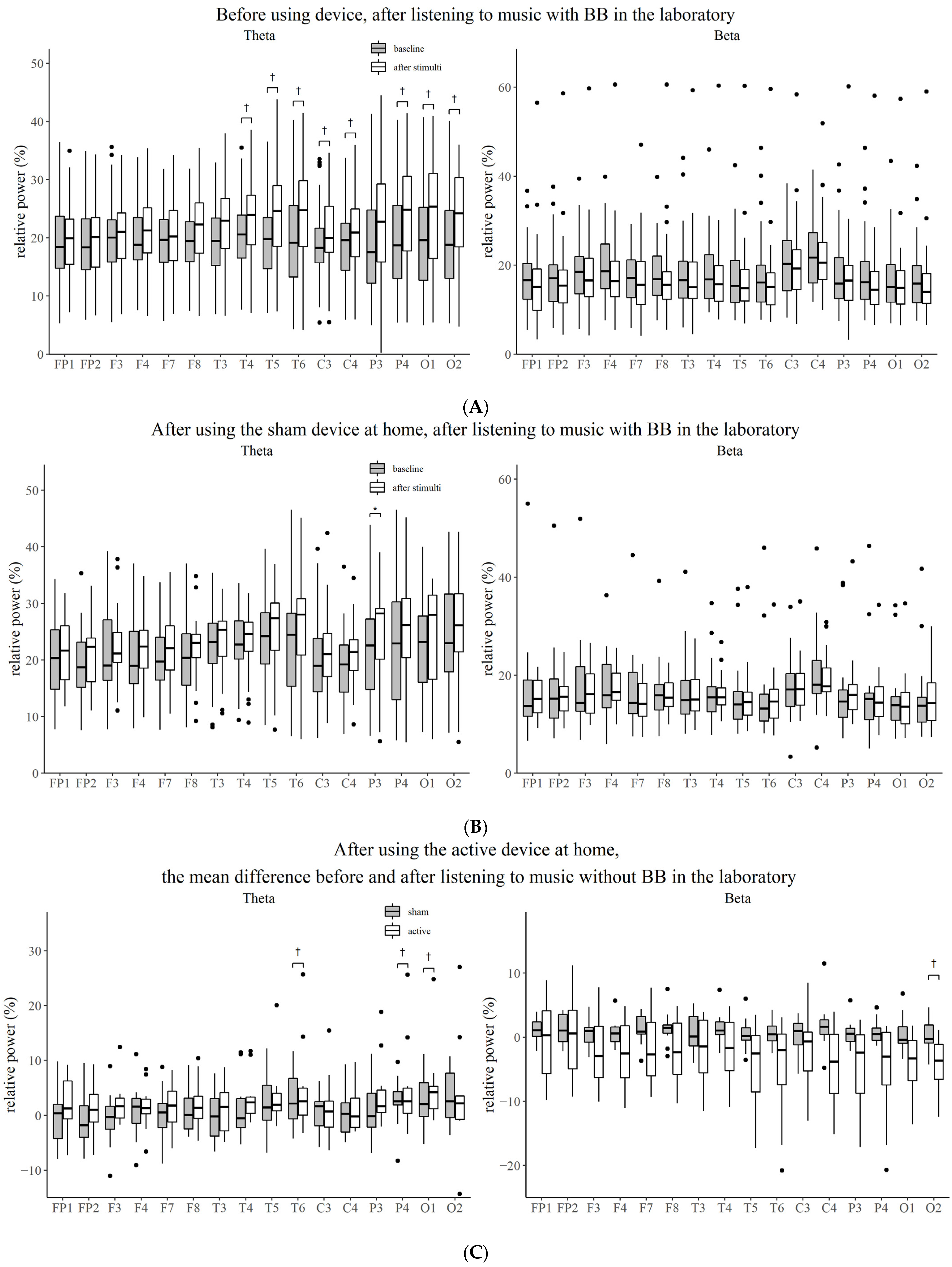
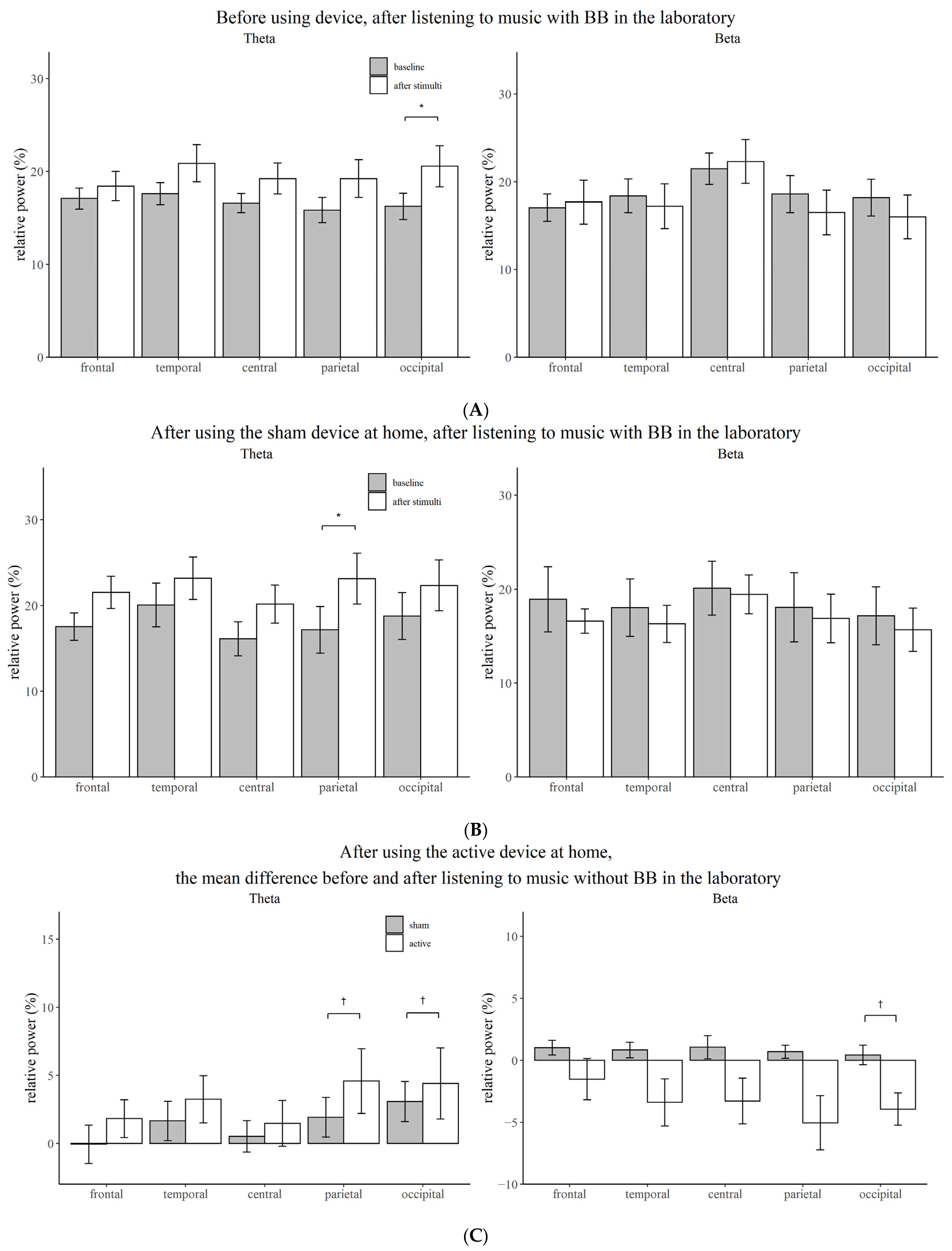
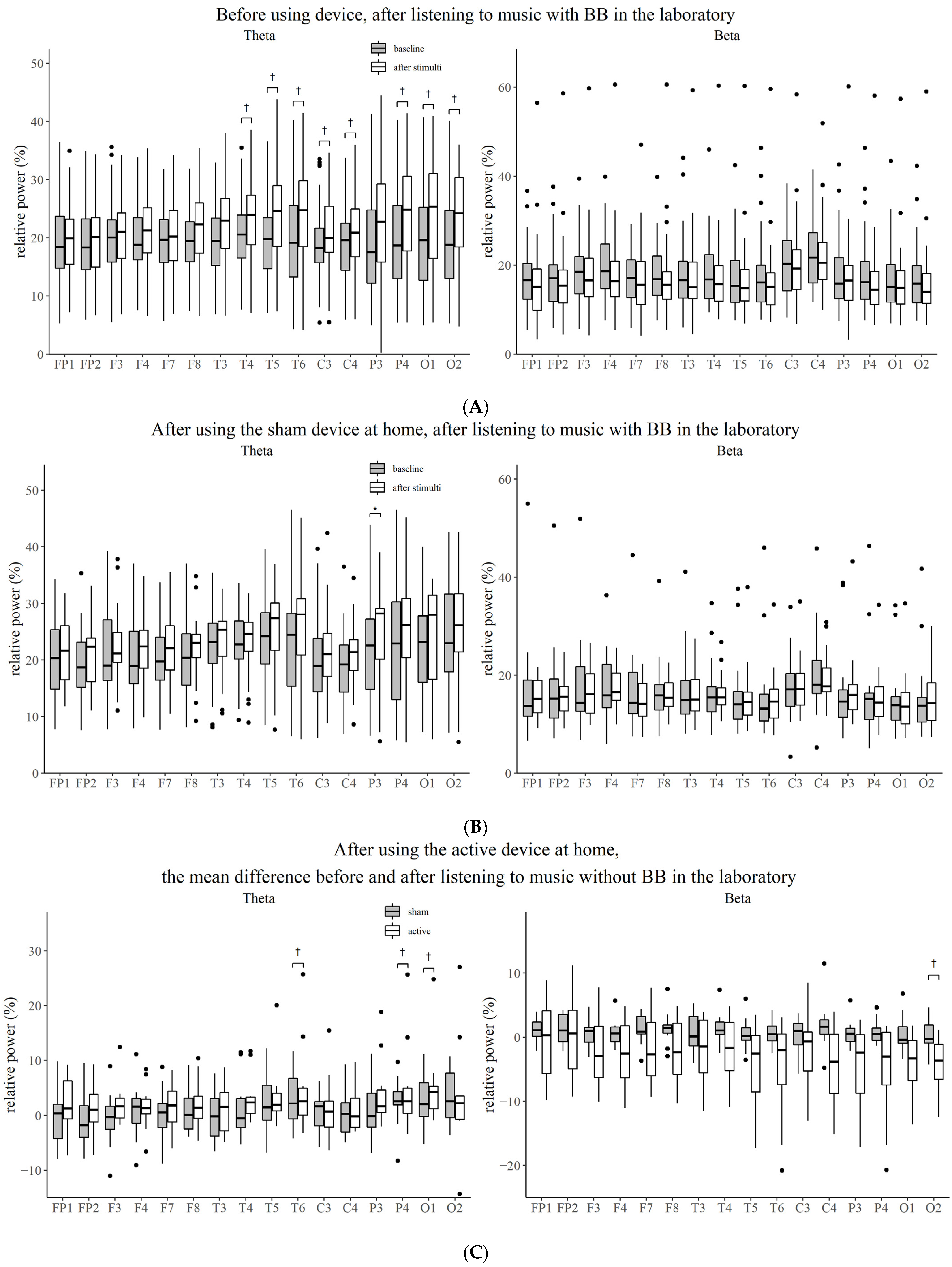
3.2. Effect of Stimuli Compared to Baseline before Using Device
3.3. Effect of Stimuli Compared to Baseline after Using Device
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ohayon, M.M.; Hong, S.-C. Prevalence of insomnia and associated factors in South Korea. J. Psychosom. Res. 2002, 53, 593–600. [Google Scholar] [CrossRef]
- Chung, S.; Cho, S.W.; Jo, M.-W.; Youn, S.; Lee, J.; Sim, C.S. The Prevalence and Incidence of Insomnia in Korea during 2005 to 2013. Psychiatry Investig. 2020, 17, 533. [Google Scholar] [CrossRef] [PubMed]
- Sivertsen, B.; Krokstad, S.; Mykletun, A.; Øverland, S. Insomnia symptoms and use of health care services and medications: The HUNT-2 study. Behav. Sleep Med. 2009, 7, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Winkelman, J.W. Insomnia disorder. NEJM 2015, 373, 1437–1444. [Google Scholar] [CrossRef]
- Bent, S.; Padula, A.; Moore, D.; Patterson, M.; Mehling, W. Valerian for sleep: A systematic review and meta-analysis. Am. J. Med. 2006, 119, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Leach, M.J.; Page, A.T. Herbal medicine for insomnia: A systematic review and meta-analysis. Sleep Med. Rev. 2015, 24, 1–12. [Google Scholar] [CrossRef]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D. Management of chronic insomnia disorder in adults: A clinical practice guideline from the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Dolenc Groselj, L.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef]
- Sateia, M.J.; Buysse, D.J.; Krystal, A.D.; Neubauer, D.N.; Heald, J.L. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: An American Academy of Sleep Medicine clinical practice guideline. J. Clin. Sleep Med. 2017, 13, 307–349. [Google Scholar] [CrossRef]
- French, D.D.; Spehar, A.M.; Campbell, R.R.; Palacios, P.; Coakley, R.W.; Coblio, N.; Means, H.; Werner, D.C.; Angaran, D.M. Outpatient benzodiazepine prescribing, adverse events, and costs. Adv. Patient Saf. Res. Implement. 2005, 1, 185–198. [Google Scholar]
- Gray, S.L.; Dublin, S.; Yu, O.; Walker, R.; Anderson, M.; Hubbard, R.A.; Crane, P.K.; Larson, E.B. Benzodiazepine use and risk of incident dementia or cognitive decline: Prospective population based study. BMJ 2016, 352, i90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billioti de Gage, S.; Pariente, A.; Bégaud, B. Is there really a link between benzodiazepine use and the risk of dementia? Opin. Drug Saf. 2015, 14, 733–747. [Google Scholar] [CrossRef] [PubMed]
- Lane, J.D.; Kasian, S.J.; Owens, J.E.; Marsh, G.R. Binaural auditory beats affect vigilance performance and mood. Physiol. Behav. 1998, 63, 249–252. [Google Scholar] [CrossRef]
- Padmanabhan, R.; Hildreth, A.; Laws, D. A prospective, randomised, controlled study examining binaural beat audio and pre-operative anxiety in patients undergoing general anaesthesia for day case surgery. Anaesthesia 2005, 60, 874–877. [Google Scholar] [CrossRef]
- Wahbeh, H.; Calabrese, C.; Zwickey, H. Binaural beat technology in humans: A pilot study to assess psychologic and physiologic effects. J. Altern. Complement. Med. 2007, 13, 25–32. [Google Scholar] [CrossRef]
- Draganova, R.; Ross, B.; Wollbrink, A.; Pantev, C. Cortical steady-state responses to central and peripheral auditory beats. Cereb. Cortex. 2008, 18, 1193–1200. [Google Scholar] [CrossRef] [Green Version]
- Wernick, J.S.; Starr, A. Binaural interaction in the superior olivary complex of the cat: An analysis of field potentials evoked by binaural-beat stimuli. J. Neurophysiol. 1968, 31, 428–441. [Google Scholar] [CrossRef]
- Schwarz, D.W.; Taylor, P. Human auditory steady state responses to binaural and monaural beats. Clin. Neurophysiol. 2005, 116, 658–668. [Google Scholar] [CrossRef]
- Karino, S.; Yumoto, M.; Itoh, K.; Uno, A.; Yamakawa, K.; Sekimoto, S.; Kaga, K. Neuromagnetic responses to binaural beat in human cerebral cortex. J. Neurophysiol. 2006, 96, 1927–1938. [Google Scholar] [CrossRef]
- Gao, X.; Cao, H.; Ming, D.; Qi, H.; Wang, X.; Wang, X.; Chen, R.; Zhou, P. Analysis of EEG activity in response to binaural beats with different frequencies. Int. J. Psychophysiol. 2014, 94, 399–406. [Google Scholar] [CrossRef]
- Stevens, L.; Haga, Z.; Queen, B.; Brady, B.; Adams, D.; Gilbert, J.; Vaughan, E.; Leach, C.; Nockels, P.; McManus, P. Binaural beat induced theta EEG activity and hypnotic susceptibility: Contradictory results and technical considerations. Am. J. Clin. Hypn. 2003, 45, 295–309. [Google Scholar] [CrossRef] [PubMed]
- Grose, J.H.; Mamo, S.K. Electrophysiological measurement of binaural beats: Effects of primary tone frequency and observer age. Ear Hear 2012, 32, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavallee, C.F.; Koren, S.A.; Persinger, M.A. A quantitative electroencephalographic study of meditation and binaural beat entrainment. J. Altern. Complement. Med. 2011, 17, 351–355. [Google Scholar] [CrossRef]
- Bonnet, M.H.; Arand, D.L. Hyperarousal and insomnia: State of the science. Sleep Med. Rev. 2010, 14, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Thorpy, M. International classification of sleep disorders. In Sleep Disorders Medicine; Springer: New York, NY, USA, 2017; pp. 475–484. [Google Scholar]
- Bang, Y.R.; yun Choi, H.; Yoon, I.-Y. Minimal effects of binaural auditory beats for subclinical insomnia: A randomized double-blind controlled study. J. Clin. Psychopharmacol. 2019, 39, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Thatcher, R.W.; Biver, C.J.; North, D.M. Real-Time Z Scores; Applied Neuroscience, Inc.: Seminole, FL, USA, 2002. [Google Scholar]
- Carrier, J.; Land, S.; Buysse, D.J.; Kupfer, D.J.; Monk, T.H. The effects of age and gender on sleep EEG power spectral density in the middle years of life (ages 20–60 years old). Psychophysiology 2001, 38, 232–242. [Google Scholar] [CrossRef]
- Latta, F.; Leproult, R.; Tasali, E.; Hofmann, E.; Van Cauter, E. Sex differences in delta and alpha EEG activities in healthy older adults. Sleep 2005, 28, 1525–1534. [Google Scholar] [CrossRef] [Green Version]
- Park, S.-K.; Sang-Ouk, L.; Jeong, I.-t.; Ju-Mong, K. Audio Apparatus and Method for inducing Brainwave Using Binaural Beat. U.S. Patent 10029066, 24 July 2018. [Google Scholar]
- Iwanaga, M.; Ikeda, M.; Iwaki, T. The effects of repetitive exposure to music on subjective and physiological responses. J. Music Ther. 1996, 33, 219–230. [Google Scholar] [CrossRef]
- Lai, H.-L.; Chang, E.-T.; Li, Y.-M.; Huang, C.-Y.; Lee, L.-H.; Wang, H.-M. Effects of music videos on sleep quality in middle-aged and older adults with chronic insomnia: A randomized controlled trial. Biol. Res. Nurs 2015, 17, 340–347. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Chang, E.-T.; Lai, H.-L. Comparing the effects of music and exercise with music for older adults with insomnia. Appl. Nurs. Res. 2016, 32, 104–110. [Google Scholar] [CrossRef]
- Chang, E.-T.; Lai, H.-L.; Chen, P.-W.; Hsieh, Y.-M.; Lee, L.-H. The effects of music on the sleep quality of adults with chronic insomnia using evidence from polysomnographic and self-reported analysis: A randomized control trial. Int. J. Nurs. Stud. 2012, 49, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-F.; Sun, Y.-L.; Zang, H.-X. Music therapy improves sleep quality in acute and chronic sleep disorders: A meta-analysis of 10 randomized studies. Intern. J. Nurs. Stud. 2014, 51, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Lazic, S.E.; Ogilvie, R.D. Lack of efficacy of music to improve sleep: A polysomnographic and quantitative EEG analysis. Intern. J. Psychophysiol. 2007, 63, 232–239. [Google Scholar] [CrossRef]
- McConnell, P.A.; Froeliger, B.; Garland, E.L.; Ives, J.C.; Sforzo, G.A. Auditory driving of the autonomic nervous system: Listening to theta-frequency binaural beats post-exercise increases parasympathetic activation and sympathetic withdrawal. Front. Psychol. 2014, 5, 1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiland, T.J.; Jelinek, G.A.; Macarow, K.E.; Samartzis, P.; Brown, D.M.; Grierson, E.M.; Winter, C. Original sound compositions reduce anxiety in emergency department patients: A randomised controlled trial. Med. J. Aust. 2011, 195, 694–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strijkstra, A.M.; Beersma, D.G.; Drayer, B.; Halbesma, N.; Daan, S. Subjective sleepiness correlates negatively with global alpha (8–12 Hz) and positively with central frontal theta (4–8 Hz) frequencies in the human resting awake electroencephalogram. Neurosci. Lett. 2003, 340, 17–20. [Google Scholar] [CrossRef]
- Takahashi, T.; Murata, T.; Hamada, T.; Omori, M.; Kosaka, H.; Kikuchi, M.; Yoshida, H.; Wada, Y. Changes in EEG and autonomic nervous activity during meditation and their association with personality traits. Int. J. Psychophysiol. 2005, 55, 199–207. [Google Scholar] [CrossRef]
- Lagopoulos, J.; Xu, J.; Rasmussen, I.; Vik, A.; Malhi, G.S.; Eliassen, C.F.; Arntsen, I.E.; Sæther, J.G.; Hollup, S.; Holen, A.; et al. Increased theta and alpha EEG activity during nondirective meditation. J. Altern. Complement. Med. 2009, 15, 1187–1192. [Google Scholar] [CrossRef]
- Ishii, R.; Canuet, L.; Ishihara, T.; Aoki, Y.; Ikeda, S.; Hata, M.; Katsimichas, T.; Gunji, A.; Takahashi, H.; Nakahachi, T.; et al. Frontal midline theta rhythm and gamma power changes during focused attention on mental calculation: An MEG beamformer analysis. Front. Hum. Neurosci. 2014, 8, 406. [Google Scholar] [CrossRef] [Green Version]
- Jirakittayakorn, N.; Wongsawat, Y. Brain responses to a 6-Hz binaural beat: Effects on general theta rhythm and frontal midline theta activity. Front. Neurosci. 2017, 11, 365. [Google Scholar] [CrossRef]
- López-Caballero, F.; Escera, C. Binaural beat: A failure to enhance EEG power and emotional arousal. Front. Hum. Neurosci. 2017, 11, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Total (N =43) | Music (N = 23) | Music with Binaural Beat (N = 20) | p | |
|---|---|---|---|---|
| Age, yr | 34.3 ± 10.4 | 32.8 ± 9.4 | 35.9 ± 11.4 | 0.338 |
| Sex | Men: N = 10 Women: N = 32 | Men: N = 6 Women: N = 16 | Men: N = 4 Women: N = 16 | 0.434 |
| BMI, kg/m2 | 22.5 ± 3.0 | 22.0 ± 2.4 | 23.0 ± 3.7 | 0.318 |
| PSQI score | 8.7 ± 2.7 | 8.7 ± 2.4 | 8.7 ± 3.0 | 0.956 |
| ESS | 9.1 ± 4.1 | 8.9 ± 3.6 | 9.3 ± 4.8 | 0.794 |
| ISI | 9.9 ± 3.1 | 10.0 ± 3.1 | 9.7 ± 3.2 | 0.721 |
| BDI | 8.1 ± 4.6 | 8.4 ± 4.8 | 7.8 ± 4.5 | 0.632 |
| STAI-S | 39.1 ± 9.2 | 37.9 ± 8.8 | 40.5 ± 9.6 | 0.364 |
| AHI, n/h | 1.6 ± 3.3 | 0.8 ± 1.6 | 2.5 ± 4.5 | 0.121 |
| WASO, min | 57.5 ± 61.0 | 61.8 ± 75.2 | 52.6 ± 40.3 | 0.628 |
| TST, min | 390.7 ± 71.0 | 392.1 ± 78.7 | 389.1 ± 63.0 | 0.893 |
| Sleep latency, min | 23.1 ± 24.8 | 18.2 ± 12.2 | 28.7 ± 33.5 | 0.197 |
| Sleep efficiency, % | 82.8 ± 14.2 | 83.0 ± 16.2 | 82.6 ± 11.8 | 0.917 |
| Stage 1, % | 7.4 ± 4.5 | 7.7 ± 5.1 | 7.1 ± 3.8 | 0.674 |
| Stage 2, % | 47.2 ± 8.4 | 47.7 ± 8.2 | 46.7 ± 8.9 | 0.707 |
| Stage 3, % | 15.9 ± 6.2 | 14.8 ± 5.0 | 17.1 ± 7.2 | 0.212 |
| REM, % | 17.8 ± 5.7 | 18.3 ± 5.8 | 17.2 ± 5.8 | 0.537 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.; Bang, Y.; Yoon, I.-Y.; Choi, H.-Y. Entrapment of Binaural Auditory Beats in Subjects with Symptoms of Insomnia. Brain Sci. 2022, 12, 339. https://doi.org/10.3390/brainsci12030339
Lee E, Bang Y, Yoon I-Y, Choi H-Y. Entrapment of Binaural Auditory Beats in Subjects with Symptoms of Insomnia. Brain Sciences. 2022; 12(3):339. https://doi.org/10.3390/brainsci12030339
Chicago/Turabian StyleLee, Eunyoung, Youngrong Bang, In-Young Yoon, and Ha-Yun Choi. 2022. "Entrapment of Binaural Auditory Beats in Subjects with Symptoms of Insomnia" Brain Sciences 12, no. 3: 339. https://doi.org/10.3390/brainsci12030339
APA StyleLee, E., Bang, Y., Yoon, I.-Y., & Choi, H.-Y. (2022). Entrapment of Binaural Auditory Beats in Subjects with Symptoms of Insomnia. Brain Sciences, 12(3), 339. https://doi.org/10.3390/brainsci12030339