
Association between Changes in White Matter Microstructure and Cognitive Impairment in White Matter Lesions

Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
2.3. Clinical Data Collection
2.4. Cognitive Measures
2.5. Image Acquisition
2.6. DTI Data Pre-Processing
2.7. TBSS Analysis
2.8. Statistical Analyses
2.9. TBSS Voxel-Wise Statistical Analyses
2.10. ROI-Wise Statistical Analysis
3. Results
3.1. Participant Characteristics
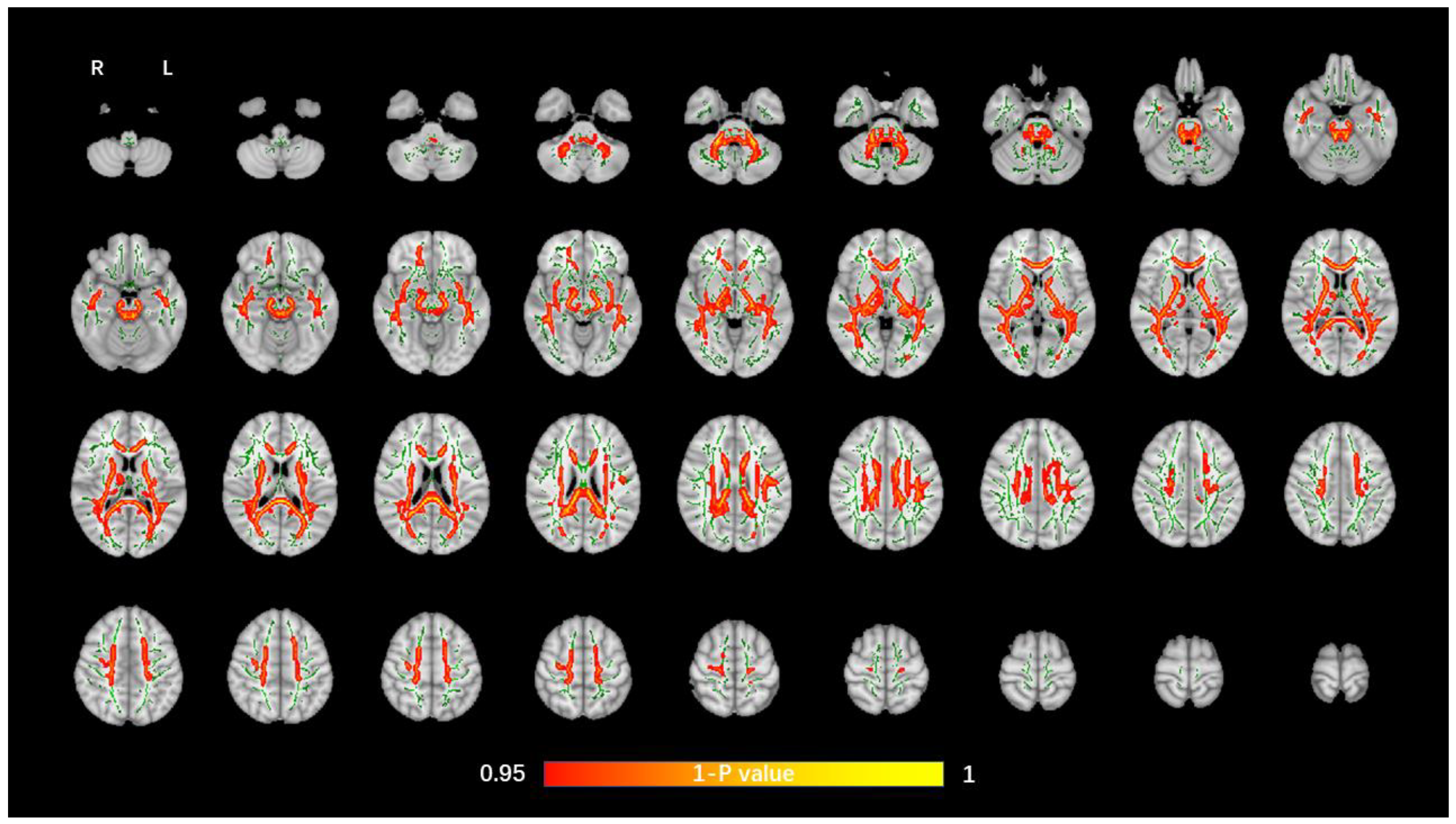
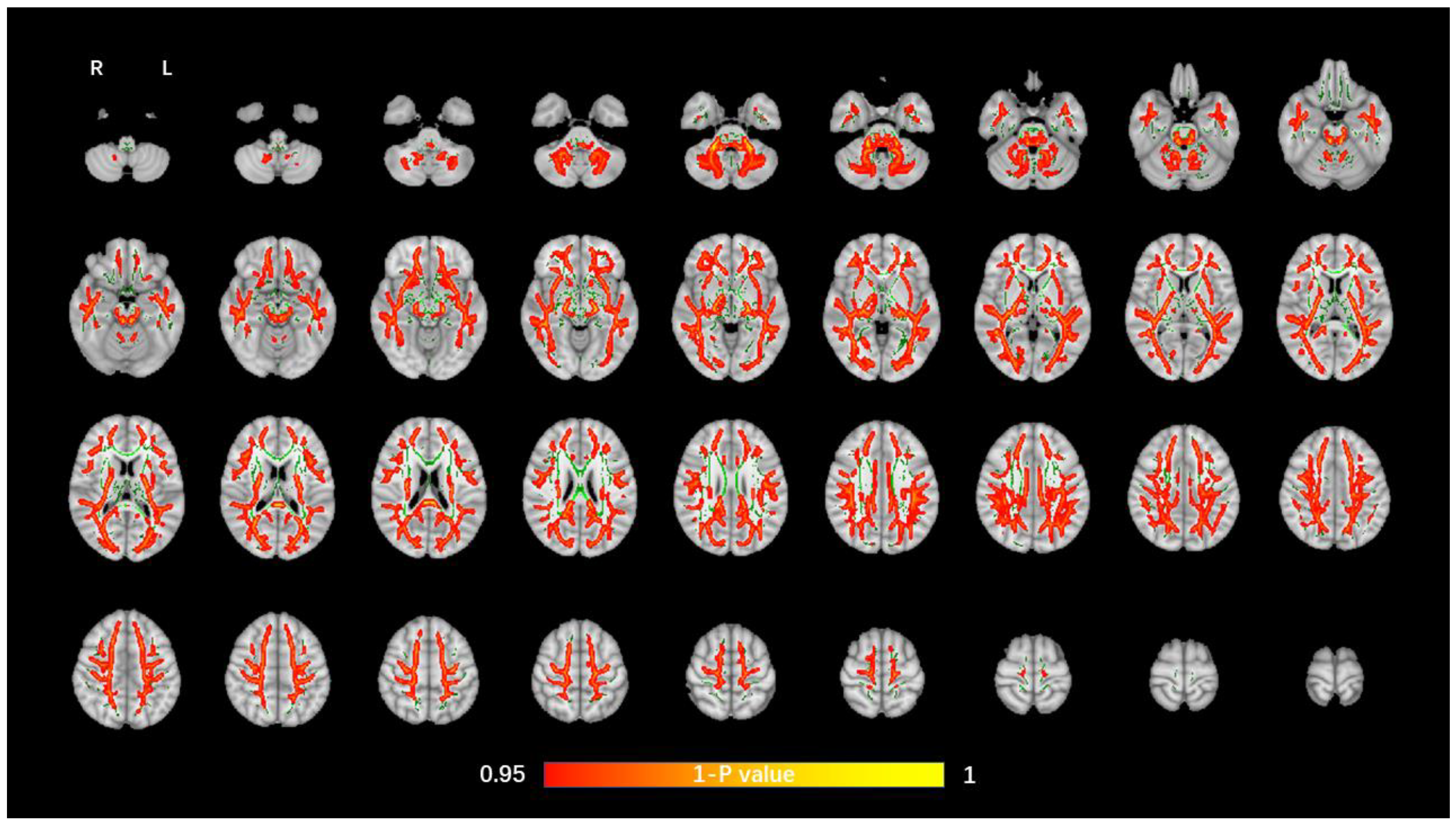
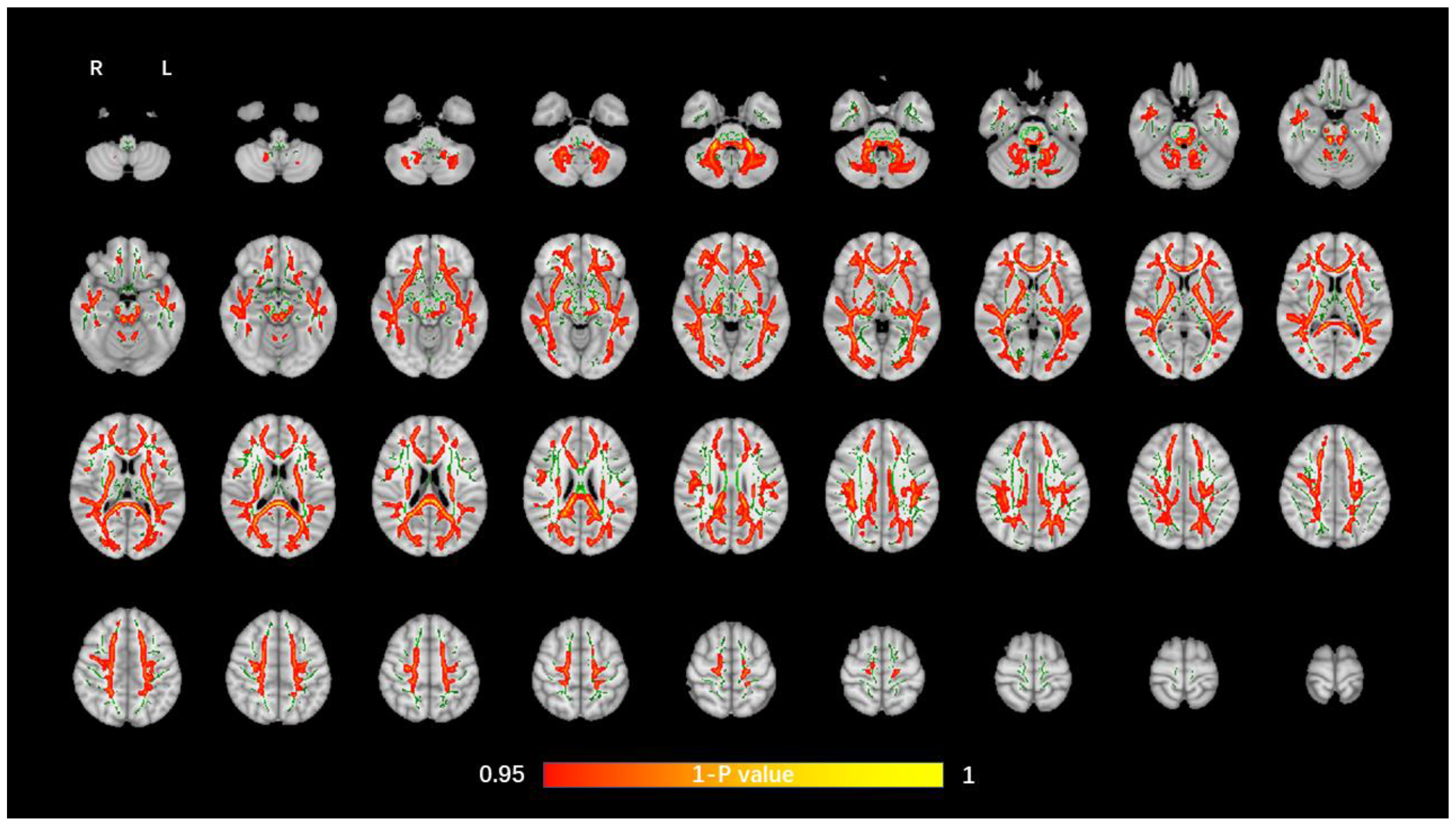
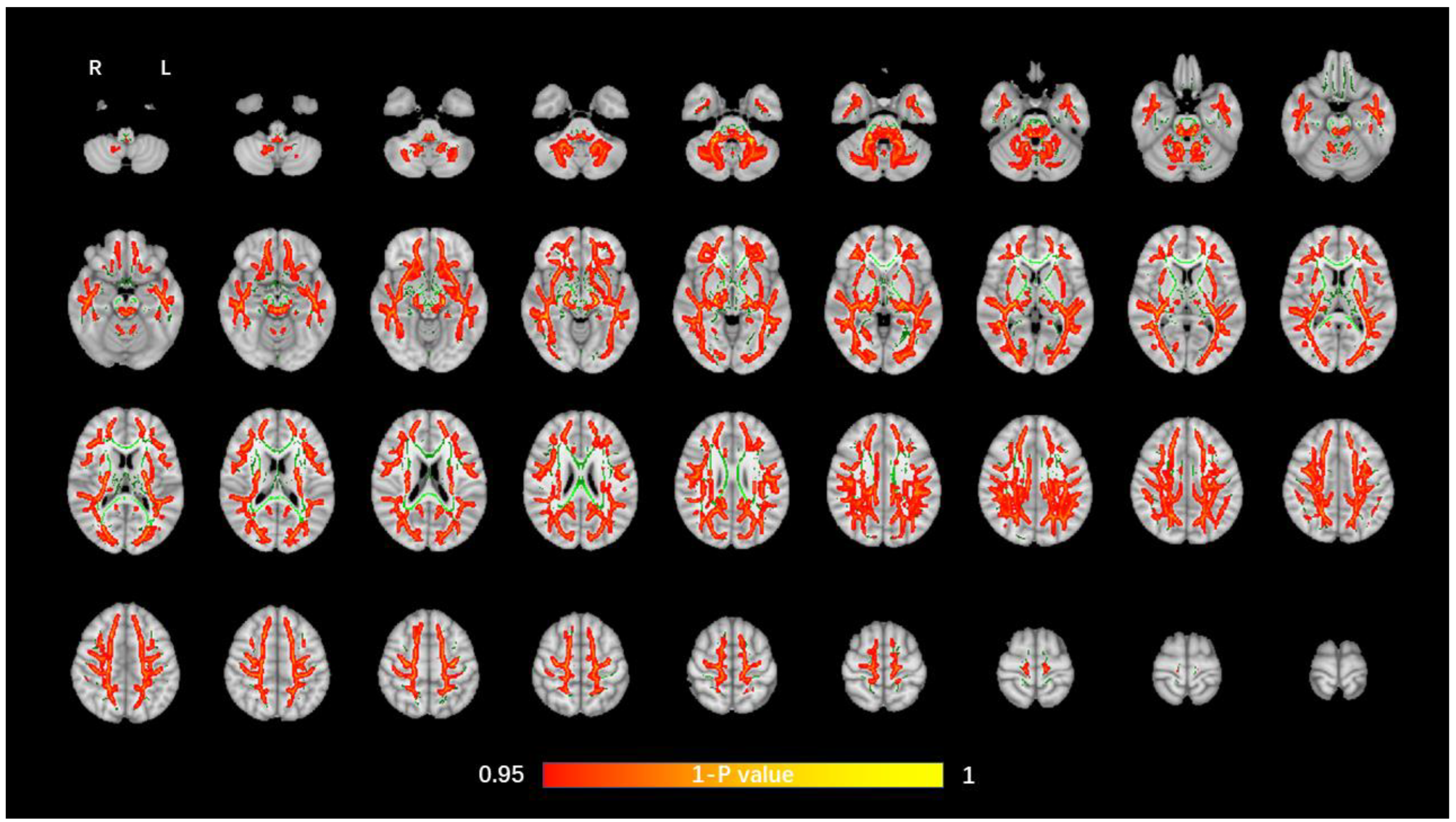
3.2. TBSS Analysis of DTI Data
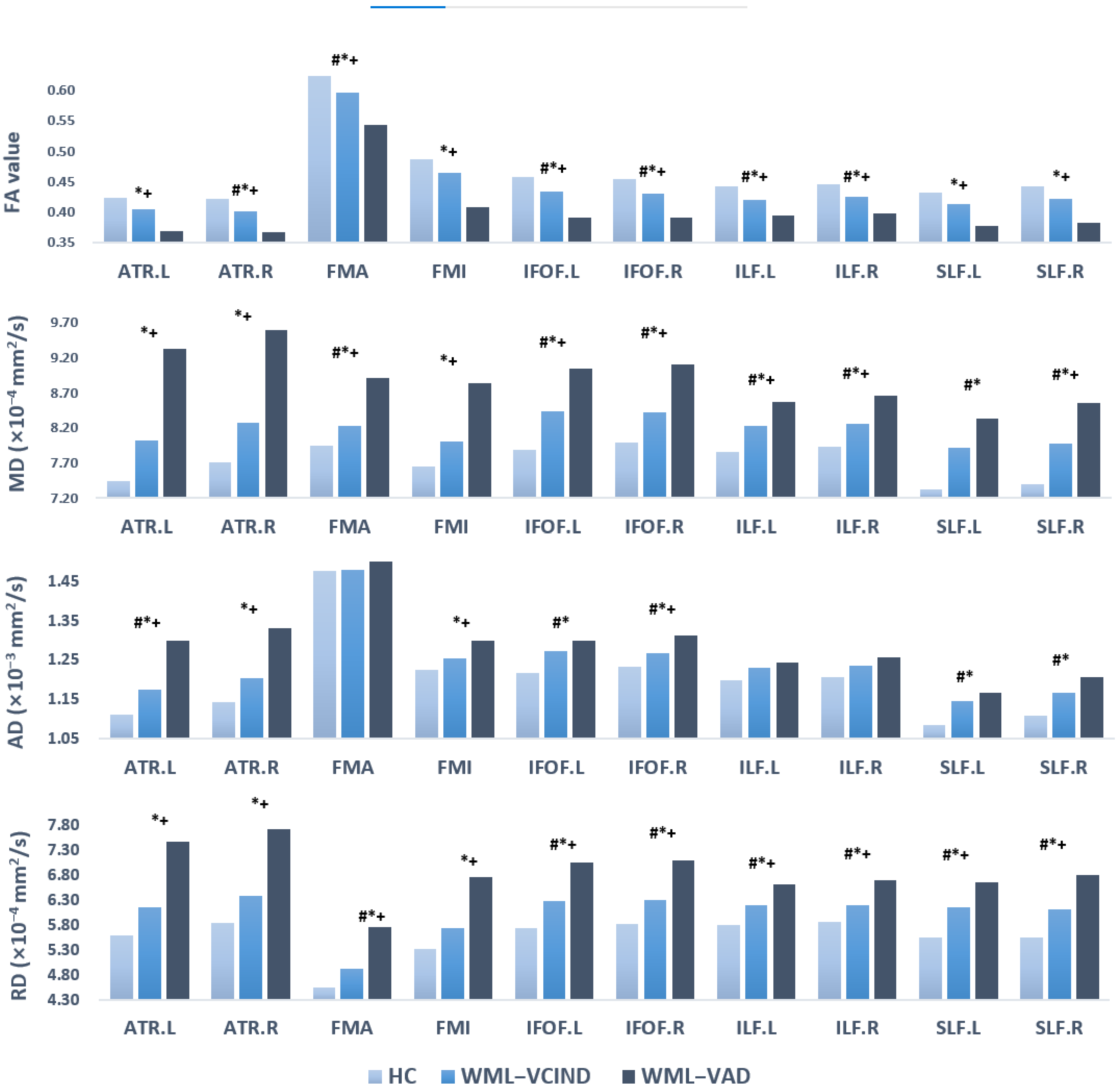
3.3. ROI Analyses
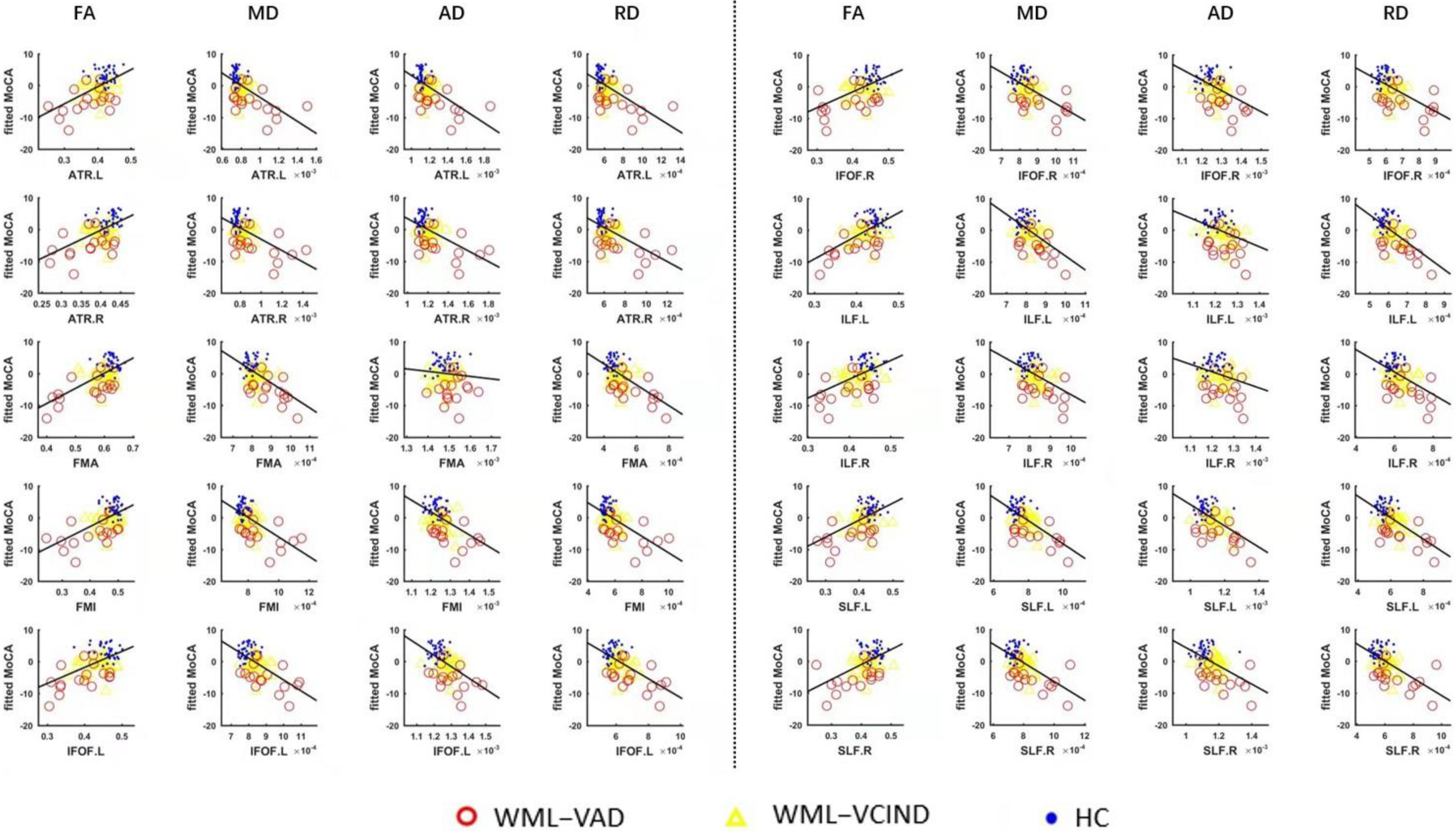
3.4. Correlation Analysis Results between the DTI Index in ROI and MoCA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alber, J.; Alladi, S.; Bae, H.J.; Barton, D.A.; Beckett, L.A.; Bell, J.M.; Berman, S.E.; Biessels, G.J.; Black, S.E.; Bos, I.; et al. White matter hyperintensities in vascular contributions to cognitive impairment and dementia (VCID): Knowledge gaps and opportunities. Alzheimer’s Dement. 2019, 5, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Weissert, R.; Bhaskar, S.M.M. Emerging role of white matter lesions in cerebrovascular disease. Eur. J. Neurosci. 2021, 54, 5531–5559. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; Malherbe, C.; Cheng, B.; Thomalla, G.; Schlemm, E. Functional connectivity changes in cerebral small vessel disease—A systematic review of the resting-state MRI literature. BMC Med. 2021, 19, 103. [Google Scholar] [CrossRef]
- Raja, R.; Rosenberg, G.; Caprihan, A. Review of diffusion MRI studies in chronic white matter diseases. Neurosci. Lett. 2019, 694, 198–207. [Google Scholar] [CrossRef]
- Croall, I.D.; Lohner, V.; Moynihan, B.; Khan, U.; Hassan, A.; O’Brien, J.; Morris, R.G.; Tozer, D.J.; Cambridge, V.C.; Harkness, K.; et al. Using DTI to assess white matter microstructure in cerebral small vessel disease (SVD) in multicentre studies. Clin. Sci. 2017, 131, 1361–1373. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Qun, X.; Qin, L.D.; Qian, L.J.; Cao, W.W.; Xu, J.R. A primary study of diffusion tensor imaging-based histogram analysis in vascular cognitive impairment with no dementia. Clin. Neurol. Neurosurg. 2011, 113, 92–97. [Google Scholar] [CrossRef]
- Cai, M.; Jacob, M.A.; Norris, D.G.; de Leeuw, F.E.; Tuladhar, A.M. Longitudinal relation between structural network efficiency, cognition, and gait in cerebral small vessel disease. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 77, 554–560. [Google Scholar] [CrossRef]
- Kalaria, R.N. Neuropathological diagnosis of vascular cognitive impairment and vascular dementia with implications for Alzheimer’s disease. Acta Neuropathol. 2016, 131, 659–685. [Google Scholar] [CrossRef]
- Liu, Y.; Duan, Y.; He, Y.; Yu, C.; Wang, J.; Huang, J.; Ye, J.; Butzkueven, H.; Li, K.; Shu, N. A tract-based diffusion study of cerebral white matter in neuromyelitis optica reveals widespread pathological alterations. Mult. Scler. 2012, 18, 1013. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Hernandez, M.C.V.; Muñoz-Maniega, S. What are white matter hyperintensities made of? relevance to vascular cognitive impairment. J. Am. Heart Assoc. 2015, 4, 001140. [Google Scholar] [CrossRef]
- Alexander, A.L.; Hurley, S.A.; Samsonov, A.A.; Adluru, N.; Hosseinbor, A.P.; Mossahebi, P.; Tromp, D.P.M.; Zakszewski, E.; Field, A.S. Characterization of cerebral white matter properties using quantitative magnetic resonance imaging stains. Brain Connect. 2011, 1, 423–446. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Friston, K. Structural and functional brain networks: From connections to cognition. Science 2013, 342, 579. [Google Scholar] [CrossRef] [PubMed]
- Dhamala, E.; Jamison, K.W.; Jaywant, A.; Dennis, S.; Kuceyeski, A. Distinct functional and structural connections predict crystallised and fluid cognition in healthy adults. Hum. Brain Mapp. 2021, 42, 3102–3118. [Google Scholar] [CrossRef]
- Chen, H.F.; Huang, L.L.; Li, H.Y.; Qian, Y.; Yang, D.; Qing, Z.; Luo, C.M.; Li, M.C.; Zhang, B.; Xu, Y. Microstructural disruption of the right inferior fronto-occipital and inferior longitudinal fasciculus contributes to WMH-related cognitive impairment. CNS Neurosci. Ther. 2020, 26, 576–588. [Google Scholar] [CrossRef] [PubMed]
- Zhong, G.; Lou, M. Multimodal imaging findings in normal-appearing white matter of leucoaraiosis: A review. Stroke Vasc. Neurol. 2016, 1, 59–63. [Google Scholar] [CrossRef]
- Tomimoto, H. White matter integrity and cognitive dysfunction: Radiological and neuropsychological correlations. Geriatr. Gerontol. Int. 2015, 15, 3–9. [Google Scholar] [CrossRef]
- Petersen, M.; Frey, B.M.; Mayer, C.; Kühn, S.; Gallinat, J.; Hanning, U.; Fiehler, J.; Borof, K.; Jagodzinski, A.; Gerloff, C.; et al. Fixel based analysis of white matter alterations in early stage cerebral small vessel disease. Sci. Rep. 2022, 12, 1581. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Tian, T.; Fan, Y.; Yang, S.; Xiong, X.; Zhang, Q.; Zhu, W. Diffusion tensor imaging reveals altered topological efficiency of structural networks in type-2 diabetes patients with and without mild cognitive impairment. J. Magn. Reson. Imaging 2022, 55, 917–927. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage 2006, 31, 1487–1505. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef]
- Magierska, J.; Magierski, R.; Fendler, W.; Kloszewska, I.; Sobow, T.M. Clinical application of the polish adaptation of the montreal cognitive assessment (moca) test in screening for cognitive impairment. Neurol. Neurochir Pol. 2012, 46, 130–139. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The montreal cognitive assessment, moca: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C. The clinical dementia rating (cdr): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Zhong, S.; Xu, P.; Yong, H.; Gong, G. PANDA: A pipeline toolbox for analyzing brain diffusion images. Front. Hum. Neurosci. 2013, 7, 42. [Google Scholar] [CrossRef]
- Peng, D. Geriatric neurology group, chinese society of geriatrics; clinical practice guideline for cognitive impairment of cerebral small vessel disease writing group. clinical practice guideline for cognitive impairment of cerebral small vessel disease. Aging Med. 2019, 2, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, Y.; Yamauchi, H.; Sawamoto, N.; Iseki, K.; Tomimoto, H.; Fukuyama, H. Diffuse tract damage in the hemispheric deep white matter may correlate with global cognitive impairment and callosal atrophy in patients with extensive leukoaraiosis. AJNR Am. J. Neuroradiol. 2012, 33, 726. [Google Scholar] [CrossRef]
- Lu, T.; Wang, Z.; Cui, Y.; Zhou, J.; Wang, Y.; Ju, S. Disrupted structural brain connectome is related to cognitive impairment in patients with ischemic leukoaraiosis. Front. Hum. Neurosci. 2021, 15, 654750. [Google Scholar] [CrossRef]
- Chen, H.J.; Gao, Y.Q.; Che, C.H.; Lin, H.; Ruan, X.-L. Diffusion tensor imaging with tract-based spatial statistics reveals white matter abnormalities in patients with vascular cognitive impairment. Front. Neuroanat. 2018, 12, 53. [Google Scholar] [CrossRef]
- Benson, G.; Hildebrandt, A.; Lange, C.; Schwarz, C.; Köbe, T.; Sommer, W.; Flöel, A.; Wirth, M. Functional connectivity in cognitive control networks mitigates the impact of white matter lesions in the elderly. Alzheimer’s Res. Ther. 2018, 10, 109. [Google Scholar] [CrossRef]
- Li, L.; Coles, C.D.; Lynch, M.E.; Hu, X. Voxelwise and skeleton-based region of interest analysis of fetal alcohol syndrome and fetal alcohol spectrum disorders in young adults. Hum. Brain Mapp. 2009, 47, S47. [Google Scholar] [CrossRef]
- Klarborg, B.; Skak Madsen, K.; Vestergaard, M.; Skimminge, A.; Jernigan, T.L.; Baaré, W.F. Sustained attention is associated with right superior longitudinal fasciculus and superior parietal white matter microstructure in children. Hum. Brain. Mapp. 2013, 34, 3216–3232. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Sun, D.; Yong, W.; Wang, Y. Subcomponents and connectivity of the inferior fronto-occipital fasciculus revealed by diffusion spectrum imaging fiber tracking. Front. Neuroanat. 2016, 10, 88. [Google Scholar] [CrossRef] [PubMed]
- Vergani, F.; Ghimire, P.; Rajashekhar, D.; Dell’acqua, F.; Lavrador, J.P. Superior longitudinal fasciculus (SLF) I and II: An anatomical and functional review. J. Neurosurg. Sci. 2021, 65, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Tu, M.C.; Lo, C.P.; Huang, C.F.; Hsu, Y.H.; Huang, W.H.; Deng, J.F.; Lee, Y.C. Effectiveness of diffusion tensor imaging in differentiating early-stage subcortical ischemic vascular disease, Alzheimer’s disease and normal ageing. PLoS ONE 2017, 12, e0175143. [Google Scholar] [CrossRef]
- Wang, Z.; Bai, L.; Liu, Q.; Wang, S.; Sun, C.; Zhang, M.; Zhang, Y. Corpus callosum integrity loss predicts cognitive impairment in Leukoaraiosis. Ann. Clin. Transl. Neurol. 2020, 7, 2409–2420. [Google Scholar] [CrossRef]
- Crockett, R.A.; Hsu, C.L.; Dao, E.; Tam, R.; Alkeridy, W.; Eng, J.J.; Handy, T.C.; Liu-Ambrose, T. Mind the Gaps: Functional networks disrupted by white matter hyperintensities are associated with greater falls risk. Neurobiol. Aging 2022, 109, 166–175. [Google Scholar] [CrossRef]
- Tuladhar, A.M.; van Norden, A.G.; de Laat, K.F.; Zwiers, M.P.; van Dijk, E.J.; Norris, D.G.; de Leeuw, F.E. White matter integrity in small vessel disease is related to cognition. Neuroimage Clin. 2015, 7, 518–524. [Google Scholar] [CrossRef]
- Zhang, C.E.; Wong, S.M.; Uiterwijk, R.; Staals, J.; Backes, W.H.; Hoff, E.I.; Schreuder, T.; Jeukens, C.R.; Jansen, J.F.; van Oostenbrugge, R.J. Intravoxel incoherent motion imaging in small vessel disease: Microstructural integrity and microvascular perfusion related to cognition. Stroke 2017, 48, 658–663. [Google Scholar] [CrossRef]
- Tuladhar, A.M.; van Dijk, E.; Zwiers, M.P.; van Norden, A.G.; de Laat, K.F.; Shumskaya, E.; Norris, D.G.; de Leeuw, F.E. Structural network connectivity and cognition in cerebral small vessel disease. Hum. Brain Mapp. 2016, 37, 300–310. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HC (n = 37) | WML-VCIND (n = 33) | WML-VaD (n = 17) | p-Value | |
|---|---|---|---|---|
| Age (years) | 58.84 ± 7.80 | 64.00 ± 9.40 # | 65.12 ± 9.10 * | 0.015 b |
| Sex (male/female, n) | 20/17 | 16/17 | 14/3 | 0.062 a |
| Education level (years) | 12.68 ± 2.84 | 11.55 ± 2.54 | 11.76 ± 2.97 | 0.209 b |
| Hypertension (n) | 24 | 24 | 7 | 0.087 a |
| Diabetes (n) | 31 | 27 | 14 | 0.975 a |
| Hyperlipemia (n) | 30 | 26 | 14 | 0.948 a |
| MoCA score | 27.41 ± 1.41 | 21.84 ± 2.49 # | 17.71 ± 4.05 *,† | <0.001 b |
| Visuospatial/Executive | 4.59 ± 1.04 | 3.41 ± 1.17 # | 2.18 ± 0.59 *,† | <0.001 b |
| Naming | 2.97 ± 0.16 | 2.74 ± 0.63 | 2.50 ± 0.73 * | 0.006 b |
| Attention | 5.89 ± 0.39 | 5.06 ± 1.15 # | 4.12 ± 1.45 *,† | <0.001 b |
| languge | 2.45 ± 0.60 | 2.03 ± 0.54 # | 1.43 ± 0.89 *,† | <0.001 b |
| abstraction | 1.81 ± 0.56 | 1.38 ± 0.80 # | 1.12 ± 0.80 * | 0.002 b |
| Delayed recall | 3.70 ± 0.99 | 1.61 ± 1.28 # | 1.43 ± 1.03 * | <0.001 b |
| Orientation | 6.00 ± 0.00 | 5.61 ± 0.71 | 4.93 ± 1.23 *,† | <0.001 b |
| WM Tracts | FA (Mean ± Std) | ANCOVA | Post Hoc Test (Bonferroni) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| WML-VCIND/HC | WML-VAD/HC | WML-VAD/WML-VCIND | |||||||
| HC (n = 37) | WML-VCIND (n = 33) | WML-VAD (n = 17) | F | p | p | p | p | ||
| 1 | ATR.L | 0.424 ± 0.023 | 0.406 ± 0.029 | 0.369 ± 0.059 | 12.636 | <0.001 * | 0.09 | <0.001 * | 0.002 * |
| 2 | ATR.R | 0.422 ± 0.022 | 0.402 ± 0.024 | 0.367 ± 0.054 | 15.464 | <0.001 * | 0.032 * | <0.001 * | 0.001 * |
| 3 | FMA | 0.625 ± 0.024 | 0.596 ± 0.031 | 0.544 ± 0.084 | 16.292 | <0.001 * | 0.025 * | <0.001 * | 0.001 * |
| 4 | FMI | 0.487 ± 0.021 | 0.466 ± 0.033 | 0.408 ± 0.079 | 16.403 | <0.001 * | 0.117 | <0.001 * | <0.001 * |
| 5 | IFOF.L | 0.459 ± 0.026 | 0.435 ± 0.033 | 0.392 ± 0.056 | 14.784 | <0.001 * | 0.021 * | <0.001 * | 0.001 * |
| 6 | IFOF.R | 0.454 ± 0.022 | 0.43 ± 0.031 | 0.392 ± 0.061 | 12.607 | <0.001 * | 0.019 * | <0.001 * | 0.002 * |
| 7 | ILF.L | 0.442 ± 0.019 | 0.42 ± 0.025 | 0.395 ± 0.047 | 13.024 | <0.001 * | 0.004 * | <0.001 * | 0.014 * |
| 8 | ILF.R | 0.445 ± 0.021 | 0.426 ± 0.03 | 0.398 ± 0.049 | 9.717 | <0.001 * | 0.033 * | <0.001 * | 0.011 * |
| 9 | SLF.L | 0.433 ± 0.021 | 0.413 ± 0.032 | 0.378 ± 0.058 | 12.677 | <0.001 * | 0.061 | <0.001 * | 0.004 * |
| 10 | SLF.R | 0.442 ± 0.026 | 0.422 ± 0.032 | 0.383 ± 0.067 | 11.98 | <0.001 * | 0.096 | <0.001 * | 0.003 * |
| WM Tracts | MD (Mean ± Std, ×10−4 mm2/s) | ANCOVA | Post Hoc Test (Bonferroni) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| WML-VCIND/HC | WML-VAD/HC | WML-VAD/WML-VCIND | |||||||
| HC (n = 37) | WML-VCIND (n = 33) | WML-VAD (n = 17) | F | p | p | p | p | ||
| 1 | ATR.L | 7.446 ± 0.376 | 8.029 ± 0.501 | 9.329 ± 2.153 | 18.479 | <0.001 * | 0.057 | <0.001 * | <0.001 * |
| 2 | ATR.R | 7.706 ± 0.388 | 8.279 ± 0.563 | 9.593 ± 2.137 | 17.417 | <0.001 * | 0.067 | <0.001 * | <0.001 * |
| 3 | FMA | 7.953 ± 0.315 | 8.225 ± 0.355 | 8.906 ± 0.804 | 18.206 | <0.001 * | 0.049 * | <0.001 * | <0.001 * |
| 4 | FMI | 7.645 ± 0.262 | 8.013 ± 0.444 | 8.840 ± 1.267 | 18.063 | <0.001 * | 0.055 | <0.001 * | <0.001 * |
| 5 | IFOF.L | 7.891 ± 0.33 | 8.440 ± 0.429 | 9.041 ± 1.054 | 19.713 | <0.001 * | <0.001 * | <0.001 * | 0.002 * |
| 6 | IFOF.R | 7.995 ± 0.335 | 8.428 ± 0.374 | 9.112 ± 1.070 | 18.381 | <0.001 * | 0.006 * | <0.001 * | <0.001 * |
| 7 | ILF.L | 7.867 ± 0.311 | 8.232 ± 0.427 | 8.568 ± 0.693 | 11.37 | <0.001 * | 0.003 * | <0.001 * | 0.043 * |
| 8 | ILF.R | 7.933 ± 0.332 | 8.268 ± 0.434 | 8.658 ± 0.738 | 9.533 | <0.001 * | 0.012 * | <0.001 * | 0.021 * |
| 9 | SLF.L | 7.324 ± 0.349 | 7.920 ± 0.448 | 8.337 ± 1.093 | 17.883 | <0.001 * | <0.001 * | <0.001 * | 0.065 |
| 10 | SLF.R | 7.395 ± 0.421 | 7.973 ± 0.440 | 8.565 ± 1.299 | 16.276 | <0.001 * | 0.002 * | <0.001 * | 0.015 * |
| WM Tracts | AD (Mean ± Std, ×10−3 mm2/s) | ANCOVA | Post Hoc Test (Bonferroni) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| WML-VCIND/HC | WML-VAD/HC | WML-VAD/WML-VCIND | |||||||
| HC (n = 37) | WML-VCIND (n = 33) | WML-VAD (n = 17) | F | p | p | p | p | ||
| 1 | ATR.L | 1.112 ± 0.039 | 1.175 ± 0.052 | 1.301 ± 0.214 | 18.364 | <0.001 * | 0.036 * | <0.001 * | <0.001 * |
| 2 | ATR.R | 1.144 ± 0.041 | 1.205 ± 0.063 | 1.332 ± 0.218 | 15.652 | <0.001 * | 0.059 | <0.001 * | <0.001 * |
| 3 | FMA | 1.477 ± 0.044 | 1.481 ± 0.045 | 1.519 ± 0.057 | 1.708 | 0.188 | |||
| 4 | FMI | 1.226 ± 0.036 | 1.254 ± 0.044 | 1.299 ± 0.081 | 12.632 | <0.001 * | 0.071 | <0.001 * | 0.010 * |
| 5 | IFOF.L | 1.219 ± 0.037 | 1.275 ± 0.043 | 1.300 ± 0.085 | 14.695 | <0.001 * | <0.001 * | <0.001 * | 0.284 |
| 6 | IFOF.R | 1.234 ± 0.041 | 1.268 ± 0.039 | 1.313 ± 0.074 | 13.16 | <0.001 * | 0.013 * | <0.001 * | 0.009 * |
| 7 | ILF.L | 1.200 ± 0.043 | 1.230 ± 0.049 | 1.245 ± 0.057 | 4.291 | 0.017 | |||
| 8 | ILF.R | 1.208 ± 0.040 | 1.237 ± 0.051 | 1.258 ± 0.061 | 4.165 | 0.019 | |||
| 9 | SLF.L | 1.084 ± 0.044 | 1.145 ± 0.052 | 1.168 ± 0.098 | 12.393 | <0.001 * | <0.001 * | <0.001 * | 0.603 |
| 10 | SLF.R | 1.108 ± 0.051 | 1.166 ± 0.049 | 1.206 ± 0.108 | 12.505 | <0.001 * | 0.001 * | <0.001 * | 0.119 |
| WM Tracts | RD (Mean ± Std, ×10−4 mm2/s) | ANCOVA | Post Hoc Test (Bonferroni) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| WML-VCIND/HC | WML-VAD/HC | WML-VAD/WML-VCIND | |||||||
| HC (n = 37) | WML-VCIND (n = 33) | WML-VAD (n = 17) | F | p | p | p | p | ||
| 1 | ATR.L | 5.607 ± 0.396 | 6.171 ± 0.527 | 7.490 ± 2.169 | 18.064 | <0.001 * | 0.076 | <0.001 * | <0.001 * |
| 2 | ATR.R | 5.839 ± 0.403 | 6.396 ± 0.553 | 7.729 ± 2.125 | 17.883 | <0.001 * | 0.077 | <0.001 * | <0.001 * |
| 3 | FMA | 4.545 ± 0.335 | 4.931 ± 0.431 | 5.762 ± 1.145 | 18.384 | <0.001 * | 0.029 * | <0.001 * | <0.001 * |
| 4 | FMI | 5.335 ± 0.270 | 5.748 ± 0.500 | 6.762 ± 1.504 | 18.392 | <0.001 * | 0.069 | <0.001 * | <0.001 * |
| 5 | IFOF.L | 5.744 ± 0.383 | 6.288 ± 0.498 | 7.056 ± 1.188 | 19.17 | <0.001 * | 0.002 * | <0.001 * | 0.001 * |
| 6 | IFOF.R | 5.822 ± 0.350 | 6.300 ± 0.454 | 7.103 ± 1.255 | 17.586 | <0.001 * | 0.009 * | <0.001 * | <0.001 * |
| 7 | ILF.L | 5.802 ± 0.301 | 6.198 ± 0.439 | 6.626 ± 0.797 | 13.693 | <0.001 * | 0.003 * | <0.001 * | 0.012 * |
| 8 | ILF.R | 5.861 ± 0.343 | 6.215 ± 0.468 | 6.700 ± 0.836 | 10.817 | <0.001 * | 0.016 * | <0.001 * | 0.007 * |
| 9 | SLF.L | 5.565 ± 0.360 | 6.156 ± 0.478 | 6.668 ± 1.192 | 18.159 | <0.001 * | 0.001 * | <0.001 * | 0.028 * |
| 10 | SLF.R | 5.552 ± 0.431 | 6.131 ± 0.486 | 6.816 ± 1.438 | 16.102 | <0.001 * | 0.005 * | <0.001 * | 0.009 * |
| WM Tracts | Correlation between FA of WM Tracts and MoCA (r Value) | Correlation between MD of WM Tracts and MoCA (r Value) | Correlation between AD of WM Tracts and MoCA (r Value) | Correlation between RD of WM Tracts and MoCA (r Value) | |
|---|---|---|---|---|---|
| 1 | ATR.L | 0.536 * | −0.571 * | −0.562 * | −0.570 * |
| 2 | ATR.R | 0.529 * | −0.544 * | −0.527 * | −0.546 * |
| 3 | FMA | 0.618 * | −0.584 * | −0.117 | −0.620 * |
| 4 | FMI | 0.570 * | −0.584 * | −0.489 * | −0.589 * |
| 5 | IFOF.L | 0.567 * | −0.645 * | −0.546 * | −0.635 * |
| 6 | IFOF.R | 0.547 * | −0.569 * | −0.444 * | −0.580 * |
| 7 | ILF.L | 0.617 * | −0.595 * | −0.360 * | −0.644 * |
| 8 | ILF.R | 0.527 * | −0.501 * | −0.294 | −0.540 * |
| 9 | SLF.L | 0.509 * | −0.651 * | −0.583 * | −0.642 * |
| 10 | SLF.R | 0.505 * | −0.600 * | −0.542 * | −0.594 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, A.-M.; Ma, Y.-L.; Li, Y.-X.; Han, Z.-Z.; Yan, N.; Zhang, Y.-M. Association between Changes in White Matter Microstructure and Cognitive Impairment in White Matter Lesions. Brain Sci. 2022, 12, 482. https://doi.org/10.3390/brainsci12040482
Hu A-M, Ma Y-L, Li Y-X, Han Z-Z, Yan N, Zhang Y-M. Association between Changes in White Matter Microstructure and Cognitive Impairment in White Matter Lesions. Brain Sciences. 2022; 12(4):482. https://doi.org/10.3390/brainsci12040482
Chicago/Turabian StyleHu, An-Ming, Yan-Ling Ma, Yue-Xiu Li, Zai-Zhu Han, Nan Yan, and Yu-Mei Zhang. 2022. "Association between Changes in White Matter Microstructure and Cognitive Impairment in White Matter Lesions" Brain Sciences 12, no. 4: 482. https://doi.org/10.3390/brainsci12040482
APA StyleHu, A.-M., Ma, Y.-L., Li, Y.-X., Han, Z.-Z., Yan, N., & Zhang, Y.-M. (2022). Association between Changes in White Matter Microstructure and Cognitive Impairment in White Matter Lesions. Brain Sciences, 12(4), 482. https://doi.org/10.3390/brainsci12040482