
Can Disruption of Basal Ganglia-Thalamocortical Circuit in Wilson Disease Be Associated with Juvenile Myoclonic Epilepsy Phenotype?

 , , , and
, , , and
Abstract
:1. Introduction
2. Case Presentation
3. Results
3.1. Voxel Based Morphometry Results
3.2. EEG-fMRI Results
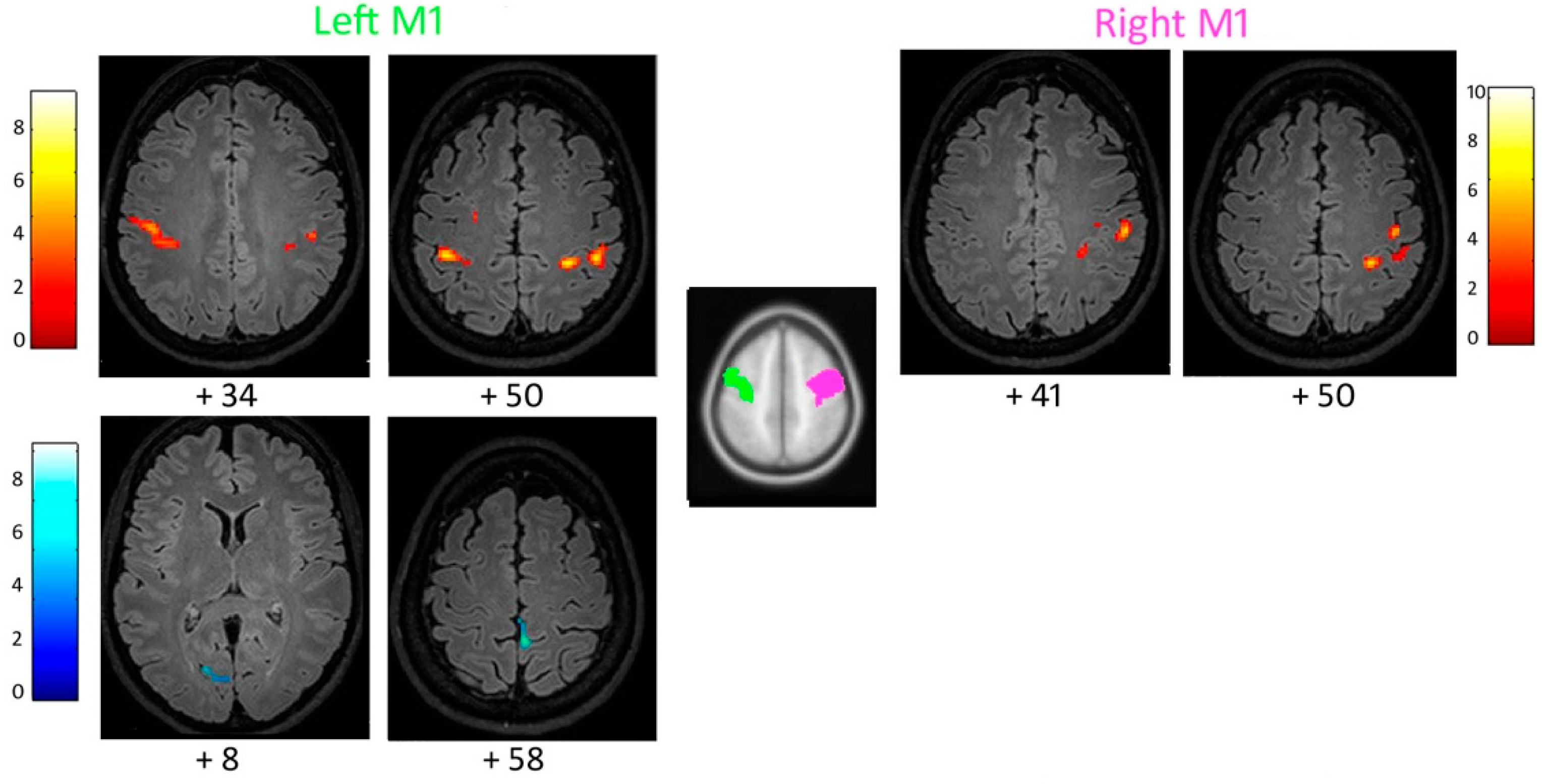
3.3. Functional Connectivity of the Primary Motor Cortex
3.4. Functional Connectivity of the Supplementary Motor Area
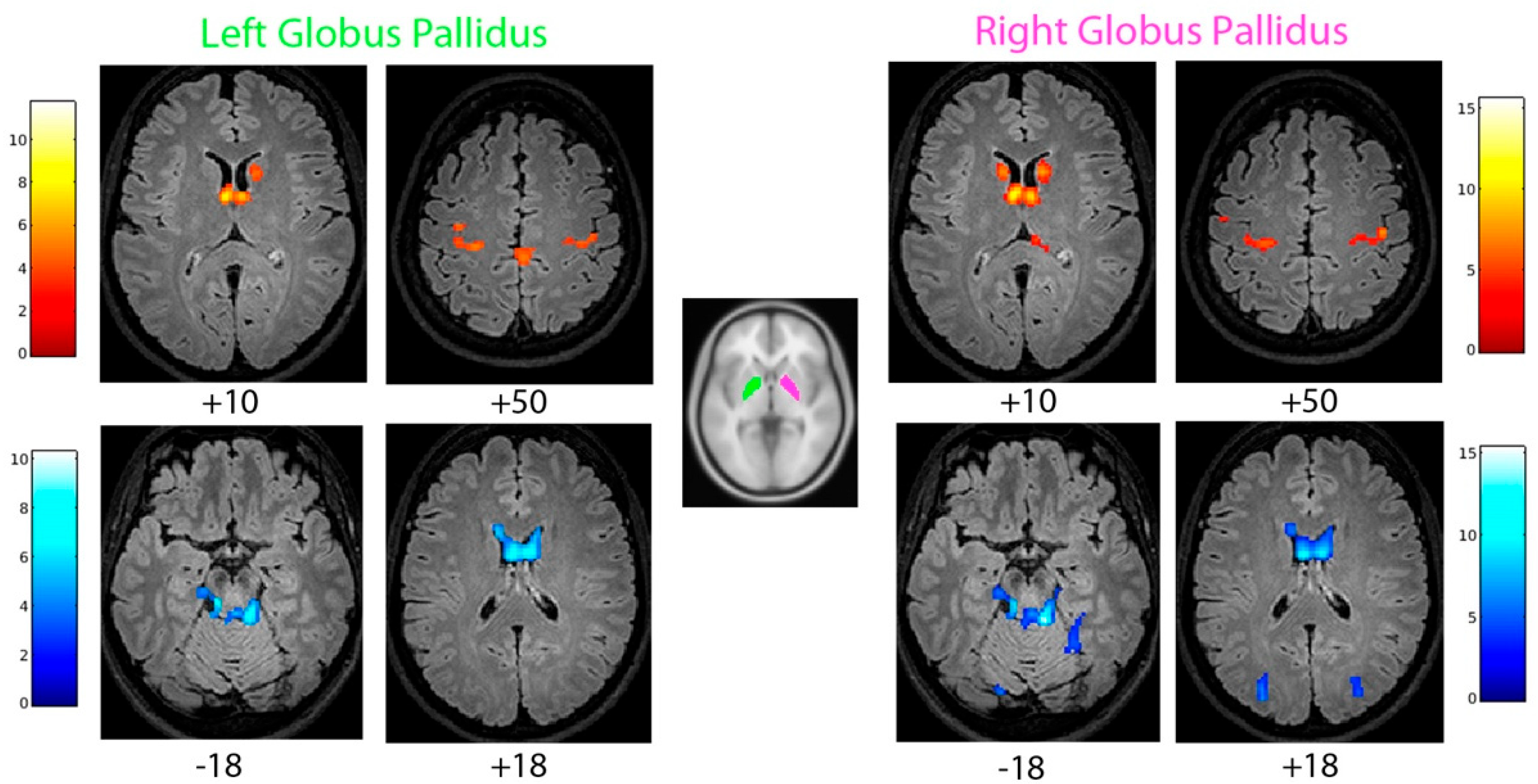
3.5. Functional Connectivity of the Globus Pallidus
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dusek, P.; Litwin, T.; Członkowska, A. Neurologic impairment in Wilson disease. Ann. Transl. Med. 2019, 7 (Suppl. 2), S64. [Google Scholar] [CrossRef] [PubMed]
- Salari, M.; Fayyazi, E.; Mirmosayyeb, O. Magnetic resonance imaging findings in diagnosis and prognosis of Wilson disease. J. Res. Med. Sci. 2018, 23, 23. [Google Scholar] [PubMed]
- Dusek, P.; Bahn, E.; Litwin, T.; Jabłonka-Salach, K.; Łuciuk, A.; Huelnhagen, T.; Madai, V.I.; Dieringer, M.A.; Bulska, E.; Knauth, M.; et al. Brain iron accumulation in Wilson disease: A postmortem 7 Tesla MRI—Histopathological study. Neuropathol. Appl. Neurobiol. 2017, 43, 514–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prashanth, L.K.; Sinha, S.; Taly, A.B.; Mahadevan, A.; Vasudev, M.K.; Shankar, S.K. Spectrum of epilepsy in Wilson’s disease with electroencephalographic, MR imaging and pathological correlates. J. Neurol. Sci. 2010, 291, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.E.; Yun, J.Y.; Yang, H.J.; Kim, H.J.; Jeon, B.S. Unusual epileptic deterioration and extensive white matter lesion during treatment in Wilson’s disease. BMC Neurol. 2013, 13, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, W. Coexistence of seizure with Wilson’s disease: A systematic review. Prog. Neurol. Psychiatry 2020, 24, 24–30. [Google Scholar] [CrossRef]
- Yacubian, E.M. Juvenile myoclonic epilepsy: Challenges on its 60th anniversary. Seizure 2017, 44, 48–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, X.; Chaitanya, G.; Asma, B.; Caciagli, L.; Bassett, D.S.; Tracy, J.I.; Sperling, M.R. Disrupted basal ganglia-thalamocortical loops in focal to bilateral tonic-clonic seizures. Brain 2020, 143, 175–190. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H. Grey and White Matter Alterations in Juvenile Myoclonic Epilepsy: A Comprehensive Review. J. Epilepsy Res. 2017, 7, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Vollmar, C.; O’Muircheartaigh, J.; Symms, M.R.; Barker, G.J.; Thompson, P.; Kumari, V.; Stretton, J.; Duncan, J.S.; Richardson, M.P.; Koepp, M.J. Altered microstructural connectivity in juvenile myoclonic epilepsy the missing link. Neurology 2012, 78, 1555–1559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Muircheartaigh, J.; Vollmar, C.; Barker, G.J.; Kumari, V.; Symms, M.R.; Thompson, P.; Duncan, J.S.; Koepp, M.J.; Richardson, M.P. Abnormal thalamocortical structural and functional connectivity in juvenile myoclonic epilepsy. Brain 2012, 135, 3635–3644. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, J.B.; Suh, S.I.; Kim, D.W. Subcortical grey matter changes in juvenile myoclonic epilepsy. NeuroImage Clin. 2018, 17, 397–404. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Regions of Interest (ROIs) | Increased Connectivity | Decreased Connectivity |
|---|---|---|
| Primary motor cortex (M1) | Left M1: with the pre- and post-central gyri bi-laterally, including right secondary somatosensory cortex. Right M1: with ipsilateral supramarginal gyrus and pre- and post-central gyri. | Left M1: with the left parahippocampal gyrus, cuneus and lingual gyrus. |
| Globus pallidus (GP) | Bilateral GP: with bilateral pre- and post-central gyri (medial portion), bilateral thalamus and the head of the caudate nucleus. | Bilateral GP: with the body of the caudate nucleus and cerebellum. Right GP: with bilateral occipital lobe and right parahippocampal gyrus. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, J.; Cavallieri, F.; Giovannini, G.; Benuzzi, F.; Ballotta, D.; Vaudano, A.E.; Ferrara, F.; Contardi, S.; Pietrangelo, A.; Corradini, E.; et al. Can Disruption of Basal Ganglia-Thalamocortical Circuit in Wilson Disease Be Associated with Juvenile Myoclonic Epilepsy Phenotype? Brain Sci. 2022, 12, 553. https://doi.org/10.3390/brainsci12050553
Rossi J, Cavallieri F, Giovannini G, Benuzzi F, Ballotta D, Vaudano AE, Ferrara F, Contardi S, Pietrangelo A, Corradini E, et al. Can Disruption of Basal Ganglia-Thalamocortical Circuit in Wilson Disease Be Associated with Juvenile Myoclonic Epilepsy Phenotype? Brain Sciences. 2022; 12(5):553. https://doi.org/10.3390/brainsci12050553
Chicago/Turabian StyleRossi, Jessica, Francesco Cavallieri, Giada Giovannini, Francesca Benuzzi, Daniela Ballotta, Anna Elisabetta Vaudano, Francesca Ferrara, Sara Contardi, Antonello Pietrangelo, Elena Corradini, and et al. 2022. "Can Disruption of Basal Ganglia-Thalamocortical Circuit in Wilson Disease Be Associated with Juvenile Myoclonic Epilepsy Phenotype?" Brain Sciences 12, no. 5: 553. https://doi.org/10.3390/brainsci12050553