
Propagation Structure of Intrinsic Brain Activity in Migraine without Aura


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Clinical Assessment
2.2. MRI Data Acquisition
2.3. Data Preprocessing
2.4. Resting-State Lag Analysis
2.5. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
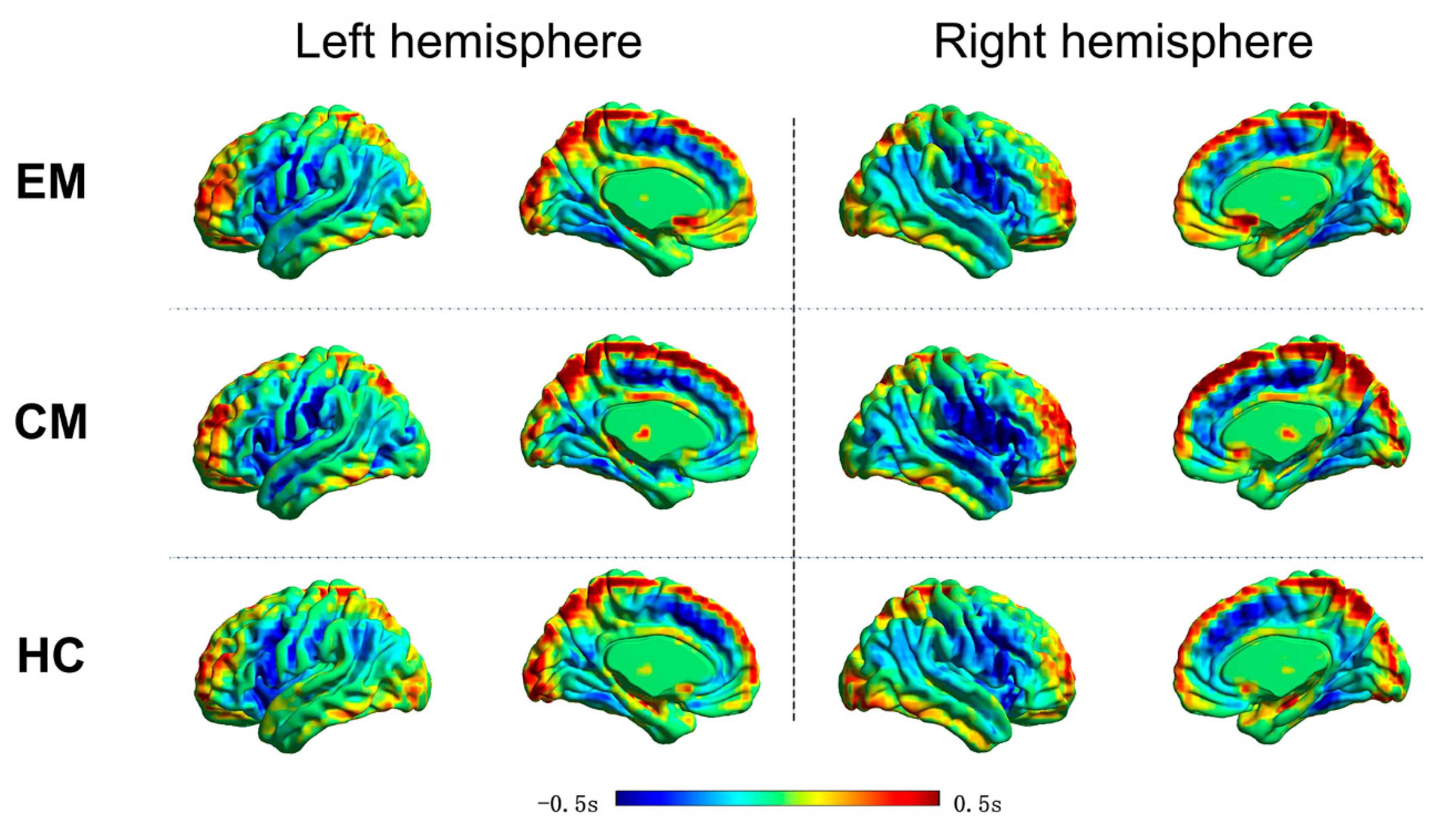
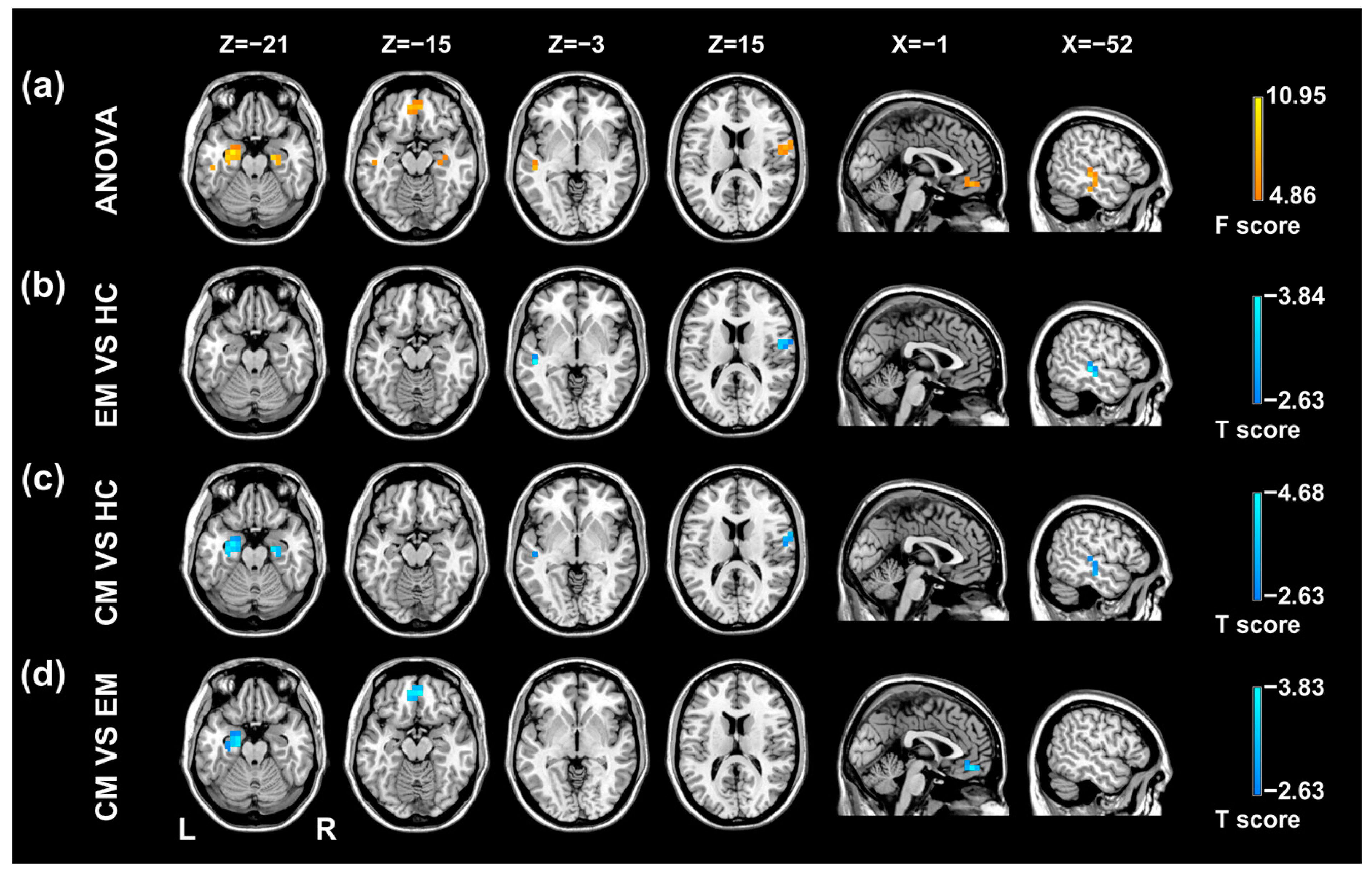
3.2. Resting-State Lag Analysis
3.3. Correlation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stovner, L.J.; Hagen, K.; Linde, M.; Steiner, T.J. The global prevalence of headache: An update, with analysis of the influences of methodological factors on prevalence estimates. J. Headache Pain 2022, 23, 34. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalagia 2018, 38, 1–211. [Google Scholar]
- Steiner, T.J.; Stovner, L.J.; Jensen, R.; Uluduz, D.; Katsarava, Z. Migraine remains second among the world’s causes of disability, and first among young women: Findings from GBD2019. J. Headache Pain 2020, 21, 137. [Google Scholar] [CrossRef] [PubMed]
- Brennan, K.; Pietrobon, D. A Systems Neuroscience Approach to Migraine. Neuron 2018, 97, 1004–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barkhof, F.; Haller, S.; Rombouts, S.A.R.B. Resting-State Functional MR Imaging: A New Window to the Brain. Radiology 2014, 272, 29–49. [Google Scholar] [CrossRef] [PubMed]
- Skorobogatykh, K.; Van Hoogstraten, W.S.; Degan, D.; Prischepa, A.; Savitskaya, A.; Ileen, B.M.; Bentivegna, E.; Skiba, I.; D’Acunto, L.; Ferri, L.; et al. Functional connectivity studies in migraine: What have we learned? J. Headache Pain 2019, 20, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwedt, T.J.; Chiang, C.-C.; Chong, C.D.; Dodick, D.W. Functional MRI of migraine. Lancet Neurol. 2015, 14, 81–91. [Google Scholar] [CrossRef]
- Lim, M.; Jassar, H.; Kim, D.J.; Nascimento, T.D.; DaSilva, A.F. Differential alteration of fMRI signal variability in the ascending tri-geminal somatosensory and pain modulatory pathways in migraine. J. Headache Pain 2021, 22, 4. [Google Scholar] [CrossRef]
- Li, Z.; Zhou, J.; Lan, L.; Cheng, S.; Sun, R.; Gong, Q.; Wintermark, M.; Zeng, F.; Liang, F. Concurrent brain structural and functional alterations in patients with migraine without aura: An fMRI study. J. Headache Pain 2020, 21, 141. [Google Scholar] [CrossRef]
- Ashina, S.; Bentivegna, E.; Martelletti, P.; Eikermann-Haerter, K. Structural and Functional Brain Changes in Migraine. Pain Ther. 2021, 10, 211–223. [Google Scholar] [CrossRef]
- Russo, A.; Silvestro, M.; Tedeschi, G.; Tessitore, A. Physiopathology of migraine: What have we learned from functional imaging? Curr. Neurol. Neurosci. Rep. 2017, 17, 95. [Google Scholar] [CrossRef] [PubMed]
- Ashina, M.; Terwindt, G.M.; Al-Karagholi, M.A.-M.; de Boer, I.; Lee, M.J.; Hay, D.L.; Schulte, L.H.; Hadjikhani, N.; Sinclair, A.J.; Ashina, H.; et al. Migraine: Disease characterisation, biomarkers, and precision medicine. Lancet 2021, 397, 1496–1504. [Google Scholar] [CrossRef]
- Sato, T.K.; Nauhaus, I.; Carandini, M. Traveling Waves in Visual Cortex. Neuron 2012, 75, 218–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majeed, W.; Magnuson, M.; Hasenkamp, W.; Schwarb, H.; Schumacher, E.H.; Barsalou, L.; Keilholz, S.D. Spatiotemporal dynamics of low frequency BOLD fluctuations in rats and humans. NeuroImage 2011, 54, 1140–1150. [Google Scholar] [CrossRef] [Green Version]
- Garg, R.; Cecchi, G.A.; Rao, A.R. Full-brain auto-regressive modeling (FARM) using fMRI. NeuroImage 2011, 58, 416–441. [Google Scholar] [CrossRef]
- Mitra, A.; Snyder, A.Z.; Hacker, C.D.; Raichle, M.E. Lag structure in resting-state fMRI. J. Neurophysiol. 2014, 111, 2374–2391. [Google Scholar] [CrossRef]
- Mitra, A.; Snyder, A.Z.; Constantino, J.N.; Raichle, M.E. The Lag Structure of Intrinsic Activity is Focally Altered in High Functioning Adults with Autism. Cereb. Cortex 2015, 27, 1083–1093. [Google Scholar] [CrossRef]
- Xu, Q.; Zhang, Z.; Liao, W.; Xiang, L.; Yang, F.; Wang, Z.; Chen, G.; Tan, Q.; Jiao, Q.; Lu, G. Time-Shift Homotopic Connectivity in Mesial Temporal Lobe Epilepsy. Am. J. Neuroradiol. 2014, 35, 1746–1752. [Google Scholar] [CrossRef] [Green Version]
- Weng, Y.; Qi, R.; Chen, F.; Ke, J.; Xu, Q.; Zhong, Y.; Chen, L.; Li, J.; Zhang, Z.; Zhang, L.; et al. The Temporal Propagation of Intrinsic Brain Activity Associate with the Occurrence of PTSD. Front. Psychiatry 2018, 9, 218. [Google Scholar] [CrossRef]
- Yuan, K.; Zhao, L.; Cheng, P.; Yu, D.; Zhao, L.; Dong, T.; Xing, L.; Bi, Y.; Yang, X.; von Deneen, K.M.; et al. Altered Structure and Resting-State Functional Connectivity of the Basal Ganglia in Migraine Patients Without Aura. J. Pain 2013, 14, 836–844. [Google Scholar] [CrossRef]
- Smyser, C.D.; Inder, T.E.; Shimony, J.S.; Hill, J.E.; Degnan, A.; Snyder, A.Z.; Neil, J.J. Longitudinal Analysis of Neural Network Development in Preterm Infants. Cereb. Cortex 2010, 20, 2852–2862. [Google Scholar] [PubMed] [Green Version]
- Power, J.D.; Barnes, K.A.; Snyder, A.Z.; Schlaggar, B.L.; Petersen, S.E. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. NeuroImage 2012, 59, 2142–2154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, X.J.; Castañón, A.N.; Ongür, D.; Whitfield-Gabrieli, S. Anticorrelations in resting state networks without global signal regres-sion. Neuroimage 2012, 59, 1420–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giove, F.; Gili, T.; Iacovella, V.; Macaluso, E.; Maraviglia, B. Images-based suppression of unwanted global signals in resting-state functional connectivity studies. Magn. Reson. Imaging 2009, 27, 1058–1064. [Google Scholar]
- Schneider, G.; Havenith, M.N.; Nikolic, D. Spatiotemporal Structure in Large Neuronal Networks Detected from Cross-Correlation. Neural Comput. 2006, 18, 2387–2413. [Google Scholar]
- Nikolić, D. Non-parametric detection of temporal order across pairwise measurements of time delays. J. Comput. Neurosci. 2007, 22, 5–19. [Google Scholar]
- Sheroziya, M.; Timofeev, I. Global intracellular slow-wave dynamics of the thalamocortical system. J. Neurosci. 2014, 34, 8875–8893. [Google Scholar]
- Cossart, R.; Aronov, D.; Yuste, R. Attractor dynamics of network UP states in the neocortex. Nature 2003, 423, 283–288. [Google Scholar]
- Zhu, Y.; Dai, L.; Zhao, H.; Ji, B.; Yu, Y.; Dai, H.; Hu, C.; Wang, X.; Ke, J. Alterations in Effective Connectivity of the Hippocampus in Migraine without Aura. J. Pain Res. 2021, 14, 3333–3343. [Google Scholar]
- Wang, T.; Chen, N.; Zhan, W.; Liu, J.; Zhang, J.; Liu, Q.; Huang, H.; He, L.; Zhang, J.; Gong, Q. Altered effective connectivity of posterior thalamus in migraine with cutaneous allodynia: A resting-state fMRI study with granger causality analysis. J. Headache Pain 2016, 17, 1–11. [Google Scholar]
- Wang, T.; Zhan, W.; Chen, Q.; Chen, N.; Zhang, J.; Liu, Q.; He, L.; Zhang, J.; Huang, H.; Gong, Q. Altered resting-state ascending/descending pathways associated with the posterior thalamus in migraine without aura. NeuroReport 2016, 27, 257–263. [Google Scholar] [PubMed] [Green Version]
- McEwen, B.S. Plasticity of the Hippocampus: Adaptation to Chronic Stress and Allostatic Load. Ann. N. Y. Acad. Sci. 2006, 933, 265–277. [Google Scholar]
- Liu, M.-G.; Chen, J. Roles of the hippocampal formation in pain information processing. Neurosci. Bull. 2009, 25, 237–266. [Google Scholar] [PubMed] [Green Version]
- Borsook, D.; Maleki, N.; Becerra, L.; McEwen, B. Understanding Migraine through the Lens of Maladaptive Stress Responses: A Model Disease of Allostatic Load. Neuron 2012, 73, 219–234. [Google Scholar] [CrossRef] [Green Version]
- Wiech, K.; Ploner, M.; Tracey, I. Neurocognitive aspects of pain perception. Trends Cogn. Sci. 2008, 12, 306–313. [Google Scholar]
- Yu, Y.; Zhao, H.; Dai, L.; Su, Y.; Wang, X.; Chen, C.; Shang, Y.; Ke, J.; Hu, C. Headache frequency associates with brain microstructure changes in patients with migraine without aura. Brain Imaging Behav. 2020, 15, 60–67. [Google Scholar]
- Coppola, G.; Di Renzo, A.; Petolicchio, B.; Tinelli, E.; Di Lorenzo, C.; Serrao, M.; Calistri, V.; Tardioli, S.; Cartocci, G.; Parisi, V.; et al. Increased neural connectivity between the hypothalamus and cortical resting-state functional networks in chronic migraine. J. Neurol. 2019, 267, 185–191. [Google Scholar]
- Li, Z.; Liu, M.; Lan, L.; Zeng, F.; Makris, N.; Liang, Y.; Guo, T.; Wu, F.; Gao, Y.; Dong, M.; et al. Altered periaqueductal gray resting state functional connectivity in mi-graine and the modulation effect of treatment. Sci. Rep. 2016, 6, 20298. [Google Scholar]
- Buckner, R.L.; Andrews-Hanna, J.R.; Schacter, D.L. The brain’s default network: Anatomy, function, and relevance to disease. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38. [Google Scholar]
- Soheili-Nezhad, S.; Sedghi, A.; Schweser, F.; Babaki, A.E.S.; Jahanshad, N.; Thompson, P.M.; Beckmann, C.F.; Sprooten, E.; Toghae, M. Structural and Functional Reorganization of the Brain in Migraine Without Aura. Front. Neurol. 2019, 10, 442. [Google Scholar]
- Deshpande, G.; Santhanam, P.; Hu, X. Instantaneous and causal connectivity in resting state brain networks derived from func-tional MRI data. Neuroimage 2011, 54, 1043–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burstein, R.; Noseda, R.; Borsook, D. Migraine: Multiple Processes, Complex Pathophysiology. J. Neurosci. 2015, 35, 6619–6629. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, M.S. See me, hear me, touch me: Multisensory integration in lateral occipital-temporal cortex. Curr. Opin. Neurobiol. 2005, 15, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Bigler, E.D.; Mortensen, S.; Neeley, E.S.; Ozonoff, S.; Krasny, L.; Johnson, M.; Lu, J.; Provencal, S.L.; McMahon, W.; Lainhart, J.E. Superior temporal gyrus, language function, and autism. Dev. Neuropsychol. 2007, 31, 217–238. [Google Scholar] [CrossRef]
- Yi, H.G.; Leonard, M.K.; Chang, E.F. The Encoding of Speech Sounds in the Superior Temporal Gyrus. Neuron 2019, 102, 1096–1110. [Google Scholar] [CrossRef]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable Intrinsic Connectivity Networks for Salience Processing and Executive Control. J. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef]
- Huang, X.; Zhang, D.; Wang, P.; Mao, C.; Miao, Z.; Liu, C.; Xu, C.; Yin, X.; Wu, X. Altered amygdala effective connectivity in migraine without aura: Evidence from resting-state fMRI with Granger causality analysis. J. Headache Pain 2021, 22, 25. [Google Scholar] [CrossRef]
- Wei, H.-L.; Chen, J.; Chen, Y.-C.; Yu, Y.-S.; Guo, X.; Zhou, G.-P.; Zhou, Q.-Q.; He, Z.-Z.; Yang, L.; Yin, X.; et al. Impaired effective functional connectivity of the sensorimotor network in interictal episodic migraineurs without aura. J. Headache Pain 2020, 21, 111. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Male/Female | Age (Year) | Education (Year) | Days with Headache a | VAS b | |
|---|---|---|---|---|---|
| EM (n = 39) | 9/30 | 39.74 (11.59) | 10.33 (4.02) | 3.75 (2.64) | 6.22 (1.77) |
| CM (n = 17) | 9/8 | 49.59 (14.64) | 9.71 (3.94) | 19.56 (4.17) | 7.24 (1.89) |
| HC (n = 35) | 15/20 | 34.91 (10.89) | 11.80 (4.92) | ||
| p value | 0.060 c | <0.001 d | 0.195 d | <0.001 e | 0.635 e |
| Brain Region | Hemi | Voxel | MNI Coordinate (x, y, z) | Temporal Lag Value | Peak F Score | ||
|---|---|---|---|---|---|---|---|
| CM | EM | HC | |||||
| STG/MTG | L | 47 | −48, −27, −3 | −0.105 | −0.118 | 0.129 | 7.59 |
| PoCG/PreCG | R | 64 | 60, −3, 15 | −0.537 | −0.387 | −0.199 | 7.12 |
| HP/PHG | R | 47 | 24, −15, −21 | −0.262 | −0.050 | 0.135 | 8.96 |
| HP/PHG | L | 92 | −24, −9, −21 | −0.316 | 0.035 | 0.128 | 10.95 |
| mPFC | L/R | 80 | −6, 45, −15 | −0.172 | 0.152 | −0.007 | 8.22 |
| Brain Region | Hemi | Voxel | MNI Coordinate (x, y, z) | Peak T Score |
|---|---|---|---|---|
| EM VS. HC | ||||
| STG/MTG | L | 32 | −48, −27, −3 | −3.84 |
| PoCG/PreCG | R | 48 | 51, −9, 15 | −3.41 |
| CM VS. HC | ||||
| STG/MTG | L | 40 | −48, −21, −15 | −3.37 |
| PoCG/PreCG | R | 48 | 66, 3, 15 | −3.57 |
| HP/PHG | L | 92 | −24, −9, −21 | −4.68 |
| HP/PHG | R | 47 | 24, −15, −21 | −4.23 |
| CM VS. EM | ||||
| HP/PHG | L | 62 | −18, −9, −21 | −3.66 |
| mPFC | L/R | 80 | 6, 45, −15 | −3.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dai, L.; Xu, Q.; Xiong, X.; Yu, Y.; Wang, X.; Dai, H.; Zhao, H.; Ke, J. Propagation Structure of Intrinsic Brain Activity in Migraine without Aura. Brain Sci. 2022, 12, 903. https://doi.org/10.3390/brainsci12070903
Dai L, Xu Q, Xiong X, Yu Y, Wang X, Dai H, Zhao H, Ke J. Propagation Structure of Intrinsic Brain Activity in Migraine without Aura. Brain Sciences. 2022; 12(7):903. https://doi.org/10.3390/brainsci12070903
Chicago/Turabian StyleDai, Lingling, Qiang Xu, Xing Xiong, Yang Yu, Ximing Wang, Hui Dai, Hongru Zhao, and Jun Ke. 2022. "Propagation Structure of Intrinsic Brain Activity in Migraine without Aura" Brain Sciences 12, no. 7: 903. https://doi.org/10.3390/brainsci12070903