
Robotic Verticalization plus Music Therapy in Chronic Disorders of Consciousness: Promising Results from a Pilot Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures
2.2. Outcome Measures
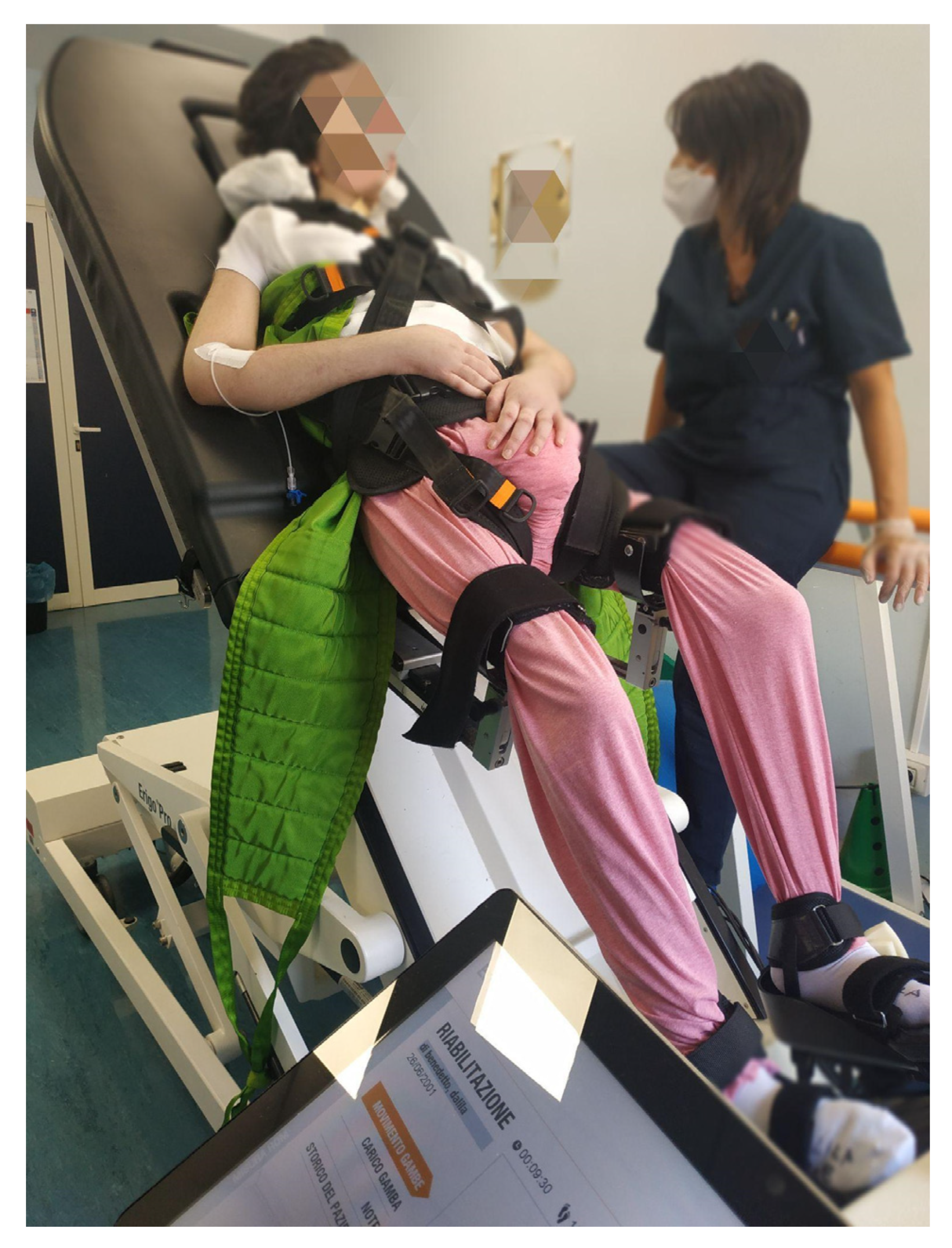
2.3. Robotic Verticalization Training (RVT)
2.4. Music Robotic Verticalization (MRV)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giacino, J.T.; Fins, J.J.; Laureys, S.; Schiff, N.D. Disorders of consciousness after acquired brain injury: The state of the science. Nat. Rev. Neurol. 2014, 10, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.; et al. Comprehensive Systematic Review Update Summary: Disorders of Consciousness. Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Arch. Phys. Med. Rehabil. 2018, 99, 1710–1719. [Google Scholar] [CrossRef] [PubMed]
- van Erp, W.S.; Lavrijsen, J.C.M.; Vos, P.E.; Laureys, S.; Koopmans, R. Unresponsive wakefulness syndrome: Outcomes from a vicious circle. Ann. Neurol. 2020, 87, 12–18. [Google Scholar] [CrossRef]
- Taveggia, G.; Ragusa, I.; Trani, V.; Cuva, D.; Angeretti, C.; Fontanella, M.; Panciani, P.P.; Borboni, A. Robotic tilt table reduces the occurrence of orthostatic hypotension over time in vegetative states. International journal of rehabilitation research. Int. J. Rehabil. Res. 2015, 38, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Krewer, C.; Luther, M.; Koenig, E.; Müller, F. Tilt Table Therapies for Patients with Severe Disorders of Consciousness: A Randomized, Controlled Trial. PLoS ONE 2015, 10, e0143180. [Google Scholar] [CrossRef]
- Godoy, D.A.; Seifi, A.; Chi, G.; Paredes Saravia, L.; Rabinstein, A.A. Intracranial Pressure Monitoring in Moderate Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Neurocritical Care 2022. [Google Scholar] [CrossRef]
- Frazzitta, G.; Zivi, I.; Valsecchi, R.; Bonini, S.; Maffia, S.; Molatore, K.; Sebastianelli, L.; Zarucchi, A.; Matteri, D.; Ercoli, G.; et al. Effectiveness of a Very Early Stepping Verticalization Protocol in Severe Acquired Brain Injured Patients: A Randomized Pilot Study in ICU. PLoS ONE 2016, 11, e0158030. [Google Scholar] [CrossRef]
- Riberholt, C.G.; Olsen, M.H.; Berg, R.M.; Mehlsen, J.; Møller, K. Dynamic cerebral autoregulation during early orthostatic exercise in patients with severe traumatic brain injury: Further exploratory analyses from a randomized clinical feasibility trial. J. Clin. Neurosci. 2021, 92, 39–44. [Google Scholar] [CrossRef]
- Grimm, T.; Kreutz, G. Music interventions in disorders of consciousness (DOC)—A systematic review. Brain Inj. 2018, 32, 704–714. [Google Scholar] [CrossRef]
- Leonardi, S.; Cacciola, A.; De Luca, R.; Aragona, B.; Andronaco, V.; Milardi, D.; Bramanti, P.; Calabrò, R.S. The role of music therapy in rehabilitation: Improving aphasia and beyond. Int. J. Neurosci. 2018, 128, 90–99. [Google Scholar] [CrossRef]
- Bodart, O.; Gosseries, O.; Laureys, S. Coma and disorders of consciousness: Scientific advances and practical considerations for clinicians. Skull Base 2013, 33, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Porcaro, C.; Nemirovsky, I.E.; Riganello, F.; Mansour, Z.; Cerasa, A.; Tonin, P.; Stojanoski, B.; Soddu, A. Diagnostic Developments in Differentiating Unresponsive Wakefulness Syndrome and the Minimally Conscious State. Front. Neurol. 2022, 12, 778951. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Kalmar, K.; Whyte, J. The JFK Coma Recovery Scale-Revised: Measurement characteristics and diagnostic utility. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef] [PubMed]
- Rossato, E.; Verzini, E.; Scandola, M.; Ferrari, F.; Bonadiman, S. Role of LCF scale as an outcome prognostic index in patients with traumatic brain injury. Neurol. Sci. 2021, 42, 2747–2752. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Collin, C.; Wade, D. Assessing motor impairment after stroke: A pilot reliability study. J. Neurol. Neurosurg. Psychiatry 1990, 53, 576–579. [Google Scholar] [CrossRef]
- Jeanne Wilcox, M.; Davis, A.; PACE. Promoting Aphasic’s Communicative Effectiveness; Department of Audiology and Speech Pathology, Memphis State University: Memphis, TN, USA, 1979. [Google Scholar]
- Ancona, E.; Quarenghi, A.; Simonini, M.; Saggini, R.; Mazzoleni, S.; De Tanti, A.; Saviola, D.; Salvi, G.P. Effect of verticalization with Erigo® in the acute rehabilitation of severe acquired brain injury. Neurol. Sci. 2019, 40, 2073–2080. [Google Scholar] [CrossRef]
- Rocca, A.; Pignat, J.-M.; Berney, L.; Jöhr, J.; Van De Ville, D.; Daniel, R.T.; Levivier, M.; Hirt, L.; Luft, A.R.; Grouzmann, E.; et al. Sympathetic activity and early mobilization in patients in intensive and intermediate care with severe brain injuries: A preliminary prospective randomized study. BMC Neurol. 2016, 16, 169. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 1 April 2022).
- Vinolo-Gil, M.J.; Casado-Fernández, E.; Perez-Cabezas, V.; Gonzalez-Medina, G.; Martín-Vega, F.J.; Martín-Valero, R. Effects of the Combination of Music Therapy and Physiotherapy in the Improvement of Motor Function in Cerebral Palsy: A Challenge for Research. Children 2021, 8, 868. [Google Scholar] [CrossRef]
- Baur, K.; Speth, F.; Nagle, A.; Riener, R.; Klamroth-Marganska, V. Music meets robotics: A prospective randomized study on motivation during robot aided therapy. J. Neuroeng. Rehabil. 2018, 15, 79. [Google Scholar] [CrossRef]
- Verger, J.; Ruiz, S.; Tillmann, B.; Romdhane, M.B.; De Quelen, M.; Castro, M.; Tell, L.; Luauté, J.; Perrin, F. Effets bénéfiques de la musique préférée sur les capacités cognitives des patients en état de conscience minimale. Rev. Neurol. 2014, 170, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.; Tillmann, B.; Luauté, J.; Corneyllie, A.; Dailler, F.; André-Obadia, N.; Perrin, F. Boosting cognition with music in patients with disorders of consciousness. Neurorehabilit. Neural Repair 2015, 29, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Sorbera, C.; Portaro, S.; Cimino, V.; Leo, A.; Accorinti, M.; Silvestri, G.; Bramanti, P.; Naro, A.; Calabrò, R.S. ERIGO: A possible strategy to treat orthostatic hypotension in progressive supranuclear palsy? A feasibility study. Funct. Neurol. 2019, 34, 93–97. [Google Scholar] [PubMed]
- Calabrò, R.S.; Naro, A.; Russo, M.; Leo, A.; Balletta, T.; Saccá, I.; De Luca, R.; Bramanti, P. Do post-stroke patients benefit from robotic verticalization? A pilot-study focusing on a novel neurophysiological approach. Restor. Neurol. Neurosci. 2015, 33, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, C.; Hu, N.; Wang, T. Music Interventions for Disorders of Consciousness: A Systematic Review and Meta-analysis. J. Neurosci. Nurs. 2020, 52, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Gomez, P.; Danuser, B. Affective and physiological responses to environmental noises and music. Int. J. Psychophysiol. 2004, 53, 91–103. [Google Scholar] [CrossRef]
- Perrin, F.; Castro, M.; Tillmann, B.; Luauté, J. Promoting the use of personally relevant stimuli for investigating patients with disorders of consciousness. Front. Psychol. 2015, 6, 1102. [Google Scholar] [CrossRef]
- Hu, Y.; Yu, F.; Wang, C.; Yan, X.; Wang, K. Can Music Influence Patients With Disorders of Consciousness? An Event-Related Potential Study. Front. Neurosci. 2021, 15, 596636. [Google Scholar] [CrossRef]
- Martínez-Molina, N.; Siponkoski, S.; Särkämö, T. Cognitive efficacy and neural mechanisms of music-based neurological rehabilitation for traumatic brain injury. Ann. N. Y. Acad. Sci. 2022. [Google Scholar] [CrossRef]
- O’Kelly, J.; James, L.; Palaniappan, R.; Taborin, J.; Fachner, J.; Magee, W.L. Neurophysiological and behavioral responses to music therapy in vegetative and minimally conscious States. Front. Hum. Neurosci. 2013, 7, 884. [Google Scholar] [CrossRef] [PubMed]
- Schnakers, C.; Magee, W.L.; Harris, B. Sensory Stimulation and Music Therapy Programs for Treating Disorders of Consciousness. Front. Psychol. 2016, 7, 297. [Google Scholar] [CrossRef] [PubMed]
- Carrière, M.; Larroque, S.K.; Martial, C.; Bahri, M.A.; Aubinet, C.; Perrin, F.; Laureys, S.; Heine, L. An Echo of Consciousness: Brain Function during Preferred Music. Brain Connect. 2020, 10, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Olszewska, A.M.; Gaca, M.; Herman, A.M.; Jednoróg, K.; Marchewka, A. How Musical Training Shapes the Adult Brain: Predispositions and Neuroplasticity. Front. Neurosci. 2021, 15, 630829. [Google Scholar] [CrossRef]
- Amico, E.; Marinazzo, D.; Di Perri, C.; Heine, L.; Annen, J.; Martial, C.; Dzemidzic, M.; Kirsch, M.; Bonhomme, V.; Laureys, S.; et al. Mapping the functional connectome traits of levels of consciousness. NeuroImage 2017, 148, 201–211. [Google Scholar] [CrossRef]


{kind=link}
| Control Group (CG) | All | Males | MCS Level | Age | Females | MCS Level | Age |
| Patients | 8 | 6 (75.00) | 2 (15.00) | ||||
| CRS-R baseline | 8 ± 3.11 | 6 | - | 75 | 6 | - | 64 |
| 9 | + | 69 | 9 | + | 55 | ||
| 7 | - | 65 | |||||
| 15 | + | 54 | |||||
| 6 | - | 73 | |||||
| 6 | - | 73 | |||||
| Time elapsed since injury (months) | 9.12 ± 2.16 | 10 | 9 | ||||
| 6 | 12 | ||||||
| 7 | |||||||
| 8 | |||||||
| 12 | |||||||
| 9 | |||||||
| Age (years) | 66 (±8.08) | 69.83 (±4.57) | 54.5 (±0.70) | ||||
| Education Elementary school Middle school High school University | 2 (25) 5 (62.5) 1 (12.5) 0 (0.00) | 1 (16.66) 5 (83.34) 0 (0.00) 0 (0.00) | 1 (50.00) 0 (0.00) 1 (50.00) 0 (0.00) | ||||
| Experimental Group (EG) | All | Males | MCS Level | Age | Females | MCS | Age |
| Patients | 8 | 5 (62.5) | 3 (37.5) | ||||
| CRS-R baseline | 10.6 ± 2.32 | 12 | + | 57 | 10 | + | 73 |
| 8 | - | 35 | 10 | + | 45 | ||
| 12 | + | 62 | 10 | + | 65 | ||
| 8 | - | 58 | |||||
| 15 | + | 60 | |||||
| Time elapsed since injury | 9.25 ± 2.05 | 9 | 6 | ||||
| 9 | 12 | ||||||
| 8 | 8 | ||||||
| 12 | |||||||
| 10 | |||||||
| Age (years) | 56.87 (±11.84) | 54.4 (±11.01) | 61 (±14.42) | ||||
| Education | |||||||
| Elementary school | 2 (25.00) | 1 (20.00) | 1 (33.3) | ||||
| Middle school | 3 (37.5) | 2 (40.00) | 1 (33.3) | ||||
| High school | 2 (25.00) | 1 (20.00) | 1 (33.3) | ||||
| University | 1 (12.25) | 1 (20.00) | 0 (0.00) | ||||
| Test/Scale | Domains | Description |
|---|---|---|
| Levels of Cognitive Functioning (LCF) | Cognitive Functioning | Each level of LCF is presented as a behavioral description in 10 narrative forms, and the physician must decide which level best describes the patient’s present behaviors:
|
| Coma Recovery Scale -Revised (CRS-R) | Consciousness State | The Italian version of the Coma Recovery Scale-Revised (CRS-R), a reliable tool that can distinguish patients in the minimally conscious state from those in a vegetative state. The CRS-R consists of 29 hierarchically organized items divided into 6 subscales addressing auditory, visual, motor, oromotor, communication, and arousal processes. It is designed to detect subtle changes in neurobehavioral status and to predict outcomes in patients with severe alterations of consciousness. |
| Functional Communication Scale (FCS) | Communicative Functioning | The FCS is a specialist language questionnaire of verbal and nonverbal abilities for investigating global communication by evaluating language abilities (verbal and nonverbal communication skills). It is carried out by the speech therapist to investigate motivation, collaboration, understanding, and language abilities. Response options range from 0 to 22. |
| Functional Independence Measure (FIM) | Functional Status | The FIM is an ordinal scale composed of 18 items with 7 levels ranging from 1 (total dependence) to 7 (total independence) designed to determine the level of disability of patients, as reflected in their need for assistance and/or aids during the execution of activities of daily living. The FIM can be subdivided into a 13-item motor subscale (motFIM) and a 5-item cognitive subscale (cognFIM). The ranges of scoring for the motor and cognitive subscales are 13 to 91 and 5 to 35, respectively. gGood interrater reliability has been demonstrated both for the TCT and for the FIM. |
| Trunk Control Test (TCT) | Trunk Movement Patterns | The TCT examines four axial movements: rolling from a supine position to the weak side (T1) and to the strong side (T2), sitting up from a lying-down position (T3), and sitting in a balanced position on the edge of the bed with feet off the ground for 30 s (T4). The scoring is as follows: 0, unable to perform movement without assistance; 12, able to perform movement but in an abnormal manner; and 25, able to complete movement normally. The TCT score is the sum of the scores obtained on the four tests (range, 0 to 100). The examiner’s score must relate solely to the performance during the test and not be based on referred data. |
| Clinical and Psychometric Scales | Music Robotic Verticalization (Median, First-Third Quartile) | Robotic Verticalization (Median, First-Third Quartile) | p-Value |
|---|---|---|---|
| CRS-R | |||
| T0 | 10 (9.5–12) | 6.5 (6–9) | 0.03 |
| T1 | 14.5 (13.5–15.25) | 7.5(6–9.25) | 0.01 |
| LCF | |||
| T0 | 4.5 (3.75–5) | 1.5 (1–2.75) | 0.052 |
| T1 | 7 (6–7.25) | 2 (1.75–3.25) | 0.03 |
| FIM | |||
| T0 | 21.5 (18–24.5) | 18 (18–19) | 0.24 |
| T1 | 25 (21.75–46.25) | 18 (18–18.75) | 0.06 |
| TCT | |||
| T0 | 12 (0–18) | 0 (0–0) | 0.14 |
| T1 | 14.5 (0–30) | 0 (0–11.25) | 0.29 |
| FCS | |||
| T0 | 24 (20.75–26.5) | 17.5(16.75–23.25) | 0.14 |
| T1 | 30.5 (23.75–44.5) | 17.5 (16.5–21.25) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Luca, R.; Bonanno, M.; Vermiglio, G.; Trombetta, G.; Andidero, E.; Caminiti, A.; Pollicino, P.; Rifici, C.; Calabrò, R.S. Robotic Verticalization plus Music Therapy in Chronic Disorders of Consciousness: Promising Results from a Pilot Study. Brain Sci. 2022, 12, 1045. https://doi.org/10.3390/brainsci12081045
De Luca R, Bonanno M, Vermiglio G, Trombetta G, Andidero E, Caminiti A, Pollicino P, Rifici C, Calabrò RS. Robotic Verticalization plus Music Therapy in Chronic Disorders of Consciousness: Promising Results from a Pilot Study. Brain Sciences. 2022; 12(8):1045. https://doi.org/10.3390/brainsci12081045
Chicago/Turabian StyleDe Luca, Rosaria, Mirjam Bonanno, Giuliana Vermiglio, Giovanni Trombetta, Ersilia Andidero, Angelo Caminiti, Patrizia Pollicino, Carmela Rifici, and Rocco Salvatore Calabrò. 2022. "Robotic Verticalization plus Music Therapy in Chronic Disorders of Consciousness: Promising Results from a Pilot Study" Brain Sciences 12, no. 8: 1045. https://doi.org/10.3390/brainsci12081045
APA StyleDe Luca, R., Bonanno, M., Vermiglio, G., Trombetta, G., Andidero, E., Caminiti, A., Pollicino, P., Rifici, C., & Calabrò, R. S. (2022). Robotic Verticalization plus Music Therapy in Chronic Disorders of Consciousness: Promising Results from a Pilot Study. Brain Sciences, 12(8), 1045. https://doi.org/10.3390/brainsci12081045