
Language Development in Preschool Duchenne Muscular Dystrophy Boys




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessment
2.3. Statistical Analysis
3. Results
3.1. DMD Group
3.1.1. Language Assessment
3.1.2. Working Memory and Visual-Motor Integration Ability
3.1.3. Attention Skills
3.2. LSD Group
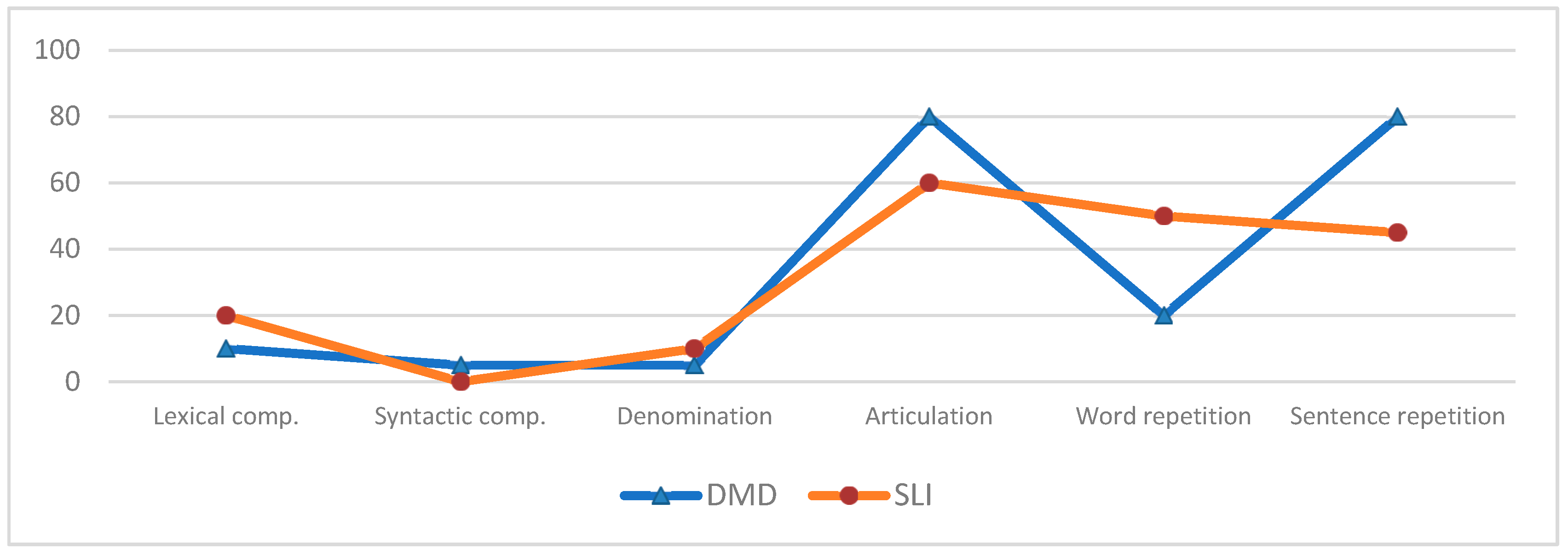
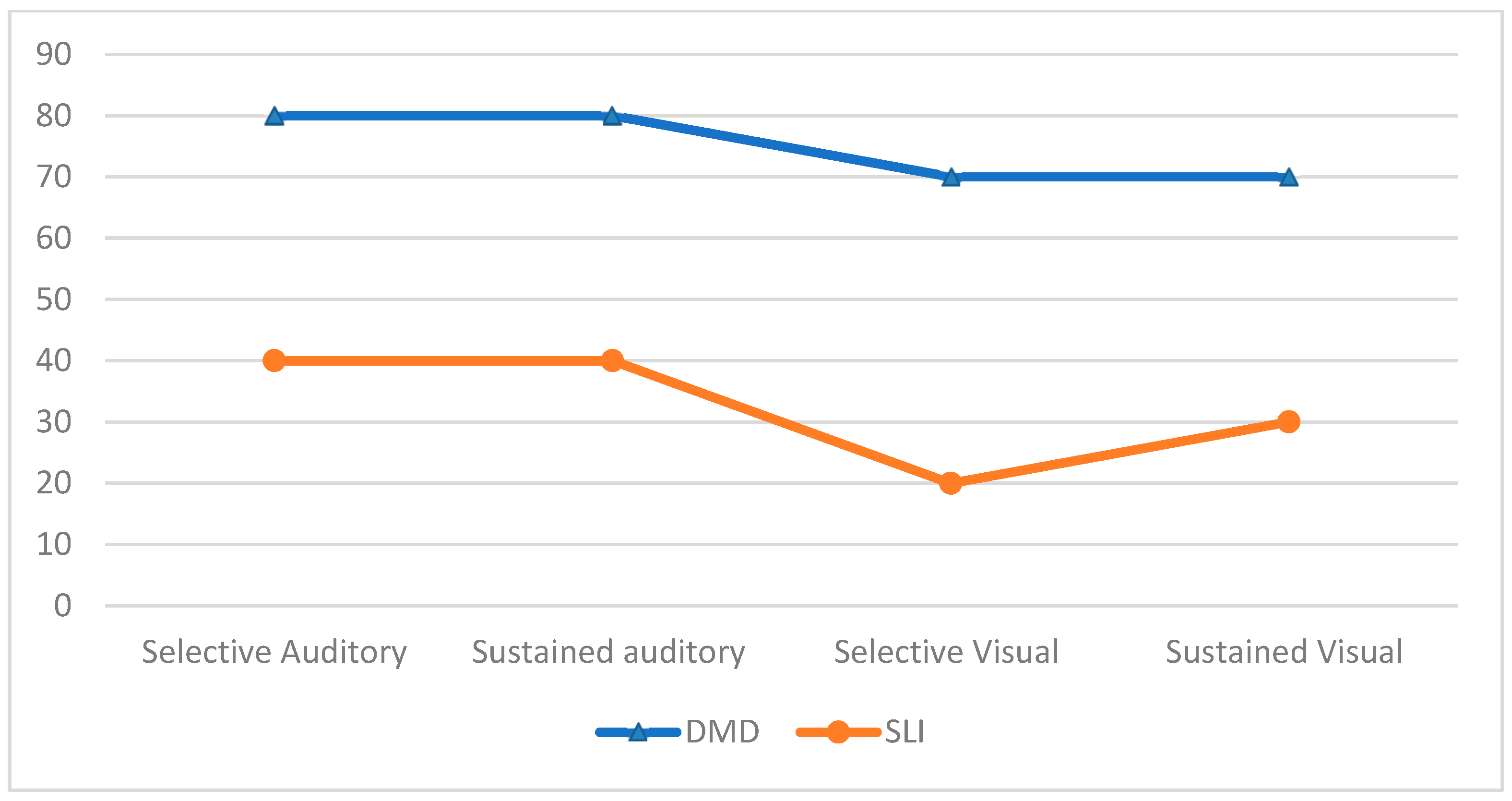
3.3. Comparison of the Tests Administered between the DMD Group and the SLI Group
3.4. Cognitive Tests and Brain Dystrophin Involvement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Battini, R.; Chieffo, D.; Bulgheroni, S.; Piccini, G.; Pecini, C.; Lucibello, S.; Lenzi, S.; Moriconi, F.; Pane, M.; Astrea, G.; et al. Cognitive profile in Duchenne muscular dystrophy boys without intellectual disability: The role of executive functions. Neuromuscul. Disord. 2018, 28, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Colombo, P.; Nobile, M.; Tesei, A.; Civati, F.; Gandossini, S.; Mani, E.; Molteni, M.; Bresolin, N.; D’Angelo, G. Assessing mental health in boys with Duchenne muscular dystrophy: Emotional, behavioural and neurodevelopmental profile in an Italian clinical sample. Eur. J. Paediatr. Neurol. 2017, 21, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Pane, M.; Lombardo, M.E.; Alfieri, P.; D’Amico, A.; Bianco, F.; Mercuri, E. Attention Deficit Hyperactivity Disorder and Cognitive Function in Duchenne Muscular Dystrophy: Phenotype-Genotype Correlation. J. Pediatrics 2012, 161, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Hinton, V.J.; Cyrulnik, S.E.; Fee, R.J.; Batchelder, A.; Kiefel, J.M.; Goldstein, E.M.; Kaufmann, P.; Darryl, C. Association of autistic spectrum disorders with dystrophinopathies. Pediatr. Neurol. 2009, 41, 339–346. [Google Scholar] [CrossRef]
- Chieffo, D.; Brogna, C.; Berardinelli, A.; D’Angelo, G. Early Neurodevelopmental Findings Predict School Age Cognitive Abilities in Duchenne Muscular Dystrophy: A Longitudinal Study. PLoS ONE 2015, 10, e0133214. [Google Scholar] [CrossRef]
- Connolly, A.M.; Florence, J.M.; Cradock, M.M.; Malkus, E.C.; Schierbecker, J.R.; Siener, C.A.; Wulf, C.O.; Anand, P.; Golumbek, P.T.; Zaidman, C.M.; et al. Motor and cognitive assessment of infants and young boys with Duchenne Muscular Dystrophy: Results from the Muscular Dystrophy Association DMD Clinical Research Network. Neuromuscul. Disord. 2013, 23, 529–539. [Google Scholar] [CrossRef]
- Lorusso, M.L.; Civati, F.; Molteni, M.; Turconi, A.C.; Bresolin, N.; D’Angelo, M.G. Specific profiles of neurocognitive and reading functions in a sample of 42 Italian boys with Duchenne Muscular Dystrophy. Child Neuropsychol. 2013, 19, 350–369. [Google Scholar] [CrossRef] [PubMed]
- Hinton, V.J.; Fee, R.J.; Goldstein, E.M.; De Vivo, D.C. Verbal and memory skills in males with Duchenne muscular dystrophy. Dev. Med. Child Neurol. 2007, 49, 123–128. [Google Scholar] [CrossRef]
- Donders, J.; Taneja, C. Neurobehavioral characteristics of children with Duchenne muscular dystrophy. Child Neuropsychol. 2009, 15, 295–304. [Google Scholar] [CrossRef]
- Snow, M.; Anderson, J.E.; Jaskobson, L.S. Neuropsychological and neurobehavioral functioning in Duchenne muscular dystrophy: A review. Neurosci. Biobehav. Rev. 2013, 37, 743–752. [Google Scholar] [CrossRef]
- Bushby, K.D.; Hill, A.; Steele, J.G. Failure of early diagnosis in symptomatic Duchenne muscular dystrophy. Lancet 1999, 353, 557–558. [Google Scholar] [CrossRef]
- D’Amico, A.; Catteruccia, M.; Baranello, G.; Politano, L.; Govoni, A.; Previtali, S.C.; Pane, M.; D’Angelo, M.G.; Bruno, C.; Messina, S.; et al. Diagnosis of Duchenne Muscular Dystrophy in Italy in the last decade: Critical issues and areas for improvements. Neuromuscul. Disord. 2017, 27, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Roper, C.E. Late diagnosis of Duchenne’s muscular dystrophy presenting as global developmental delay. Br. Med. J. 2001, 323, 37–38. [Google Scholar]
- Hinton, V.J.; Nereo, N.E.; Fee, R.J.; Cyrulnik, S.E. Social behavior problems in boys with Duchenne muscular dystrophy. J. Dev. Behav. Pediatr. 2006, 27, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Shana, E.; Cyrulnika, V.J. Duchenne muscular dystrophy: A cerebellar disorder? Neurosci. Biobehav. Rev. 2008, 32, 486–496. [Google Scholar]
- Pane, M.; Mazzone, E.S.; Sormani, M.P.; Messina, S.; Vita, G.L.; Fanelli, L.; Berardinelli, A.; Torrente, Y.; D’Amico, A.; Lanzillotta, V.; et al. 6 Minute walk test in Duchenne MD patients with different mutations: 12 month changes. PLoS ONE 2014, 9, e83400. [Google Scholar] [CrossRef]
- Pane, M.; Scalise, R.; Berardinelli, A.; D’Angelo, G.; Ricotti, V.; Mercuri, E. Early neurodevelopmental assessment in Duchenne muscular dystrophy. Neuromuscul. Disord. 2013, 23, 451–455. [Google Scholar] [CrossRef]
- Connolly, A.M.; Florence, J.M.; Cradock, M.M.; Eagle, M.; Flanigan, K.M.; McDonald, C.M.; Karachunski, P.I.; Darras, B.T.; Bushby, K.; Malkus, E.C.; et al. One year outcome of boys with Duchenne muscular dystrophy using the Bayley-III scales of infant and toddler development. Pediatr. Neurol. 2014, 50, 557–563. [Google Scholar] [CrossRef]
- Marini, A.; Marotta, L.; Bulgheroni, S.; Fabbro, F. Batteria per la Valutazione del Linguaggio in Bambini dai 4 ai 12 Anni, BVL_4–12; Giunti O.S.: Milano, Italy, 2015. [Google Scholar]
- Andrea, B.; Ernesto, S. Test delle campanelle modificato. Psichiatr. Dell’infanzia Dell’ Adolesc. 1997, 64, 73–84. [Google Scholar]
- Bertelli, B.; Bilancia, G. Batterie per la Valutazione dell’Attenzione Uditiva e della Memoria di Lavoro Fonologica nell’Età Evolutiva, VAUMeLF; Giunti O.S.: Milano, Italy, 2006. [Google Scholar]
- Cyrulnik, S.E.; Fee, R.J.; Batchelder, A.; Kiefel, J.; Goldstein, E.; Hinton, V.J. Cognitive and adaptive deficits in young children with Duchenne muscular dystrophy (DMD). J. Int. Neuropsychol. Soc. 2008, 14, 853–861. [Google Scholar] [CrossRef]
- Hinton, V.J.; De Vivo, D.C.; Nereo, N.E.; Goldstein, E.; Stern, Y. Selective deficits in verbal working memory associated with a known genetic etiology: The neuropsychological profile of Duchenne muscular dystrophy. J. Int. Neuropsychol. Soc. 2001, 7, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Marini, A.; Lorusso, M.L.; D’Angelo, M.G.; Civati, F.; Turconi, A.C.; Fabbro, F.; Bresolin, N. Evaluation of narrative abilities in patients suffering from Duchenne Muscular Dystrophy. Brain Lang. 2007, 102, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Billard, C.; Gillet, P.; Barthez, M.; Hommet, C.; Bertrand, P. Reading ability and processing in Duchenne muscular dystrophy and spinal muscular atrophy. Dev. Med. Child Neurol. 1998, 40, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Fabbro, F.; Marini, A.; Felisari, G.; Comi, G.P.; D’Angelo, M.G.; Turconi, A.C.; Bresolin, N. Language disturbances in a group of participants suffering from Duchenne muscular dystrophy: A pilot study. Percept. Mot. Ski. 2007, 104, 663–676. [Google Scholar] [CrossRef] [PubMed]
- Hinton, V.J.; De Vivo, D.C.; Nereo, N.E.; Goldstein, E.; Stern, Y. Poor verbal working memory across intellectual level in boys with Duchenne dystrophy. Neurology 2000, 54, 2127–2132. [Google Scholar] [CrossRef] [PubMed]
- Papagno, C.; Comi, A.; Riva, M.; Bizzi, A.; Vernice, M.; Casarotti, A.; Bello, L. Mapping the brain network of the phonological loop. Hum. Brain Mapp. 2017, 38, 3011–3024. [Google Scholar] [CrossRef]
- Hickok, G. The cortical organization of speech processing: Feedback control and predictive coding the context of a dual-stream model. J. Commun. Disord. 2012, 45, 393–402. [Google Scholar] [CrossRef]
- Fridriksson, J.; Yourganov, G.; Bonilha, L.; Basilakos, A.; Den Ouden, D.B.; Rorden, C. Revealing the dual streams of speech processing. Proc. Natl. Acad. Sci. USA 2016, 113, 15108–15113. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Test | SLI (n = 20) N (%) | DMD (n = 20) N (%) | Mann–Whitney U Results | Chi-Squared/FET Results |
|---|---|---|---|---|
| Lexical comprehension | U = 175.000, z = −0.695, p = 0.512 | p = 0.661, FET | ||
| NP | 16 (80) | 18 (90) | ||
| P | 4 (20) | 2 (10) | ||
| Syntactic comprehension | U = 206.000, z = 0.176, p = 0.883 | |||
| NP | 20 (100) | 20 (100) | ||
| P | 0 (0) | 0 (0) | ||
| Denomination | ||||
| NP | 20 (100) | 20 (100) | U = 174.500, z = −0.714, p = 0.495 | |
| P | 0 (0) | 0 (0) | ||
| Articulation | U = 209.500, z = 0.268, p = 0.799 | p = 1.000, FET | ||
| NP | 4 (20) | 4 (20) | ||
| P | 16 (80) | 16 (80) | ||
| Word repetition | U = 112.500, z = –2.392, p = 0.017 * | X2 (1, N = 40) = 3.956, p = 0.047 * | ||
| NP | 10 (50) | 16 (80) | ||
| P | 10 (50) | 4 (20) | ||
| Nonword repetition | U = 312.000, z = 3.099, p = 0.002 * | p= 0.003 *, FET | ||
| NP | 20 (100) | 12 (60) | ||
| P | 0 (0) | 8 (40) | ||
| Sentence repetition | U = 272.000, z = 1.982, p = 0.052 | X2 (1, N = 40) = 5.227, p = 0.022 * | ||
| NP | 11 (55) | 4 (20) | ||
| P | 9 (45) | 16 (80) | ||
| Visual attention rapidity | U = 320.500, z = 3.262, p = 0.001 * | X2 (1, N = 40) = 10.101, p = 0.001 * | ||
| NP | 16 (80) | 6 (30) | ||
| P | 4 (20) | 14 (70) | ||
| Visual attention accuracy | U = 258.500, z = 1.584, p = 0.114 | X2 (1, N = 40) = 6.400, p = 0.011 * | ||
| NP | 14 (70) | 6 (30) | ||
| P | 6 (30) | 14 (70) | ||
| Auditory attention (ACPT1) | U = 263.500, z = 1.729, p = 0.086 | X2 (1, N = 40) = 6.667, p = 0.010 * | ||
| NP | 12 (60) | 4 (20) | ||
| P | 8 (40) | 16 (80) | ||
| Auditory attention (ACPT2) | U = 313.500, z = 3.078, p = 0.002 * | X2 (1, N = 40) = 6.667, p = 0.010 * | ||
| NP | 12 (60) | 4 (20) | ||
| P | 8 (40) | 16 (80) | ||
| Auditory attention (ACPT3) | U = 375.000, z = 4.747, p < 0.001 * | X2 (1, N = 40) = 15.000, p < 0.001 * | ||
| NP | 14 (70) | 2 (10) | ||
| P | 6 (30) | 18 (90) | ||
| Auditory attention (ACPT4) | U = 316.000, z = 3.164, p = 0.001 * | X2 (1, N = 40) = 10.989, p < 0.001 * | ||
| NP | 12 (60) | 2 (10) | ||
| P | 8 (40) | 18 (90) | ||
| ST1 | U = 272.000, z = 2.001, p = 0.052 | X2 (1, N = 40) = 10.989, p < 0.001 * | ||
| NP | 12 (60) | 2 (10) | ||
| P | 8 (40) | 18 (90) | ||
| ST2 | U = 270.000, z = 1.936, p = 0.060 | X2 (1, N = 40) = 10.989, p < 0.001 * | ||
| NP | 12 (60) | 2 (10) | ||
| P | 8 (40) | 18 (90) |
| Test | DMD 44 (n = 9) N (%) | DMD 45–51 (n = 5) N (%) | DMD > 51 (n = 4) N (%) | DMD > 62 (n = 2) N (%) | FET Results |
|---|---|---|---|---|---|
| Lexical comprehension | p = 0.005 * | ||||
| NP | 9 (100) | 5 (100) | 4 (100) | 0 (100) | |
| P | 0 (0) | 0 (0) | 0 (0) | 2 (100) | |
| Syntactic comprehension | |||||
| NP | 9 (100) | 5 (100) | 4 (100) | 2 (100) | |
| P | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Denomination | |||||
| NP | 9 (100) | 5 (100) | 4 (100) | 2 (100) | |
| P | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Articulation | p = 0.167 | ||||
| NP | 4 (44.4) | 0 (0) | 0 (0) | 0 (100) | |
| P | 5 (55.6) | 5 (100) | 4 (100) | 2 (100) | |
| Word repetition | p = 0.002 * | ||||
| NP | 9 (100) | 5 (100) | 2 (50) | 0 (100) | |
| P | 0 (0) | 0 (0) | 2 (50) | 2 (100) | |
| Nonword repetition | p = 0.239 | ||||
| NP | 7 (77.8) | 3 (60) | 2 (50) | 0 (100) | |
| P | 2 (22.2) | 2 (40) | 2 (50) | 2 (100) | |
| Sentence repetition | p = 0.167 | ||||
| NP | 4 (44.4) | 0 (0) | 0 (0) | 0 (100) | |
| P | 5 (55.6) | 5 (100) | 4 (100) | 2 (100) | |
| Visual attention rapidity | p = 0.430 | ||||
| NP | 4 (44.4) | 2 (40) | 0 (0) | 0 (100) | |
| P | 5 (55.6) | 3 (60) | 4 (100) | 2 (100) | |
| Visual attention accuracy | p = 0.430 | ||||
| NP | 4 (44.4) | 2 (40) | 0 (0) | 0 (100) | |
| P | 5 (55.6) | 3 (60) | 4 (100) | 2 (100) | |
| Auditory attention (ACPT1) | p = 0.167 | ||||
| NP | 4 (44.4) | 0 (0) | 0 (0) | 0 (100) | |
| P | 5 (55.6) | 5 (100) | 4 (100) | 2 (100) | |
| Auditory attention (ACPT2) | p = 0.167 | ||||
| NP | 4 (44.4) | 0 (0) | 0 (0) | 0 (100) | |
| P | 5 (55.6) | 5 (100) | 4 (100) | 2 (100) | |
| Auditory attention (ACPT3) | p = 0.763 | ||||
| NP | 2 (22.2) | 0 (0) | 0 (0) | 0 (100) | |
| P | 7 (77.8) | 5 (100) | 4 (100) | 2 (100) | |
| Auditory attention (ACPT4) | p = 0.763 | ||||
| NP | 2 (22.2) | 0 (0) | 0 (0) | 0 (100) | |
| P | 7 (77.8) | 5 (100) | 4 (100) | 2 (100) | |
| ST1 | p = 0.763 | ||||
| NP | 2 (22.2) | 0 (0) | 0 (0) | 0 (100) | |
| P | 7 (77.8) | 5 (100) | 4 (100) | 2 (100) | |
| ST2 | p = 0.763 | ||||
| NP | 2 (22.2) | 0 (0) | 0 (0) | 0 (100) | |
| P | 7 (77.8) | 5 (100) | 4 (100) | 4 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chieffo, D.P.R.; Moriconi, F.; Mastrilli, L.; Lino, F.; Brogna, C.; Coratti, G.; Altobelli, M.; Massaroni, V.; Norcia, G.; Ferraroli, E.; et al. Language Development in Preschool Duchenne Muscular Dystrophy Boys. Brain Sci. 2022, 12, 1252. https://doi.org/10.3390/brainsci12091252
Chieffo DPR, Moriconi F, Mastrilli L, Lino F, Brogna C, Coratti G, Altobelli M, Massaroni V, Norcia G, Ferraroli E, et al. Language Development in Preschool Duchenne Muscular Dystrophy Boys. Brain Sciences. 2022; 12(9):1252. https://doi.org/10.3390/brainsci12091252
Chicago/Turabian StyleChieffo, Daniela Pia Rosaria, Federica Moriconi, Ludovica Mastrilli, Federica Lino, Claudia Brogna, Giorgia Coratti, Michela Altobelli, Valentina Massaroni, Giulia Norcia, Elisabetta Ferraroli, and et al. 2022. "Language Development in Preschool Duchenne Muscular Dystrophy Boys" Brain Sciences 12, no. 9: 1252. https://doi.org/10.3390/brainsci12091252
APA StyleChieffo, D. P. R., Moriconi, F., Mastrilli, L., Lino, F., Brogna, C., Coratti, G., Altobelli, M., Massaroni, V., Norcia, G., Ferraroli, E., Lucibello, S., Pane, M., & Mercuri, E. (2022). Language Development in Preschool Duchenne Muscular Dystrophy Boys. Brain Sciences, 12(9), 1252. https://doi.org/10.3390/brainsci12091252