

Cerebral Hemodynamic Changes during Unaffected Handgrip Exercises in Stroke Patients: An fNIRS Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- Aged between 40 and 70, no gender limitation;
- Convalescent patients with ischemic stroke (first stroke), and course of disease between 1 and 6 months;
- Patients with hemiplegia and the muscle strength of both upper and lower limbs on the hemiplegic side ≤ grade 3 (manual muscle testing MMT), without any functional impairment on the healthy side;
- The ability to perform some aerobic rehabilitation by permission of the attending physician;
- A normal cognitive level (Mini-Mental State Examination, MMSE score > 21 points), the ability to understand the movement instructions of the rehabilitation therapist;
- Not taking any psychotropic drugs.
- The exclusion criteria were as follows:
- Patients whose condition continued to deteriorate, or whose vital signs were unstable;
- Brain damage not limited to one hemisphere;
- Other serious medical conditions, such as having a pacemaker;
- The patient or their family members refused to sign informed consent.
2.2. Experimental Procedure
2.2.1. Basic Data Collection
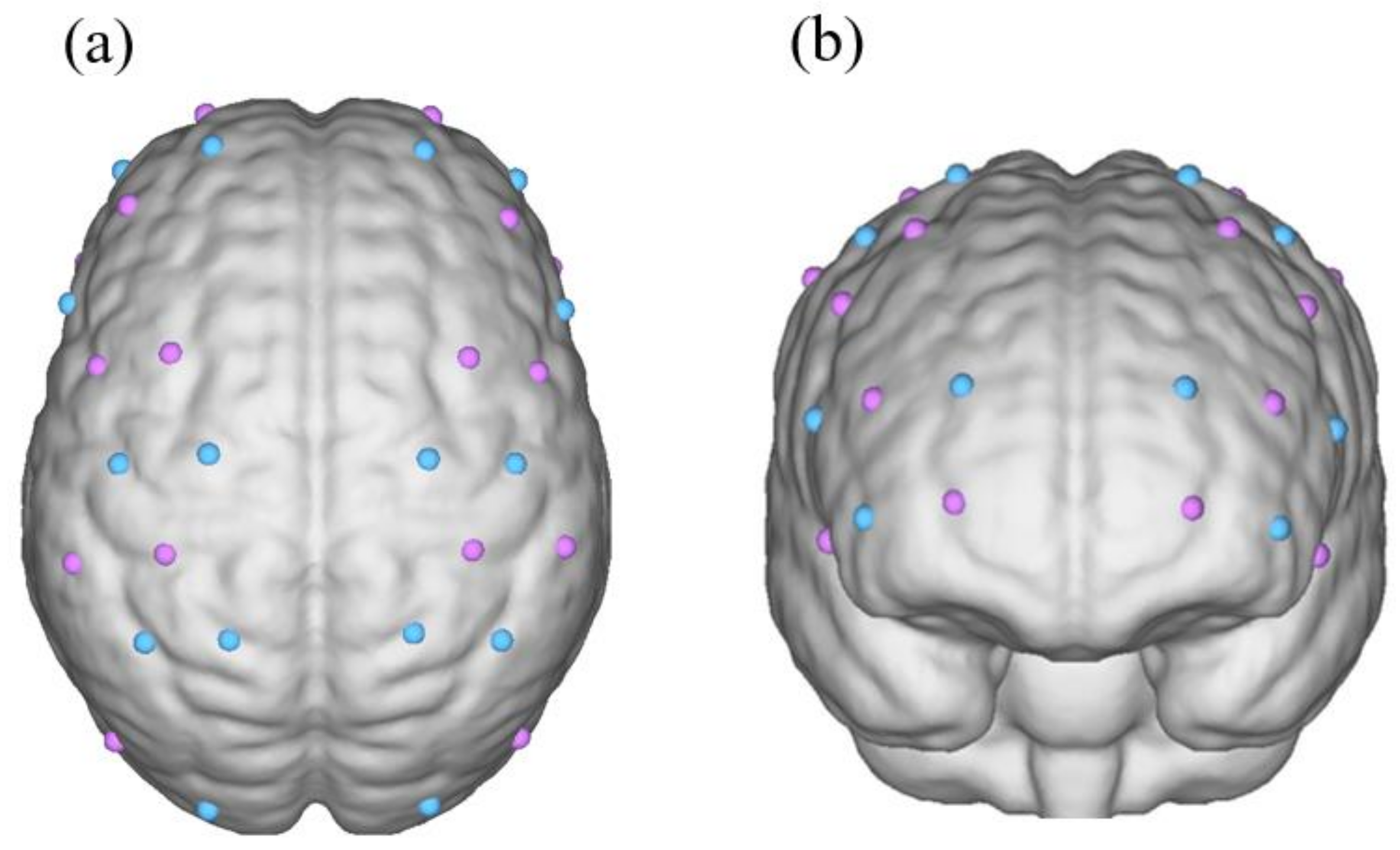
2.2.2. Introduction of fNIRS
2.2.3. fNIRS Data Acquisition
2.3. Data Processing and Analysis
- The fNIRS data of 10 patients with a left-sided hemisphere infarction were flipped using the mirror transformation technique [39], such that the fNIRS data of all 20 patients with a hemisphere infarction were transformed into a right-sided hemisphere infarction to facilitate data processing.
- Based on the concentration of oxygenated hemoglobin in all channels in each ROI divided by the number of channels in each ROI, we obtained the mean oxyhemoglobin of each ROI in the task and rest states. The Shapiro–Wilk method was used to test the normality of the differences between these groups, and data corresponding to the normal distribution were expressed as the mean ± standard deviation. The concentration of HbO in the task and rest state of each grip strength level group were tested using a paired t-test to detect the activation of the ROIs in each hemisphere.
- Levene’s test was applied to calculate the homogeneity of variance in each group. A one-way ANOVA and LSD tests were used to determine whether there were differences in the activation of the ROIs between the different handgrip groups.
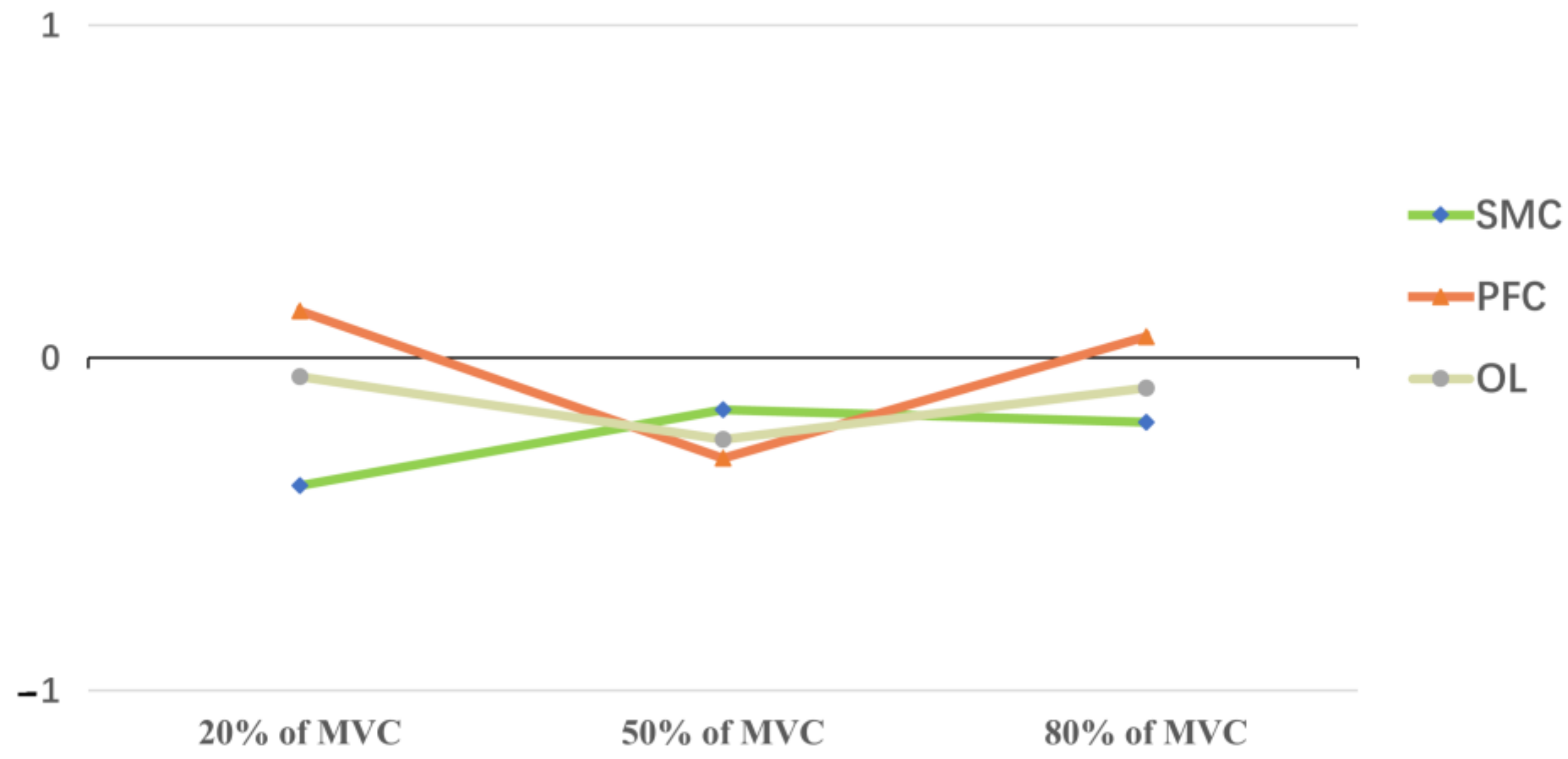
- The calculation of the laterality index (LI) was performed as follows: we calculated the average change in ΔHbO (mean of task HbO concentration–mean of rest HbO concentration) in the ROI of each subject’s ipsilesional and contralesional hemispheres using the formula: (mean ΔHbO ipsilesional–mean ΔHbO contralesional)/(mean ΔHbO ipsilesional + mean ΔHbO contralesional) [40,41]. The results were the relative changes in the HbO in the ROIs in the ipsilesional and contralesional hemispheres. If the LI > 0, the ROIs of the ipsilesional hemispheres were dominant. If LI < 0, the ROIs of the contralesional hemisphere were considered dominant.
3. Results
3.1. Clinical Details of Stroke Patients
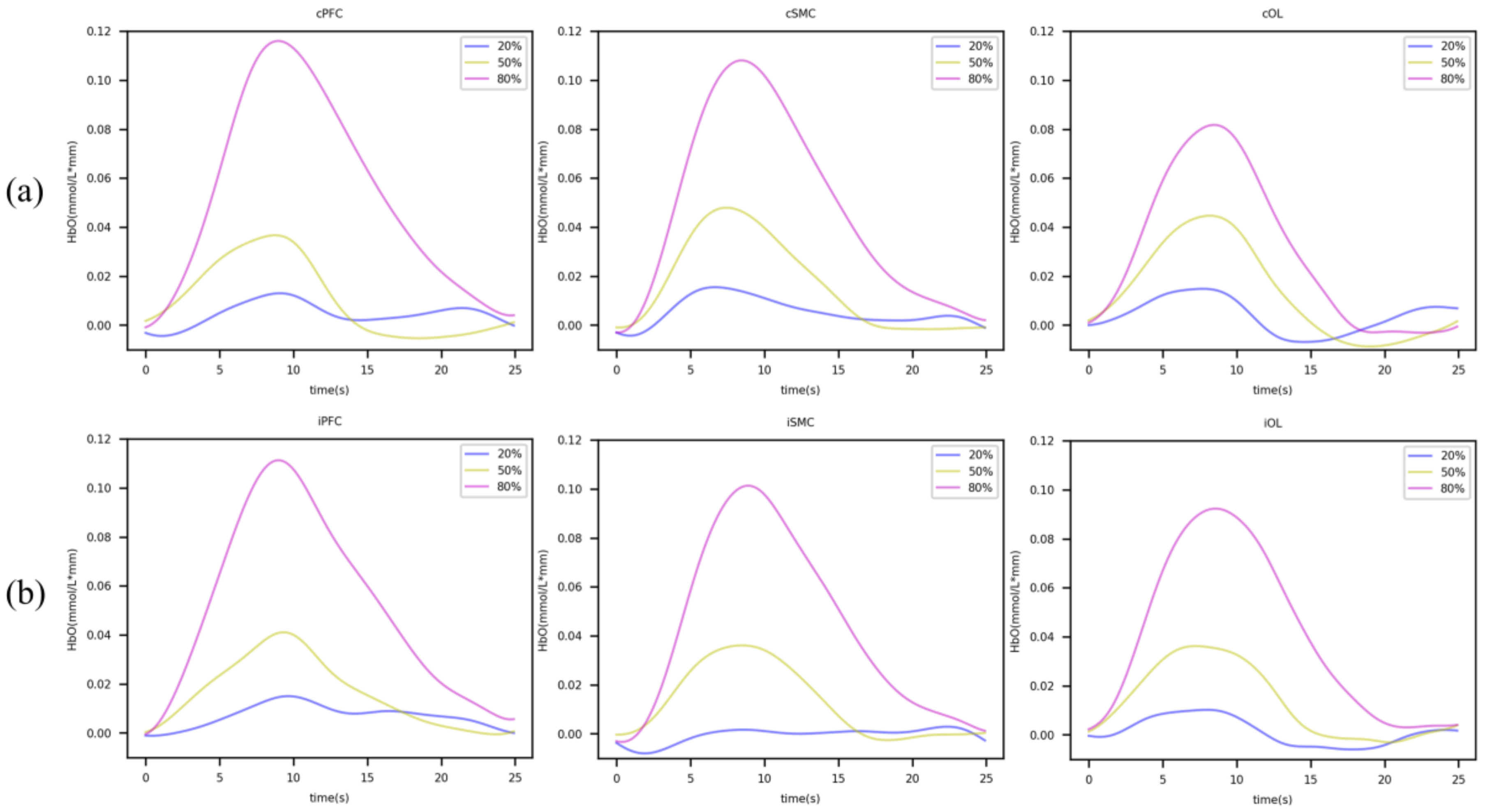
3.2. Activation of Brain Regions in Grip Tasks of Different Strengths
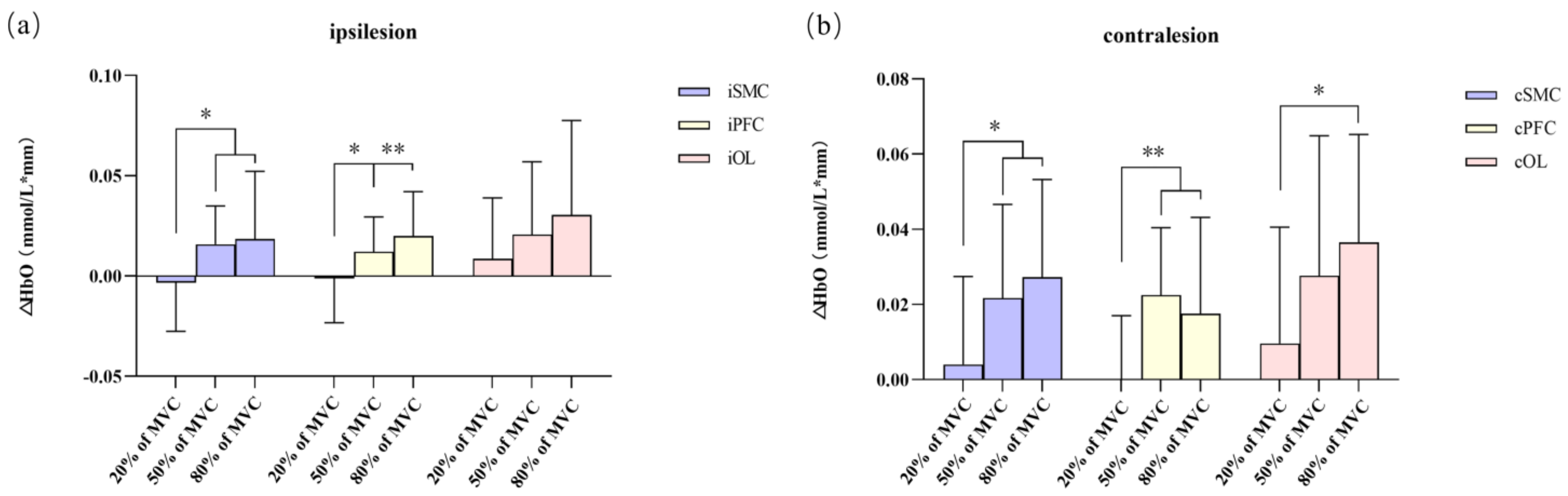
3.3. Difference in HbO Changes in ROIs of Different Grip Strength Groups
3.4. Lateral Index
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Macleod, M.R.; Fisher, M.; O’Collins, V.; Sena, E.S.; Dirnagl, U.; Bath, P.M.; Buchan, A.; Van Der Worp, H.B.; Traystman, R.J.; Minematsu, K.; et al. Reprint: Good laboratory practice: Preventing introduction of bias at the bench. J. Cereb. Blood Flow Metab. 2009, 29, 221–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, Y.; Shim, J.S.; Oh, B.M.; Seo, H.G. Grip Strength on the Unaffected Side as an Independent Predictor of Functional Improvement After Stroke. Am. J. Phys. Med. Rehabil. 2017, 96, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Bailey, E.L.; Smith, C.; Sudlow, C.L.; Wardlaw, J.M. Pathology of lacunar ischemic stroke in humans—A systematic review. Brain Pathol. 2012, 22, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Yeo, B.T.; Krienen, F.M.; Sepulcre, J.; Sabuncu, M.R.; Lashkari, D.; Hollinshead, M.; Roffman, J.L.; Smoller, J.W.; Zöllei, L.; Polimeni, J.R.; et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol. 2011, 106, 1125–1165. [Google Scholar] [CrossRef] [PubMed]
- Swayne, O.B.; Rothwell, J.C.; Ward, N.S.; Greenwood, R.J. Stages of motor output reorganization after hemispheric stroke suggested by longitudinal studies of cortical physiology. Cereb. Cortex 2008, 18, 1909–1922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmichael, S.T. Emergent properties of neural repair: Elemental biology to therapeutic concepts. Ann. Neurol. 2016, 79, 895–906. [Google Scholar] [CrossRef] [Green Version]
- Sehm, B.; Steele, C.J.; Villringer, A.; Ragert, P. Mirror Motor Activity During Right-Hand Contractions and Its Relation to White Matter in the Posterior Midbody of the Corpus Callosum. Cereb. Cortex 2016, 26, 4347–4355. [Google Scholar] [CrossRef] [Green Version]
- Buetefisch, C.M. Role of the Contralesional Hemisphere in Post-Stroke Recovery of Upper Extremity Motor Function. Front. Neurol. 2015, 6, 214. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Zhang, D.; Zhao, Y.Y.; Hai, H.; Ma, Y.W. Effects of high-frequency repetitive transcranial magnetic stimulation over the contralesional motor cortex on motor recovery in severe hemiplegic stroke: A randomized clinical trial. Brain Stimul. 2020, 13, 979–986. [Google Scholar] [CrossRef]
- Park, J.W.; Oh, J.C.; Lee, J.W.; Yeo, J.S.; Ryu, K.H. The effect of 5Hz high-frequency rTMS over contralesional pharyngeal motor cortex in post-stroke oropharyngeal dysphagia: A randomized controlled study. Neurogastroenterol. Motil. 2013, 25, 324-e250. [Google Scholar] [CrossRef]
- Dewanjee, P.; Tran, G.; Stewart, J.C.; Quinlan, E.B.; Dodakian, L.; McKenzie, A.; See, J.; Cramer, S.C. Structural Integrity of the Corpus Callosum Correlates with Sensorimotor Impairment after Stroke. American-heart-association/american Stroke Association International 2015. Stroke 2015, 46, A2. [Google Scholar]
- Carson, R.G. Inter-hemispheric inhibition sculpts the output of neural circuits by co-opting the two cerebral hemispheres. J. Physiol. 2020, 598, 4781–4802. [Google Scholar] [CrossRef] [PubMed]
- Bundy, D.T.; Souders, L.; Baranyai, K.; Leonard, L.; Schalk, G.; Coker, R.; Moran, D.W.; Huskey, T.; Leuthardt, E.C. Contralesional Brain-Computer Interface Control of a Powered Exoskeleton for Motor Recovery in Chronic Stroke Survivors. Stroke 2017, 48, 1908–1915. [Google Scholar] [CrossRef] [PubMed]
- Aswendt, M.; Pallast, N.; Wieters, F.; Baues, M.; Hoehn, M.; Fink, G.R. Lesion Size- and Location-Dependent Recruitment of Contralesional Thalamus and Motor Cortex Facilitates Recovery after Stroke in Mice. Transl. Stroke Res. 2021, 12, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.H.; Chang, W.H.; Ohn, S.H.; Kim, S.T.; Bang, O.Y.; Pascual-Leone, A.; Kim, Y.H. Longitudinal changes of resting-state functional connectivity during motor recovery after stroke. Stroke 2011, 42, 1357–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coscia, M.; Wessel, M.J.; Chaudary, U.; Millán, J.D.R.; Micera, S.; Guggisberg, A.; Vuadens, P.; Donoghue, J.; Birbaumer, N.; Hummel, F.C. Neurotechnology-aided interventions for upper limb motor rehabilitation in severe chronic stroke. Brain 2019, 142, 2182–2197. [Google Scholar] [CrossRef] [Green Version]
- Barker, R.N.; Brauer, S.G. Upper limb recovery after stroke: The stroke survivors’ perspective. Disabil. Rehabil. 2005, 27, 1213–1223. [Google Scholar] [CrossRef]
- Guggisberg, A.G.; Nicolo, P.; Cohen, L.G.; Schnider, A.; Buch, E.R. Longitudinal Structural and Functional Differences Between Proportional and Poor Motor Recovery After Stroke. Neurorehabil. Neural Repair. 2017, 31, 1029–1041. [Google Scholar] [CrossRef] [Green Version]
- Russell, W.; Pritchard-Wiart, L.; Manns, P.J. Clinician perspectives on cross-education in stroke rehabilitation. Disabil. Rehabil. 2018, 40, 2644–2649. [Google Scholar] [CrossRef]
- Pearcey, G.E.P.; Smith, L.A.; Sun, Y.; Zehr, E.P. 1894 revisited: Cross-education of skilled muscular control in women and the importance of representation. PLoS ONE 2022, 17, e0264686. [Google Scholar] [CrossRef]
- Hortobágyi, T.; Taylor, J.L.; Petersen, N.T.; Russell, G.; Gandevia, S.C. Changes in segmental and motor cortical output with contralateral muscle contractions and altered sensory inputs in humans. J. Neurophysiol. 2003, 90, 2451–2459. [Google Scholar] [CrossRef]
- Lee, M.; Carroll, T.J. Cross education: Possible mechanisms for the contralateral effects of unilateral resistance training. Sport. Med. 2007, 37, 1–14. [Google Scholar] [CrossRef]
- Ehrensberger, M.; Simpson, D.; Broderick, P.; Monaghan, K. Cross-education of strength has a positive impact on post-stroke rehabilitation: A systematic literature review. Top. Stroke Rehabil. 2016, 23, 126–135. [Google Scholar] [CrossRef]
- Munn, J.; Herbert, R.D.; Gandevia, S.C. Contralateral effects of unilateral resistance training: A meta-analysis. J. Appl. Physiol. 2004, 96, 1861–1866. [Google Scholar] [CrossRef] [Green Version]
- Farthing, J.P.; Krentz, J.R.; Magnus, C.R. Strength training the free limb attenuates strength loss during unilateral immobilization. J. Appl. Physiol. 2009, 106, 830–836. [Google Scholar] [CrossRef] [Green Version]
- Derosière, G.; Alexandre, F.; Bourdillon, N.; Mandrick, K.; Ward, T.E.; Perrey, S. Similar scaling of contralateral and ipsilateral cortical responses during graded unimanual force generation. Neuroimage 2014, 85 Pt 1, 471–477. [Google Scholar] [CrossRef]
- Carson, R.G.; Riek, S.; Mackey, D.C.; Meichenbaum, D.P.; Willms, K.; Forner, M.; Byblow, W.D. Excitability changes in human forearm corticospinal projections and spinal reflex pathways during rhythmic voluntary movement of the opposite limb. J. Physiol. 2004, 560 Pt 3, 929–940. [Google Scholar] [CrossRef]
- Hanajima, R.; Ugawa, Y.; Machii, K.; Mochizuki, H.; Terao, Y.; Enomoto, H.; Furubayashi, T.; Shiio, Y.; Uesugi, H.; Kanazawa, I. Interhemispheric facilitation of the hand motor area in humans. J. Physiol. 2001, 531 Pt 3, 849–859. [Google Scholar] [CrossRef]
- Leff, D.R.; Orihuela-Espina, F.; Elwell, C.E.; Athanasiou, T.; Delpy, D.T.; Darzi, A.W.; Yang, G.Z. Assessment of the cerebral cortex during motor task behaviours in adults: A systematic review of functional near infrared spectroscopy (fNIRS) studies. Neuroimage 2011, 54, 2922–2936. [Google Scholar] [CrossRef]
- Yücel, M.A.; Selb, J.; Boas, D.A.; Cash, S.S.; Cooper, R.J. Reducing motion artifacts for long-term clinical NIRS monitoring using collodion-fixed prism-based optical fibers. Neuroimage 2014, 85 Pt 1, 192–201. [Google Scholar] [CrossRef] [Green Version]
- Shibuya, K.; Kuboyama, N.; Tanaka, J. Changes in ipsilateral motor cortex activity during a unilateral isometric finger task are dependent on the muscle contraction force. Physiol. Meas. 2014, 35, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Di Pino, G.; Pellegrino, G.; Assenza, G.; Capone, F.; Ferreri, F.; Formica, D.; Ranieri, F.; Tombini, M.; Ziemann, U.; Rothwell, J.C.; et al. Modulation of brain plasticity in stroke: A novel model for neurorehabilitation. Nat. Rev. Neurol. 2014, 10, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Cheng, L.; Yang, G.Y.; Tong, S.; Sun, J.; Miao, F. Functional Activation-Informed Structural Changes during Stroke Recovery: A Longitudinal MRI Study. BioMed Res. Int. 2017, 2017, 4345205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilves, N.; Männamaa, M.; Laugesaar, R.; Ilves, N.; Loorits, D.; Vaher, U.; Kool, P.; Ilves, P. Language lateralization and outcome in perinatal stroke patients with different vascular types. Brain Lang. 2022, 228, 105108. [Google Scholar] [CrossRef] [PubMed]
- Dai, T.H.; Liu, J.Z.; Sahgal, V.; Brown, R.W.; Yue, G.H. Relationship between muscle output and functional MRI-measured brain activation. Exp. Brain Res. 2001, 140, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zheng, Y.; Wang, D.; Wang, L.; Ma, J.; Zhang, J.; Xu, W.; Li, D.; Zhang, D. Application of a common spatial pattern-based algorithm for an fNIRS-based motor imagery brain-computer interface. Neurosci. Lett. 2017, 655, 35–40. [Google Scholar] [CrossRef]
- Scholkmann, F.; Spichtig, S.; Muehlemann, T.; Wolf, M. How to detect and reduce movement artifacts in near-infrared imaging using moving standard deviation and spline interpolation. Physiol. Meas. 2010, 31, 649–662. [Google Scholar] [CrossRef] [Green Version]
- Pinti, P.; Scholkmann, F.; Hamilton, A.; Burgess, P.; Tachtsidis, I. Current Status and Issues Regarding Pre-processing of fNIRS Neuroimaging Data: An Investigation of Diverse Signal Filtering Methods Within a General Linear Model Framework. Front. Hum. Neurosci. 2019, 12, 505. [Google Scholar] [CrossRef] [Green Version]
- Mihara, M.; Fujimoto, H.; Hattori, N.; Otomune, H.; Kajiyama, Y.; Konaka, K.; Watanabe, Y.; Hiramatsu, Y.; Sunada, Y.; Miyai, I.; et al. Effect of Neurofeedback Facilitation on Poststroke Gait and Balance Recovery: A Ran domized Controlled Trial. Neurology 2021, 96, e2587–e2598. [Google Scholar] [CrossRef]
- Brumer, I.; De Vita, E.; Ashmore, J.; Jarosz, J.; Borri, M. Implementation of clinically relevant and robust fMRI-based language lateralization: Choosing the laterality index calculation method. PLoS ONE 2020, 15, e0230129. [Google Scholar] [CrossRef]
- Tang, Q.; Li, G.; Liu, T.; Wang, A.; Feng, S.; Liao, X.; Jin, Y.; Guo, Z.; He, B.; McClure, M.A.; et al. Modulation of interhemispheric activation balance in motor-related areas of stroke patients with motor recovery: Systematic review and meta-analysis of fMRI studies. Neurosci. Biobehav. Rev. 2015, 57, 392–400. [Google Scholar] [CrossRef]
- Du, Q.; Luo, J.; Cheng, Q.; Wang, Y.; Guo, S. Vibrotactile enhancement in hand rehabilitation has a reinforcing effect on sensorimotor brain activities. Front. Neurosci. 2022, 16, 935827. [Google Scholar] [CrossRef]
- Yang, C.L.; Lim, S.B.; Peters, S.; Eng, J.J. Cortical Activation During Shoulder and Finger Movements in Healthy Adults: A Functional Near-Infrared Spectroscopy (fNIRS) Study. Front. Hum. Neurosci. 2020, 14, 260. [Google Scholar] [CrossRef]
- Shibuya, K.; Kuboyama, N.; Yamada, S. Complementary activation of the ipsilateral primary motor cortex during a sustained handgrip task. Eur. J. Appl. Physiol. 2016, 116, 171–178. [Google Scholar] [CrossRef]
- Shibuya, K.; Sadamoto, T.; Sato, K.; Moriyama, M.; Iwadate, M. Quantification of delayed oxygenation in ipsilateral primary motor cortex compared with contralateral side during a unimanual dominant-hand motor task using near-infrared spectroscopy. Brain Res. 2008, 1210, 142–147. [Google Scholar] [CrossRef]
- Andrushko, J.W.; Gould, L.A.; Renshaw, D.W.; Ekstrand, C.; Hortobágyi, T.; Borowsky, R.; Farthing, J.P. High Force Unimanual Handgrip Contractions Increase Ipsilateral Sensorimotor Activation and Functional Connectivity. Neuroscience 2021, 452, 111–125. [Google Scholar] [CrossRef]
- Brown, C.E.; Aminoltejari, K.; Erb, H.; Winship, I.R.; Murphy, T.H. In vivo voltage-sensitive dye imaging in adult mice reveals that somatosensory maps lost to stroke are replaced over weeks by new structural and functional circuits with prolonged modes of activation within both the peri-infarct zone and distant sites. J. Neurosci. 2009, 29, 1719–1734. [Google Scholar] [CrossRef] [Green Version]
- Dijkhuizen, R.M.; Ren, J.; Mandeville, J.B.; Wu, O.; Ozdag, F.M.; Moskowitz, M.A.; Rosen, B.R.; Finklestein, S.P. Functional magnetic resonance imaging of reorganization in rat brain after stroke. Proc. Natl. Acad. Sci. USA 2001, 98, 12766–12771. [Google Scholar] [CrossRef] [Green Version]
- Lemon, R.N. Descending pathways in motor control. Annu. Rev. Neurosci. 2008, 31, 195–218. [Google Scholar] [CrossRef] [Green Version]
- Trunk, B.H.; Ziegler, L.; Gharabaghi, A. Ipsilateral corticospinal maps correspond to severe poststroke motor impairment. Brain Stimul. 2022, 15, 758–760. [Google Scholar] [CrossRef]
- Wolff, W.; Thürmer, J.L.; Stadler, K.M.; Schüler, J. Ready, set, go: Cortical hemodynamics during self-controlled sprint starts. Psychol. Sport Exerc. 2019, 41, 21–28. [Google Scholar] [CrossRef]
- Ge, R.; Wang, Z.; Yuan, X.; Li, Q.; Gao, Y.; Liu, H.; Fan, Z.; Bu, L. The effects of two game interaction modes on cortical activation in subjects of different ages: A functional near-infrared spectroscopy study. IEEE Access 2021, 9, 11405–11415. [Google Scholar] [CrossRef]
- Tachtsidis, I.; Scholkmann, F. False positives and false negatives in functional near-infrared spectroscopy: Issues, challenges, and the way forward. Neurophotonics 2016, 3, 31405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Ejaz, N.; Hertler, B.; Branscheidt, M.; Widmer, M.; Faria, A.V.; Harran, M.D.; Cortes, J.C.; Kim, N.; Celnik, P.A.; et al. Separable systems for recovery of finger strength and control after stroke. J. Neurophysiol. 2017, 118, 1151–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilon, J.F.; De Serres, S.J.; Feldman, A.G. Threshold position control of arm movement with anticipatory increase in grip force. Exp. Brain Res. 2007, 181, 49–67. [Google Scholar] [CrossRef]
- Sturm, W.; Willmes, K. On the functional neuroanatomy of intrinsic and phasic alertness. Neuroimage 2001, 14 Pt 2, S76–S84. [Google Scholar] [CrossRef]
- Herold, F.; Behrendt, T.; Törpel, A.; Hamacher, D.; Müller, N.G.; Schega, L. Cortical hemodynamics as a function of handgrip strength and cognitive performance: A cross-sectional fNIRS study in younger adults. BMC Neurosci. 2021, 22, 10. [Google Scholar] [CrossRef]
- Jiang, Z.; Wang, X.F.; Kisiel-Sajewicz, K.; Yan, J.H.; Yue, G.H. Strengthened functional connectivity in the brain during muscle fatigue. Neuroimage 2012, 60, 728–737. [Google Scholar] [CrossRef] [Green Version]
- Richter, M.; Amunts, K.; Mohlberg, H.; Bludau, S.; Eickhoff, S.B.; Zilles, K.; Caspers, S. Cytoarchitectonic segregation of human posterior intraparietal and adjacent parieto-occipital sulcus and its relation to visuomotor and cognitive functions. Cereb. Cortex 2019, 29, 1305–1327. [Google Scholar] [CrossRef]
- Brancaccio, A.; Tabarelli, D.; Belardinelli, P. A New Framework to Interpret Individual Inter-Hemispheric Compensatory Communication after Stroke. J. Pers. Med. 2022, 12, 59. [Google Scholar] [CrossRef]
- Carroll, T.J.; Herbert, R.D.; Munn, J.; Lee, M.; Gandevia, S.C. Contralateral effects of unilateral strength training: Evidence and possible mechanisms. J. Appl. Physiol. 2006, 101, 1514–1522. [Google Scholar] [CrossRef] [Green Version]
- Bice, A.R.; Xiao, Q.; Kong, J.; Yan, P.; Rosenthal, Z.P.; Kraft, A.W.; Smith, K.P.; Wieloch, T.; Lee, J.M.; Culver, J.P.; et al. Homotopic contralesional excitation suppresses spontaneous circuit repair and global network reconnections following ischemic stroke. eLife 2022, 11, e68852. [Google Scholar] [CrossRef]
- Bradnam, L.V.; Stinear, C.M.; Barber, P.A.; Byblow, W.D. Contralesional hemisphere control of the proximal paretic upper limb following stroke. Cereb. Cortex 2012, 22, 2662–2671. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.L.; Potter-Baker, K.A.; Cunningham, D.A.; Li, M.; Sankarasubramanian, V.; Lee, J.; Jones, S.; Sakaie, K.; Wang, X.; Machado, A.G.; et al. Stratifying chronic stroke patients based on the influence of contralesional motor cortices: An inter-hemispheric inhibition study. Clin. Neurophysiol. 2020, 131, 2516–2525. [Google Scholar] [CrossRef]
- Rostrup, E.; Law, I.; Pott, F.; Ide, K.; Knudsen, G.M. Cerebral hemodynamics measured with simultaneous PET and near-infrared spectroscopy in humans. Brain Res. 2002, 954, 183–193. [Google Scholar] [CrossRef]
- Fu, Y.; Zhang, Q.; Yu, C.; Zhang, J.; Wang, N.; Zuo, S.; Zhang, N. Longitudinal Assessment of Motor Recovery of Contralateral Hand after Basal Ganglia Infarction Using Functional Magnetic Resonance Imaging. BioMed Res. Int. 2016, 2016, 7403795. [Google Scholar] [CrossRef] [Green Version]
- Buetefisch, C.M.; Wei, L.; Gu, X.; Epstein, C.M.; Yu, S.P. Neuroprotection of Low-Frequency Repetitive Transcranial Magnetic Stimulation after Ischemic Stroke in Rats. Ann. Neurol. 2022. [Google Scholar] [CrossRef]
- Zong, X.; Gu, J.; Zhou, S.; Ding, D.; Hu, Y.; Tucker, L.; Huang, Z.; Geng, D.; Gao, D. Continuous theta-burst stimulation enhances and sustains neurogenesis following ischemic stroke. Theranostics 2022, 12, 5710–5726. [Google Scholar] [CrossRef]
- Adeyemo, B.O.; Simis, M.; Macea, D.D.; Fregni, F. Systematic review of parameters of stimulation, clinical trial design characteristics, and motor outcomes in non-invasive brain stimulation in stroke. Front. Psychiatry 2012, 3, 88. [Google Scholar] [CrossRef] [Green Version]
- James, J.; McGlinchey, M.P. How active are stroke patients in physiotherapy sessions and is this associated with stroke severity? Disabil. Rehabil. 2022, 44, 4408–4414. [Google Scholar] [CrossRef]
- Mulder, T. Motor imagery and action observation: Cognitive tools for rehabilitation. J. Neural Transm. 2007, 114, 1265–1278. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects Number | Sex | Age (Year) | Site of Lesion | Course of Disease (Days) | Affected Side | MMSE | MMT | MVC(Kg) | FMA |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 56 | R, PI | 31 | L | 30 | 2+ | 23.3 | 40 |
| 2 | M | 52 | R, PI, BGI | 62 | L | 30 | 2 | 18.5 | 42 |
| 3 | M | 50 | R, PLI, TLI, BGI | 35 | L | 28 | 1+ | 15.8 | 36 |
| 4 | M | 53 | R, BGI | 105 | L | 29 | 2+ | 18.2 | 39 |
| 5 | M | 52 | R, BGI | 96 | L | 27 | 1 | 14.5 | 26 |
| 6 | M | 58 | R, BGI | 38 | L | 28 | 3 | 21 | 42 |
| 7 | M | 53 | R, PI | 64 | L | 30 | 2 | 17.5 | 36 |
| 8 | F | 53 | R, PLI, BGI | 36 | L | 28 | 0 | 13.6 | 22 |
| 9 | M | 64 | R, BGI, PI | 39 | L | 30 | 0 | 18.4 | 28 |
| 10 | M | 59 | R, BGI, PLI | 58 | L | 26 | 3 | 22.6 | 35 |
| 11 | M | 57 | L, BGI, PI | 48 | R | 30 | 0 | 16.8 | 27 |
| 12 | M | 65 | L, TI | 31 | R | 25 | 0 | 14.8 | 29 |
| 13 | F | 64 | L, BGI | 112 | R | 30 | 3 | 13.5 | 33 |
| 14 | M | 53 | L, PI | 41 | R | 28 | 2+ | 14.8 | 37 |
| 15 | M | 40 | L, BGI | 55 | R | 30 | 0 | 22.5 | 21 |
| 16 | F | 60 | L, FLI, TLI, PLI | 30 | R | 29 | 0 | 9.9 | 36 |
| 17 | M | 51 | L, FLI, PLI | 33 | R | 30 | 3 | 19.8 | 40 |
| 18 | M | 65 | L, PI | 60 | R | 27 | 0 | 10.5 | 20 |
| 19 | F | 53 | L, FLI, BGI, OLI | 32 | R | 28 | 0 | 11.5 | 19 |
| 20 | F | 69 | L, BGI | 30 | R | 30 | 0 | 14.9 | 26 |
| ROI | cSMC | iSMC | cPFC | iPFC | cOL | iOL | |
|---|---|---|---|---|---|---|---|
| 20% of MVC | HbOTS | 0.007 ± 0.023 | −0.002 ± 0.022 | 0.004 ± 0.017 | 0.006 ± 0.017 | 0.009 ± 0.019 | 0.006 ± 0.026 |
| HbORS | 0.003 ± 0.017 | 0.001 ± 0.017 | 0.004 ± 0.016 | 0.007 ± 0.020 | −0.000 ± 0.026 | −0.002 ± 0.019 | |
| T | 0.77 | −0.613 | 0.008 | −0.232 | 1.393 | 1.265 | |
| P | 0.451 | 0.547 | 0.993 | 0.819 | 0.180 | 0.221 | |
| d | 0.172 | 0.137 | 0.002 | 0.052 | 0.311 | 0.283 | |
| 50% of MVC | HbOTS | 0.028 ± 0.029 | 0.021 ± 0.027 | 0.023 ± 0.027 | 0.022 ± 0.022 | 0.028 ± 0.041 | 0.025 ± 0.044 |
| HbORS | 0.014 ± 0.031 | 0.006 ± 0.024 | 0.001 ± 0.024 | 0.010 ± 0.023 | 0.001 ± 0.028 | 0.004 ± 0.024 | |
| T | 2.374 | 3.706 | 5.603 | 3.105 | 3.320 | 2.557 | |
| P | 0.028 * | 0.001 ** | 0.000 *** | 0.006 ** | 0.004 ** | 0.019 * | |
| d | 0.531 | 0.829 | 1.253 | 0.694 | 0.742 | 0.572 | |
| 80% of MVC | HbOTS | 0.061 ± 0.042 | 0.053 ± 0.047 | 0.061 ± 0.041 | 0.061 ± 0.047 | 0.049 ± 0.055 | 0.056 ± 0.067 |
| HbORS | 0.034 ± 0.032 | 0.034 ± 0.042 | 0.043 ± 0.042 | 0.041 ± 0.040 | 0.013 ± 0.042 | 0.026 ± 0.037 | |
| T | 4.684 | 2.440 | 3.071 | 4.045 | 5.669 | 2.893 | |
| P | 0.000 *** | 0.025 * | 0.006 ** | 0.001 ** | 0.000 *** | 0.009 ** | |
| d | 1.047 | 0.546 | 0.687 | 0.904 | 1.267 | 0.647 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Yu, Y.; Gao, W.; Hong, Y.; Shen, X. Cerebral Hemodynamic Changes during Unaffected Handgrip Exercises in Stroke Patients: An fNIRS Study. Brain Sci. 2023, 13, 141. https://doi.org/10.3390/brainsci13010141
Ma Y, Yu Y, Gao W, Hong Y, Shen X. Cerebral Hemodynamic Changes during Unaffected Handgrip Exercises in Stroke Patients: An fNIRS Study. Brain Sciences. 2023; 13(1):141. https://doi.org/10.3390/brainsci13010141
Chicago/Turabian StyleMa, Yuqin, Yang Yu, Wen Gao, Yongfeng Hong, and Xianshan Shen. 2023. "Cerebral Hemodynamic Changes during Unaffected Handgrip Exercises in Stroke Patients: An fNIRS Study" Brain Sciences 13, no. 1: 141. https://doi.org/10.3390/brainsci13010141
APA StyleMa, Y., Yu, Y., Gao, W., Hong, Y., & Shen, X. (2023). Cerebral Hemodynamic Changes during Unaffected Handgrip Exercises in Stroke Patients: An fNIRS Study. Brain Sciences, 13(1), 141. https://doi.org/10.3390/brainsci13010141