
Preventive Strategies for Cognitive Decline and Dementia: Benefits of Aerobic Physical Activity, Especially Open-Skill Exercise


Abstract
:1. Introduction
2. Effects of Physical Activity and Exercise Interventions on the Prevention of Cognitive Decline and Dementia
3. Possible Mechanisms Underlying the Effects of Physical Activity and Exercise Interventions on Cognitive Decline and Dementia Prevention
4. Differential Effects of OSE and CSE on the Prevention of Cognitive Decline and Dementia
5. Possible Differences among Sports Classified as OSE in Terms of Their Impact on Cognitive Function
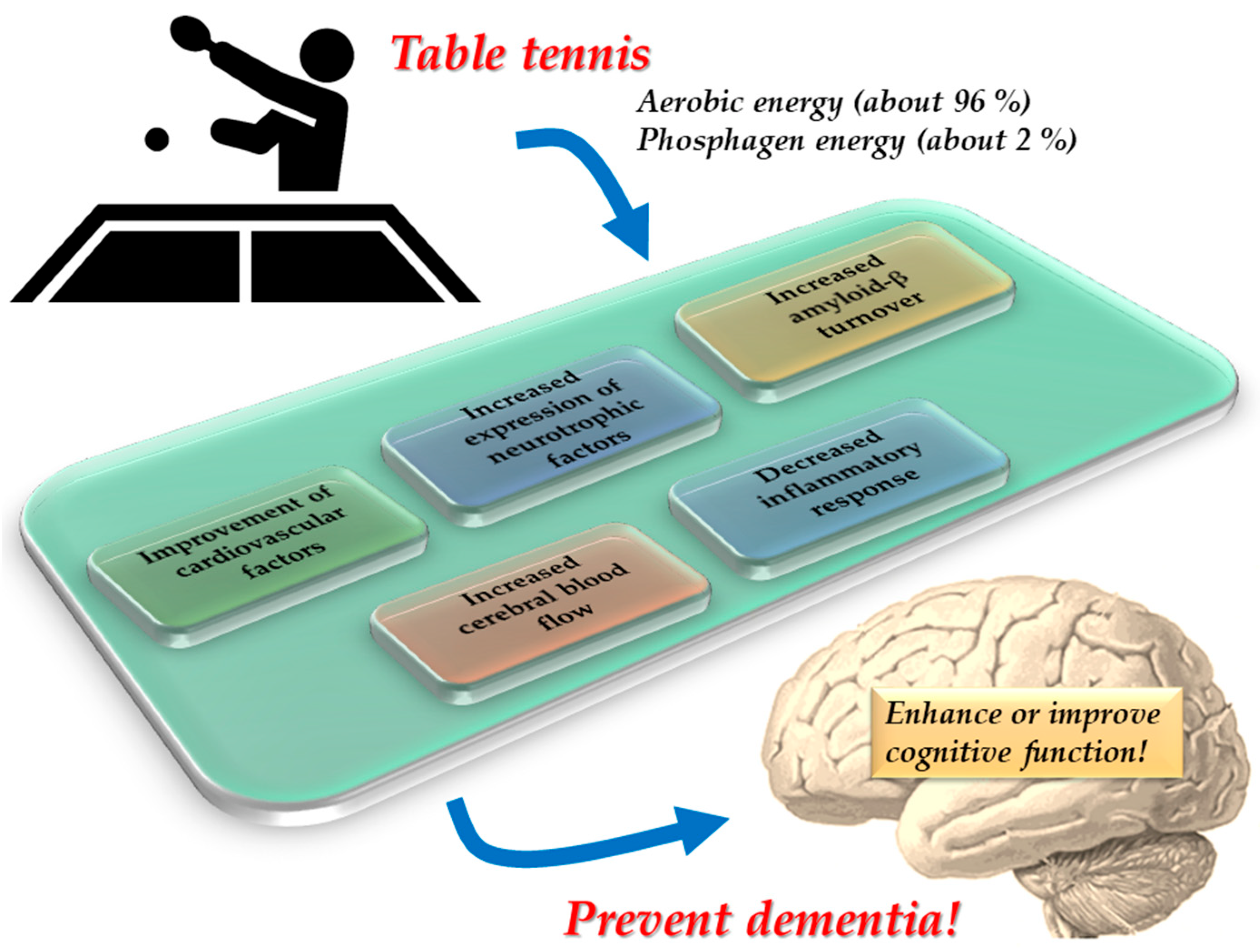
6. Benefits of Table Tennis for Brain Health Maintenance and Dementia Prevention
7. Conclusions and Prospects
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Dementia. Available online: https://www.who.int/en/news-room/fact-sheets/detail/dementia (accessed on 10 March 2023).
- Alzheimer’s Association. 2022 Alzheimer’s disease facts and figures. Alzheimers. Dement. 2022, 18, 700–789. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Manly, J.J.; Jones, R.N.; Langa, K.M.; Ryan, L.H.; Levine, D.A.; McCammon, R.; Heeringa, S.G.; Weir, D. Estimating the prevalence of dementia and mild cognitive impairment in the US: The 2016 Health and Retirement Study Harmonized Cognitive Assessment Protocol Project. JAMA Neurol. 2022, 79, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Achraf, A.; Zou, L.; Apfelbacher, C.; Erickson, K.I.; Müller, N.G. COVID-19, physical (in-)activity, and dementia prevention. Alzheimers. Dement. 2020, 6, e12091. [Google Scholar] [CrossRef]
- Nuzum, H.; Stickel, A.; Corona, M.; Zeller, M.; Melrose, R.J.; Wilkins, S.S. Potential benefits of physical activity in MCI and dementia. Behav. Neurol. 2020, 2020, 7807856. [Google Scholar] [CrossRef] [Green Version]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M.; Cooper, H.; Strauman, T.A.; Welsh-Bohmer, K.; Browndyke, J.N.; Sherwood, A. Aerobic exercise and neurocognitive performance: A meta-analytic review of randomized controlled trials. Psychosom. Med. 2010, 72, 239–252. [Google Scholar] [CrossRef]
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E.; et al. Physical activity, cognition, and brain outcomes: A review of the 2018 physical activity guidelines. Med. Sci. Sport. Exerc. 2019, 51, 1242–1251. [Google Scholar] [CrossRef]
- Chen, F.T.; Hopman, R.J.; Huang, C.J.; Chu, C.H.; Hillman, C.H.; Hung, T.M.; Chang, Y.K. The effect of exercise training on brain structure and function in older adults: A systematic review based on evidence from randomized control trials. J. Clin. Med. 2020, 9, 914. [Google Scholar] [CrossRef] [Green Version]
- Srinivas, N.S.; Vimalan, V.; Padmanabhan, P.; Gulyás, B. An overview on cognitive function enhancement through physical exercises. Brain Sci. 2021, 11, 1289. [Google Scholar] [CrossRef] [PubMed]
- Öhman, H.; Savikko, N.; Strandberg, T.E.; Pitkälä, K.H. Effect of physical exercise on cognitive performance in older adults with mild cognitive impairment or dementia: A systematic review. Dement. Geriatr. Cogn. Disord. 2014, 38, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Ito, K.; Shimokata, H.; Washimi, Y.; Endo, H.; Kato, T. A randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairment. PLoS ONE 2013, 8, e61483. [Google Scholar] [CrossRef] [Green Version]
- Heyn, P.; Abreu, B.C.; Ottenbacher, K.J. The effects of exercise training on elderly persons with cognitive impairment and dementia: A meta-analysis. Arch. Phys. Med. Rehabil. 2004, 85, 1694–1704. [Google Scholar] [CrossRef]
- Demurtas, J.; Schoene, D.; Torbahn, G.; Marengoni, A.; Grande, G.; Zou, L.; Petrovic, M.; Maggi, S.; Cesari, M.; Lamb, S.; et al. Physical activity and exercise in mild cognitive impairment and dementia: An umbrella review of intervention and observational studies. J. Am. Med. Dir. Assoc. 2020, 21, 1415–1422.e6. [Google Scholar] [CrossRef]
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst. Rev. 2013, 12, CD006489. [Google Scholar]
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst. Rev. 2015, 4, CD006489. [Google Scholar]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia; WHO Guidelines; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Behrendt, T.; Kirschnick, F.; Kröger, L.; Beileke, P.; Rezepin, M.; Brigadski, T.; Leßmann, V.; Schega, L. Comparison of the effects of open vs. closed skill exercise on the acute and chronic BDNF, IGF-1 and IL-6 response in older healthy adults. BMC Neurosci. 2021, 22, 71. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Zou, L.; Loprinzi, P.D.; Quan, M.; Huang, T. Effects of open versus closed skill exercise on cognitive function: A systematic review. Front. Psychol. 2019, 10, 1707. [Google Scholar] [CrossRef] [Green Version]
- Zhu, H.; Chen, A.; Guo, W.; Zhu, F.; Wang, B. Which type of exercise is more beneficial for cognitive function? A meta-analysis of the effects of open-skill exercise versus closed-skill exercise among children, adults, and elderly populations. Appl. Sci. 2020, 10, 2737. [Google Scholar] [CrossRef] [Green Version]
- Gallaway, P.J.; Miyake, H.; Buchowski, M.S.; Shimada, M.; Yoshitake, Y.; Kim, A.S.; Hongu, N. Physical activity: A viable way to reduce the risks of mild cognitive impairment, Alzheimer’s disease, and vascular dementia in older adults. Brain Sci. 2017, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamer, M.; Chida, Y. Physical activity and risk of neurodegenerative disease: A systematic review of prospective evidence. Psychol Med. 2009, 39, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Valecchi, D.; Bacci, D.; Abbate, R.; Gensini, G.F.; Casini, A.; Macchi, C. Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J. Intern. Med. 2011, 269, 107–117. [Google Scholar] [CrossRef]
- Stephen, R.; Hongisto, K.; Solomon, A.; Lönnroos, E. Physical activity and Alzheimer’s disease: A systematic review. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 733–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J. The relationship between physical activity and dementia: A systematic review and meta-analysis of prospective cohort studies. J. Gerontol. Nurs. 2018, 44, 22–29. [Google Scholar] [PubMed]
- Barha, C.K.; Davis, J.C.; Falck, R.S.; Nagamatsu, L.S.; Liu-Ambrose, T. Sex differences in exercise efficacy to improve cognition: A systematic review and meta-analysis of randomized controlled trials in older humans. Front. Neuroendocrinol. 2017, 46, 71–85. [Google Scholar] [CrossRef]
- Yamasaki, T. Benefits of table tennis for brain health maintenance and prevention of dementia. Encyclopedia 2022, 2, 1577–1589. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International exercise recommendations in older adults (ICFSR): Expert consensus guidelines. J. Nutr. Health Aging. 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Lautenschlager, N.L.; Cox, K.; Hill, K.D.; Pond, D.; Ellis, K.A.; Dow, B.; Hosking, D.; Chong, T.; You, E.; Curran, E.; et al. Physical Activity Guidelines for Older Australians with Mild Cognitive impairment or Subjective Cognitive Decline; Dementia Collaborative Research Centres: Melbourne, Australia, 2018; Available online: http://www.dementia.unsw.edu.au/ (accessed on 30 January 2023).
- De la Rosa, A.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; Millan, F.; Salvador-Pascual, A.; García-Lucerga, C.; Blasco-Lafarga, C.; Garcia-Dominguez, E.; Carretero, A.; Correas, A.G.; et al. Physical exercise in the prevention and treatment of Alzheimer’s disease. J. Sport Health Sci. 2020, 9, 394–404. [Google Scholar] [CrossRef]
- Kim, Y.J.; Han, K.D.; Baek, M.S.; Cho, H.; Lee, E.J.; Lyoo, C.H. Association between physical activity and conversion from mild cognitive impairment to dementia. Alzheimers Res. Ther. 2020, 12, 136. [Google Scholar] [CrossRef]
- Di Liegro, C.M.; Schiera, G.; Proia, P.; Di Liegro, I. Physical activity and brain health. Genes 2019, 10, 720. [Google Scholar] [CrossRef] [Green Version]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [Green Version]
- Stillman, C.M.; Lopez, O.L.; Becker, J.T.; Kuller, L.H.; Mehta, P.D.; Tracy, R.P.; Erickson, K.I. Physical activity predicts reduced plasma β amyloid in the cardiovascular health study. Ann. Clin. Transl. Neurol. 2017, 4, 284–291. [Google Scholar] [CrossRef]
- Cassilhas, R.C.; Viana, V.A.; Grassmann, V.; Santos, R.T.; Santos, R.F.; Tufik, S.; Mello, M.T. The impact of resistance exercise on the cognitive function of the elderly. Med. Sci. Sport. Exerc. 2007, 39, 1401–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, C.L.; Wang, C.H.; Pan, C.Y.; Chen, F.C. The effects of long-term resistance exercise on the relationship between neurocognitive performance and GH, IGF-1, and homocysteine levels in the elderly. Front. Behav. Neurosci. 2015, 9, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.W.; McTiernan, A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; Cholerton, B.A.; et al. Effects of aerobic exercise on mild cognitive impairment: A controlled trial. Arch. Neurol. 2010, 67, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Stein, A.M.; da Silva, T.M.V.; Coelho, F.G.M.; Rueda, A.V.; Camarini, R.; Galduróz, R.F.S. Acute exercise increases circulating IGF-1 in Alzheimer’s disease patients, but not in older adults without dementia. Behav. Brain Res. 2021, 396, 112903. [Google Scholar] [CrossRef]
- Vital, T.M.; Stein, A.M.; de Melo Coelho, F.G.; Arantes, F.J.; Teodorov, E.; Santos-Galduróz, R.F. Physical exercise and vascular endothelial growth factor (VEGF) in elderly: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Pedrinolla, A.; Venturelli, M.; Fonte, C.; Tamburin, S.; Di Baldassarre, A.; Naro, F.; Varalta, V.; Giuriato, G.; Ghinassi, B.; Muti, E.; et al. Exercise training improves vascular function in patients with Alzheimer’s disease. Eur. J. Appl. Physiol. 2020, 120, 2233–2245. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Roh, H.T. Taekwondo enhances cognitive function as a result of increased neurotrophic growth factors in elderly women. Int. J. Environ. Res. Public Health 2019, 16, 962. [Google Scholar] [CrossRef] [Green Version]
- Liang, K.Y.; Mintun, M.A.; Fagan, A.M.; Goate, A.M.; Bugg, J.M.; Holtzman, D.M.; Morris, J.C.; Head, D. Exercise and Alzheimer’s disease biomarkers in cognitively normal older adults. Ann. Neurol. 2010, 68, 311–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomoto, T.; Liu, J.; Tseng, B.Y.; Pasha, E.P.; Cardim, D.; Tarumi, T.; Hynan, L.S.; Munro Cullum, C.; Zhang, R. One-year aerobic exercise reduced carotid arterial stiffness and increased cerebral blood flow in amnestic mild cognitive impairment. J. Alzheimers Dis. 2021, 80, 841–853. [Google Scholar] [CrossRef] [PubMed]
- van der Kleij, L.A.; Petersen, E.T.; Siebner, H.R.; Hendrikse, J.; Frederiksen, K.S.; Sobol, N.A.; Hasselbalch, S.G.; Garde, E. The effect of physical exercise on cerebral blood flow in Alzheimer’s disease. Neuroimage Clin. 2018, 20, 650–654. [Google Scholar] [PubMed]
- Nascimento, C.M.; Pereira, J.R.; de Andrade, L.P.; Garuffi, M.; Talib, L.L.; Forlenza, O.V.; Cancela, J.M.; Cominetti, M.R.; Stella, F. Physical exercise in MCI elderly promotes reduction of pro-inflammatory cytokines and improvements on cognition and BDNF peripheral levels. Curr. Alzheimer. Res. 2014, 11, 799–805. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Heilmann, F.; Weinberg, H.; Wollny, R. The impact of practicing open- vs. closed-skill sports on executive functions—A meta-analytic and systematic review with a focus on characteristics of sports. Brain Sci. 2022, 12, 1071. [Google Scholar] [CrossRef]
- Dai, C.T.; Chang, Y.K.; Huang, C.J.; Hung, T.M. Exercise mode and executive function in older adults: An ERP study of task-switching. Brain Cogn. 2013, 83, 153–162. [Google Scholar] [CrossRef]
- Guo, W.; Wang, B.; Lu, Y.; Zhu, Q.; Shi, Z.; Ren, J. The relationship between different exercise modes and visuospatial working memory in older adults: A cross-sectional study. PeerJ 2016, 4, e2254. [Google Scholar]
- Huang, C.-J.; Lin, P.-C.; Hung, C.-L.; Chang, Y.-K.; Hung, T.-M. Type of physical exercise and inhibitory function in older adults: An event-related potential study. Psychol. Sport Exerc. 2014, 15, 205–211. [Google Scholar]
- Li, D.; Huang, C.-J.; Liu, S.C.; Chang, K.H.; Hung, T.M. Exercise type relates to inhibitory and error processing functions in older adults. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2019, 26, 865–881. [Google Scholar] [CrossRef]
- Tsai, C.L.; Wang, W.L. Exercise-mode-related changes in task-switching performance in the elderly. Front. Behav. Neurosci. 2015, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.L.; Wang, C.H.; Pan, C.Y.; Chen, F.C.; Huang, S.Y.; Tseng, Y.T. The effects of different exercise types on visuospatial attention in the elderly. Psychol. Sport Exerc. 2016, 26, 130–138. [Google Scholar] [CrossRef]
- Wang, B.; Guo, W. Exercise mode and attentional networks in older adults: A cross-sectional study. PeerJ 2020, 8, e8364. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Ottoboni, G.; Tessari, A.; Setti, A. One bout of open skill exercise improves cross-modal perception and immediate memory in healthy older adults who habitually exercise. PLoS ONE 2017, 12, e0178739. [Google Scholar]
- Tsai, C.L.; Pan, C.Y.; Chen, F.C.; Tseng, Y.T. Open- and closed-skill exercise interventions produce different neurocognitive effects on executive functions in the elderly: A 6-month randomized, controlled trial. Front. Aging Neurosci. 2017, 9, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ke, L.; Lanlan, Z.; Jian, Z.; Jianing, W. Comparison of open-skill and closed-skill exercises in improving the response inhibitory ability of the elderly: A protocol for a randomised controlled clinical trial. BMJ Open 2021, 11, e051966. [Google Scholar] [PubMed]
- Hung, C.L.; Tseng, J.W.; Chao, H.H.; Hung, T.M.; Wang, H.S. Effect of acute exercise mode on serum brain-derived neurotrophic factor (BDNF) and task switching performance. J. Clin. Med. 2018, 7, 301. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, D.; Yıldırım, C.; Akcan, F.; Özdal, M.; Abakay, Z.; Bağçeci, A. The investigation of visual and auditory reaction time in racket sports by skills and sedentary. Eur. J. Phys. Educ. Sport Sci. 2019, 5, 11–18. [Google Scholar]
- Can, S.; Kilit, B.; Arslan, E.; Suveren, S. The comparison of reaction time of male tennis players, table tennis players and the ones who don’t exercise at all in 10 to 12 age groups. Niğde Univ. J. Phys. Educ. Sport Sci. 2014, 8, 195–201. [Google Scholar]
- Japan Table Tennis Therapy Association. Available online: https://www.takkyu-ryoho.or.jp/ (accessed on 10 March 2023).
- Bounce Alzheimer’s Therapy Foundation. Available online: https://www.batfoundation.com/ (accessed on 10 March 2023).
- Schmikli, S.L.; Backx, F.J.; Kemler, H.J.; van Mechelen, W. National survey on sports injuries in the Netherlands: Target populations for sports injury prevention programs. Clin. J. Sport Med. 2009, 19, 101–106. [Google Scholar]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.; Ngandu, T.; Rusanen, M.; Antikainen, R.; Bäckman, L.; Havulinna, S.; Hänninen, T.; Laatikainen, T.; Lehtisalo, J.; Levälahti, E.; et al. Multidomain lifestyle intervention benefits a large elderly population at risk for cognitive decline and dementia regardless of baseline characteristics: The FINGER trial. Alzheimers Dement. 2018, 14, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Vostrý, M. Combined therapy for patients after ischemic stroke from the point of view of comprehensive rehabilitation. J. Educ. Cult. Soc. 2020, 1, 119–125. [Google Scholar] [CrossRef]
- Vostrý, M.; Fischer, S.; Lanková, B. The effect of combined therapy on the support and development of social skills of people with multiple sclerosis in senior age. Neuroendocrinol. Lett. 2020, 41, 270–274. [Google Scholar] [PubMed]


{kind=link}
| Adults Aged ≥ 65 Years |
|---|
|
|
|
|
|
|
| Possible Mechanisms |
|---|
|
|
|
|
|
| OSE | CSE |
|---|---|
Special environments
Task requirements
| Special environments
Task requirements
|
| OSE | CSE |
|---|---|
Category 4
Category 3
| Category 2
Category 1
|
| References | Participants and Study Protocol (1. Study Design; 2. Participants; 3. Exercise experience or intervention; and 4. Cognitive tasks; 5. Cognitive functions) | Main Findings |
| Dai et al. [50] |
| (Task-switching paradigm)
|
| Guo et al. [51] |
| (Visuospatial working memory task)
|
| Huang et al. [52] |
| (Eriksen flanker task)
|
| Li et al. [53] |
| (Stroop color-word interference task)
|
| Tsai and Wang [54] |
| (Task-switching paradigm)
|
| Tsai et al. [55] |
| (Central cue Posner paradigm)
|
| Wang and Guo [56] |
| (Attention network test)
|
| O’Brien et al. [57] |
| (Sound-induced flash illusion task)
|
| Tsai et al. [58] |
| (Task-switching paradigm)
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamasaki, T. Preventive Strategies for Cognitive Decline and Dementia: Benefits of Aerobic Physical Activity, Especially Open-Skill Exercise. Brain Sci. 2023, 13, 521. https://doi.org/10.3390/brainsci13030521
Yamasaki T. Preventive Strategies for Cognitive Decline and Dementia: Benefits of Aerobic Physical Activity, Especially Open-Skill Exercise. Brain Sciences. 2023; 13(3):521. https://doi.org/10.3390/brainsci13030521
Chicago/Turabian StyleYamasaki, Takao. 2023. "Preventive Strategies for Cognitive Decline and Dementia: Benefits of Aerobic Physical Activity, Especially Open-Skill Exercise" Brain Sciences 13, no. 3: 521. https://doi.org/10.3390/brainsci13030521
APA StyleYamasaki, T. (2023). Preventive Strategies for Cognitive Decline and Dementia: Benefits of Aerobic Physical Activity, Especially Open-Skill Exercise. Brain Sciences, 13(3), 521. https://doi.org/10.3390/brainsci13030521