1. Introduction
Proneness to emotion dysregulation and insecure attachment are maladaptive features of borderline personality (BP), which can be found to be widely distributed within the population, as well as a psychopathological severity continuum that includes the clinical entity of borderline personality disorder at the most extreme pole [
1,
2,
3,
4,
5]). Despite the different conceptualizations of BP, which vary in the emphasis they attribute to the role of emotion dysregulation [
6,
7] or attachment/mentalization disturbances [
8], such factors can be viewed as closely and inevitably connected. Nevertheless, researchers have often investigated the roles of emotion dysregulation and attachment disturbance in BP in separate studies; thus, the question of how emotional dysregulation and attachment entwine in this disorder has remained unanswered.
The Diagnostic and Statistical Manual of mental disorders (DSM-IV-TR) describes emotion dysregulation of BP disorder in terms of “affective instability due to a marked reactivity of mood”, with a specific emphasis on anger regulation in terms of “inappropriate, intense anger or difficulty controlling anger” [
9]. Studies on emotion dysregulation in BP disorder have shown the existence of general difficulties in regulating emotions [
3,
10,
11] corroborated by neuroimaging evidence of impairments in the fronto-limbic brain circuits implicated in the cognitive control of emotions in BP patients [
4,
5,
12]. The perpetuation of emotional dysregulation in BP can be attributed to the limited use of adaptive emotion regulation strategies and the habitual use of maladaptive strategies (for a meta-analysis see [
13]). For example, to regulate emotions, BP patients report relying on suppression [
14,
15], rumination [
16,
17,
18], experiential avoidance [
19,
20], and emotional avoidance [
21,
22]. In the specific case of anger, previous studies have reported high levels of trait anger in BP patients [
3,
23,
24] Furthermore, anger suppression and rumination seem to be prominent factors in association with BP features [
3,
25,
26,
27] and have been linked to aggressive behaviours [
28,
29] and self-harming [
30].
Regarding interpersonal difficulties in BP disorder, the DSM [
9] describes them as “frantic efforts to avoid real or imagined abandonment” and “unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation”, which strongly imply the prominence of attachment difficulties. Previous studies have reported that individuals with borderline traits tend to have a perception of others as malevolent [
3,
31,
32] and to view themselves as unlovable and inherently bad [
33,
34,
35,
36]. These difficulties, seen through the lens of attachment theory, are believed to derive from maladaptive mental representations of the self and others [
37,
38]. In agreement, studies on adult attachment clearly converge in indicating a strong association between BP and insecure attachment, together with its inverse relationship with secure attachment [
38,
39]. Among insecure attachment categories, preoccupied and unresolved–disorganized subtypes emerged as overrepresented in BP disorder in interview-based studies [
40,
41,
42,
43] Self-report studies, which have investigated the dimensions of anxiety and avoidance in the adult romantic attachments of BP patients, indicate the dimension of attachment anxiety as the one most strongly correlated with BP traits, even if avoidance was also reported as an associated factor [
44].
The connection between attachment and emotion regulation has been emphasized in recent contributions in the field of attachment research [
45,
46,
47]. From this perspective, in cases of distress, individuals with avoidant attachment tend to inhibit or block the activation of the attachment system, and to keep attachment needs and tendencies deactivated, leading to the inhibition or suppression of emotional [
48]. On the contrary, individuals with anxious attachment tend to hyper-activate the attachment system, resulting in the chronic intensification of negative emotions that demand attention and care or that emphasize a person’s vulnerability and neediness [
49]. An alternative view asserts that the association between attachment and emotion regulation styles may differ depending on the specific emotion involved and its role in attachment-related interpersonal dynamics [
50,
51]. Indeed, while the outward expression of some negative emotions (e.g., sadness, anxiety, fear, and shame) may serve to elicit attention and maintain proximity with others, the outward expression of anger may potentially reduce the likelihood of others offering support and therefore compromise the maintenance of interpersonal relationships. Due to the scarcity of studies specifically focused on anger regulation, such alternative hypotheses have not been empirically verified [
52].
Regarding the interplay between anger regulation and attachment in relation to BP, the available evidence suggests that temperamental variability in anger experience mediates the association between attachment and BP [
53,
54,
55]. Only a few studies have investigated the role of anger regulation as a mediator of this association [
56,
57,
58], suggesting that secure attachment may function as a buffer against BP disorder by enhancing the use of positive emotion regulation strategies, while negative emotion regulation strategies seem to dilute the protective effect of secure attachment [
56]. However, to our knowledge, no study has yet investigated how the regulation of anger may influence the association between attachment and BP. Due to the relevance of anger dysregulation in BPD, the investigation of its role as a possible mediator between attachment and BPD features deserves special attention.
In the present study, we aimed to explore the relationship between attachment orientations, BP traits and anger regulation, with a further aim of investigating how anger regulation works in concert with or in opposition to attachment variables, culminating in BP features. To better explore these associations, we considered several domains of BP features (affective instability, identity problems, negative relationships, and self-harm). Regarding anger regulation, we referred to the taxonomy of adaptive and maladaptive anger regulation processes proposed by Spielberger and colleagues [
59]. Among maladaptive processes, “anger out” refers to a failure in anger regulation that leads to excessive or inappropriate expressions of anger towards other persons or objects, while “anger in” refers to the tendency to hold in, turn to the self and suppress angry feelings. The adaptive form of regulation refers to active attempts to avoid anger externalization through physical and verbal expressions (“anger control out”) or by calming down or cooling off (“anger control in”). Our main hypothesis was that attachment insecurity is associated with greater use of maladaptive forms of emotion regulation and less anger control, and that these anger regulation difficulties, in turn, exacerbate BP features.
4. Discussion
Anger regulation is a core aspect of BP, and attachment orientations strongly influence the way individuals manage their emotions. This study was designed to investigate the role of different aspects of anger regulation as potential mediators of the associations between attachment orientations and several dimensions of BP features, including affect instability, identity problems, relational difficulties and self-harm.
The analysis of the associations between attachment orientations and BP confirmed previous evidence indicating that attachment anxiety and avoidance are strongly associated with BP features in both non-clinical [
32,
71]) and clinical populations [
72,
73]. Of note, we observed such associations considering both the total BP scores and the four symptomatic domains tapped by the PAI-BOR questionnaire (Affective Instability, Identity Problems, Negative Relationships, and Self-Harm).
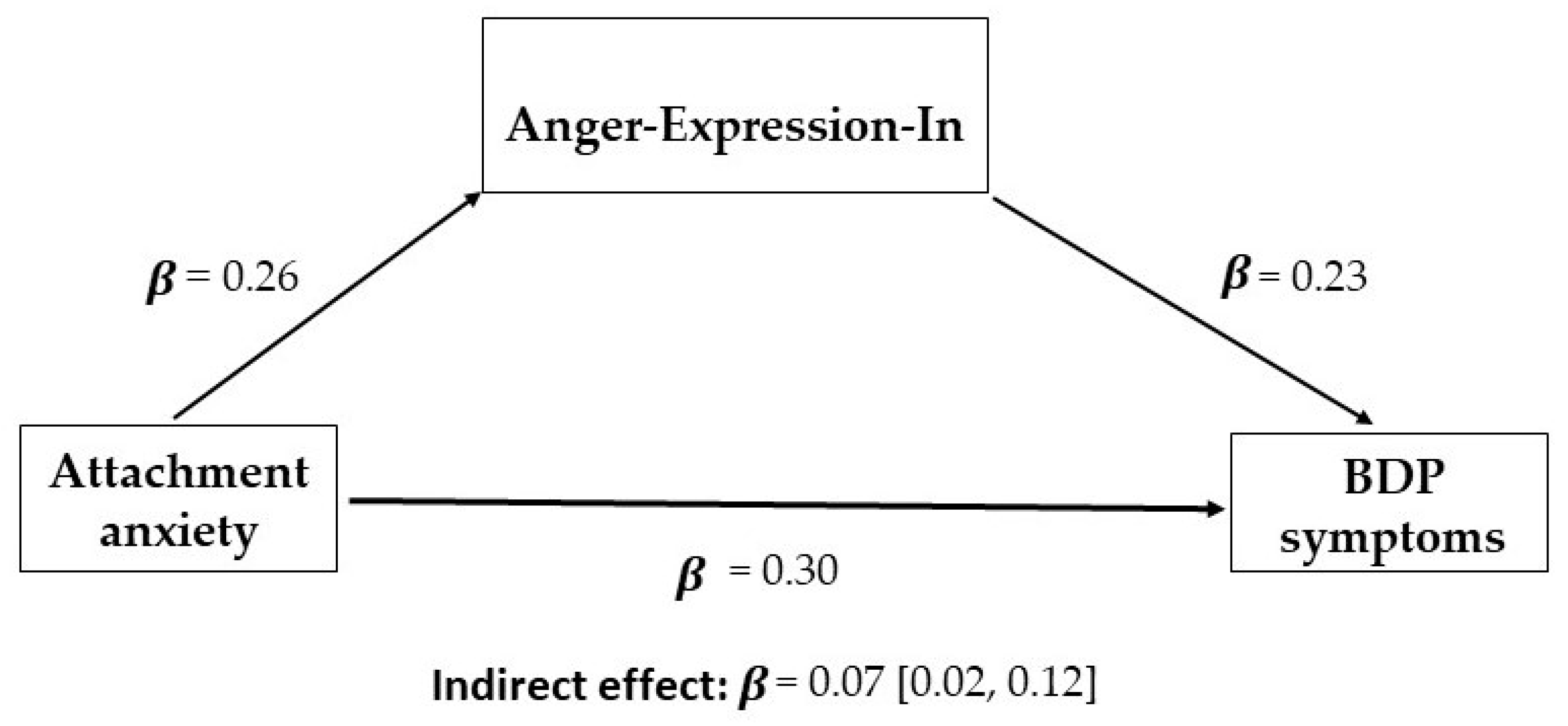
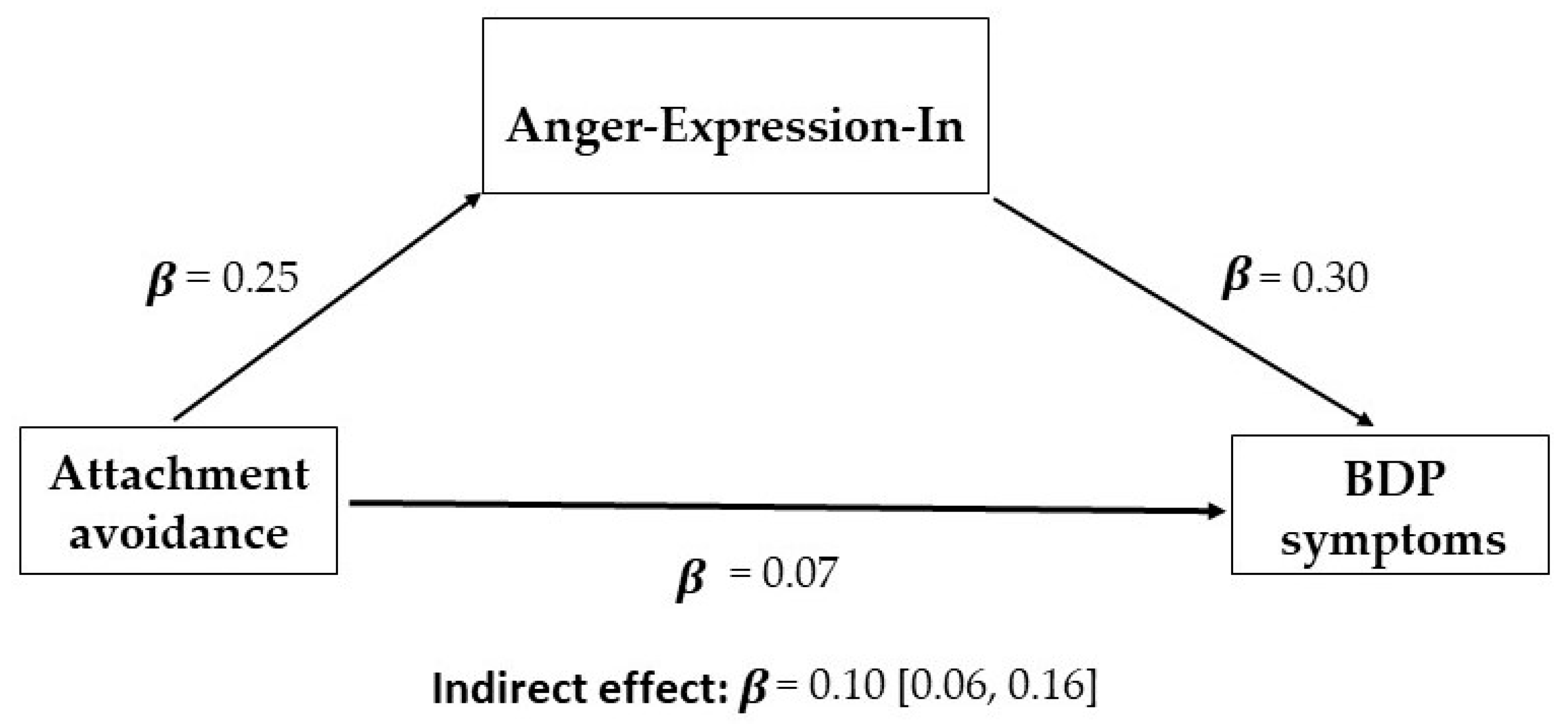
With regard to the associations between anger regulation and attachment, we identified the internal expression of anger as the most relevant source of individual differences associated with attachment. This subscale refers to the extent to which people hold things in and suppress anger when they are angry [
59]. These variables were positively associated with both anxious and avoidant attachment orientations, and were also predictive of BP. Importantly, the mediation analyses showed that the suppression of anger was also a significant mediator in the association between insecure attachment orientations and BP. Thus, participants having high levels of attachment insecurity were more likely to hold in their angry reactions, and this tendency, in turn, was predictive of higher scores in BP.
On the basis of the previous literature on attachment-related differences in emotion regulation [
45,
46,
48], the association between the tendency to suppress anger and attachment avoidance is expected, while in the case of attachment anxiety, the expectation is an association with the tendency to under-regulate emotions [
74] Instead, our results are more in line with the hypothesis that attachment-related differences in emotion regulation are emotion-specific [
50,
51]. According to this hypothesis, attachment-related differences in emotion regulation are oriented to the satisfaction of attachment needs. Individuals who are high in attachment anxiety tend to under-regulate other negative emotions, but they may instead implement a suppression strategy when dealing with anger specifically [
52]. Suppressing anger, indeed, may be more congruent with the attachment goal of abandonment avoidance [
75]. Even though the literature concerning the specific dynamics of anger regulation in association with attachment styles is still scarce, the association between attachment anxiety and anger suppression has indeed been reported in previous studies [
52,
76].
The specificity of attachment-related differences in anger regulation may also explain the results concerning the external control of anger. The external control of anger is defined as the expenditure of energy to monitor and control the physical or verbal expressions of outward anger (for example, they may increase the risk of being aggressive or hostile toward other people or objects) [
5]. This variable was negatively associated with BP avoidant attachment orientation (whereas the association with attachment anxiety was not significant). In this case, the mediational analysis showed that the external control of anger was a marginal mediator in the association between avoidant attachment orientation and BP (especially for the Affective Instability and Identity Problems subscales). Thus, participants having high levels of attachment avoidance were less likely to externally control anger, and this tendency, in turn, was predictive of higher scores of BP. The interaction of high suppression and low external control of anger may reflect the dynamics of maladaptive anger rumination, which was previously reported as a characteristic of BP in both clinical [
29,
77,
78] and non-clinical populations [
78]. According to the “emotional cascade model” [
79], high levels of negative effects in people with BP trigger rumination, which in turn intensifies the negative effect. As part of a vicious cycle, the intensification of the negative effect may lead to the dysregulated behaviours described in BP patients, such as self-harm or substance abuse [
25,
28,
30].
The lack of behavioural control is in line with the evidence of aggressive and self-harm behaviours in BP patients [
80], suggesting that difficulties in emotional control could be a critical factor in contributing to the behavioural characteristics of BP disorder. Of note, in the present study, BP features in the domain of self-harm were predicted by less control of outside anger, whereas it was not significantly predicted by suppression. Thus, the poor capacity to control anger in particular could determine a higher rate of aggressive and self-harm behaviours, possibly suggesting that the incapacity to control anger spreads both outwardly and inwardly. In this sense, rumination and aggressive behaviour can be viewed as two faces of the same coin of emotion regulation difficulties, leading to cognitive or behavioural avoidance of adaptive anger and increased anger dysregulation [
81].
There are a few noteworthy limitations in the present study. First, although our sample was reasonably large, it was composed of healthy participants. In future studies, working on samples composed of individuals affected by borderline personality disorder may help to better establish the relationship between borderline personality, attachment orientations and anger regulation. Second, this study relied entirely on self-reported measures. Future studies will likely benefit from the use of more sophisticated diagnostic procedures, such as clinician-administered diagnostic measures for the assessment of borderline personality, and semi-structured interviews for the assessment of attachment styles (e.g., Adult Attachment Interview; [
82]). Moreover, among self-reports, the subscale Negative Relationships of the PAI-BOR has limited reliability (
α = 0.56); thus, results concerning this domain must be considered with hesitation. Finally, although the mediation models involving anger regulation were statistically significant, the cross-sectional design of our study makes it impossible to draw causal inferences.
Clinical Implications
Attachment-related behaviours are theorized to be stable from childhood to adulthood [
83] and this hypothesis has been largely confirmed by attachment research [
84,
85]. Even if research supports the suggestion that attachment styles may change during the course of psychotherapy ([
86,
87], this achievement can be considered difficult. Due to this difficulty in changing attachment styles, the examination of the mediating effects of other variables, which may be better modified through clinical interventions, has relevant clinical implications. In recent years, emotion regulation strategies have emerged as a key element for the reduction of psychological difficulties associated with attachment [
88]. In this perspective, the results of the present study may have crucial clinical implications for the treatment of BPD.
First, we suggest that psychological treatments of BP patients should aim for the reduction of the “holding in” strategy to regulate anger. Among others, useful therapeutic techniques may include encouraging the identification and expression of anger (expressive techniques), as well as exposure to anger (behavioural techniques) and the parallel building of anger tolerance through the promotion of acceptance-based regulation, as opposed to suppression and rumination [
89]. Considering the observed interplay between attachment and anger regulation, the therapeutic relationship may also have a key role. The adaptive expression of anger can take advantage of the security of the therapeutic setting. Moreover, encouraging and validating adaptive anger expression, as well as expressing empathy, would help in the construction of more adaptive ways of expressing spontaneous emotions [
90,
91]. Second, when ruminative processes or uncontrolled behavioural expressions of anger are active, therapeutic interventions can be used to block emotion dysregulation and promote the use of more adaptive strategies of emotion regulation [
92,
93,
94,
95]. For example, useful techniques may include the identification of maladaptive forms of regulation, distinguishing adaptive anger expression from suppression or rumination, paying attention to the negative consequences of turning anger toward the self (anger in), and all forms of anger mentalization techniques.








{kind=link}
{kind=link}