In our study, we demonstrated on a large series of 57 patients with PAs operated through an ETTA that this approach can both represent a valid alternative and an effective complementary route for the TCA, with a radical resection rate of 57.9% (33 cases) and hypersecretion resolution in 64.3% of cases (9 out of 14). Indeed, the ETTA has proved not only to allow the surgeon to manage through a trans-sphenoidal route those adenomas not approachable with a standard EEA and otherwise requiring a TCA (for example, because of their purely supradiaphragmatic location or due to atypical irregular morphology); it was also proved that the ETTA can be combined with a TCA, as reported in two cases in our series, for those asymmetrical tumors whose lateral extension would represent a limit for the ETTA. This is, to our knowledge, the largest surgical case series focusing on ETTA, which includes and compares all the different types of PAs suitable for the approach and discusses their indications.
4.1. Classification, Surgical Indications and EOR
The indications for an ETTA for PAs have been controversial in clinical practice and in the dedicated literature, and few studies have specifically considered this topic [
16,
17,
20,
21]. While well established in clinical practice for complex anterior skull base neoplasms, the ETTA conflicts with some fundamental principles of pituitary surgery, such as avoidance of diaphragm violation, with the consequent intra-operative CSF leak, and selective tumor resection, with the sparing of the gland and stalk structures to preserve the endocrinological function. Moreover, in the vast majority of cases, PAs—also including large or giant tumors—arise inside the sella from the pituitary gland, and they usually extend toward the suprasellar space in a caudocranial direction, displacing the diaphragm upwards. Therefore, after central debulking of the intrasellar part, the dome progressively descends in a downward direction, increasing its likelihood of being delivered through a conventional endoscopic endonasal approach without any need for a supradiaphragmatic extension. It has been hypothesized that less than 10% of PAs have an unsuitable morphology for a conventional EEA, thus requiring an alternative route, such as the TCA [
31,
32]. In 2013, Barazi et al. proposed that for these rare and selected cases unsuitable for a standard EEA, the ETTA could be considered as an alternative to the TCA, combining the advantages of the trans-sphenoidal corridor with the possibility to resect supradiaphragmatic PAs (
Figure 1). Our series confirms that only few cases require this extended approach, accounting for 2.4% in our series of 2351 endoscopic endonasal adenomectomies, which should be considered exclusively for those cases with peculiar features, which makes them unapproachable with an EEA, which remains the first choice for PAs. In particular, based on the tumor location and morphology, these authors identify three possible types of PAs potentially suitable for the ETTA.
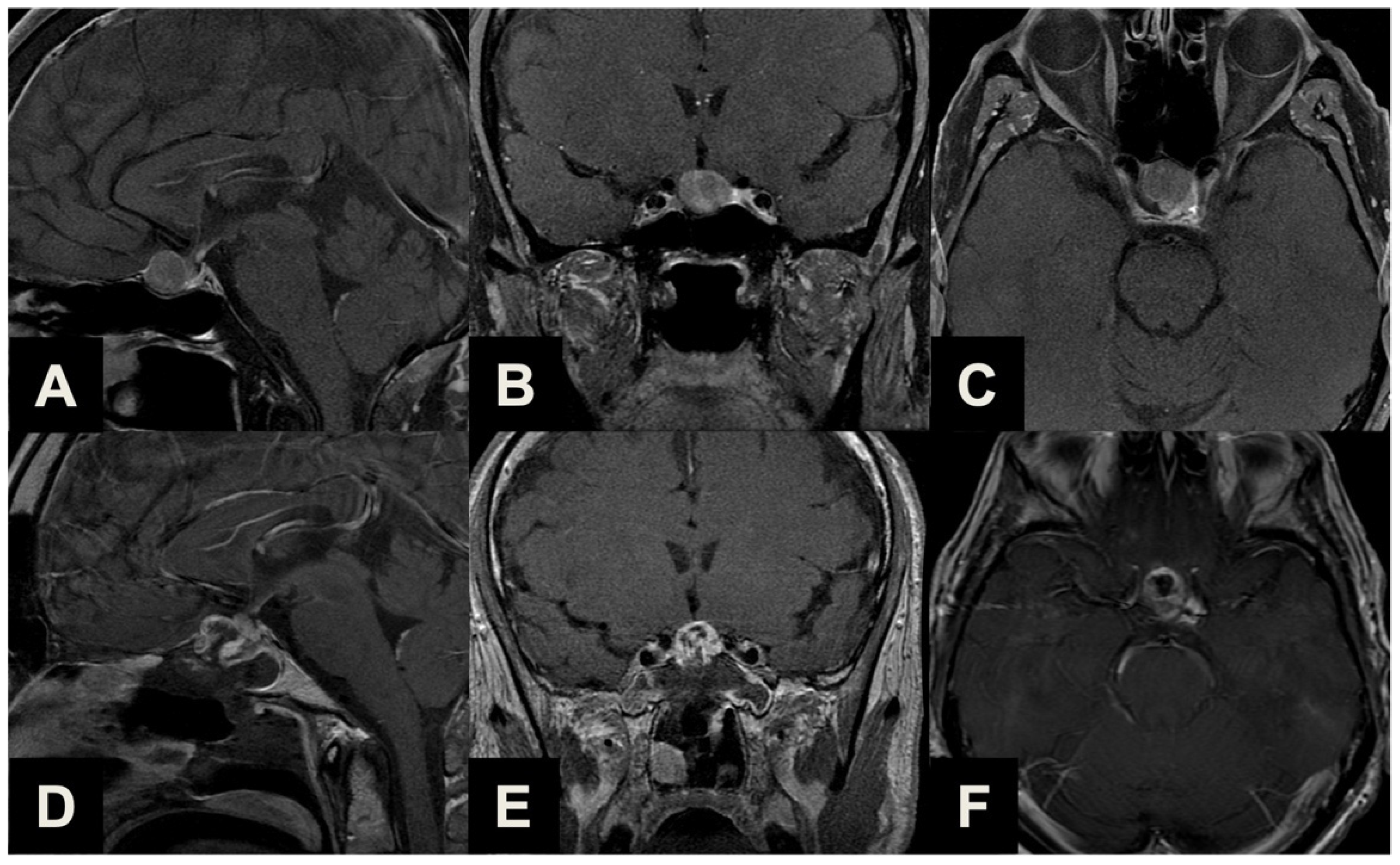
Ectopic peduncular or supradiaphragmatic peri-stalk PAs (Type 1,
Table 1,
Figure 2) are uncommon occurrences, as represented in our series (16, 28.1%), mostly including 5 (31.3%) ectopic secreting microadenomas of the pituitary stalk and 11 (68.7%) remnants or recurrences after previous partial surgeries of purely supradiaphragmatic macroadenomas. These tumors are not suitable for a conventional EEA because of the lack of any sellar infradiaphragmatic component, thus requiring a complete supradiaphragmatic corridor.
PAs with sub-frontal extension (Type 2,
Table 1,
Figure 3) are rare tumors (7, 12.3%) with a supra- or infradiaphragmatic sub-frontal extension, which extends rostrally up or beyond the tuberculum sellae, which prevents this portion from descending into the intrasellar cavity during tumor resection and which would require an unfavorable approach direction for a conventional EEA.
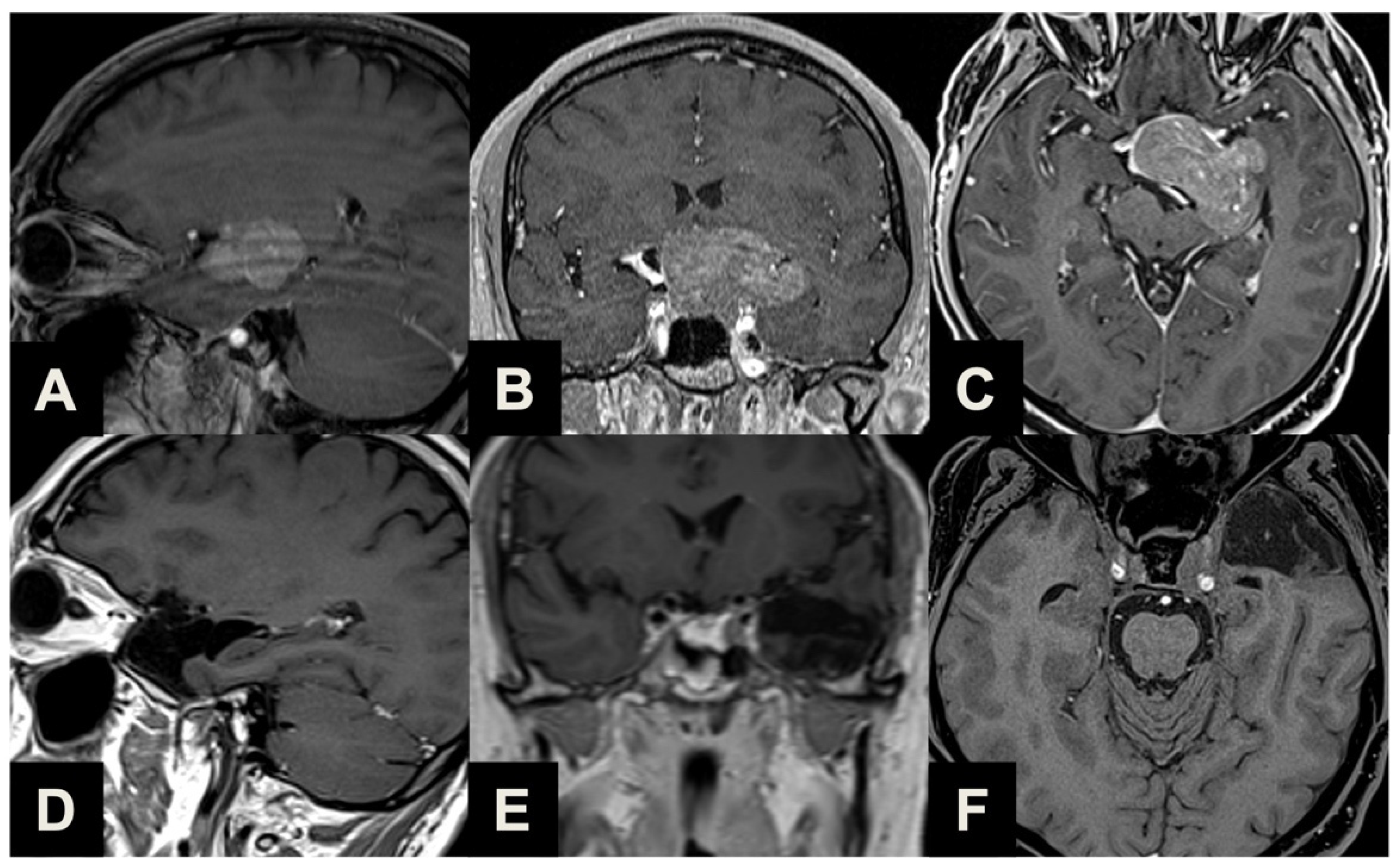
Finally, the most common indication for an ETTA was represented in our series by PAs presenting with a major extrasellar component (34, 59.6%) (Type 3,
Table 1,
Figure 4), such as macroadenomas with a suprasellar supradiaphragmatic component exceeding the sellar volume (i.e., air balloon PAs) unlikely to be delivered through the sella with an EEA, and macroadenomas with both a large intrasellar infradiaphragmatic part and a large suprasellar supradiaphragmatic portion connected through a narrow isthmus (i.e., snowman PAs), which impairs their resection through an EEA.
In some cases, a firm consistency may prevent the dome of the tumor from descending into the surgical cavity, and we primarily prefer to avoid extending the approach to these cases, instead using angled instruments and scopes to entirely remove the tumor. However, we noted that an increased consistency was reported in a significant number of PAs (21.1%), confirming that these tumors represent a challenge for the pituitary surgeon.
The flexibility of the approach, developed as an extension of the standard endoscopic endonasal route, also provides an opportunity for intra-operative conversion if required by the neoplasm features and surgical findings. Although in many cases, an ETTA is planned from the very beginning of the procedure (purely supradiaphragmatic neoplasms, major suprasellar extension), in other cases, where the standard endoscopic endonasal approach fails to achieve a satisfactory result (i.e., firm consistency of the neoplasm, non-descending diaphragm leading to suprasellar remnants), it can be intra-operatively extended to the ETTA to gain access to the supradiaphragmatic space. It is therefore our standard practice to preserve the septal mucosa during the first steps of every PA resection procedure, in case the harvesting of the naso-septal flap would later be unexpectedly necessary.
Radical resection was achieved in 57.9% of cases, in line with previous reports [
17]. This result should be outlined in the context of a highly complex case series, encompassing very large lesions with atypical morphology, vessel encasement and a significant number of secondary treatments. Indeed, comparing these results with those reported for the TCA series, we can observe a comparable degree of resection [
32,
34,
35,
36]. In our study, surgery for remnants and recurrences was observed to be a predictor of PR (
p = 0.033), probably due to the presence of adherences and scarring from previous approaches, precluding optimal and safe surgical maneuvers [
37]. Moreover, a close vessel relationship was also a factor precluding GTR (
p < 0.001), considering that surgical dissection around major cranial vessels is extremely challenging, even for experienced hands [
38]. It is also conceivable that advanced intra-operative imaging tools, such as intra-operative MRI, although never used in our surgical series, could help the surgeon increase the EOR by means of locating small remnants in the surgical cavity not detected by the surgeon’s eye, as reported in the literature [
39,
40]. Conversely, this could lengthen the duration of the procedure.
Although the ETTA represents an excellent extracranial approach for the suprasellar space, avoiding any brain retraction or vasculo-nervous manipulation, it poses an intrinsic drawback for the more lateral tumor extension than the carotid and the optic nerve planes. In these cases, the TCA could be proposed as a complementary approach to the ETTA (
Figure 5) [
41]. The lateral growing pattern of the neoplasm usually provides a “natural” surgical corridor for the TCA, while the ETTA helps the surgeon resect and debulk the median and paramedian part of the lesion, addressing the deepest intra- and suprasellar portion abutting the chiasm or the third ventricle from the ventral corridor, allowing for the achievement of a greater EOR and reducing the risk of recurrence [
42]. However, it should be remarked that in our series, we noted that the combination of an ETTA with a TCA would add significant morbidity, namely increasing the risk of post-operative DI (
p = 0.018) [
43]. Therefore, the choice of a combined TCA–ETTA approach should be balanced in an optimal risk–benefit assessment.
4.2. Surgical Complications
The incidence of post-operative CSF leak in our case series was 8.7% (five cases). All of them underwent a prompt endoscopic endonasal revision, and none of them developed meningitis. These results are in line with those reported by Khan et al., who assessed a pooled CSF leak incidence of 9% in a recent systematic review of extended endonasal approaches [
44]. Indubitably, this rate is higher than those reported for conventional EEA, and this represents the main disadvantage of this approach. Throughout the years, the developing surgical experience and skills and the introduction of innovative repair techniques for large osteo-dural defects, such as the naso-septal flap, have led to an evolution in our techniques for skull base reconstruction. In our series, we observed no significant difference in CSF leak rates when comparing patients who underwent reconstruction with different techniques, as well as between the first and the second half of the case series. The only predictor of CSF leak was represented by higher BMI, which was also recognized as a negative prognostic factor in other series of endoscopic endonasal skull base cases [
45,
46,
47]. Moreover, a careful management of post-operative nasal care, with periodic saline irrigation and ENT evaluations, allows the patients to preserve an acceptable quality of life during the uncomfortable phase of crusting and nasal remucosalization, quantified over three months [
21,
48,
49].
Other complications were represented by the following incidences of 1.8% of post-operative epistaxis, 1.8% of meningitis requiring antibiotic treatment, 3.5% of asymptomatic brain ischemia, 3.5% of transient third cranial nerve palsy and 10.5% of surgical field hematomas, which required surgical treatment in 50% of cases. Analyzing the non-negligible incidence of surgical field hematomas, the remnant tumor apoplexy could be hypothesized as a strong risk factor for this occurrence. Unexpectedly, in only three cases (out of a total of six experiencing post-operative hemorrhages) was a non-radical resection performed. It is our opinion that, despite tumor remnant apoplexy being a crucial issue very well known to pituitary surgeons, the suprasellar, subarachnoid extension of our approach could slightly increase per se the risk factor for post-operative bleeding, unavoidably manipulating small capillaries and branches of hypophyseal arteries, which could bleed in a large emptied post-operative surgical cavity. Conversely, a resection as extensive as permitted, respecting vascular anatomy, should be the primary concern for the pituitary surgeon to also decrease the occurrence of swelling and bleeding of the remnant (especially in those cases, where a gross total resection is not amenable), whose risk, although reducible, could never be zero. The incidence of these complications represents a consequence of the expansion of the surgical approach into the supradiaphragmatic space. Comparing our complication rates with other ETTA series, we observe a similar incidence [
21,
50,
51], and it is important to remark that they are in line with the overall complication rates of the TCA approaches, confirming that, although the ETTA has a higher complication rate compared to the EAA, it is not more unfavorable than the TCA [
32].
4.3. Clinical Outcome
The most significant advantage of the ETTA is represented by the favorable clinical outcome. Full or partial regression of pre-operative visual acuity and field symptoms was observed in, respectively, 33.3% and 73.5% of cases. As reported by many authors, early decompression of the optic structures and vessel-preserving dissection enabled by the ETTA are the key features determining such positive results, which are significantly superior to the TCA for sellar and suprasellar pathologies [
50,
52,
53]. Similarly, our endocrinological outcome, with 26.3% of new-onset DI and 29.8% of anterior pituitary function worsening, seems not to be inferior to the TCA [
54].
In the context of an optimal multi-disciplinary management, the individuation of the predictors of visual and endocrinological post-operative impairment is crucial. In our cohort, the major predictors of post-operative DI were the volume (
p = 0.048), maximal diameter (
p = 0.006), vessel encasement (
p = 0.030), subarachnoid invasion (
p = 0.040) and inclusion of the TCA (
p = 0.016). Neurohypophysis and pituitary stalk are delicate structures, which are strongly affected when performing the ETTA. If in smaller lesions, namely Type 1 and 2, the stalk can be visualized, dissected and preserved early, in larger invasive lesions, it is displaced, and it can be inadvertently harmed after surgical maneuvers and dissection [
55]. Similarly, lesions with vessel encasement and subarachnoid invasion require prolonged surgical maneuvering, increasing the risk of meningo-hypophysial artery damage with consequent pituitary function deficits. Similarly, the neurovascular manipulation and dissection unavoidable in transcranial approaches represents a negative prognostic predictor of post-operative DI development. The predictors of unsatisfactory visual outcomes were larger lesion volume (
p = 0.027), diameter (
p = 0.017) and re-do surgery (
p = 0.024) for comparable reasons with the involvement of optic nerves, chiasm and tracts.

 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




